Article Text

Abstract
Objective To systematically review and synthesise patellofemoral joint reaction force (PFJRF) in healthy individuals and those with patellofemoral pain and osteoarthritis (OA), during everyday activities, therapeutic exercises and with physical interventions (eg, foot orthotics, footwear, taping, bracing).
Design A systematic review with meta-analysis.
Data sources Medline, Embase, Scopus, CINAHL, SportDiscus and Cochrane Library databases were searched.
Eligibility criteria Observational and interventional studies reporting PFJRF during everyday activities, therapeutic exercises, and physical interventions.
Results In healthy individuals, the weighted average of mean (±SD) peak PFJRF for everyday activities were: walking 0.9±0.4 body weight (BW), stair ascent 3.2±0.7 BW, stair descent 2.8±0.5 BW and running 5.2±1.2 BW. In those with patellofemoral pain, peak PFJRF were: walking 0.8±0.2 BW, stair ascent 2.5±0.5 BW, stair descent 2.6±0.5 BW, running 4.1±0.9 BW. Only single studies reported peak PFJRF during everyday activities in individuals with patellofemoral OA/articular cartilage defects (walking 1.3±0.5 BW, stair ascent 1.6±0.4 BW, stair descent 1.0±0.5 BW). The PFJRF was reported for many different exercises and physical interventions; however, considerable variability precluded any pooled estimates.
Summary Everyday activities and exercises involving larger knee flexion (eg, squatting) expose the patellofemoral joint to higher PFJRF than those involving smaller knee flexion (eg, walking). There were no discernable differences in peak PFJRF during everyday activities between healthy individuals and those with patellofemoral pain/OA. The information on PFJRF may be used to select appropriate variations of exercises and physical interventions.
- biomechanical phenomena
- knee
- osteoarthritis
- exercises
Statistics from Altmetric.com
Introduction
Patellofemoral pain affects more than 20% of adolescents and adults.1 It is thought that patellofemoral pain precedes patellofemoral osteoarthritis (OA)2–4—which affects more than 50% of individuals with knee pain or OA.5 Both patellofemoral pain and OA are associated with considerable burden, typically resulting in persistent symptoms, impaired function and poor quality of life.6–11
The patellofemoral joint plays a critical role in knee joint function, particularly during activities involving large flexion ranges (eg, squatting, stair ascent/descent).12 The patella, which is attached to the quadriceps tendon proximally and the patellar tendon distally, acts as a complex lever to enhance the mechanical advantage of the quadriceps muscle by increasing the moment arm of the knee extensors.13 The tension in the quadriceps muscle and patella tendon drives the patella against the surface of the distal femur, creating a reaction force, the patellofemoral joint reaction force (PFJRF), at the average point of contact. In its simplest sense, the PFJRF can increase due to greater quadriceps muscle force and increasing knee flexion—which causes the angle of pull between the quadriceps and the patellar tendon to become more acute.14 As the PFJRF is influenced by the quadriceps muscle force and knee flexion angle, some everyday activities and therapeutic exercises will expose the patellofemoral joint to a higher magnitude of PFJRF than others. As an example, a deep squat involves a high knee flexion angle and greater demand on the quadriceps muscle, results in a high magnitude of PFJRF.15
The PFJRF is distributed throughout the region of contact between the patella and femur, giving rise to a distribution of contact pressure (also known as contact stress) across the contact area.16 Excessive patellofemoral joint contact pressure might be harmful to the patellofemoral joint and may contribute to the development and progression of patellofemoral pain and OA.17 18 In a normally aligned patellofemoral joint, activities involving high knee flexion do not necessarily translate to excessive patellofemoral joint contact pressure, as the contact area increases with knee flexion angle.14 Currently, as direct measurement of in vivo patellofemoral joint forces, contact areas, and pressure distributions require invasive methodologies,17 computational modelling methods are used to infer patellofemoral joint forces and pressures. A common mathematical approach to quantify patellofemoral joint contact force involves the input of participant-specific parameters (ie, knee joint flexion angle and knee extensor moment) to a planar model of the knee constructed from previously published cadaveric data (typically containing mathematic representations of tibiofemoral joint and patellofemoral joint motion, the quadriceps effective moment arm, and the geometric relationship between quadriceps force, the patellar ligament and PFJRF) (figure 1). Patellofemoral joint contact pressure may then be estimated using the PFJRF and an approximation of patellofemoral contact area, typically obtained from imaging studies. A previously published systematic review highlights that large variability in patellofemoral joint contact area measurement used to calculate patellofemoral joint contact pressure19—for example, patellofemoral contact area from cadavers, from healthy individuals, and those with patellofemoral pain from previous studies have been used to calculate patellofemoral joint contact pressure. Although synthesising the evidence on patellofemoral joint contact pressure is problematic due to large variability in methodology, the evidence on PFJRF during movement tasks may be synthesised to gain important insights for understanding biomechanical changes associated with patellofemoral pain and/or OA.
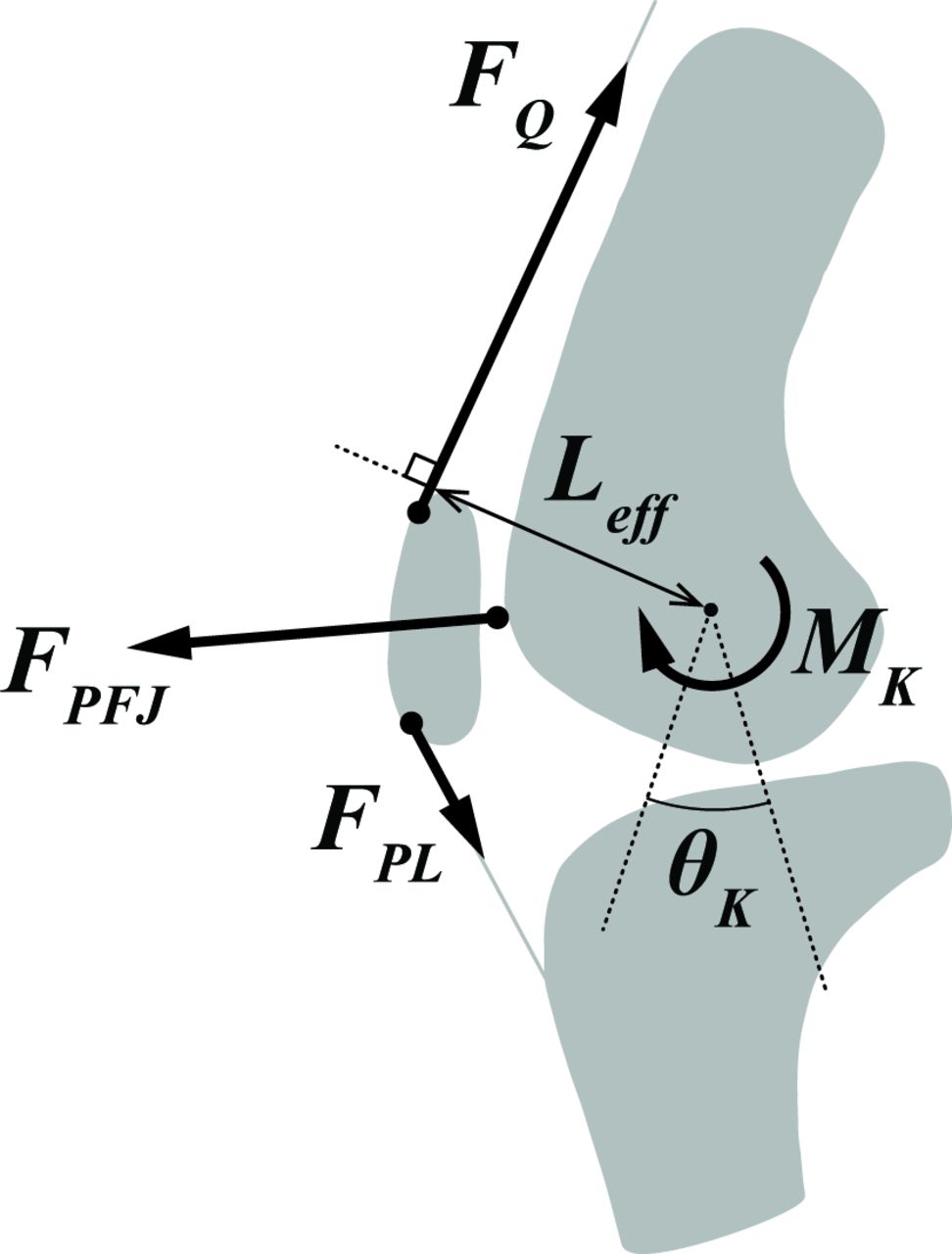
Typical planar schematic model of the knee. At any time instant:  is the knee flexion angle;
is the knee flexion angle;  is the instantaneous total quadriceps force vector;
is the instantaneous total quadriceps force vector;  is the instantaneous patellar ligament force vector;
is the instantaneous patellar ligament force vector;  is the instantaneous internal knee extension moment;
is the instantaneous internal knee extension moment;  is the instantaneous effective moment arm of the quadriceps about the knee joint centre; and
is the instantaneous effective moment arm of the quadriceps about the knee joint centre; and  is the instantaneous patellofemoral joint reaction force (PFJRF).
is the instantaneous patellofemoral joint reaction force (PFJRF).
Therapeutic exercises, such as quadriceps muscle strengthening, are recommended as a core treatment for patellofemoral pain and OA,20 21 and can be performed in various positions and knee flexion angles. A comprehensive summary of PFJRF during a range of activities and therapies will assist clinicians to select and prescribe therapeutic exercises and physical interventions to offload and/or progressively load the patellofemoral joint. Thus, this systematic review aimed to evaluate PFJRF during everyday activities, therapeutic exercises and physical interventions in healthy individuals. Since elevated joint reaction force is one factor that is thought to increase joint contact pressure,22 this systematic review also aimed to determine whether the magnitude of PFJRF is elevated in the presence of patellofemoral pain or patellofemoral OA.
Methods
Protocol
This systematic review is reported with reference to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Checklist. The protocol was prospectively registered on the PROSPERO International Prospective Register for Systematic Reviews website (CRD42016033552, registered January 2016). When we registered the study protocol, we were interested in evaluating PFJRF and patellofemoral joint contact pressure. Since then, a systematic review on methods to assess patellofemoral joint contact pressure concluded that there is considerable variability in patellofemoral joint contact pressure due to differences among methods and models and thus, data may not be comparable.19 Therefore, we only focused on PFJRF in this systematic review.
Literature search strategy
A comprehensive search strategy was devised using guidelines from the Cochrane Collaboration. The following electronic databases were searched with no date or language restrictions: Medline via Ovid, Embase via EBSCO, Scopus, CINAHL via EBSCO, SportDiscus, Cochrane Library. Our search combined three key concepts covering both Medical Subject Headings and keywords: patellofemoral, force/load and activity (online supplemental table 1). The original search strategy included terms to identify studies reporting PFJRF and patellofemoral joint contact pressure (load and stress are sometimes interchangeably used); however, the present review only focused on PFJRF.
Supplemental material
Two teams of two investigators (HFH and MCMK; BEP and PS) reviewed titles and abstracts for eligibility, and where relevant, full-text versions were screened and included in the review if they fulfilled selection criteria. Any disagreements were discussed and resolved in a consensus meeting. Reference lists of included publications were manually searched recursively until no additional eligible publications were identified.
Selection criteria
Selection criteria were as follows: (i) cross-sectional studies reporting PFJRF in healthy individuals, individuals with patellofemoral pain and/or patellofemoral OA during everyday activities and/or therapeutic exercises; or (ii) interventional studies investigating effects of physical interventions (eg, foot orthotics, footwear, taping, bracing) and gait retraining interventions on PFJRF in healthy individuals, individuals with patellofemoral pain and/or patellofemoral OA during everyday activities and/or therapeutic exercises.
No restrictions were placed on age, sex and method of recruitment. Reviews, case reports, conference proceedings, dissertations and unpublished studies were excluded. We excluded non-human, cadaver, pure biomechanical simulation studies that did not explicitly use data from human participants, including parametric studies using computational modelling, and quasi-static experimental studies. Studies with a sample size of less than 10 and non-English language publications were excluded. For this systematic review, and to allow for a wide range of methodological approaches, we defined the PFJRF broadly and simply as the magnitude of the net reaction force between the patella and femur due to the action of the quadriceps muscle and patellar tendon on the patella at any given knee flexion angle. Studies included did not have to explicitly define the PFJRF, but needed to, at minimum provide enough methodological detail to be able to determine that the approach met our broad definition of PFJRF.
Data extraction and synthesis
Participant characteristics (eg, age, sex, body mass, height), sample size, type and details of activities, exercises and interventions, PFJRF (peak or average), and units of analysis were extracted and entered into an Excel spreadsheet independently by two reviewers (HFH, BEP). We extracted the magnitude of PFJRF reported by each selected study as is, regardless of the specifics of the calculation approach, particularly whether the patellofemoral joint was modelled in two-dimension or three-dimension. Any disagreements and unresolved items were taken to a third reviewer (PS) for consensus. If sufficient data on PFJRF were not reported in the published article or online supplemental material, the corresponding author was contacted to request further data. If the author did not provide the requested information, the study was excluded. If multiple studies presented data from one cohort, the study with the most complete data was included. We converted PFJRF in N/kg to body weight (BW) by dividing it by 9.81 to pool studies. When multiple studies were available, the weighted average of means and SD were calculated (Comprehensive Meta-analysis Software V.3). Peak PFJRF and average PFJRF were evaluated separately. When PFJRF was reported in N (Newton), we used average body mass to obtain approximate PFJRF in BW (N÷average mass in kg×9.81). This method provides an approximation and thus, these data were not used when calculating pooled mean and SDs. Results of individual studies (mean±SD) that reported PFJRF in healthy individuals, individuals with patellofemoral pain or OA during various everyday activities, therapeutic exercises and physical interventions are graphically displayed using forest plots. To conduct meta-analysis of cross-sectional studies in individuals with patellofemoral pain/OA compared with healthy individuals, at least three studies were required.23 We planned to judge τ2 with 95% CIs, and the I2 values to determine heterogeneity (>75% signs of considerable heterogeneity). We planned to generate funnel plots for meta-analyses when at least 10 studies were available. When meta-analyses were not possible, we reported mean differences with 95% CIs (Review Manager V.5.3) for individual studies reporting PFJRF in individuals with patellofemoral pain or OA compared with healthy individuals.
Supplemental material
Supplemental material
Supplemental material
Methodological quality
Two investigators (MCMK and MGK) evaluated the methodological quality of included studies using the modified Downs and Black checklist.24 The checklist consists of 27 items organised into five domains: reporting, external validity, internal validity and power. The risk of bias was assessed using the following five sections within the internal validity domain: performance bias, reporting bias, detection bias, selection bias and attrition bias. For non-intervention studies, most items within the performance, selection, and attrition bias domains were not applicable. All items were scored as ‘+’ (yes) or ‘−’ (no or unable to determine), except for one item in the reporting section (item 5), which was scored as ‘++’ (distribution of principal confounders clearly described), ‘+’ (partially described) or ‘−’ (not described or unable to determine). In the original version of the Downs and Black checklist, item 27 that refers to power calculation is rated from 0 to 5 based on a range of study powers. In the present version of the checklist, we modified the scoring of item 27 and rated it as ‘+’ (power calculation performed) or ‘−’ (power calculation not performed). Any inter-rater disagreements were discussed in a consensus meeting and unresolved items were taken to a third reviewer (HFH) for consensus.
Results
Study selection, study characteristics and risk of bias
The comprehensive search strategy identified 8080 records, with the original search conducted on 14 January 2019 and updated on 2 November 2020. Following the removal of duplicates, 5349 abstracts were screened. The full text of 227 studies was retrieved and screened (figure 2). In total, 71 articles were included in the systematic review.25–95 There were 63 within-subject studies (56 healthy individuals, 7 patellofemoral pain), 1 randomised controlled trial in healthy individuals (online supplemental table 2) and

Study selection.
7 cross-sectional studies comparing patellofemoral pain or OA with healthy individuals (5 patellofemoral pain, 2 patellofemoral OA) (online supplemental table 3). The methods used to determine PFJRF in the included studies are presented in online supplemental table 4.
The results of the methodological quality evaluation using the modified Downs and Black checklist are presented in table 1. To summarise, most studies scored positively on the reporting domain. All included studies indicated a high risk of bias for external validity. Most of the studies did not report sample size calculations. Most studies had a low risk of reporting bias and detection bias. The scores for the selection bias were mixed. There were only six studies evaluated for performance and attrition bias. All six studies were of high risk for performance bias, and three studies were of high risk for attrition bias.
Methodological quality of the included studies assessed using the modified Downs and Black checklist
PFJRF during walking, stair ambulation and running
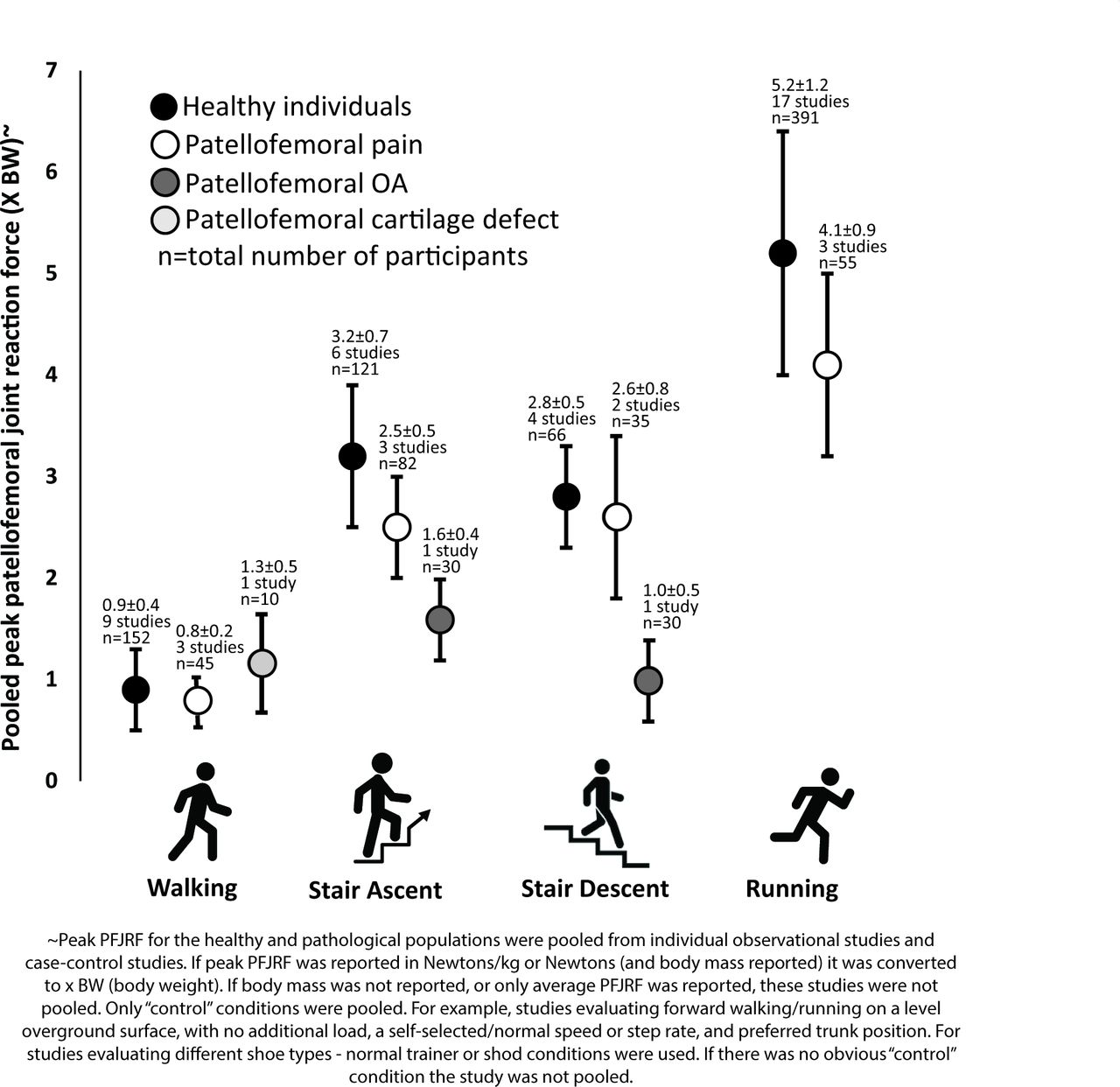
We identified 11 studies that reported peak PFJRF during walking in healthy individuals.36 38 39 41 51 63 71 83 84 88 92 The average walking speed ranged from 1.33 m/s to 1.50 m/s. Of these 11 studies, we were able to pool peak PFJRF from nine studies (0.9±0.4 BW)36 38 39 41 63 71 83 84 92 (figure 3). Data from two studies could not be pooled—one study reported peak PFJRF in N88 and one study examined the effects of different heel heights on peak PFJRF, but it was not clear which condition was the baseline condition.51 Three studies reported peak PFJRF during walking in individuals with patellofemoral pain.36 38 64 The average walking speed ranged from 1.32 m/s to 1.36 m/s, and the pooled peak PFJRF was 0.8±0.2 BW36 38 64 (figure 3). There was only one study that reported peak PFJRF in individuals with patellofemoral articular cartilage defects (1.3±0.5 BW)83 (figure 3). The average walking speed was 1.55 m/s.

Pooled peak patellofemoral joint reaction force (mean±SD) during walking, stair ambulation and running. OA, osteoarthritis.
Nine studies reported PFJRF during stair ambulation.28 38 39 41 42 48 65 84 85 During stair ascent, pooled peak PFJRF in healthy individuals was 3.2±0.7 BW28 38 39 41 48 84 based on six studies and 2.5±0.5 BW in those with patellofemoral pain based on three studies,38 42 65 and peak PFJRF in individuals with patellofemoral OA was 1.6±0.4 BW48 based on a single study (figure 3). During stair descent, pooled peak PFJRF in healthy individuals was 2.8±0.5 BW38 39 48 84 based on four studies and 2.6±0.8 BW in those with patellofemoral pain38 65 based on two studies, and peak PFJRF was 1.0±0.5 BW in individuals with patellofemoral OA48 based on one study (figure 3).
We identified 27 studies that reported PFJRF during running.25 26 34 35 38 39 50 52 56–59 61 68 69 74–76 78 80–82 87 90 91 93 94 Pooled peak PFJRF in healthy individuals was 5.2±1.2 BW25 35 38 39 52 56–58 61 68 74 80–82 87 90 94 based on 17 studies and 4.1±0.9 BW in individuals with patellofemoral pain34 38 78 based on three studies during running (figure 3). The average running speed ranged from 2.33 m/s to 4.47 m/s in healthy individuals and 2.77 m/s to 4.00 m/s in individuals with patellofemoral pain.
PFJRF during walking, stair ambulation and running with physical interventions
Many single studies reported PFJRF during walking, stair ambulation and running with variations such as gait speed, step length and strike pattern, and physical interventions such as foot orthotics, knee brace and footwear (figure 4). Due to considerable variability, we were unable to calculate pooled estimates.

Peak patellofemoral joint reaction force (PFJRF), unless otherwise specified, during walking, stairs ambulation and running.
PFJRF during other everyday activities, therapeutic exercises and physical interventions
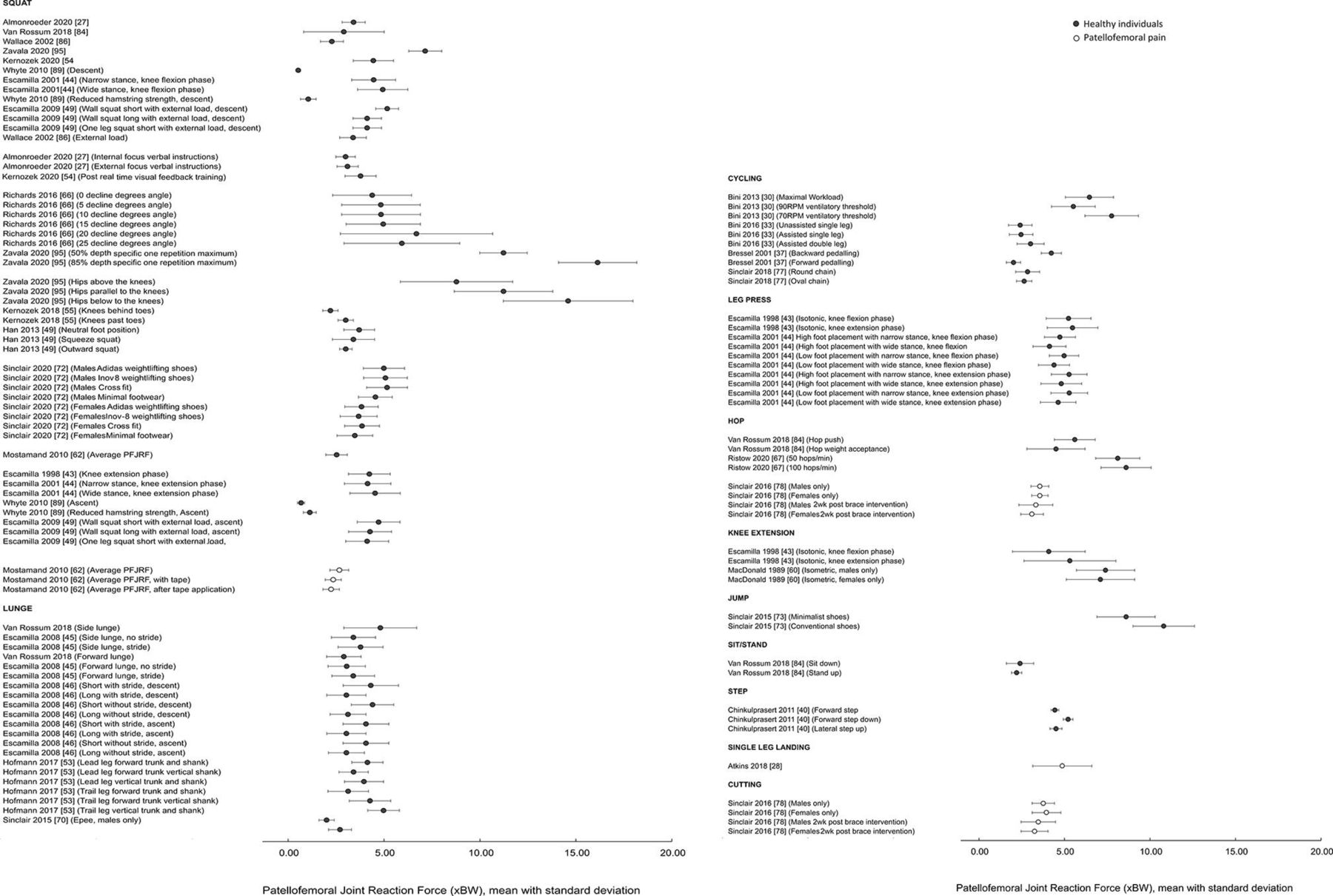
Studies also reported PFJRF during various everyday activities and therapeutic exercises such as squatting, lunging, cycling, jumping, hopping and stepping with variations, and physical interventions (eg, tape, footwear) in healthy individuals and those with patellofemoral pain (figure 5). However, it was not possible to pool the PFJRF during these activities due to different variations and conditions used. Two studies reported PFJRF in %workload during cycling and one study reported PFJRF in Newtons during leg isometric leg press but did not report body mass.31 32 79 Thus, estimates of PFJRF in BW could not be calculated for these three studies.

Peak patellofemoral joint reaction force (PFJRF), unless otherwise specified, during therapeutic exercises and physical interventions. Note squat is bodyweight/unloaded unless otherwise specified. RPM, repetitions per minute. Two cycling studies and one leg press study are not presented in this figure because we were unable to estimate PFJRF in birth weight (BW).
Comparison of PFJRF between healthy individuals and those with patellofemoral pain/OA
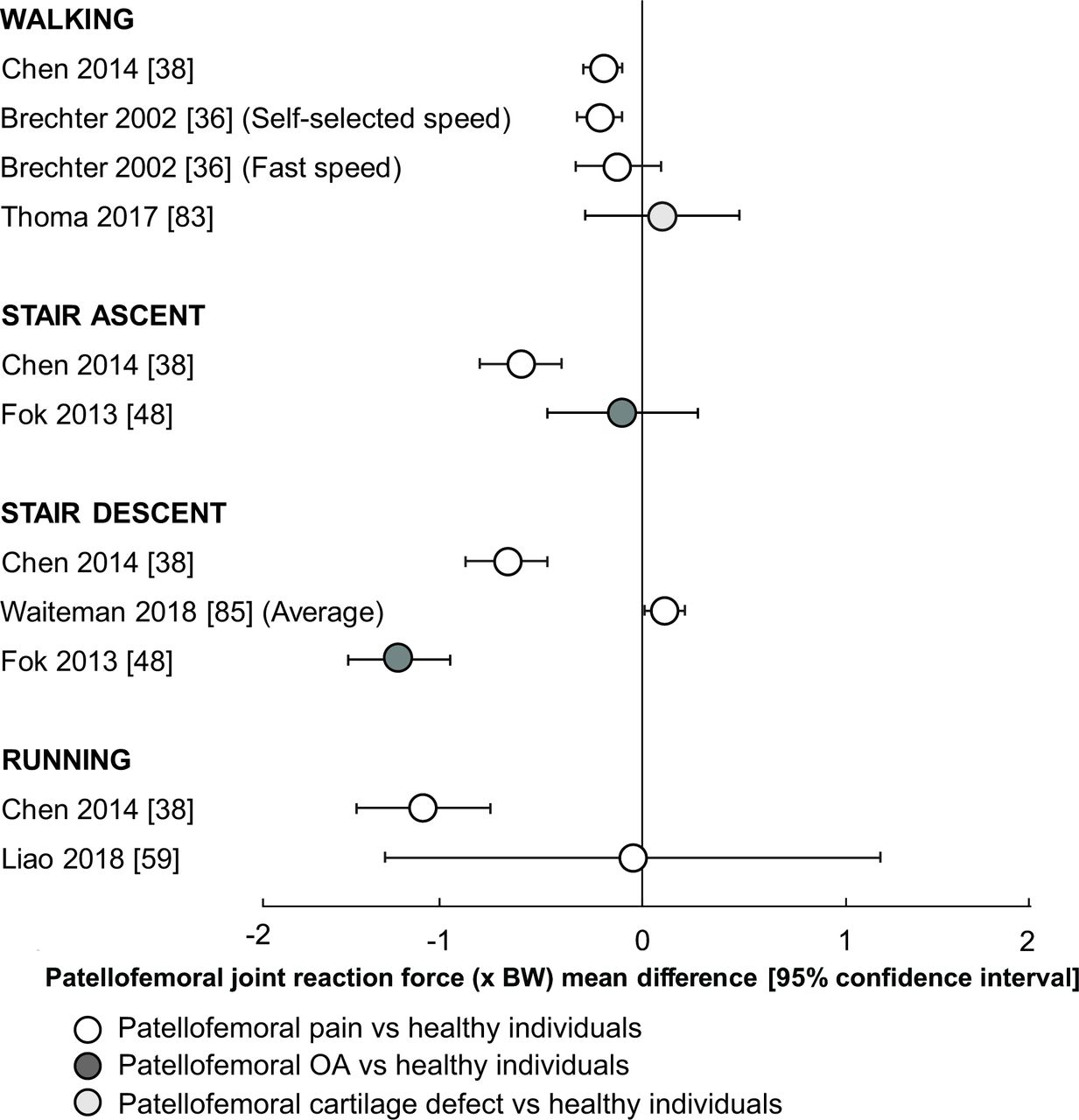
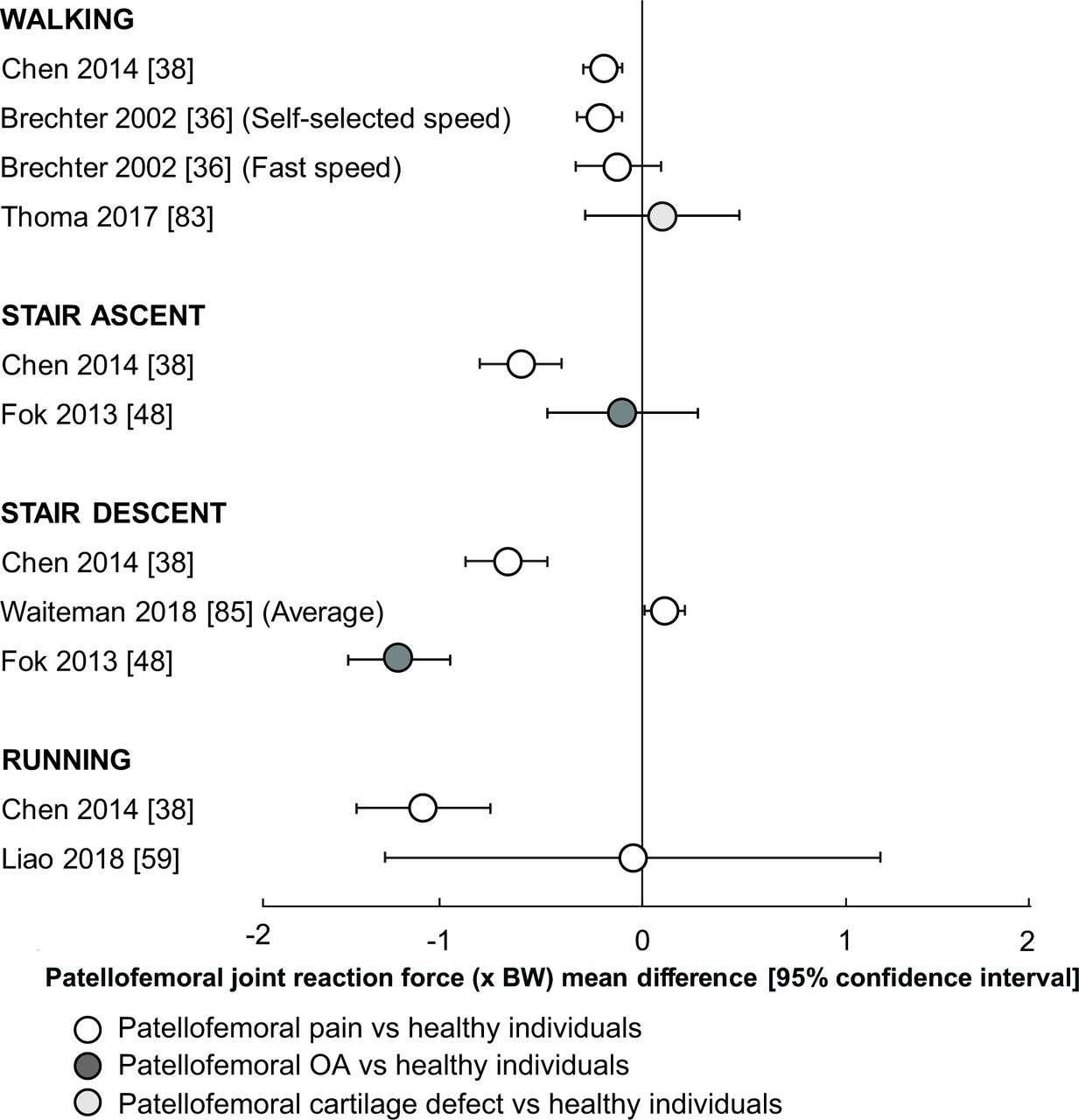
As only one or two cross-sectional studies were available reporting PFJRF in individuals with patellofemoral pain or OA compared with healthy individuals during different everyday activities, therapeutic exercises and physical interventions, and thus we did not conduct meta-analyses. As mostly single studies were available, we did not a conduct certainty assessment. Two studies reported peak PFJRF in individuals with patellofemoral pain relative to healthy individuals during walking36 38 (figure 6)—one study reported lower peak PFJRF in those with patellofemoral pain,38 and the other reported lower peak PFJRF in individuals with patellofemoral pain during self-selected walking, but not during fast walking.36 One study reported peak PFJRF during stair ascent and stair descent in individuals with patellofemoral pain relative to healthy individuals,38 and reported lower peak PFJRF in those with patellofemoral pain (figure 6). One study reported average PFJRF during stair descent and reported higher average PFJRF in individuals with patellofemoral pain relative to healthy individuals.85 Two studies reported peak PFJRF during running38 59—one study reported lower peak PFJRF in individuals with patellofemoral pain relative to healthy individuals38 and the other reported no differences between those with patellofemoral pain and healthy individuals.59 One study reported peak PFJRF in those with patellofemoral articular cartilage defects compared with healthy individuals during walking83 and reported no differences. One study reported peak PFJRF in those with patellofemoral OA compared with healthy individuals during stair ambulation48 and reported lower peak PFJRF in individuals with patellofemoral OA during stair descent, but no differences during stair ascent (figure 6).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comparisons of peak patellofemoral joint reaction force, unless otherwise specified, between healthy individuals and those with patellofemoral pain or patellofemoral osteoarthritis (OA).
Discussion
Summary of findings
This systematic review aimed to evaluate PFJRF during everyday activities, therapeutic exercises and physical interventions in healthy individuals, and in those with patellofemoral pain and/or patellofemoral OA. Based on weighted average means for healthy individuals and individuals with patellofemoral pain, there does not appear to be any discernable differences in peak PFJRF individuals with patellofemoral pain during walking, running, and stair ambulation. We identified the PFJRF during a range of everyday activities and exercises (eg, squat, lunge) in healthy individuals and those with patellofemoral pain.
PFJRF during everyday activities, therapeutic exercises and physical interventions
Our findings confirm that activities involving larger knee flexion (eg, stairs ambulation/squat) create a higher magnitude of PFJRF than activities involving smaller knee flexion (eg, level walking). In healthy individuals, peak PFJRF on average was 0.90×BW (95% CI 0.84 to 0.96) during walking, 3.2×BW (95% CI 3.1 to 3.3) during stair ascent, 2.8×BW (95% CI 2.7 to 2.9) during stair descent and 5.2×BW (95% CI 5.1 to 5.3) during running. Due to the wide range of exercise variations and conditions used in these studies, we could not calculate weighted mean PFJRF for therapeutic exercises. Based on individual studies (ie, not pooled), the magnitude of peak PFJRF reported ranged from approximately 1 to 18×BW for therapeutic exercises—for example, peak PFJRF observed ranged from 1 to 18×BW during squat, 3 to 6×BW during lunge, 1 to 7×BW cycling, 9 to 11×BW during jumping. Based on peak PFJRF values observed, some exercise variations expose the patellofemoral joint to higher PFJRF than others—for example, higher peak PFJRF were reported during lunge with stride than lunge without stride, and during squat with knees beyond toes than squat with knees behind toes. This systemic review provides a useful summary of PFJRF during everyday activities and therapeutic exercises with variations and physical interventions that could be a valuable resource for clinicians.
Interestingly, large differences in peak PFJRF were observed between studies for some of the tasks, in particular squatting (~1×BW to 18×BW). These differences may have been due to task variations and the models used. For example, Zavala et al 95 included results of loaded squats up to the participant’s one repetition maximum—this involves the addition of substantial mass (1×BW or greater) to the shoulder/upper torso. Furthermore, Zavala et al accounted for knee-spanning muscle co-contractions. The combination of additional mass and co-contractions would lead to significantly greater PFJRF compared with other studies we have included. Another example is the study by van Rossum and colleagues,84 their results were much lower than Zavala study but comparable to other studies, and we could attribute the differences to more sophisticated modelling methods that included a tibiofemoral joint and a patella with a deformable contact surface geometry. Also, the participants undertook squats to 90° knee flexion—PFJRF would be smaller at 90° knee flexion compared with maximum squats or deep squats. Furthermore, each participant was required to squat to a ‘self-perceived’ 90° knee flexion, so there could be considerable variation. Whyte et al 89 reported the lowest peak PFJRF during squatting compared with other studies included. The reason is unclear—perhaps the simple model approach used may not adequately estimate quadriceps force for shallow squats.
Does PFJRF differ between healthy individuals and those with patellofemoral pain or OA?
The weighted average means of PFJRF indicate that peak PFJRF may not be elevated in individuals with patellofemoral pain during walking, running and stair ambulation. Results from the few available cross-sectional studies directly comparing individuals with patellofemoral pain and healthy individuals indicated lower peak PFJRF in individuals with patellofemoral pain during walking and stair ambulation, with inconsistent results from two studies for running. The results of the cross-sectional studies were broadly consistent, although more studies are required. Some studies also reported PFJRF in individuals with patellofemoral pain during other activities and therapeutic exercises (eg, hopping, squat, gait retraining for cadence) and physical interventions (eg, brace, tape, orthotics). There were only single cross-sectional studies available reporting PFJRF in individuals with patellofemoral articular cartilage or OA relative to healthy individuals. The results indicated no differences in peak PFJRF between individuals with patellofemoral articular cartilage during walking, and no differences in peak PFJRF during stair ascent, but lower peak PFJRF during stair descent in individuals with patellofemoral OA when compared with healthy individuals. Due to the paucity of studies, this review cannot provide insight into the PFJRF in individuals with patellofemoral OA during therapeutic exercises and physical interventions. We encourage readers to keep the following in mind when interpreting these findings: (i) comparisons of peak PFJRF between healthy individuals and individuals with patellofemoral pathology during everyday activities are based on weighted average mean observations, and not statistical comparisons, and (ii) although the results of cross-sectional studies directly comparing healthy individuals and individuals with patellofemoral pathology indicate no differences or lower PFJRF in individuals with patellofemoral pathology, these results are based on one or two studies.
A dominant biomechanical theory is that elevated average patellofemoral joint contact pressure, which is influenced by both reaction forces and contact area, may contribute to degenerative changes in articular cartilage.96 If, as our analysis indicates, peak PFJRF is similar in individuals with patellofemoral pain, then elevated patellofemoral joint contact pressure may instead be driven by smaller patellofemoral joint contact areas. This effect could be caused by altered frontal plane alignment, movement patterns, and muscular coordination that have been observed in individuals with patellofemoral pain/OA, such as greater patellofemoral malalignment (this can reduce the patellofemoral joint contact area and thus increase the patellofemoral joint pressure),97 98 reduced knee flexion excursion, and quadriceps force deficits due to muscle weakness.99–103 It is also likely that altered movement patterns that lead to a lower PFJRF might be a strategy (conscious or unconscious) to reduce pain,104 105 or due to fear of movement.106
A concurrent theory proposes that not just the magnitude of joint loading, but also changes in the location of the applied loading may contribute to altered joint mechanobiology.107 Altered kinematics associated with patellofemoral pain may shift the locations of centres of contact pressure within the patellofemoral joint. This may lead to abnormally elevated contact pressures in regions of cartilage that are not accustomed to high pressures, and diminished pressures in regions that are accustomed to higher pressures. Both may trigger adverse changes in articular cartilage and contribute to the development and progression of patellofemoral OA. A contrary theory is that lower PFJRF in individuals with pain and/or OA might contribute to the progression of early OA changes in the knee. Following ACL reconstruction, lower peak PFJRF during running and hopping are evident108 109 and theorised to be related to post-traumatic OA progression. Similarly, lower tibiofemoral joint forces were associated with tibiofemoral OA development in a study of 22 individuals following ACL reconstruction.110 While the factors associated with OA development and progression following knee trauma and ACL reconstruction will be different, and more complex than those for patellofemoral pain/OA, it is possible that sustained ‘underloading’ during everyday activities may be detrimental to joint health. Further longitudinal studies are required to explore this theory.
Clinical and research implications
This is the first study to synthesise the evidence on PFJRF during various everyday activities, therapeutic exercises and physical interventions in healthy individuals, individuals with patellofemoral pain, and OA.
This information could be useful for clinicians when selecting and prescribing therapeutic exercises and physical interventions based on the magnitude of PFJRF to offload and/or progressively load the patellofemoral joint. Although the area of contact gradually increases as the knee is flexed to offset higher PFJRF, the information presented in this review can be used to select appropriate variations of exercises—that is, exercises that result in lower PFJRF than others at the same knee flexion angle (eg, forward vs side lunge)—gait retraining (eg, trunk position) and physical interventions (eg, shoes, orthotics). Individuals with patellofemoral pain and patellofemoral OA have a higher body mass index compared with healthy individuals.111 We reported the PFJRF values normalised to BW, where possible. This information can be easily understood by patients and may be used to highlight that body mass does matter when it comes to the patellofemoral joint, and excess BW can expose the patellofemoral joint to harmful loads.
Our systematic review also has important research implications. It is evident from this systematic review that there is a paucity of studies investigating PFJRF during everyday activities, therapeutic exercises and physical interventions in individuals with patellofemoral OA. Further, we require larger studies with more consistent methods and longitudinal data to understand the role of PFJRF in the development and progression of patellofemoral pain and OA. Further to this, studies included in this review, in general, indicated a high risk of bias for external and internal validity. Previous investigations have reported that biomechanics data can be reliably collected across multiple gait analysis laboratories.112 113 Therefore, high methodological quality studies with more consistent methods can offer opportunities to combine data across multiple gait analysis laboratories to overcome the small sample size limitations of independent studies.
Limitations
Several limitations should be acknowledged. We did not include studies in languages other than English. Our decision to only include English language studies was due to limited resources available to translate. We also did not evaluate the evidence on patellofemoral joint contact pressure in this systematic review. This was because patellofemoral joint contact pressure data are often not comparable due to large variability in methods and models used.19 Sample sizes were generally small in the included studies (most studies had fewer than 30 participants). Further, it was not possible to formally evaluate publication bias as fewer than 10 studies were available for most everyday activities, exercises and physical interventions. We also did not conduct certainty assessment, as mostly single studies were available reporting PFJRF in individuals with patellofemoral pain/OA compared with healthy individuals. In addition, we excluded data from unpublished or grey literature, and this may have influenced the results. However, evidence from a systematic review shows that this is only the case in a minority of reviews.114 Another point to consider is that most approaches to calculating PFJRF used source data from cadaveric studies of healthy individuals115 to inform the calculation of necessary intermediate variables, such as the effective moment arm of the quadriceps about the knee in planar models using best-fit functions, or Hill-type muscle properties in three-dimensional musculoskeletal models, for example. Thus, two additional limitations should be considered when interpreting PFJRF values for healthy individuals and those with patellofemoral pathology during dynamic tasks: (i) anatomical, physiological and biomechanical data from cadavers may not best represent those of living people; and (ii) such data from healthy individuals may not best represent the anatomical, physiological and biomechanical characteristics of those with patellofemoral pathology. Thus, this limitation should be considered when interpreting PFJRF values for healthy individuals and those with patellofemoral pathology during dynamic tasks. Further to this, the pooled PFJRF data for healthy individuals and those with patellofemoral pain/OA are mostly from studies that did not compare the two groups directly. Additionally, we synthesised data from the selected studies as-is and did not distinguish the reported PFJRF based on the methodological approach, including whether the magnitude of the PFJRF was derived from a two-dimensional or three-dimensional model of the knee. While this was a necessary compromise to enable the synthesis of limited available reported data, most selected studies (87%) used a two-dimensional planar knee model to estimate PFJRF from quadriceps forces. A separate, in-depth review of methodological approaches towards the calculation of PFJRF would be necessary to evaluate modelling differences in the calculation of PFJRF. Finally, the differences in gait speed may explain the differences in PFJRF between healthy individuals and those with patellofemoral pain/OA. Lower limb walking gait variables are sensitive to change with alterations in walking speed.116 Traditionally, biomechanical research studies have used one of three methodological approaches when it comes to walking speed: allowing participants to walk at their natural self-selected speed; walking at a prescribed speed, or statistically accounting for potential differences in walking speed.117 Much debate continues regarding the selection of the appropriate approach and the subsequent interpretation of conclusions, as no approach overcomes all possible limitations. It is possible that the differences we observed in PFJRF between healthy individuals and those with patellofemoral pain/OA may be due to differences in gait speed. However, as walking speed may be associated with pain or disease severity,117 118 the differences in walking speed may be the consequence of patellofemoral pathology. Therefore, we did not account for the differences in gait speed in the weighted average of means.
Conclusions
Everyday activities and therapeutic exercises involving higher knee flexion (eg, squatting) expose the patellofemoral joint to higher PFJRF than those involving smaller knee flexion (eg, level walking)—however, in normally aligned patellofemoral joint the contact area increases as the knee flexes, thus the differences in the patellofemoral joint contact pressure between activities may be smaller. This systematic review indicates that individuals with patellofemoral pain do not appear to have elevated peak PFJRF during everyday activities; however, a lower PFJRF applied to a smaller patellofemoral joint contact area can still produce a higher patellofemoral joint pressure. In this systematic review, we summarised the evidence on PFJRF during a range of activities and therapeutic exercises with/without physical interventions, and this can serve as a valuable resource for clinicians.
What is already known?
A dominant biomechanical theory is that higher patellofemoral joint reaction force (PFJRF), which might result in a larger patellofemoral joint pressure, may contribute to the development and progression of patellofemoral pain and/or osteoarthritis.
Evidence on PFJRF in healthy individuals and those with patellofemoral pain/osteoarthritis during everyday activities, therapeutic exercises and physical interventions has not been synthesised.
What are the new findings?
Peak PFJRF does not appear to be elevated in individuals with patellofemoral pain or patellofemoral osteoarthritis compared with healthy individuals.
Everyday activities and therapeutic exercises involving larger knee flexion expose the patellofemoral joint to greater peak PFJRF.
This knowledge might guide clinicians in selecting and prescribing therapeutic exercises and physical interventions for those with patellofemoral pain and/or osteoarthritis.
Larger studies with more consistent methods and longitudinal data are required to understand the role of PFJRF in the development and progression of patellofemoral pain/osteoarthritis.
Ethics statements
Patient consent for publication
Ethics approval
This study does not involve human participants.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @harvihart, @Knee_Howells, @mattgmking1
Contributors All authors contributed to the conception and design of the study, data analyses and interpretation, and drafting or revising of the manuscript.
Funding HFH is supported by a Canadian Institutes of Health Research Fellowship. AGC is a recipient of a National Health and Medical Research Council Early Career Fellowship (Neil Hamilton Fairley Clinical Fellowship, APP1121173).
Disclaimer The funders had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.