Article Text

Abstract
Objective Exertional heat stroke (EHS), characterised by a high core body temperature (Tcr) and central nervous system (CNS) dysfunction, is a concern for athletes, workers and military personnel who must train and perform in hot environments. The objective of this study was to determine whether algorithms that estimate Tcr from heart rate and gait instability from a trunk-worn sensor system can forward predict EHS onset.
Methods Heart rate and three-axis accelerometry data were collected from chest-worn sensors from 1806 US military personnel participating in timed 4/5-mile runs, and loaded marches of 7 and 12 miles; in total, 3422 high EHS-risk training datasets were available for analysis. Six soldiers were diagnosed with heat stroke and all had rectal temperatures of >41°C when first measured and were exhibiting CNS dysfunction. Estimated core temperature (ECTemp) was computed from sequential measures of heart rate. Gait instability was computed from three-axis accelerometry using features of pattern dispersion and autocorrelation.
Results The six soldiers who experienced heat stroke were among the hottest compared with the other soldiers in the respective training events with ECTemps ranging from 39.2°C to 40.8°C. Combining ECTemp and gait instability measures successfully identified all six EHS casualties at least 3.5 min in advance of collapse while falsely identifying 6.1% (209 total false positives) examples where exertional heat illness symptoms were neither observed nor reported. No false-negative cases were noted.
Conclusion The combination of two algorithms that estimate Tcr and ataxic gate appears promising for real-time alerting of impending EHS.
- hot temperature
- heat-shock response
- physical activity
- preventive medicine
Data availability statement
No data are available. Data are not publicly available.
Statistics from Altmetric.com
Introduction
Exertional heat stroke (EHS) is a life-threatening illness in which exercise, environment, clothing and other factors combine to produce a rapid and abnormal increase in core body temperature (Tcr) (often higher than 40.5°C) and central nervous system (CNS) dysfunction.1–3
EHS often presents as a state of confusion coupled with extreme fatigue and can rapidly progress to unconsciousness, organ damage and, in ~5% cases, death.4 Gold standard treatment is rapid cooling by whole-body immersion in ice water.5 6 Reducing the time Tcr is at very high temperatures is critical to minimising organ damage and overall prognosis.5 Survival of EHS without medical complications is dependent on the rapid recognition, rapid cooling and rapid advanced treatment.7
While advances have been made in environmental monitoring and managing environmental risk (high temperatures and high humidity) by moving exercise to cooler periods of the day, EHS8 9 remains a perennial problem for many high-intensity activities,10 11 with many cases occurring in temperate or cool conditions.12–14 A major contributing factor in these cases was individual motivation to complete a task. This is a common theme in team settings, where an individual may be feeling unwell but is motivated to perform/does not want to let down his/her team members or may face other pressure to continue.15 16
Individual attributes may contribute to susceptibility to EHS. Factors such as being unacclimatised to the heat, overweight, lacking in physical fitness, having prior illnesses, underlying medical conditions, dehydration, and drug and alcohol use have all been as associated with EHS.4 5 12 14 17 18 However, no single factor can explain EHS incidence, and only a small percentage of the overall group of study participants who have developed EHS had these literature-identified risk factors.14 19 Likewise, many individuals with these risk factors never develop EHS.18
An approach to reduce the incidence and severity of EHS is to use body-worn sensors to identify individuals with prodromal signs of emerging illness and to refer them for medical care before pathology can evolve.20 21 Practical real-time methods exist to estimate Tcr,22 and actigraphy can be used to assess gait. While Tcr alone is a poor predictor of who will succumb to EHS,5 a high Tcr in combination with CNS dysfunction is quite specific to diagnosing EHS. In a number of studies, ataxic gait/wobbly gait has been identified as one of the precursors to EHS.14 23 24 This change from a regular gait to one of ataxia may offer some insight into CNS dysfunction.
Coordination of human movement (defined as the motion of one body segment relative to another) is regulated by the cerebellum.25 Injury to the cerebellum, such as a cerebrovascular accident or EHS, can cause gait abnormalities, such as ataxia.26 Triaxial torso-worn accelerometers can identify ground contact time during running27 and differentiate between walking with and without an external load,28 and appear suitable for field use.29 Because torso accelerometry can detect small perturbations in different activities, it is plausible that changes in torso accelerometry profiles could be indicative of ataxic gait due to CNS dysfunction versus exercise-induced balance loss.30 31
The purpose of this study was to examine whether gait markers and estimated core temperature (ECTemp) from high-intensity exercise could be used in combination to predict EHS in advance of occurrence.
Methods
Subjects
Data were collected on 1806 (1701 men and 105 women) US military personnel (mean±SD: age=23±4 years, height=1.77±0.08 m, body weight=78.1±10.4 kg) who were recruited from various military units and monitored while engaged in high-intensity military training activities (n=42) that, in most cases, included a pass/fail motivational component. Personnel participated in one (n=95), two (n=1043), three (n=460) or one of two multiday (n=208) activities (<72 hours), and except for the multiday participants, activities were separated by 24–48 hours.
High-intensity military training activities
The military training activities where data were collected were chosen based on their history of heat stroke incidents to increase the likelihood of recording data from an individual who succumbed to an EHS. Activities monitored included runs of 4 and 5 miles to be completed in 40 min or less while wearing shorts and t-shirts; 7-mile (2-hour completion requirement) and 12-mile (3-hour completion requirement) ruck marches, where participants wore long pants and long-sleeved shirts as part of their regular military uniform and carried a 14 kg load which included a military rifle. Two multiday training activities (~3 days’ duration) that included periods of ruck marching, runs and other periods of movement were also monitored.
Adequate fluid intake was encouraged prior to the events by training and medical staff, and for the 5-mile runs and ruck marches, water stations were located every 2.5/3.0 miles along the event route.
Measures
Prior to the training event, questionnaires were administered to collect self-reported demographic and wellness information from individuals regarding age, height, weight, Army Physical Fitness Training (APFT) 2-mile run times (that can be related to aerobic fitness32), whether feeling unwell, currently taking medications, currently using dietary supplements, received any immunisations within the last 30 days, whether they had visited a doctor or had an illness in the last 60 days, and to estimate their fluid intake within the last 12 hours. Heart rate (from ECG, recorded every 5 s) and triaxial accelerometry (128 Hz, ADXL362 chip, ±8 g; Analogue Devices, Norwood, Massachusetts, USA) were logged using a custom torso-worn physiological monitoring system (Heat Illness Prevention System; Odic, Littleton, Massachusetts, USA: weight=16 g, dimensions=7.0×4.3×0.9 cm), which was donned the day before the activity.
For participants who suffered an EHS, rectal temperatures were taken by trained medical officers (analogue thermometer) as they were cooled via the ice sheet method33 prior to evacuation to the military base’s medical facility. Final diagnoses for each of the patients who had EHS were obtained from the training unit as provided by the medical facility.
To examine whether an EHS case differed from their cohort for age, height, weight or APFT times, we identified when any of these parameters deviated from the cohort mean by more than 2 SDs. In these cases and after testing for normality (Shapiro-Wilk test, IBM SPSS Statistics V.26), we used the generalised extreme Studentised deviate test (computed according to the NIST/SEMATECH e-Handbook of Statistical Methods 34) to examine if this parameter could be considered a significant (α=0.05) outlier compared with the cohort. The intent of this analysis was to document any unique factors among EHS cases compared with their cohort. Results are presented as mean±SD.
Estimated core temperature
ECTemp was computed according to Buller et al,22 where initial core temperatures were estimated at 37.1°C and the initial variance was set to 0.02°C. Overall, the ECTemp algorithm has been validated in over 14 studies with more than 300 subjects and generally performs reliably from study to study, with similar root mean square error values (<0.30°C), bias, and limits of agreement (generally less than ±0.63°C).35
Gait instability assessment
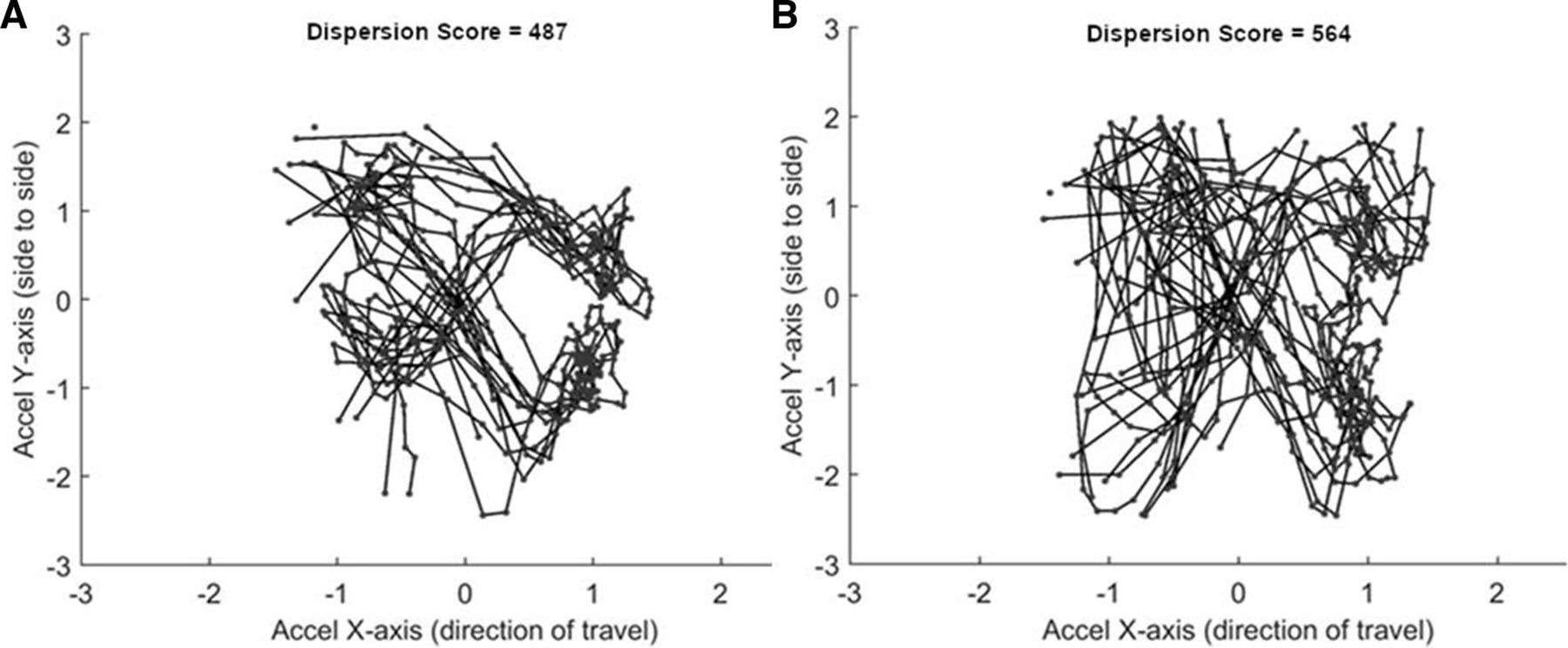
A gait instability score was developed from two separate features derived from the three-axis accelerometry data: autocorrelation peak heights and a dispersion score. Both of these features were baselined to each individual. The autocorrelation peak height features represent gait regularity by the consistency of acceleration time series at the periodicities of steps (vertical and longitudinal axes) and strides (lateral axis). Similarly, the dispersion features represent gait regularity by the level of clustering (and hence consistency) of repeated gait patterns across multiple steps, within each acceleration axis (figure 1 illustrates this concept).

Cross plot of a 5 s frame of normalised 128 Hz accelerometry data from the horizontal and longitudinal axes showing successive step-to-step acceleration patterns. (A) A more regular pattern and with a lower dispersion score compared with (B), which has less regularity, a more dispersed pattern and a higher dispersion score.
As our dataset contained bouts of either running alone (5 and 4 mile runs) or walking and running combined (ruck marches of 7 and 12 miles), it was necessary to segment the data into periods of walk and run so that periods of activity were compared with like previous periods. The full accelerometry processing pipeline and computation of the gait instability risk score are described in the online supplemental data 1.
Supplemental material
EHS detection
EHS detection algorithms were developed that used ECTemp, Gait Instability Score and the two measures combined. For EHS detection based on ECTemp, a Gaussian log-likelihood model was used, as shown in equation (1)
 (1)
(1)
where ECTempmax
=41.0°C and ECTempσ
was set to 1.0; if  , then
, then  was set to 0 (the maximum log-likelihood value). The final combined EHSrisk score is computed by summing the ECTemprisk likelihood with the individualised gait instability score for both walking and running movement types, and picking the highest combined score for either walking or running (equations 2, 3, and 4).
was set to 0 (the maximum log-likelihood value). The final combined EHSrisk score is computed by summing the ECTemprisk likelihood with the individualised gait instability score for both walking and running movement types, and picking the highest combined score for either walking or running (equations 2, 3, and 4).
 (2)
(2)
 (3)
(3)
 (4)
(4)
EHSrisk is a unitless score that can increase due to either ECTrisk or Gaitrisk or both. For EHS classification we varied the thresholds of the EHSrisk, Gaitrisk and ECTrisk so that we could identify all EHS cases (100% true positive rate) and minimise the number of false positives when all EHS cases were identified. Performance of the classifiers was examined by determining the false-positive rates (per event) when all EHS cases were identified. Further, we examined how the false-positive rates changed when the classifier thresholds were adjusted to increase the time of EHS prediction. We examined whether the predict-ahead time and the false-positive rate could be improved by increasing the number of allowed false negatives to be one and two.
The acceptability of false-positive rates will be governed by an organisation’s tolerance of risk along with their resources to respond to real-time predictions of EHS. For the military units, we have worked with, conducting a visual check-in and exertional heat illness assessment on 10 soldiers out of 150 during the course of a 3-hour exercise is well within their capacity.
Finally, the total number of examples of high-risk movement activities that could be used in the gait and ECTemp analysis was 3422 generated from participants whose data contained acceptable HR and accelerometry.
Results
EHS cases
Six individuals suffered from an EHS while completing one of the observed training events. Table 1 provides the event and individual characteristics and whether the individuals who had EHS differed from their cohort. All individuals who suffered from an EHS were male.
Event and EHS subject characteristics
Prior to the event, all individuals who had EHS reported feeling well and had no recent illness. None reported taking medications or dietary supplements; only one had a recent immunisation, and all reported consuming a similar amount of fluid as their cohort. Overall (n=3322), questionnaire responses prior to the training event indicated that 12% of participants felt unwell before the event and 7% had a prior illness within the last 60 days, and about 4% had reported taking supplements, medications or had recent immunisations. In all but one incident (as reported in table 1), these risk factors did not occur in conjunction with a recorded exertional heat illness.
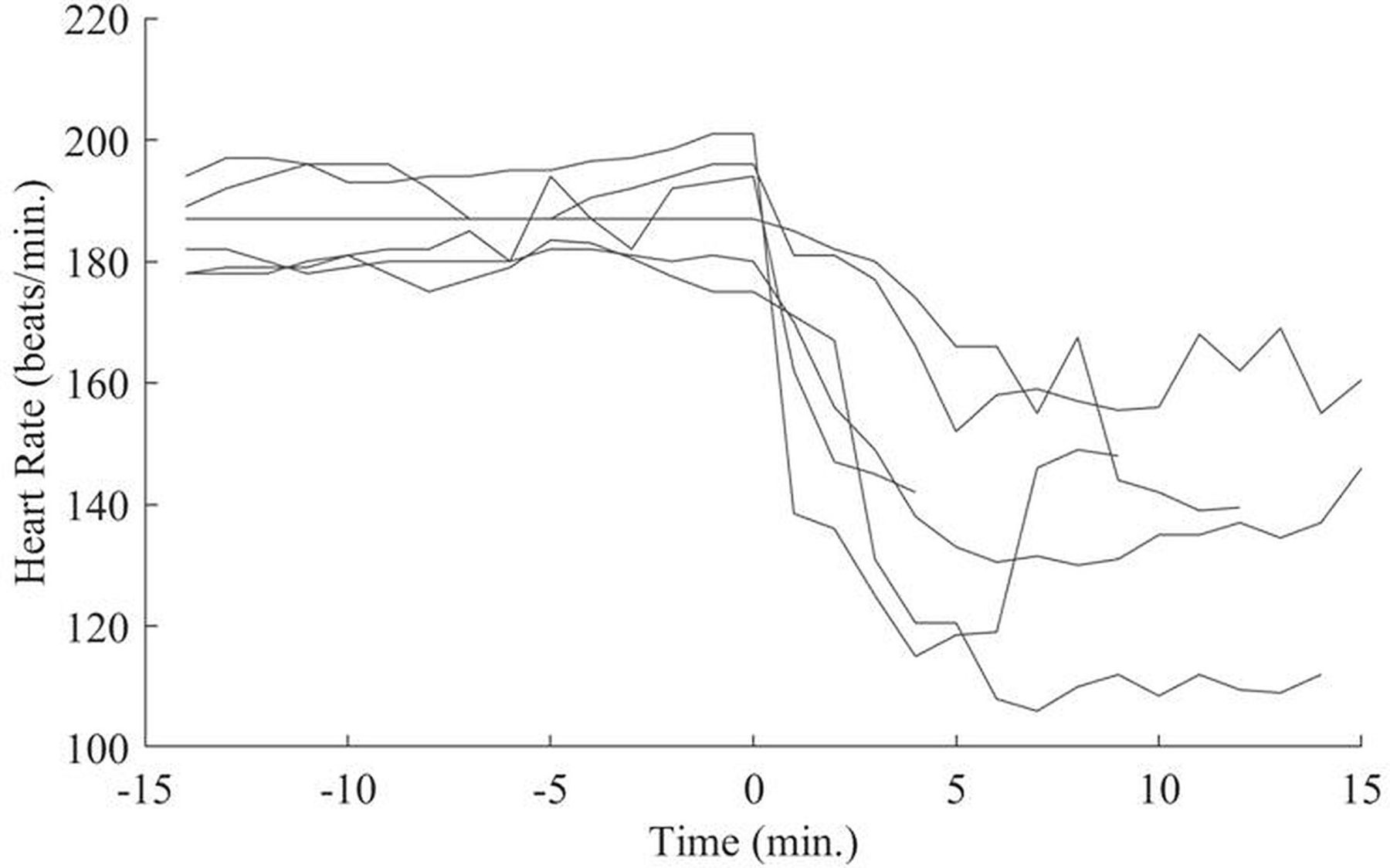
Heart rates for EHS volunteers were near their estimated maximal prior to stopping/collapse, and while they did decrease postcollapse, they remained elevated above resting levels (figure 2).
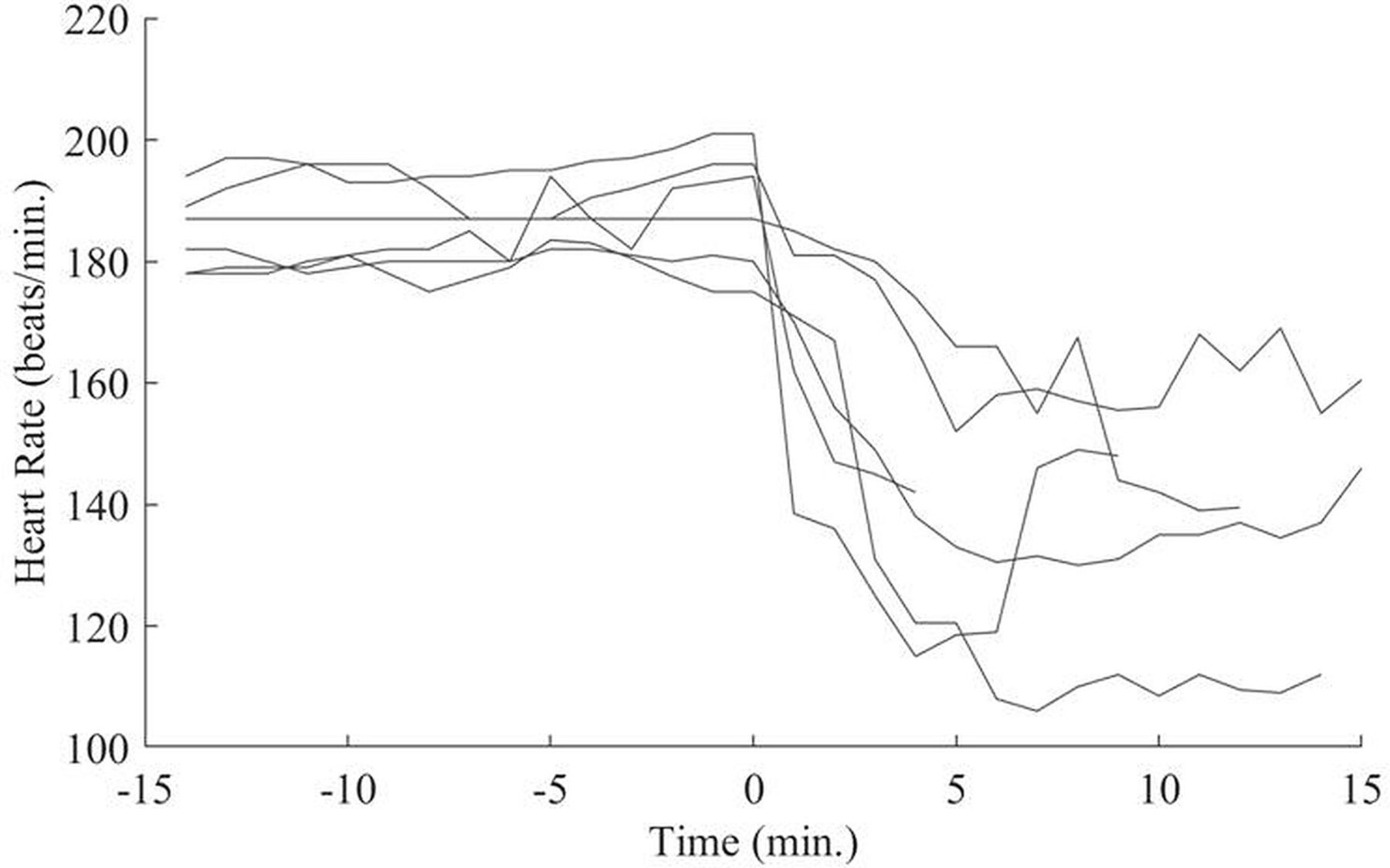
Heart rate for the six exertional heat stroke cases 15 min prior and postcollapse.
ECTemp and gait instability
For the six events where an EHS case occurred, the ECTemp in these individuals, in general, was hotter than most but was not specific in uniquely identifying the individuals who had EHS (figure 3). The gait instability score appeared to identify those who will experience an EHS with high specificity, but it also identified some other individuals not experiencing an EHS depending on the threshold chosen (figure 4).
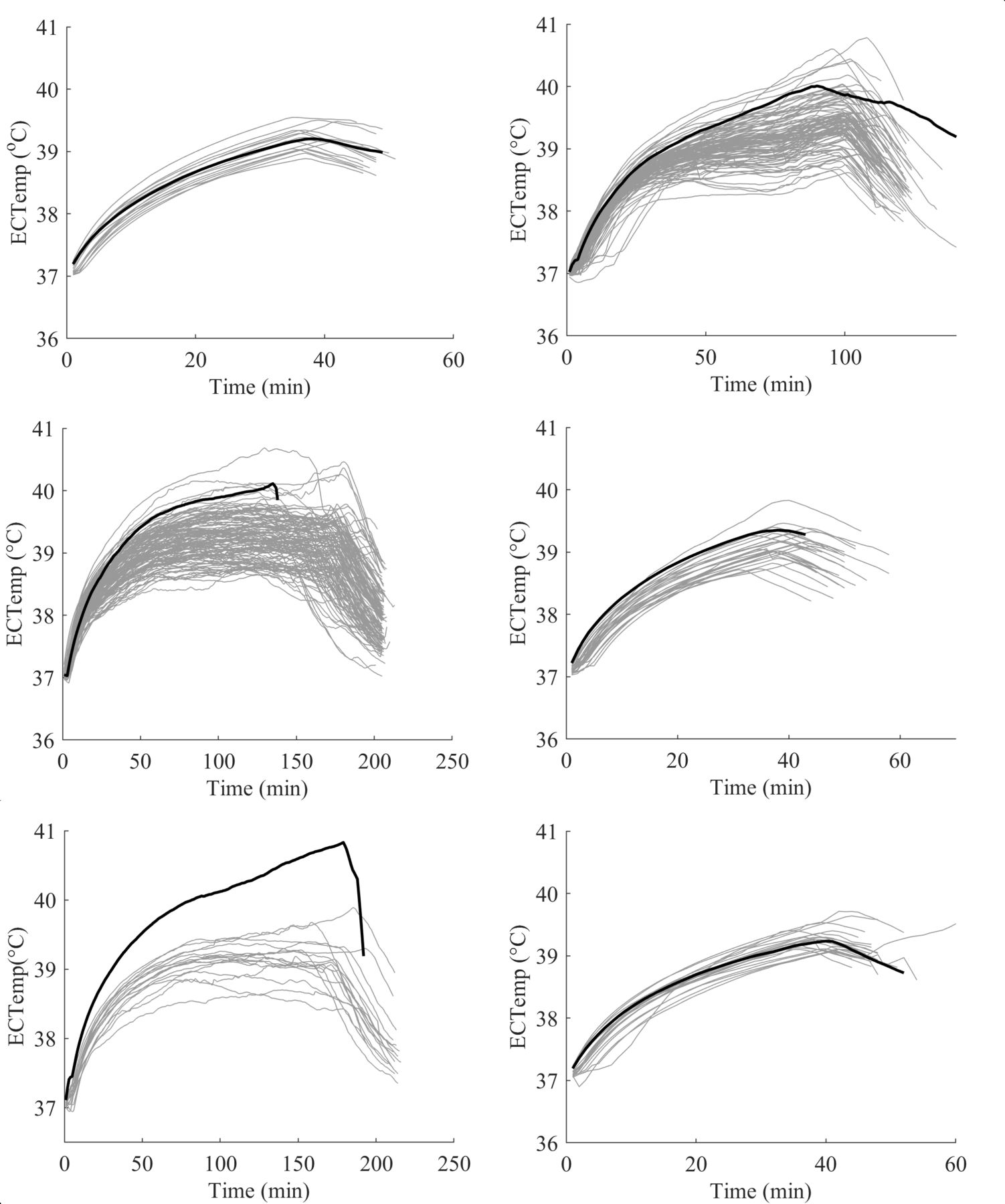
ECTemp for all subjects from six events where an individual suffered an EHS. Black bold lines indicate the EHS cases, while grey lines indicate other subjects with no exertional heat illness reported. ECTemp, estimated core temperature; EHS, exertional heat stroke.

Gait instability score for all subjects from six events where an individual suffered from EHS. Black bold lines indicate EHS cases, while grey lines indicate other subjects with no exertional heat illness reported. Time is from the beginning of the event to the event end. EHS, exertional heat stroke.
EHS prediction
False-positive rates for the three EHS classifiers were 26.7%, 2.7% and 0.9% (out of a total of 3416 examples where EHS was not identified), for ECTemp alone, gait instability alone, and the combination of ECTemp and gait instability, respectively. The classification thresholds were set to obtain 100% true positives with minimised false positives and were approximately 30 s prior to collapse.
As predict-ahead times were increased from 30 s to 300 s, the classification threshold became progressively smaller, resulting in a rise in false-positive rates (figure 5). For the EHSrisk (ECTemp+gait instability), as the prediction interval was doubled, there was a doubling in false-positive rate such that at 30, 60, 120 and 240 s, the false-positive rate was 0.9%, 1.9%, 4.5% and 9.4%, respectively. Predicting 300 s in advance resulted in a false-positive rate of 17.9%. However, between 120 s and 210 s, the false-positive rate remains fairly constant, increasing from 4.5 to 6.1. Figure 6, shows the EHSrisk score computed for all 3422 activities with the six EHS cases plotted in black and with the 210 s prediction threshold of 1.95 highlighted.

Predict-ahead time and false-positive rate for the gait instability score alone and in combination with ECTemp. ECTemp, estimated core temperature; EHS, exertional heat stroke.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
EHSrisk score for all high-risk activities. Black lines show the EHSrisk score for those participants diagnosed with a heat stroke. The dashed line shows the 3.5 min prediction threshold. EHS, exertional heat stroke.
As the number of false negatives was increased from one to two, the false-positive rate at 210 s decreases from 5.7% to 3.5%. When two false negatives were accepted, the predict-ahead time could be extended to 300 s with a false-positive rate of 4.4%.
Discussion
This study demonstrates the ability to predict EHS cases up to 3.5 min before occurrence with the combined assessment of ECTemp and gait instability metrics. The ability to predict and respond to EHS events and apply rapid cooling techniques that reduce Tcr at >0.15 °C/min within the first 30 min of EHS is key for good outcomes.7 Similarly, an ability to receive an early indication of impending EHS is suggested as a means of reducing the incidence of EHS in elite sporting events.20 While small, the 3.5 min early warning provided by the EHSrisk algorithm is more than 10% of this time window and would provide a cooling advantage of >0.5°C over current approaches of responding to collapse. In many remote settings, time is lost by identifying the location of a collapsed individual and sending medical and cooling resources to that point. Often the patient has to be transported to reach effective cooling mechanisms, such as ice water immersion.
Self-reported data showed no common risk factors among the EHS cases. Only two of the EHS cases indicated potential pre-existing risk factors where one volunteer was on the heavier end of the weight distribution than others in his cohort, and one had recently received an immunisation. These factors often do show up in combination with others for EHS cases, but by themselves would not predict EHS.27 This is highlighted when these factors are considered in the context of all subjects who had these same initial starting factors but did not experience an exertional heat illness. Additionally, all six EHS cases reported no use of medications and dietary supplements; all reported feeling well the morning of the training event; and all reported consuming adequate fluids within 12 hours of the event. While a deficit in fluid replacement can systematically lead to increased heat storage and additional rise in Tcr,36 the ECTemp algorithm performs similarly in both populations of euhydrated and dehydrated.22
All six of the EHS cases occurred at relatively high humidities, but care should be taken in these results. Efficient thermoregulation comes from the combination of three major heat transfer mechanisms of convection, radiation and evaporative heat loss.37 Early success in reducing military exertional heat illness came by moving events to early in the morning before the rise in daytime temperatures and where individuals would not be subject to solar radiation.8 9 While humidity is naturally higher at these early morning times, the reduction in temperature and limited solar radiation far out way the effect of high humidity. The activities for all our EHS cases were predawn and occurred at low WBGT levels that would not call for any modification of work rates. Additionally, two of the six EHS cases occurred in relatively mild environmental conditions (air temperature <15°C). This is consistent with previous findings of significant numbers of EHS cases and fatalities occurring in moderate temperatures.12 14
Estimated Tcr in five of the six EHS cases was in the upper portion of the cohort prior to EHS onset, but it alone was not a good discriminant of who was going to develop EHS. This finding is in agreement with earlier work suggesting that attainment of an individual core temperature threshold by itself is a poor predictor of heat stroke.1 In our dataset, two EHS cases have ECTemp values that are relatively low, close to 39.2°C at the point of collapse. Given the algorithm’s 95% CI of ±0.63°C,22 it could be expected for some individuals to fall at the bottom of this distribution, but it is illustrative that core temperatures alone do not predict EHS with a level of discrimination necessary to be useful for early EHS symptomology detection. The effect of the lower core temperatures on the combined EHSrisk classification can be seen when the false-negative count is relaxed. When two false negatives are tolerated, the EHSrisk classifier predicts the other four heat strokes at least 5 min in advance with a false-positive rate of 4.4%.
Gait instability was acceptably accurate in discriminating the six EHS cases prior to the point of collapse, suggesting that CNS dysfunction, especially cerebellar dysfunction, becomes significant enough to affect a highly trained and basic autonomous function such as gait. This also fits with many anecdotal observations that individuals experiencing heat stroke have an ataxic gait.14 23 24 26 However, extending the predict-ahead time lead to at least 3.5 min in advance increased the false-positive rate to 14%. Combining gait irregularity and ECTemp reduced this false-positive rate to 6.1%. The low number of false positives would suggest that the EHSrisk score is differentiating well between exercise-induced balance loss from fatigue30 31 and ataxic gait induced by EHS. The combination of ECTemp and gait instability as an EHSrisk score corresponds naturally to the clinical definition of high temperature combined with CNS dysfunction.
Strengths and limitations
Due to the rare nature of EHS and the ability to collect data prior to an EHS, the gait irregularity score and EHSrisk score were developed using only six subjects. With the large number of non-EHS cases, we can be fairly confident in the false-positive rate, but importantly, the false-negative rate remains undetermined.
The ‘false-positive’ label is specific to individuals in an event that did not subsequently lead to collapse. It is unknown whether these individuals whose gait became significantly more irregular were suffering from an exertional heat illness that did not progress to EHS, or from a musculoskeletal injury or were truly false positives.
The EHSrisk score is dependent on automatically learning an individual’s ‘normal’ gait during the course of an event. Thus, the current approach only works when a regular gait can be established, such as during a run or ruck march. It may have less applicability when a regular gait cannot be assumed, such as in firefighting or other occupational labour tasks where work is intermittent.
It should be noted that once an individual transitions to an EHS state, the underlying assumptions of the ECTemp model are no longer valid. The ECTemp algorithm is based on an HR to Tcr relationship that captures a consistent ratio of cardiac output for fuel and oxygen delivery to the muscles, and for blood flow to the skin across a range of environmental conditions. Our data show that in all the EHS cases, the HR drops once ambulation stops, which would lead to a decrease in ECTemp. This is contrary to the actual rapid rise in Tcr expected during thermoregulatory dysfunction1 and observed Tcr prior to evacuation. This underlines the importance that once EHS has occurred and treatment by medical staff has begun, a measured rectal temperature is critical. Measured Tcr provides important EHS diagnosis information and provides both cooling efficacy and cooling stopping points.
Finally, the current algorithm is based on an estimate of Tcr derived from heart rate and uses chest worn accelerometry to assess gait. This is both a strength and a weakness. A single, easy to don and wear chest sensor was used to maximise recruitment and enable large-scale data collection facilitating the observation of six rare EHS outcomes. Similarly, the simplicity of these measures allow for the algorithm to be translated to other fairly common sports physiological monitors. However, we anticipate (with some evidence from the relaxed false negative analysis) that by monitoring direct measures such as Tcr and using more advanced inertial measurement devices located on the legs,38 the EHSrisk prediction algorithm could be improved by reducing the false-positive rate and increasing prediction times.
Conclusion
By combining two independent methods, one assessing body core temperature (ECTemp) and the second assessing gait irregularity, we have demonstrated that a real-time EHS risk algorithm was capable of identifying all six observed EHS cases 3.5 min in advance with only a 6.1% (n=209) false-positive rate out of 3416 examples. In the current dataset, we have zero examples of false negatives, which are necessary to assess the true efficacy of the algorithm. The EHSrisk score required only two sensor inputs: minute-by-minute heart rate and triaxis torso accelerometry. These measures are fairly ubiquitous in modern health and fitness wearables. With the use of simple wearables, the EHSrisk score provides a means to alert medical staff to an individual who is in imminent risk of EHS, thus reducing the time to treatment and hopefully improving prognosis for recovery.
What are the findings?
Exertional heat stroke (EHS) can be predicted several minutes in advance of collapse from measurements of heart rate and accelerometry that assess body temperature and gait instability.
Physiological measurements from six volunteers prior to and postcollapse from EHS are used to develop a heat stroke classification algorithm.
Over 3400 examples of runs and timed road marches show only a 6.1% false-positive rate for a 3.5 min advance warning of EHS.
How might it impact on clinical practice in the future?
Use of common wearable physiological monitors could provide advance warning of EHS to both individuals and medical personnel, allowing timely interventions.
Data availability statement
No data are available. Data are not publicly available.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Medical Research and Development Command Institutional Review Board (Frederick, Maryland) on 15 June 2018 (number M-10720). Participants gave informed consent to participate in the study before taking part. This study was conducted under the oversight of the US Army Medical Research and Development Command Institutional Research Board in accordance with the principles embodied in the Declaration of Helsinki and in accordance with the US statutory requirements.
Acknowledgments
The authors thank all the Soldiers and Marines who consented to take part in this study along with their training commands. Collecting these data would not have been possible without their assistance. We wish to also thank Mr Oscar Powers, CPT Davel, and MAJ Bascom for their support in collecting data at Fort Leonard Wood, Missouri. We extend our thanks also to Mr Alexander Welles, Ms Nancy Delosa and Tara Boettcher for their enabling software and data organisation that made so much of this study simple. We also thank Mr Alan Harner and Dr Reed Hoyt for their encouragement and support of these field studies. Finally, we thank Dr Scott Montain for his encouragement, leadership and ongoing support of this study, and his detailed critical review of the manuscript.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Study conception and design: MBul, RF, JS, MG and MBur; significant data acquisition: MBul, MBur, MG, BAB, MJM, KD, TM, CK, RF and CM; significant data analysis: MBul, EA, MJM, KD, TM, LW, BT and JRW; significant writing: MBul, RF, EA and JRW; critical review and revision input: all listed authors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer The views expressed in this paper are those of the authors and do not reflect the official policy of the Department of Army or Department of Defence (DoD). The MIT Lincoln Laboratory contribution to this work was supported by the Department of the Army under Air Force Contract No. FA8702-15-D-0001.
Competing interests MBul is the listed inventor on a patent for estimating core body temperature from heart rate, also known as estimated core temperature (ECTemp). Ownership of the ECTemp patent is held by the US Department of the Army. MBul, RF, JS, BT and JRW and LW are the listed inventors on a patent application, 'System and Method to Predict Exertional Heat Stroke from Torso-Worn Sensor'. This patent is jointly owned by the US Department of the Army and Massachusetts Institute of Technology, Lincoln Laboratory. As part of the Department of Defense employee incentive programmes, MBul, RF and JS are entitled to receive a portion of royalty payments for any licensing of the algorithms.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.