Article Text

Abstract
Objective The efficacious Activate injury prevention exercise programme has been shown to prevent injuries in English schoolboy rugby union. There is now a need to assess the implementation and effectiveness of Activate in the applie setting.
Methods This quasi-experimental study used a 24-hour time-loss injury definition to calculate incidence (/1000 hours) and burden (days lost/1000 hours) for individuals whose teams adopted Activate (used Activate during season) versus non-adopters. The dose-response relationship of varying levels of Activate adherence (median Activate sessions per week) was also assessed. Player-level rugby exposure, sessional Activate adoption and injury reports were recorded by school gatekeepers. Rate ratios (RR), adjusted by cluster (team), were calculated using backwards stepwise Poisson regression to compare rates between adoption and adherence groups.
Results Individuals in teams adopting Activate had a 23% lower match injury incidence (RR 0.77, 95% CI 0.55 to 1.07), 59% lower training injury incidence (RR 0.41, 95% CI 0.17 to 0.97) and 26% lower match injury burden (95% CI 0.46 to 1.20) than individuals on non-adopting teams. Individuals with high Activate adherence (≥3 sessions per week) had a 67% lower training injury incidence (RR 0.33, 95% CI 0.12 to 0.91) and a 32% lower match injury incidence (RR 0.68, 95% CI 0.50 to 0.92) than individuals with low adherence (<1 session per week). While 65% of teams adopted Activate during the season, only one team used Activate three times per week, using whole phases and programme progressions.
Conclusion Activate is effective at preventing injury in English schoolboy rugby. Attention should focus on factors influencing programme uptake and implementation, ensuring Activate can have maximal benefit.
- Rugby
- Athletic Injuries
- Preventive Medicine
- Adolescent
Data availability statement
No data are available. All publicly available data are available in the manuscript or online supplemental files. It is not possible to share further information, individual injury and exposure data, due to its confidential nature and the age of the participants.
Statistics from Altmetric.com
Introduction
Rugby Union (henceforth rugby) is a contact sport played in English schools by over 500 000 young people weekly.1 Rugby has come under scrutiny at all levels of the game due to the reported injury risk2–4 and the consequences such injuries may have on player health.5 6 The Rugby Football Union (RFU; governing body for English Rugby Union) has been promoting the Activate injury prevention exercise programme to reduce injury risk in youth rugby. Activate is a 15–20 min warm-up programme, designed to be completed prior to training and matches, with progressive, age-specific programmes.7
Activate efficacy was assessed in a 2015 randomised controlled trial of 31 independent schools (83 teams across under-15/16/18 age groups) in England over a 4-month season.7 Intention-to-treat analysis found an unclear effect of using Activate on overall match injury incidence (rate ratio (RR)=0.85) but lower upper-limb injury (RR=0.66) and concussion (RR=0.71) incidence. Per-protocol analyses (≥3 times per week) found teams using Activate had 72% fewer overall match injuries (RR=0.28), 72% fewer contact injuries (RR=0.28), and 59% fewer concussions (RR=0.41) compared with teams in the control group.7 However, only 16% of teams managed to complete Activate thrice weekly. This is concerning, as adherence rates in applied settings are likely to be lower given the contextual barriers in successfully implementing sports injury prevention programmes.8 This may partly explain why injury rates have not dramatically reduced in various sports settings despite considerable efforts in the injury prevention field to make sport safer.9 10
Neuromuscular training programmes appear to have a dose–response relationship with injury rates, with three sessions per week providing the greatest preventative effect.11 This evidence is supported by findings of the Activate efficacy study, where teams with high compliance (≥3 times per week) had significantly lower match injury incidence vs those with low compliance (0–2 times per week; RR=0.61).7 There is evidence that neuromuscular training programmes provide a preventative effect when completed once or twice per week.11 12 In the Activate efficacy trial, teams with these levels of compliance were clustered with those with zero compliance, and the preventative effect of one-two sessions per week was not assessed.7 A recent survey of English schoolboy rugby coaches reported that adopting teams used Activate twice per week.13 Therefore, evaluating the effect of varying levels of weekly dosage would empower end-users to make an informed decision regarding their Activate adherence.
The primary objective of this study was to assess the effectiveness of Activate to lower match and training injury rates (incidence and burden) in schoolboy rugby union (under-12 to under-19). The secondary objective was to examine the dose–response relationship between weekly Activate adherence and injury incidence.
Methods
Recruitment and participants
Schoolboy rugby teams (under 12 to under 19) were invited to join the study through an email sent to their Head Coach or Director of Rugby/Sport in June–August 2019. School names were taken from the RFU competitions website, with contact email addresses sought online.
Participants, players from school teams who had agreed to participate in the project, completed an electronic assent form (http://www.onlinesurveys.ac.uk), with parental consent for those under the age of 18 years old.
Activate
Activate is a warm-up exercise programme designed to be used three times per week prior to rugby training and matches. There are three age-specific programmes (under-15/16/18) incorporating balance, resistance and plyometric exercises, each containing four phases to be progressed throughout the season (every 4–8 weeks).14 Activate was disseminated by the RFU in 2017 following the publication of the efficacy study.7 Coaches could access resources freely through the RFU website and attend regional workshops delivered by RFU community rugby coaches, who received specific Activate training.15 In 2018, all resources became available open access and workshops were replaced by a ‘workshop on demand’ system. These implementation and dissemination strategies, including the workshops, were conducted by the RFU external to this study.
Data collection
Gatekeepers (generally the head coach) were provided with a bespoke excel worksheet to collect their teams’ rugby attendance, rugby exposure (minutes), injury data and Activate use throughout the season (July–September 2019 to December 2019–April 2020 depending on school and competitions). Operationalised definitions are presented in table 1.
Operationalised study definitions
Player-level data were collected, allowing direct analysis between individual exposure and injury risk.16 Team training duration for each session was matched with session attendance registers, where gatekeepers recorded which players participated in each session, to record player training exposure. Individual match exposure was calculated by dividing overall player minutes (players on the pitch x match duration) and divided by the number of players marked as present.
Activate adoption was self-reported by the gatekeeper for every training session and match (dichotomous: ‘yes/no’). Adopting teams recorded which exercises were used for each session, with no minimum threshold to determine whether a team used the programme. No information regarding exercise parameters (sets and reps) or exercise fidelity (performing exercises competently) was recorded. Median weekly Activate adherence was calculated by cross-referencing attendance registers and the team’s Activate use for that session. Participants were not instructed whether to use Activate. Instead, this type 1 effectiveness-implementation study17 observed end-users voluntarily using Activate (ie, no implementation strategy was involved in the study). No training was provided to participants outside of the RFU resources available to all coaches nationwide.
The injury report form detailed: player name, injury date, return to full participation (deemed so by the gatekeeper), training/match, mechanism, body location, injury type. Specific injury diagnoses were not recorded except for suspected concussions where, as per RFU policy,18 any player suspected of sustaining a concussion must be removed from play and stood down for a minimum time prior to returning to play after clearance by a medical professional. Prepopulated categories for injury mechanism, location and type, were used on the worksheet to ensure consistency of data collection.19
Missing attendance registers were imputed using a last observation carried forward method (408 missing registers/25 318 exposures=2%).20 No individuals had more than 10% of their attendance registers missing and thus all records were retained for analysis. Exposure for injured individuals participating in training prior to their recorded return to play date were not included in the analysis until after they were cleared to return. This was to create consistency as those injured might be training but were likely imposed with training restrictions prior to returning to play. If an individual was injured but the severity was unknown (due to the season ending (n=19) or missing data (n=1)) they were not included in any subsequent analysis after the injury date. Sessions missed due to injury were not included when calculating adherence.
Analysis
Analysis was completed using Microsoft Excel (V.16.0) and Stata (V.16.0). For the primary research question, individuals were grouped by their team’s Activate adoption or non-adoption. For the secondary research question, individuals were grouped by their median weekly Activate adherence throughout the season (low= <1 session per week, medium= 1 to <3 sessions, high=≥3 sessions). The low adherence group included all individuals from teams in the non-adoption group with zero Activate adherence, plus those from the adoption group with low adherence.
Injury incidence (injuries/1000 player-hours) and injury burden (days lost/1000 player-hours), presented with 95% CIs, were estimated for each group using backwards stepwise Poisson regression, adjusted for cluster (team). Predictor variables included Activate adoption/adherence and playing age group. Incidence and burden RRs were calculated using the same method, with the non-adoption group the referent for the primary research question and the group with lower adherence the referent for the secondary research question. Statistical significance was set at p<0.05.
Sample size
A sample size calculation was performed for the primary research question, using a significance level of 0.05 and power of 80%.21 Injury incidence (34.3/1000 hours), mean cluster (team) size (n=24 players) and individual rugby exposure (9 hours) were based on previous data collected from the same playing cohort.22 A 40% lower injury incidence was estimated from a meta-analysis investigating neuromuscular training programmes and injury risk.11 As such, the number of teams required per arm was 14. Anticipating each school would have two teams, the study required nine schools per arm. Using a conservative estimated drop-out rate of 60%, 22 schools were needed.
Results
In total, 289 schools were emailed to join the study (figure 1). Fifty-seven schools agreed to participate, with 15 dropping out during the data collection phase and a further 22 schools not providing data at the end of the season (likely due to COVID-19). Data were received from 20 schools (41 teams), with 7 schools (16 teams) subsequently excluded due to providing incomplete datasets, predominately a failure to record individual exposure (online supplemental file 1). Consequently, 13 schools (25 teams, 659 players) were included in the study.
Supplemental material

Flow diagram highlighting the recruitment process, study participation and the impact of COVID-19 on retention.
COVID-19
The school rugby season was affected by COVID-19 in March 2020, when the season was abruptly terminated due to a lockdown. Most schools that finished playing in December 2019 had already provided their datasets; however, after this point many gatekeepers were unreachable and did not provide data, being classified as study drop-outs.
Activate implementation
Of the 25 teams included in the study, 16 adopted Activate during the season. Of these 16 teams, 2 did not record which exercises they used for each session and are excluded from this implementation section. Cumulative utilisation was 98%, with thirteen teams using Activate at all sessions and one team using Activate at 70% of sessions. Adopting teams had a mean utilisation frequency of 3.2 Activate sessions per week (range 2.1–4.0) and a utilisation fidelity of 9.8 Activate exercises per session (range 4–15). Only four teams used Activate phases in their entirety, with the remaining using exercises from various phases. Half of the teams progressed the programme throughout the season, but only two used exercises from phases 3 or 4. Only one team implemented Activate three times per week, using each phase in its entirety, while progressing the phases throughout the season.
Activate adoption
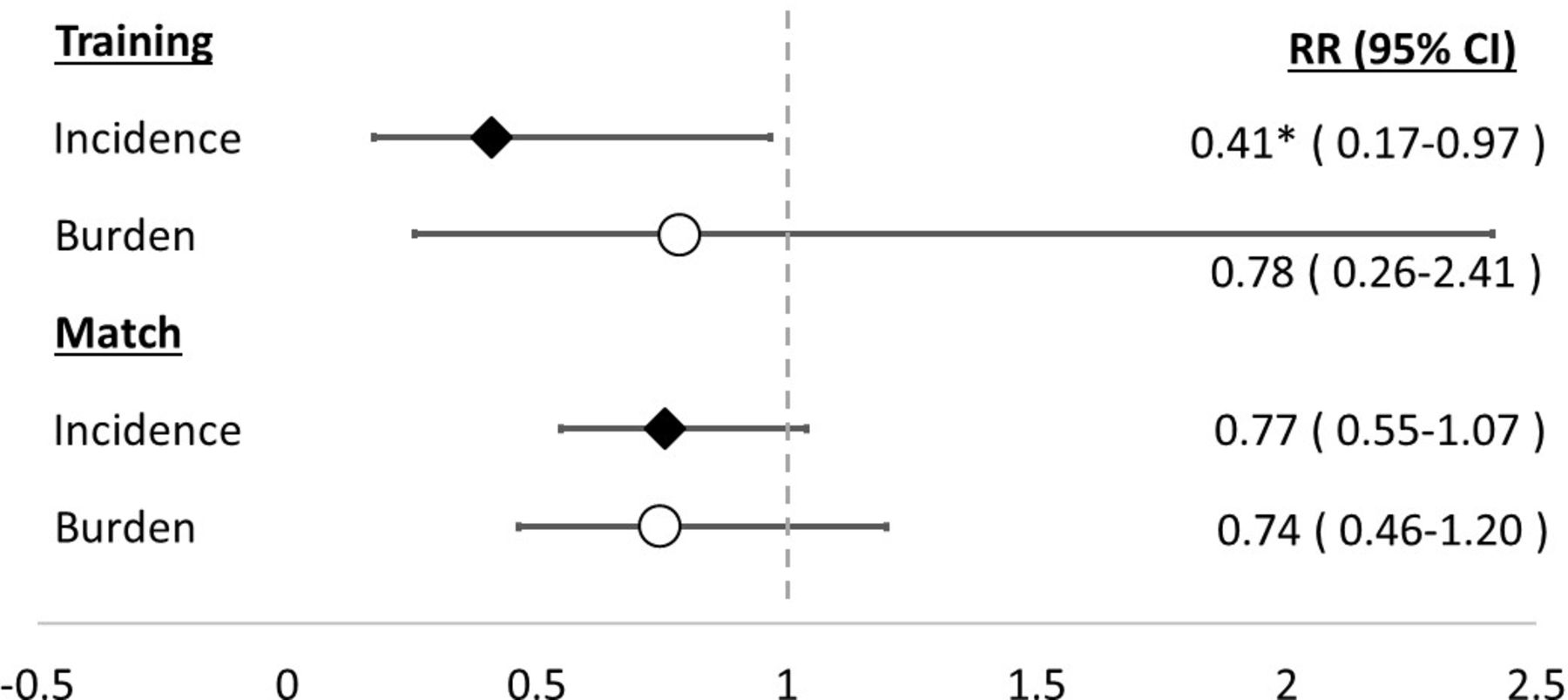
Individuals from teams adopting Activate (n=16) amassed 16 853 player-hours, sustaining 84 injuries (table 2). Individuals from non-adopting teams (n=9) recorded 7828 player-hours and 58 injuries. Individuals in teams adopting Activate had a 23% lower match injury incidence (figure 2) and 59% lower training injury incidence compared with non-adopting teams (p<0.05). Match injury burden was 26% lower in the adopting group. Descriptive information relating to injury types and mechanisms is presented in online supplemental file 2.
Supplemental material
Descriptive statistics by Activate adoption

Incidence and burden rate ratios (RRs) (adjusted for playing age group and cluster (team)) by Activate adoption group. RR<1 favours the adoption group. *p<0.05.
Activate adherence
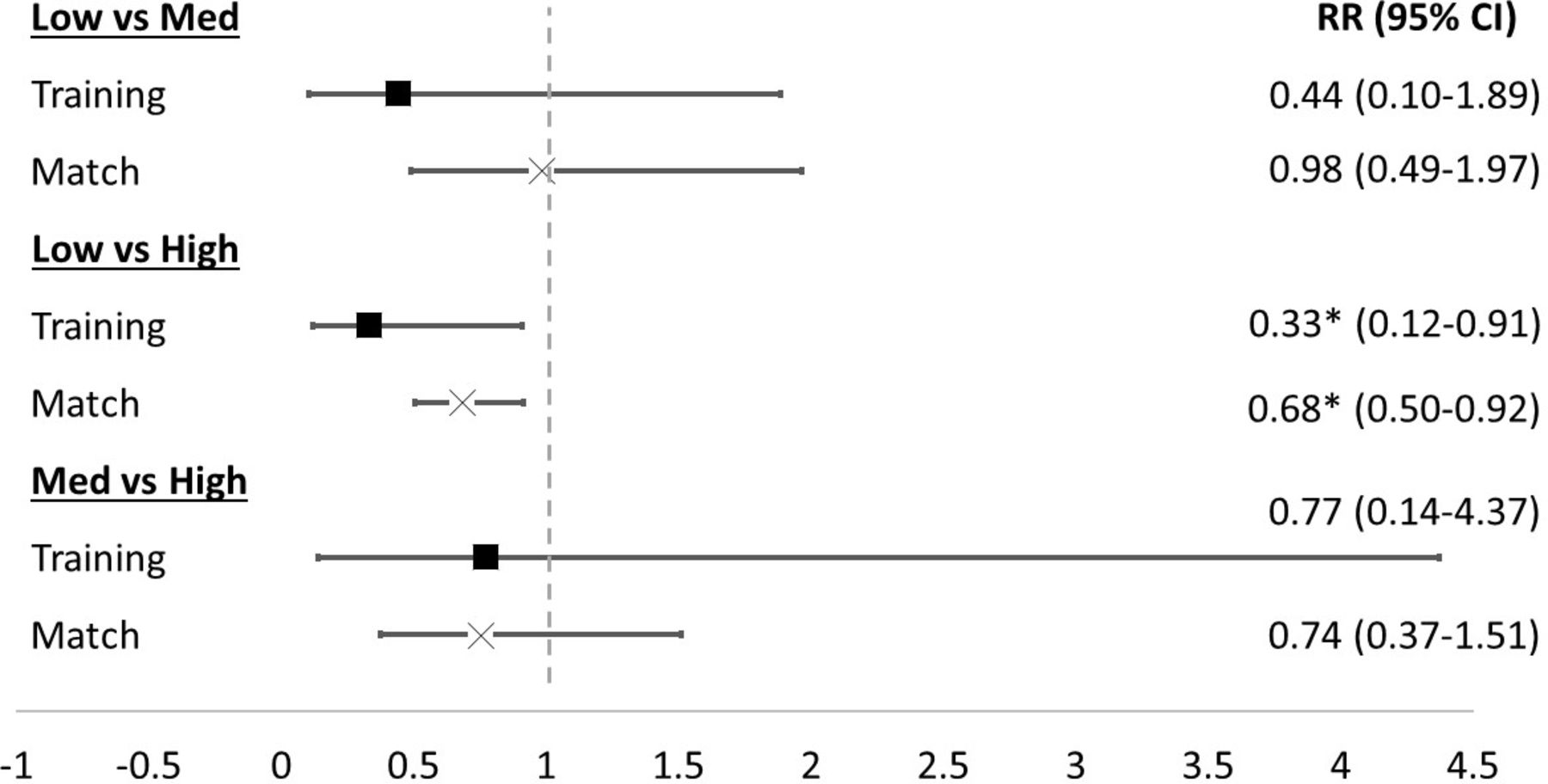
Individuals with high Activate adherence (≥3 sessions per week) had a 67% lower training injury incidence (p<0.05; figure 3) and 32% lower match injury incidence (p<0.05) than individuals with low adherence (<1 session per week). Descriptive statistics by adherence groups is presented in table 3.
Descriptive statistics by median Weekly Activate adherence group

{kind=link}
{kind=link}
{kind=link}
Training and match incidence rate ratios (RRs) (adjusted for playing age group and cluster (team)) per Activate adherence level. RR<1 favours the group with greater adherence. *p<0.05
Discussion
This is the first study to investigate the effectiveness of the Activate injury prevention exercise programme to prevent injuries in schoolboy rugby union. Individuals playing for teams adopting Activate had a lower match and training injury incidence when compared with those not using Activate. Individuals with high weekly Activate adherence (≥3 Activate sessions per week) had a lower match and training injury incidence than those with low adherence (<1 Activate session per week). Activate appears effective at lowering injury risk in schoolboy rugby union, with maximum benefit when completing the programme three times per week.
Activate implementation
Two-thirds of teams adopted Activate during the season, which is positive as more established sports injury prevention programmes have been hampered by poor programme uptake.23–25 Adopting teams reported high cumulative utilisation (adopting Activate at 98% of sessions) and utilisation frequency (mean 3.2 Activate sessions per week). This level of implementation is surprising, as coaches from a similar cohort reporting only using Activate twice per week.13 Utilisation fidelity varied (mean 9.8 exercises per session), with some teams only using four exercises per session and only two teams using whole phases. Most teams modified the programme content, which is commonplace in the sports injury prevention literature.26–28 Modifications to the programme and its delivery may be necessary to ensure Activate can be successfully used in a school context, where time, expertise and facilities are known barriers to implementation.13 29 30 However, the extent to which programmes can be modified before losing their preventative effect is unknown and an area for future research.
Activate adoption
Significantly different training injury incidence was found when comparing individuals by their team’s Activate adoption. Furthermore, the RR point estimates for match incidence and burden are clinically relevant, advocating Activate use in the applied setting. There is strong evidence that neuromuscular training programmes provide preventative effects in a variety of youth sports,11 31 including rugby.7 32 However, programmes are often evaluated in randomised controlled trials33 and this study is one of the first studies to assess the effectiveness of a neuromuscular training programme after efficacy has been established. This is important, as efficacious intervention are not guaranteed to be effective in an applied environment, due to contextual barriers which are not present in controlled studies.8 While there is a need to assess Activate effectiveness in other populations, especially as the programme has been disseminated worldwide, focus on English schoolboy rugby should be on improving Activate implementation to ensure the programme can provide maximum benefit nationwide.
Activate adherence
Individuals adopting Activate had a median weekly adherence of three sessions per week, which is an improvement over the 16% of teams in the original efficacy study that managed to maintain this level of exposure.7 The results confirm a dose–response relationship between adherence and injury incidence, with significantly lower training and match injury incidence found in the high adherence group compared with the low adherence group. This is consistent with a meta-analysis of neuromuscular training programmes that showed maximum benefit is achieved with three sessions per week (RR 0.40, 95% CI 0.31 to 0.53), and smaller preventative effects when completed twice per week (RR 0.50, 95% CI 0.29 to 0.86).11 Using Activate thrice weekly is strongly advocated to have maximum effect, but if that cannot be achieved, end-users are encouraged to use Activate once to twice per week to reduce injury risk. Completing Activate outside of a rugby environment and away from the pitch may increase Activate exposure. A recent study investigating the 11+ found removing strengthening exercises from the warm-up and using them postsession improved adherence without negating preventative effects.34 A similar approach for Activate would reduce the time needed to complete a warm-up, overcoming a commonly reported barrier from rugby coaches.13 However, if exercises have an acute preactivation effect, they may need to be completed immediately prior to rugby exposure. The mechanistic effect of Activate has not been evaluated and this should be investigated prior to advocating this approach.
Limitations
To mitigate selection bias, the extensive recruitment database included all schools playing in RFU competitions and others for which contact details could be found. In an attempt to improve the representativeness of the study, in comparison to the efficacy study,7 which only included under-15 to 18-year-old independent schoolboy rugby teams, government funded state schools were invited and the age range was increased (under-12 to under-19). Despite more state schools than independent schools being invited, a larger number of the latter participated in the study, likely reflective of being better resourced to dedicate time to the study and record the required information. This limits the generalisability of these results in this context. Furthermore, it is unclear whether these results are generalisable to a schoolgirl rugby population, where the aetiology and pathology of injury is largely unknown but likely different from schoolboy rugby players.
The number of schools recruited in preseason (n=57) exceeded the required amount based on the sample size calculation (n=44). This study was a substudy of a longitudinal injury surveillance project,22 which used team-level exposure, and 15 teams were excluded as they did not record individual-level exposure required for this study. The season ended abruptly in March 2020 due to COVID-19 and 22 participating schools were unreachable after this point. The study is, therefore, likely underpowered and there is a risk of type II error when comparing results between groups.
Activate adoption and adherence was self-reported by gatekeepers. This information was not verified as it was not permitted to attend school sites to observe sessions. To mitigate reporting bias, Activate was not used in any recruitment correspondence and the aims of the study were not advertised to participants, instead focusing on the injury surveillance aim of the wider project. However, reporting bias and recall bias might explain the higher than anticipated levels of adherence and cumulative utilisation in comparison to similar studies.13 26
Warm-up strategies employed by non-adopting teams was not investigated as it was not deemed feasible to ask coaches to record their individual warm-up strategies. School rugby coaches have demonstrated knowledge that a rugby-specific warm-up, and certain components such as balance and strength, can lower rugby injury risk.13 35 If non-adopting coaches possess this knowledge and used similar exercises to those contained within the Activate programme, it may have diminished any difference between the groups.
Various confounders may influence an individual’s injury risk, including previous injury, playing position, playing experience and physical characteristics.36 A preseason survey was developed to capture this information to allow the results to be adjusted for covariates. Unfortunately, the age of the participants meant it was not possible to contact them directly and surveys were sent to their gatekeepers to pass on. The response level was inadequate, and the limited returned information was insufficient for analysis. In this population, playing age group is likely related to many of these confounders. For example, older players will likely have a greater playing experience, injury history, and have more mature physical attributes in comparison to younger players. Playing age group was accounted for, partially mitigating the omission of these collinear variables, but their independent effects could not be assessed. Training load may also be a confounder for injury risk, although this has not previously been explored in a youth rugby population. In this study, those adopting Activate had a greater training exposure than non-adopters. It is unclear whether this is due to fewer injuries resulting in greater training exposure, or possibly greater training exposure resulting in a protective effect for injury.
Conclusion
Individuals adopting Activate had a significantly lower training injury incidence than non-adopters, with point estimates suggesting lower match incidence and burden. Participants completing Activate three times per week had significantly lower training and match incidence compared with those with low (<1 session) weekly adherence. Two-thirds of teams adopted Activate, with most completing Activate three times per week. However, Activate was often not implemented as intended, with teams not using whole phases or failing to progress the programme. Engaging end-users to explore barriers to Activate use is integral to understanding how implementation can be maximised and schoolboy rugby made safer.
Key messages
What is already known?
A randomised controlled trial found Activate to be efficacious in reducing injury risk in schoolboy rugby union.
What this study adds?
Activate is effective at lowering youth rugby injury risk in the applied setting.
Individuals with high Activate adherence (3+times per week) had significantly lower training and match injury incidence than those with low adherence (<1 time per week).
How might this research affect research, practice or policy?
Providing knowledge of Activate effectiveness can be used to promote greater adoption and adherence among end-users.
Establishing Activate effectiveness means research should now focus on maximising implementation.
Data availability statement
No data are available. All publicly available data are available in the manuscript or online supplemental files. It is not possible to share further information, individual injury and exposure data, due to its confidential nature and the age of the participants.
Ethics statements
Patient consent for publication
Ethics approval
The study had ethical approval from the Research Ethics Approval Committee for Health at the University of Bath (EP 17/18 167).
Acknowledgments
The authors would like to thank all the schools, coaches and players who participated in this study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @cigney, @drkeithstokes, @drsimonroberts, @Dr_CMcKay
Contributors CB, CDM and KAS devised the initial concept of the study, with MVH and SPR providing advice and guidance. CB and MVH completed all the data collection and data cleaning. CB analysed all the data. CB wrote all manuscript drafts, with critical appraisal from CDM and KAS. All authors approved the final version of the manuscript ready for submission. CB is listed as the guarantor for the study.
Funding CB completed this study as part of his PhD, which is funded by the Rugby Football Union.
Competing interests KAS is the medical research lead for the Rugby Football Union.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.