Article Text

Abstract
Background Mild internal jugular vein (IJV) compression, aimed at increasing intracranial fluid volume to prevent motion of the brain relative to the skull, has reduced brain injury markers in athletes suffering repeated traumatic brain injuries. However, an increase in intracranial volume with IJV compression has not been well demonstrated. This study used transorbital ultrasound to identify changes in optic nerve sheath diameter (ONSD) as a direct marker of accompanying changes in intracranial volume.
Methods Nineteen young, healthy adult volunteers (13 males and 6 females) underwent IJV compression of 20 cm H2O low in the neck, while in upright posture. IJV cross-sectional area at the level of the cricoid cartilage, and the change in right ONSD 3 mm behind the papillary segment of the optic nerve, were measured by ultrasound. Statistical analysis was performed using a paired t-test with Bonferroni correction.
Results Mean (SD) cross-sectional area for the right IJV before and after IJV compression was 0.10 (0.05) cm2 and 0.57 (0.37) cm2, respectively (p=0.001). ONSD before and after IJV compression was 4.6 (0.5) mm and 4.9 (0.5) mm, respectively (p=0.001).
Conclusions These data verify increased cerebral volume following IJV compression, supporting the potential for reduced brain ‘slosh’ as a mechanism connecting IJV compression to possibly reducing traumatic brain injury following head trauma.
- brain concussion
Data availability statement
Data are available on reasonable request. Data are available on reasonable request. Please contact corresponding author: 0000-0002-9304-0751.
Statistics from Altmetric.com
Introduction
A well-known principle regarding moving tanks containing liquids is that acceleration or change in direction causes them to develop waves which propagate, reflect, cancel and summate chaotically (ie, ‘slosh’). Slosh theory holds that the contents of our encased central nervous systems do not fully fill their containers. Acceleration-deceleration forces may, therefore, lead to ‘rattle’, wherein the brain bounces back and forth, striking the inner tables of the skull and causing surface contusions; and to ‘slosh’, where the distortion, compression, stretching and twisting of tissue causes damage to cellular and neurovascular structures. Complete filling of a partially liquid-filled container establishes a single centre of gravity as if it were solid, mitigating both rattle and slosh. The Monro-Kellie doctrine dictates that the space housing the brain can be filled only by tissue, cerebral-spinal fluid and blood. Applying internal jugular vein (IJV) compression was assumed to retain sufficient blood in the skull to fill, or at least decrease the intracranial compliance. Studies in a mouse model demonstrated that IJV compression leads to dramatic reductions of traumatic brain injury (TBI) from direct head trauma.1 2 Subsequent studies have confirmed brain protective effects of IJV compression in the accumulated trauma of contact sports.3–10
A critical gap in verifying the sequence of events between the IJV compression and slosh mitigation is the demonstration of filling the intracranial compartment and thereby reduction of the intracranial compliance. In upright humans, IJV compression must cause blood to back up against gravity, into the intracranial space, specifically the venous capacitance vessels and dural sinuses. It may, nevertheless, still not completely fill the intracranial compartment as blood can readily be redirected to drain via a high-flow capacity vertebral venous plexus, particularly at rest with quiescent circulation. As such, the filling of the intracranial compartment and reduction of the intracranial compliance is the crucial link in understanding the potential mechanism of IJV compression’s function in protecting the brain.
Filling of the intracranial volume capacity may occur without an increase in intracranial pressure (ICP), but an increase in ICP confirms its filling and encroachment on the limits of its compliance. In previous studies, we have shown that small increases in ICP can be detected by ultrasound-measured optic nerve sheath diameter (ONSD).11 The aim of this study is to verify the filling of intracranial compliance following IJV compression as evidenced by ONSD.
Materials and methods
Nineteen healthy volunteers (mean age 37.9) were recruited and provided informed consent prior to participation in this prospective observational study. Exclusion criteria included a history of previous TBI or known elevated ICP.
Two independent investigators recruited all volunteers and performed all ultrasound measurements on the IJV and ONSD. Ultrasound scans were performed on the right IJV cross-sectional area and ONSD before and after application of the IJV compression. IJV compression was applied in the sitting position with an elastic adjustable neck collar comprising two rectangular sponge pads (2 cm × 3 cm) over the IJV bilaterally, just superior to the clavicle. A 100 mL saline intravenous fluid bag was attached to a calibrated pressure transducer (Edwards Life Sciences Corp, Irvine, California, USA), which was placed between the collar and the back of each volunteer’s neck. The neck collar was tightened by traction of the Velcro elastic straps until a pressure of 20±1 mm Hg was achieved (figure 1). Once the correct pressure was achieved, multiple measurements of both the IJV and ONSD were performed over the course of approximately 3–4 min confirming steady levels. Ultrasound of the IJVs was performed at the level of the cricoid cartilage cephalad to the neck collar. Measurements were taken before and after the application of the cervical collar with increases in cross-sectional diameter confirming the application of adequate outflow resistance. The right eye was closed and covered with transparent film (Tegaderm 3M, London, Ontario, Canada). Transorbital ultrasound studies were performed using a SonoSite Edge ultrasound system (FUJI FILM SonoSite, Bothell, Washington, USA) with a high frequency (7–11 MHz) linear probe in the transverse plane as described previously.11 The ONSD was assessed 3 mm behind the papillary segment of the optic nerve, as maximal changes in the ONSD were expected in this region (figure 2). Statistical analysis comparing the changes in ONSD and IJV area before and after application of IJV compression was performed using a paired t-test with Bonferroni correction.

Application of IJV compression device in the sitting position. IJV, internal jugular vein.

Changes in IJV area (A) and ONSD (B) before and after the application of the neck collar. The ONSD is measured 3 mm behind the papilla in a perpendicular axis. IJV, internal jugular vein; ONSD, optic nerve sheath diameter.
Results
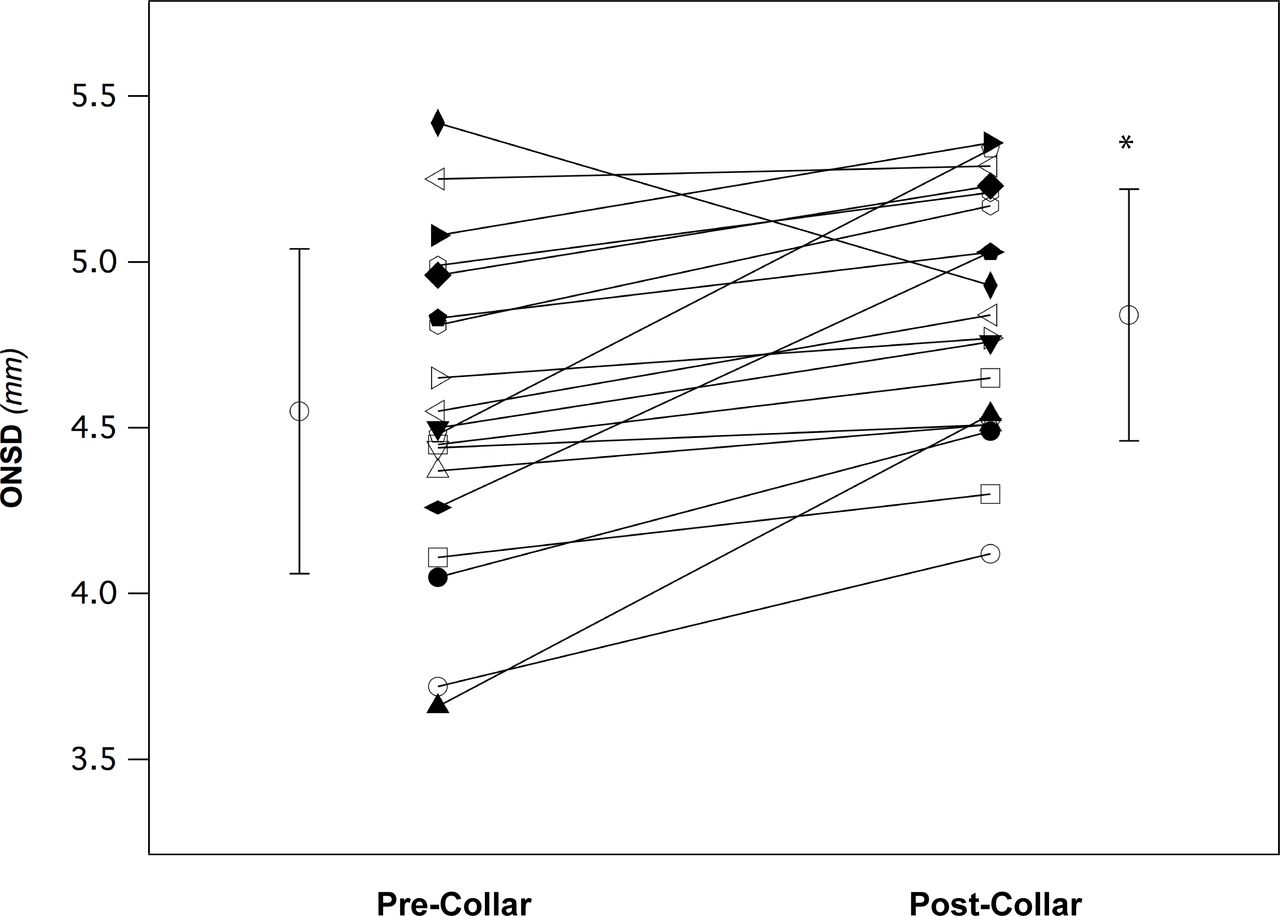
At baseline, the mean (SD) cross-sectional area for the right IJV at the level of the cricoid was 0.10 (0.05) cm2 with ONSD 4.6 (0.5) mm. After application of IJV compression, IJV cross-sectional area increased to 0.57 (0.37) cm2 with a corresponding increase of ONSD to 4.9 (0.5) mm (p=0.001) for both (table 1). Individual and mean (SD) changes in ONSD, both precollar and postcollar, are shown in figure 3.
Baseline characteristics and changes in study variables with before and after IJV compression

{kind=link}
{kind=link}
{kind=link}
Individual and mean (SD) changes in optic nerve sheath diameter (ONSD) at precollar and postcollar. *Values are significant; p<0.001.
Discussion
The main finding of this study was that IJV compression low in the neck of upright healthy volunteers resulted in an increase in the ONSD, a validated surrogate marker for an increase in ICP, and in turn, confirms the filling of the intracranial compliance in accordance with the Monro-Kellie doctrine. Previous investigations examining the IJV flow after neck compression in upright humans calculated that it would take about 6 mL of blood and ~2 s to fill the IJV into the skull and begin to encroach on the intracranial compliance.12 In the healthy population, patent occipital veins act as pressure relief valves resulting in only modest ONSD once the cerebral compliance is full. Thus, the unequivocal ONSD substantiates the physical link between IJV compression, and potential reduction in rattle and slosh, and thereby theoretical protection against TBI.
ONSD as a measure of ICP
ONSD ultrasound is a recently described non-invasive point-of-care surrogate measure for ICP.13 The optic nerve sheath is part of the continuous dura enveloping the cerebrum and communicates directly with the cerebrospinal fluid. Changes in ICP, rather than volume, are reflected in changes in ONSD. The reproducible relationships between ONSD and ICP has been demonstrated by the use of hypercapnia-induced increases in cerebral blood volume.11 14 15 ONSD is particularly convenient for the study of subjects in the sitting position, as radiological methods such as CT and MRI traditionally require subjects be supine. The intracranial compliance may, of course, be exhausted without an increase in ICP; however, the reverse is not possible. The increases in ICP following IJV compression confirmed the filling of the intracranial compartment and reduction of intracranial compliance, verifying the crucial step that may mitigate slosh effects following acceleration and blast forces.
Slosh theory
In humans, considerable recent research supports the claim that wearing IJV compression collars can effectively confer a protective benefit against concussions or measured effects of multiple head impacts. Prospective studies have demonstrated wearing IJV compression collars results in fewer MRI diffusor tensor imaging (DTI) markers of brain injury in competitive football players,3–5 hockey players6 and soccer players.7 8 Critics of this work have challenged the use of DTI as markers of brain injury,16 but the data remains remarkably consistent across sports and subjects. IJV compression has also been studied using functional MRI, consistently showing a reduction in brain activation changes during working memory tasks after just a single season, in both football9 and soccer7 10 players. Finally, IJV compression has reduced adverse changes on fMRI17 and electroencephalography18 associated with blast exposures.
Study limitations
A key limitation of this study is our inability to make direct measurements of intracranial volume prejugular and postjugular compression, or assess actual intracranial slosh and rattle. We have used an indirect measure of ICP in the form of ONSD, which is a validated technique and close surrogate. Furthermore, in our study we applied jugular compression using a static extrinsic pressure of 20 mm Hg. The OSND is used as a threshold measure—that is, binary, distended versus not distended. It has not been calibrated to ICP, much less IVJ pressure. The OSND crucial element for slosh is filling of the compartment rather than in increase in ICP. As such, any OSND implies a filling of the intracranial compliance. The degree of pressure required to effectively compress the IJV is variable between individuals, and this is directly affected by levels of hydration, anatomy and physiological variations between individuals. The crucial aspect is to provide sufficient compression to increase the flow resistance sufficiently to back up the IJV blood into the skull. Any further compression is not useful in this regard. Our application of a consistent 20 cm H20 pressure was designed to be above the minimal threshold for all subjects.
We performed a series of measurements immediately post IJV compression lasting 3–4 min, and therefore, did not evaluate the sustained effect of IJV compression on the ONSD. However, previous studies have shown a sustained increase in both ICP and intraocular pressure for 15 min and venous pressure for 20 min after the application of a neck collar in mouse and dog models, respectively.1 19 Further research looking at this effect during rigorous exercise over a prolonged time periods would be useful to confirm the continuous benefit of IJV compression throughout the course of sports and recreational activities.
An additional limitation of our study is the small sample size which prevents further analysis as to effects of age, sex or body mass index.
Clinical implications
Although this study does not specifically examine if IJV compression reduces concussions, it does support the potential mechanism for reducing slosh by increasing cerebral volume even in upright position. Currently, there are limited clinical studies to support the theory that jugular compression may provide brain protection during head trauma. As this holds tremendous potential, this is a critical area of future work in IJV compression and concussion research to investigate clinical outcome data.
Conclusion
This study confirms that there is an increase in cerebral volume following mild IJV compression in upright position. These data help support the potential for reduced brain ‘slosh’ as a mechanism connecting IJV compression to possibly reducing brain injury following head trauma.
What are the findings?
Evaluation of changes in optic nerve sheath diameter demonstrate that jugular venous compression increases cerebral volume and supports the contention that reduced slosh is the potential mechanism of brain protection during head trauma.
How might it impact on clinical practice in the future?
Jugular venous compression during contact sports and activities at risk for head trauma may play a pivotal role in reducing traumatic brain injuries.
Data availability statement
Data are available on reasonable request. Data are available on reasonable request. Please contact corresponding author: 0000-0002-9304-0751.
Ethics statements
Patient consent for publication
Ethics approval
University Health Network Research Ethics Board (14-8014 A).
References
Footnotes
Contributors MD contributed to the experimental design, data acquisition, analysis, manuscript and is responsible for the overall content as the guarantor. ZH contributed to data acquisition and analysis and manuscript. CTAB helped with drafting of manuscript and editing. JF contributed to experimental design and manuscript. LV contributed to experimental design and manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.