Article Text

Abstract
Objective To investigate the effectiveness of videoconferencing exercise interventions for people with chronic diseases.
Design Systematic review incorporating meta-analysis.
Data sources PubMed, Cinahl, MEDLINE, Web of Science, Embase and Scopus.
Eligibility criteria The current literature was searched following Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines. Trials analysing participants with chronic disease undergoing aerobic and/or resistance exercise training over videoconferencing, with exercise capacity and/or quality of life outcomes were included. Meta-analyses were conducted for between-group comparisons of exercise capacity and quality of life. Risk of bias was analysed using the Downs and Black quality checklist and the certainty of evidence with Grading of Recommendations, Assessment, Development and Evaluation (GRADE).
Results Thirty-two trials were included in this review, of which 12 were comparator trials. Small–moderate between-group (videoconferencing vs comparator) effects favouring videoconferencing were seen for studies using a non-exercising comparator for exercise capacity (standardised mean difference (SMD)=0.616, 95% CI 0.278 to 0.954; p=<0.001) and quality of life (SMD=0.400, 95% CI 0.099 to 0.701; p=0.009). Small effects favouring videoconferencing were observed for studies using an exercising comparator for quality of life (SMD=0.271, 95% CI 0.028 to 0.515; p=0.029) and exercise capacity (SMD=0.242, 95% CI 0.059 to 0.426; p=0.009). Moderate risk of bias was identified for included studies (16.3±3.6/28), with GRADE certainty ratings of ‘low’ (quality of life) and ‘moderate’ (exercise capacity). Session attendance was 70% and was reported in 23 trials. No serious adverse events relating to videoconferencing were found. Nine trials documented the total number of technical issues that occurred in 17% of the sessions. Positive satisfaction outcomes were associated with ease of access and usefulness of technology.
Conclusion In patients with chronic disease, videoconferencing exercise interventions appear to be feasible and effective for improving exercise capacity and quality of life. More robust methodology is needed in future studies to improve the certainty of the evidence.
PROSPERO registration number CRD42020191243.
- exercise
- exercise training
- meta-analysis
- noncommunicable diseases
Statistics from Altmetric.com
Background
In 2016, an estimated 41 million people worldwide died of chronic disease.1 Physical inactivity is a known modifiable risk factor for several chronic diseases, regardless of age, sex, ethnicity or body mass index (BMI).2 Exercise interventions in several chronic disease groups have been associated with improved disease control.3 Advances in digital health technology are transforming the way in which health professionals manage patients. Furthermore, telehealth is a rapidly growing service delivery model for the management of chronic disease. The uptake of telehealth services has been especially significant in the wake of the global COVID-19 pandemic, which has challenged the concepts of healthcare delivery.4
Telehealth is described as the use of telecommunication techniques for the purpose of providing telemedicine, medical education and health education over a distance.5 A systematic review focusing on telemonitoring demonstrated improved glycaemic control and body mass in people with diabetes.6 Telemonitoring with synchronous (ie, real-time) feedback from clinicians resulted in further improvements to metabolic measures, compared with interventions that did not use this approach.6 Videoconferencing exercise interventions involve the synchronous delivery of exercise via a video-linked appointment. The effectiveness and feasibility of videoconferencing interventions remain ambiguous across various chronic disease groups.
Traditional forms of exercise in chronic disease include in-person hospital-based programmes, such as cardiac rehabilitation. These types of exercise programmes have been proven to be safe and effective, leading to decreased rates of mortality and hospital readmissions.7 8 Despite this, participation in these programmes is low, with less than 50% of eligible patients attending cardiac rehabilitation programmes worldwide.6 7 Logistical, personal, programme and healthcare system factors all influence patient adherence to these programmes.7 Although associated with improved health outcomes, in-person cardiac rehabilitation programmes are costly at the organisational level.9 Synchronous telehealth programmes, such as videoconferencing exercise interventions, may be a suitable alternate delivery method to address the limitations associated with traditional in-person training and better support patient preference.
Therefore, the primary aim of this systematic review was to determine the clinical effectiveness of videoconferencing exercise interventions in patients with chronic disease. This review also aimed to determine the feasibility of delivery for included trials. Effectiveness was assessed using a meta-analysis of changes in exercise capacity and quality of life. Feasibility was determined by investigating session attendance rates, adherence to exercise prescription during the session, safety, technical issues and participant satisfaction.
Methods
The methodology and results of this systematic review and meta-analysis are presented according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement.10 The review was registered under trial number CRD42020191243 through PROSPERO international prospective register of systematic reviews on 14 July 2020.
Terminology
Videoconferencing: the use of synchronous telecommunication in the form of a video-linked appointment.11 Videoconferencing exercise interventions involve a health professional supervising participants through an exercise session over a two-way audiovisual platform.
Exercise capacity: the maximum amount of physical exertion that a person can sustain.12 Exercise capacity tests are typically assessed either via distance travelled by the participant over a certain time frame, time-on-test for a graded treadmill test to exhaustion or peak power during a graded cycle ergometer test to exhaustion. Exercise capacity has been shown to be a predictor of all-cause mortality across a range of chronic conditions.13
Quality of life: a multidimensional construct, generally describing an individual’s self-perception of their quality of life.14 It is typically assessed through self or clinician administered questionnaires considering multiple different domains of an individual’s life (ie, physical, emotional and social). The term health-related quality of life is used to describe an individual’s self-perceived quality of life as it pertains to health-related issues.14
Search strategy
Searches were completed through six electronic databases from inception to 1 August 2021 by one reviewer (RB). The databases included were PubMed, Cinahl, MEDLINE, Web of Science, Embase and Scopus. Key search terms included ‘exercise’, ‘resistance training’, ‘strength training’, ‘physical activity’, ‘aerobic training’, ‘endurance training’, ‘exercise intervention’, ‘telerehabilitation’, ‘videoconferencing’, ‘telehealth’ and ‘telemedicine’. Recursive searching of reference lists for all identified papers was conducted. Only completed clinical trials were reviewed. Conference abstracts and dissertations were excluded. More information on the database search strategies is provided in online supplemental material 1. The selection process for included studies is in figure 1.
Supplemental material

Flowchart selection of studies (Preferred Reporting Items for Systematic Reviews and Meta-Analyses).
Eligibility criteria: participants, intervention, comparator, outcomes (PICO)
Participants
Included studies were not restricted by age or sex. Participants with chronic disease in accordance with the Australian Institute of Health and Well-being definition, ‘long lasting disease with persistent effects ranging from mild to severe’, were included.15
Intervention
Studies were included if they assessed an exercise intervention incorporating resistance and/or aerobic training delivered remotely via videoconferencing. Exercise sessions must have been conducted on a weekly basis for part of the intervention. Sessions must have been delivered via videoconferencing by an appropriately qualified healthcare professional. Studies were included into the meta-analysis if they presented mean (SD) preintervention and postintervention exercise capacity and/or quality of life scores, or if these data were obtained via author contact. Interventions of any length and any follow-up period were included for analysis. Interventions were excluded if studies were unclear about participant characteristics (ie, non-specific low back pain), rehabilitation following arthroplasty surgery, balance or neuromotor-focused exercise programming, electrical stimulation assistance trials, exergaming studies not employing an aerobic/resistance training approach or non-remote videoconferencing trials.
Comparator
Both comparator and single-arm studies were included. For comparator trials, both exercising and non-exercising comparator groups were included.
Outcomes
Studies were included if they reported changes in exercise capacity and/or quality of life. Quality of life data were included if they assessed more than one domain of life (eg, physical, mental and social). Quality of life questionnaires presenting multiple domain scores rather than total scores were averaged to include into the meta-analysis.16 For studies presenting multiple quality of life assessments, one was chosen for entry into the meta-analysis. Feasibility outcomes were session attendance rates, adherence to exercise prescription during the session, safety, technical issues and participant satisfaction.
Data extraction
Data describing participant and study characteristics, eligibility criteria, exercise intervention protocol and details of supplementary interventions were extracted by two independent reviewers (RB and KJR). Differences between the two reviewers were mediated through discussion with a third reviewer (SK). Where further information was needed, authors were contacted via email. All exercise capacity and quality of life data not included in manuscripts were obtained via author contact.
Study quality
Study quality was assessed by two independent researchers (RB and KJR) using the Downs and Black checklist.17 Differences between the two reviewers were mediated through discussion with a third reviewer (SK). Study reporting, external validity, internal validity (confounding and bias) and statistical power were assessed. Types of bias assessed include selection bias, confirmation bias, observation bias and confounding bias. Both comparator and single-arm studies were assessed. The checklist includes 27 criteria, with the highest possible score being 28. If a criterion was ambiguous or unable to be determined, it was scored as 0.
Confidence in cumulative estimates
The Grading of Recommendations, Assessment, Development and Evaluation (GRADE) was used to assess the certainty of evidence for exercise capacity and quality of life outcomes. GRADE analysis assesses risk of bias, indirectness, inconsistency, imprecision and other factors at the outcome level.18 Indirectness was assessed via analysis of the study population regarding the PICO statement. Inconsistency was determined via inspection of meta-analyses plots for overlap of CIs, difference and magnitude of point estimates. Heterogeneity was identified via the Q test and I2 statistic. Imprecision was assessed via analysis of summary effect CIs and statistical thresholds. Publication bias and assumptions for normality were determined via visual inspection of funnel plot analysis and Egger’s statistic. Skewness was assessed via mean/SD of scores, sensitivity analyses of post-trial outcome measures and visual inspection of funnel plots.19
Meta-analyses
Meta-analyses were completed using Comprehensive Meta-Analysis software V.3 (Biostat, Englewood, New Jersey, USA).20 Meta-analyses were conducted for the effects of the interventions on exercise capacity and quality of life. For these analyses, preintervention and postintervention means/SD and the sample size per group were used. Comparator trials compared the videoconferencing group with either an exercise group or a non-exercising group, while single-arm trials were analysed using their predata–postdata. A within-group Cohen’s d effect size (ES) was calculated to estimate change from baseline for each group. We assumed a conservative precorrelation–postcorrelation of 0.5 measured within each comparison group for the controlled trials.21
For our primary analyses, in comparator trials, a between-group meta-analysis for exercise capacity and quality of life was conducted. For the ES difference between groups, standardised mean differences (SMDs) from predata–postdata were used. This was due to the multiple forms of exercise capacity and quality of life tests between trials. Difference in means (MD) was used for single-arm exercise capacity measures, as only the 6 min Walk Test (6MWT) was administered in all single-arm studies. Prespecified levels of magnitude for SMD were set at 0.2 for small, 0.5 for moderate and 0.8 for large. The SMD and 95% CI were calculated using random effect meta-analysis with inverse of variance. Random effects meta-analysis allows for differences in the treatment effect to be present and accounted for throughout the included trials.22 23 Heterogeneity was assessed using the Q-test (statistical significance determined as p=0.1), and between-study variability was calculated by the I2 statistic. Values of 0%–25%, 26%–74% and ≥75% were considered to indicate low, moderate and high heterogeneity, respectively. Subgroup analysis was conducted for exercising/non-exercising comparator groups. To evaluate the robustness of our analyses, we conducted sensitivity analyses: (1) to assess the individual influence of each study by removing each study from the model once to see its effect on the overall results and (2) running precorrelation–postcorrelation at levels of 0.6, 0.7, 0.8 and 0.9 to assess influence on the overall result.
Results
Figure 1 shows 11 947 papers were identified, with 32 included in the qualitative synthesis, and 29 progressing to meta-analysis. Twelve studies were comparator trials, and 20 were single-arm trials. Three single-arm trials were excluded due to the required information not being received via author contact.24–26
Participant characteristics
Participant characteristics are displayed in table 1. A total of 1049 subjects participated across all studies (757 in comparator trials and 292 in single-arm trials). Mean age was 60±13 years and mean BMI was 26.7±3 kg/m2 (63±8 years and 30±2 kg/m2 for comparator trials, 58±15 years and 25.3±2.7 kg/m2 for single-arm trials). Overall, most trials (n=12, 38%) recruited participants with a pulmonary condition.27–38 Other chronic disease domains included cardiac diseases (n=5, 16%),39–43 metabolic disorders (n=3, 9%),44–46 neurological disorders (n=7, 22%),47–53 cancer (n=3, 9%)54–56 and musculoskeletal conditions (n=1, 3%).57 One trial recruited participants from multiple disease groups.58 The most common conditions were chronic obstructive pulmonary disease (COPD), chronic heart failure and stroke, accounting for 488 (48%) of participants across trials.
Design and participant characteristics
Intervention characteristics
Details of the videoconferencing exercise interventions are summarised in table 2. Six trials delivered resistance training45 47–49 52 56; 3 used aerobic training29 30 51; and 23 had a combination of both resistance and aerobic training.27 28 31–44 46 50 53–55 57 58 Eighteen trials used online software with monitoring29 34–37 39–41 46 47 50 51 53–58; 7 had installable systems paired with online monitoring30–32 38 43 44 52 and seven used unspecified systems to facilitate videoconferencing sessions.27 28 33 42 45 48 49 Group-based exercise sessions were delivered for 15 trials27–30 33 35 37 39 40 46 52–54 56 58; individual sessions were led for 1431 32 34 36 38 42–44 47 49–51 55 57; and in three trials, the delivery mode was not specified.41 45 48 Intervention duration ranged from 3 to 104 weeks, with 8 weeks being the most common (n=11, 35%). In the comparator trials, seven had an exercising comparator group (eg, in-person delivery of exercise),28 30 40 42 44 48 50 and four had a non-exercising comparator group.35 41 45 46 Three comparator trials followed a three-arm approach. One had two exercising comparator groups,48 and two had both exercising and non-exercising comparator groups.44 57
Details of videoconferencing exercise interventions
Outcome measures
Exercise capacity and quality of life data from the 12 comparator trials are provided in table 3 (see online supplemental material 2 for single-arm trials). Fourteen trials assessed both exercise capacity and quality of life28–31 33 35 36 40 41 43 44 46 55 58; 5 assessed exercise capacity35 41 45 47 56; and 13 assessed quality of life.27 32 34 37 38 48 49 51–54 57 The most common exercise capacity measure was the 6MWT (n=17). The most common quality of life questionnaire was the 36-Item Short Form Survey (SF-36) (n=6).
Exercise capacity and quality of life outcome measures (comparator trials) according to patient disease/condition
Exercise capacity
Between-group differences favouring videoconferencing (p<0.05) were reported in 5 of the 10 comparator trials for exercise capacity.30 35 41 44 45 For all trials, within-group improvements in the videoconferencing group (p<0.05) were observed for 12 out of 19 trials.28 30 31 35 41 42 44 45 50 55 56 58 Clinically meaningful differences in the 6MWT were found among single-arm trials.29 31 33 36 43 55 56 58
Quality of life
Between-group differences favouring videoconferencing (p<0.05) were reported in four of the nine comparator trials for quality of life.28 35 41 46 Quality of life significantly decreased in one non-exercising comparator group.35 For all trials, within-group improvements in the videoconferencing group (p<0.05) were observed in 10 out of 27 trials.27 28 30 32 35 37 41 46 52 58
Attendance
Attendance to exercise sessions was reported in 24 trials.27–30 32–35 39–42 44–47 50–53 55–57 Modalities of reporting attendance varied among trials, with the most common form being mean±SD of attended sessions (n=8, 26%). In trials providing mean±SD data, attendance to videoconferencing exercise interventions was 70%. No trials reported adherence to exercise prescription in session. See online supplemental material 3 for data on session attendance rates.
Safety
Adverse events as part of the intervention were reported in 75% (n=9) of the comparator trials and 45% (n=9) of single-arm trials. No serious adverse events related to any videoconferencing exercise intervention were reported. No comparator trials reported an increased number of exercise-related adverse events in the intervention group compared with either an exercising or non-exercising comparator group. See online supplemental material 3 for data on safety.
Technical issues
Nine trials (28%) reported the total number of technical issues in delivering videoconferencing, affecting 17% of total sessions.28–30 34 35 46 51 55 Common technical issues reported include disturbances to audiovisual connection and poor internet quality. See online supplemental material 3 for data on technical issues.
Participant satisfaction
Seventeen trials reported participant satisfaction post intervention.27 29 32 34 37 39 40 42 44 47 50–55 57 Both quantitative and qualitative assessments were taken, the most common being a qualitative interview (n=7). Generally positive outcomes were reported for satisfaction measures across trials, with participants citing ease of access and usefulness of technology as main drivers of satisfaction.27 32 34 37 44 47 50–52 54 55 57 See online supplemental material 3 for data on participant satisfaction.
Methodological quality and confidence in cumulative effect
The mean Downs and Black score was 16.3±3.6 (minimum=11, maximum=23) for all trials (18.6±4.1 in comparator, 14.9±2.4 in single-arm) out of a possible 28. Cumulatively, moderate risk of bias was seen in all trials, categorised by cut-off points used in previous studies.59 Assessor blinding was present in 67% (n=8/12) of comparator trials and 25% (n=5/20) of single-arm trials. Allocation concealment was conducted in 67% (n=8/12) of comparator trials. Certainty of effect was determined to be moderate for exercise capacity and low for quality of life via GRADE analysis. Risk of bias of included studies and indirectness of intervention methodology had the main impacts on the level of certainty. See online supplemental material 4 for Downs and Black checklist and online supplemental material 5 for GRADE analysis.
Meta-analyses
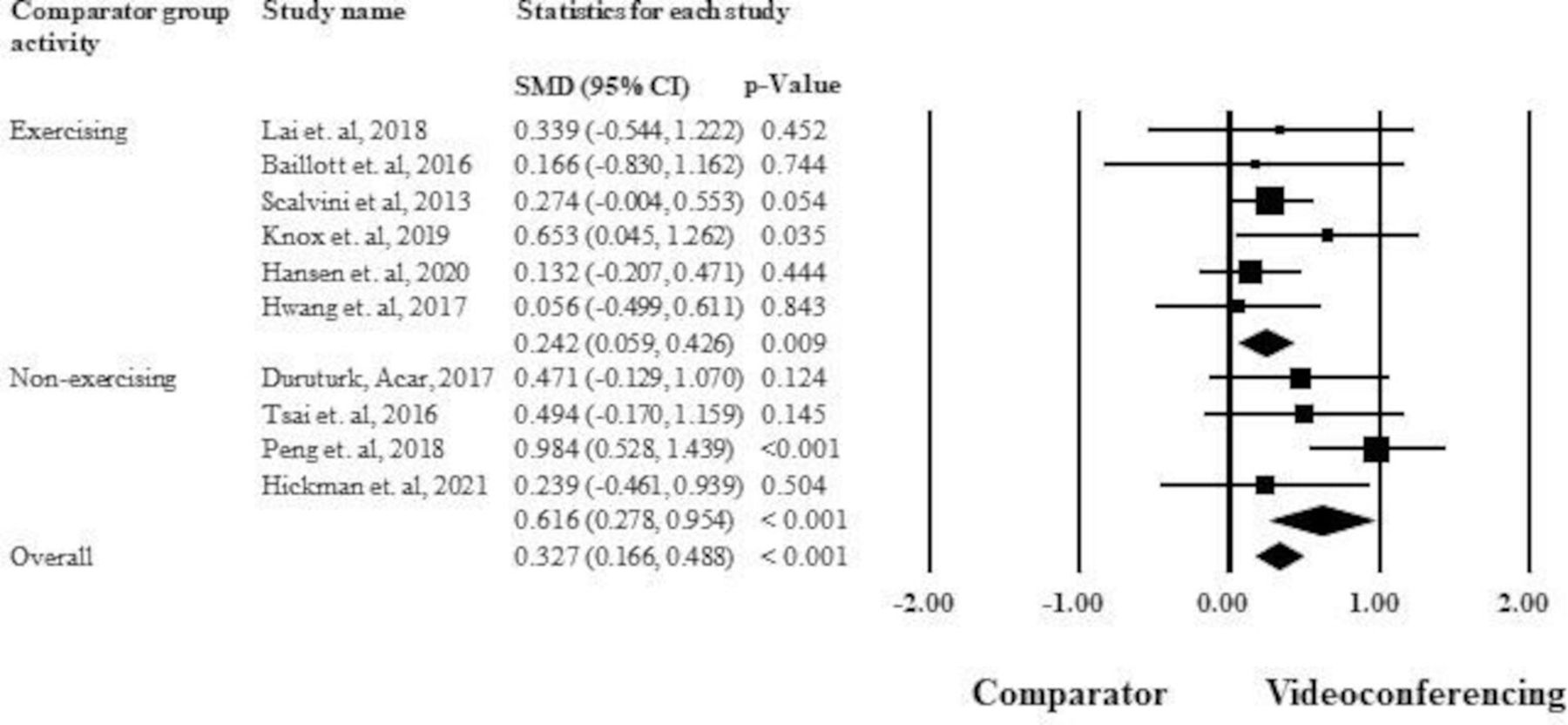
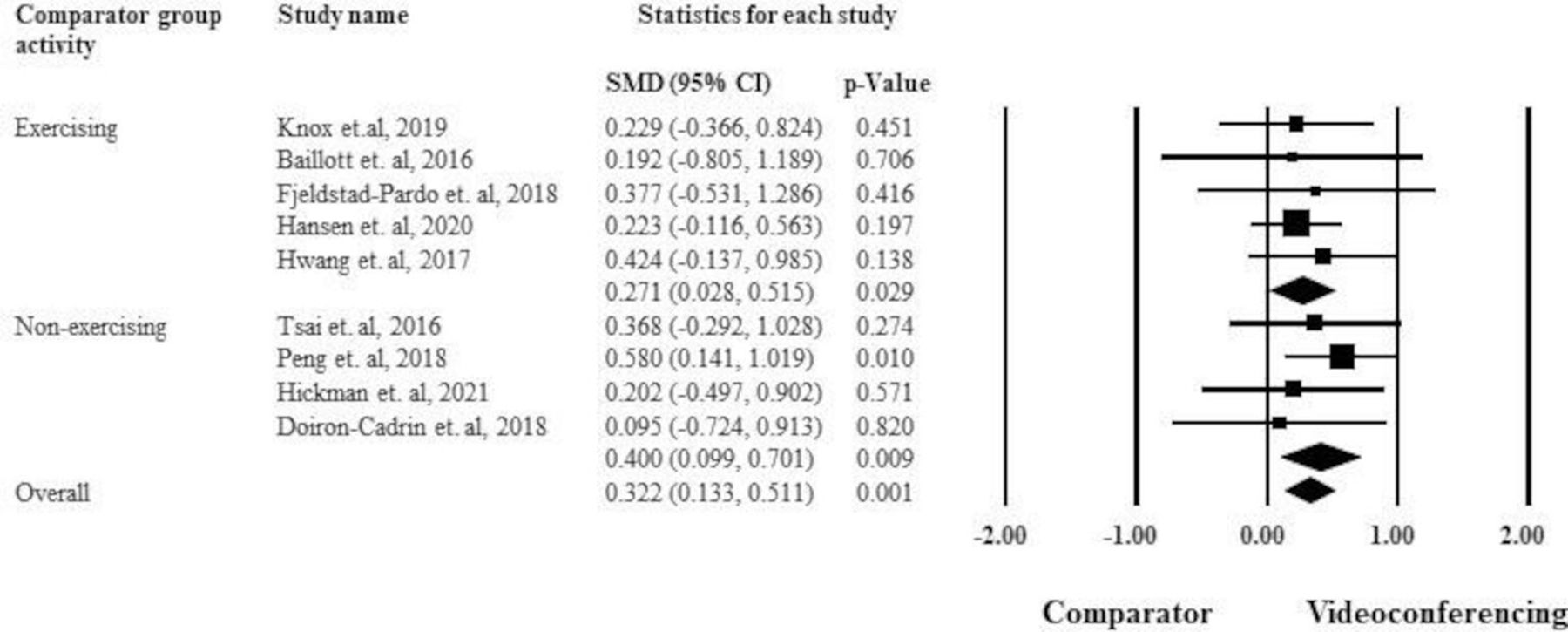
The between-group analyses for videoconferencing versus comparator, subgrouped via comparator group activity, are presented for exercise capacity (figure 2) and quality of life (figure 3). A small summary effect (including both exercising and non-exercising comparator groups) was observed overall favouring videoconferencing for exercise capacity (SMD=0.327, 95% CI 0.166 to 0.488, p=<0.001; I2=24.3%) and quality of life (SMD=0.322, 95% CI 0.133 to 0.511, p=0.001; I2=0%). Studies using an exercising comparator group showed a small effect favouring videoconferencing for exercise capacity (SMD=0.242, 95% CI 0.059 to 0.426, p=0.009; I2=0%). When subgrouped by non-exercising comparators, there was a moderate effect for exercise capacity (SMD=0.616, 95% CI 0.278 to 0.954, p≤0.001; I2=23.8%). An effect favouring videoconferencing was observed for quality of life when grouped via both exercising (SMD=0.271, 95% CI 0.028 to 0.515, p=0.029; I2=0%) and non-exercising comparators (SMD=0.400, 95% CI 0.099 to 0.701, p=0.009; I2=0%). Single-arm studies showed a small effect for exercise capacity (MD=34.2 m, 95% CI 15.5 to 53 m, p≤0.001, I2=0%; online supplemental material 6) and quality of life (SMD=0.459, 95% CI 0.265 to 0.654, p≤0.001, I2=19.6%; online supplemental material 7). Most studies were determined to be not skewed and visual inspection of funnel plots suggested low risk of publication bias, with Egger’s statistic showing no bias for quality of life (comparator trials, p=0.33; single-arm trials, p=0.21) and exercise capacity (comparator trials, p=0.31, single-arm trials, p=0.33).
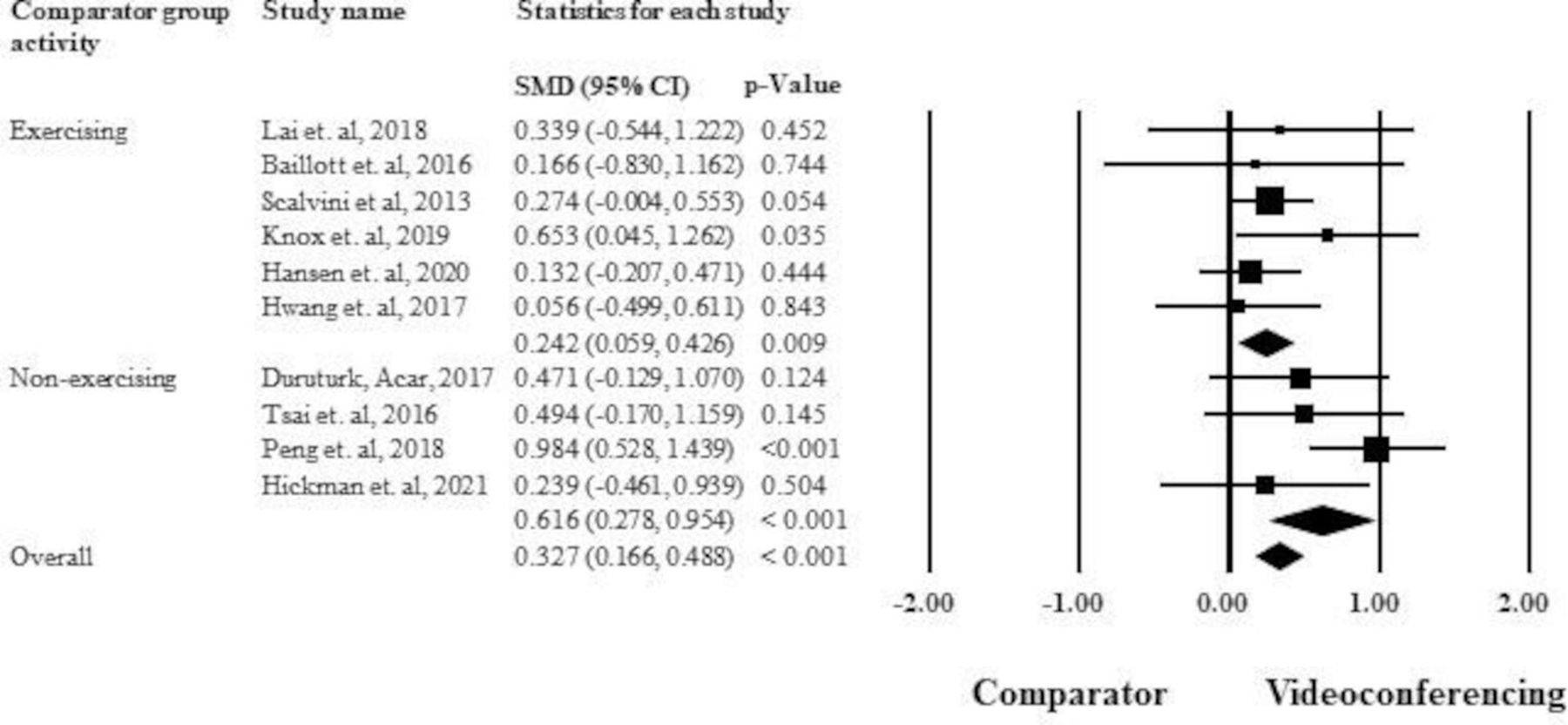
Meta-analysis of exercise capacity for comparator trials, subgrouped by comparator group activity. SMD, standardised mean difference.

{kind=link}
{kind=link}
{kind=link}
Meta-analysis of quality of life for comparator trials, subgrouped by comparator group activity. SMD, standardised mean difference.
Discussion
This systematic review with meta-analyses assessed the effectiveness and feasibility of videoconferencing exercise interventions for people with chronic diseases. The analyses combined 32 trials (29 in meta-analyses), including 1049 participants. Disease groups included pulmonary conditions, cardiac disease, neurological disorders, metabolic disorders, cancer and musculoskeletal conditions. Pooled data demonstrated that videoconferencing was an effective exercise delivery modality for improving exercise capacity and quality of life. Feasibility was also assured through the analysis of session attendance rates, adherence to exercise prescription during the session, safety, technical issues and participant satisfaction. This has important clinical ramifications for practitioners who are seeking to adopt these technologies to enable more equitable access to exercise service delivery. This is especially pertinent in response to the global COVID-19 pandemic.
Effectiveness of videoconferencing exercise interventions
The pooled data demonstrated that videoconferencing was effective at improving exercise capacity and quality of life for patients with chronic disease. Moderate to low certainty rating was identified through GRADE for both exercise capacity and quality of life outcomes. Observation bias was uncovered due to low rates of assessor blinding and allocation concealment across trials. Small sample sizes, limited comparative data and an overall moderate risk of bias score for included studies decrease the confidence in the findings. Importantly, this outlines the need for methodologically robust trials to be conducted in the future.
Nevertheless, given the known influence of exercise training per se on exercise capacity and quality of life outcomes, and that exercising and non-exercising comparators were included, exercising/non-exercising subgroup analyses were conducted to ensure accurate representation of data. It was found that improvements in exercise capacity with videoconferencing interventions exceeded both exercising and non-exercising comparator groups. This was common across supervised and unsupervised exercise among comparator groups. Additionally, a significant improvement favouring videoconferencing was observed for quality of life when subgrouped by exercising and non-exercising comparators. These data demonstrated that videoconferencing may be at least as effective as in-person interventions and superior to no intervention. In addition, analysis of single-arm trials demonstrated improvements in both outcomes. A pooled mean difference of 34.2 m postintervention was identified for the 6MWT, which is clinically meaningful across different forms of chronic disease.60–63 However, these trials were without a comparator group, and therefore the risk of biased outcomes (including regression to the mean) is high, and this finding must be interpreted with caution. Due to the inclusion of different outcome measures leading to the use of SMD, we are unable to infer clinical meaningfulness on SMD specific outcomes. The low levels of heterogeneity identified via the I2 and Q statistics, as well as the small number of studies in each subgroup, negate the need for metaregression. The results of this meta-analysis align with previous literature suggesting that various forms of telerehabilitation may be as effective at improving health markers as in-person services in chronic disease64–69 and warrant further investigation through more robust trials.
The inclusion criteria for this review required aerobic and/or resistance exercise training. Different modalities of exercise training (eg, balance, neuromotor and flexibility) are also well suited for delivery over videoconferencing. Traditional classes such as tai-chi and yoga have been delivered via videoconferencing with high levels of efficacy, safety and patient satisfaction.70–74 These types of interventions have demonstrated improvements in quality of life and ability to undertake activities of daily living.70 71 73 74 Along with aerobic and resistance training, these modalities have the potential to improve various health-related outcomes. Therefore, we suggest that health professionals undertaking a videoconferencing exercise approach to training should base their modality selection on specific goals for each person’s health condition and individual preferences. Additionally, health professionals should strive to align intervention delivery with patient-preferred outcomes and goals. Videoconferencing exercise interventions may also be an important addition to the clinical armoury supporting patient preference. Overall, videoconferencing may be applied as an alternative modality to traditional rehabilitation services to high levels of effectiveness where in-person delivery is not possible or preferable.35 40 75 76
Feasibility of videoconferencing exercise interventions
Feasibility of service delivery is crucial for the widespread implementation and uptake of videoconferencing exercise interventions. Expert guidance is needed to ensure the risks of adverse events are kept to a minimum.77 78 Concerns for the safety of participants are compounded in videoconferencing sessions where capacity to action adverse events is diminished.79 However, resistance and aerobic exercise improve common risk factors associated with chronic disease.80–82 This emphasises the need for exercise to be incorporated into chronic disease management. With videoconferencing presenting a unique opportunity to deliver the beneficial effects of exercise remotely, risk analysis must be undertaken to address safety. Previous literature has identified that telerehabilitation poses no increased risk of adverse events than usual care in chronic disease settings.83 In the present review, no trial reported an increased number of exercise-related adverse events in the videoconferencing group.
Telehealth technologies play an important role in connecting patients and clinicians.84 A potential barrier of the implementation of telehealth interventions is the presence of technical issues.84–86 Commonly reported technical issues include disturbances to audiovisual quality and diminished connectivity.86 87 Additionally, health professional perception and acceptance of telerehabilitation can be a significant barrier. Lack of in-person treatment for complex patients, diminished vital sign monitoring and decreased confidence with the reliability of online technology present as barriers to implementation.88 89 Presence of technical issues presented as a barrier to participation in the listed trials, with nine trials reporting the total number of technical issues affecting 17% of total sessions overall.28 30 34 35 46 51 55 57 A recent systematic review in patients who had a stroke suggested that even though technical issues can be present in telerehabilitation, steps can be taken to ensure they are minimised preparticipation.90 These include the provision of technical support (both in-home and external) and the gradual scaling of administrative coaching, where increased time with technology is taking place in the first week of use.90 Additionally, required bandwidth, practice with technology, security of transmitted images and dependability of equipment are aspects to consider pre-implementation to increase patient and health professional confidence in adopting telerehabilitation.91 Furthermore, the preliminary data collected in this review can suggest that videoconferencing exercise interventions may have acceptable levels of usability. Future studies should investigate this observation further in people with chronic diseases. Additionally, administrative workforce development for the facilitation of videoconferencing sessions should be encouraged within healthcare settings to lessen the burden on health professionals. The addition of a support team to organise and enable videoconferencing may help to expand the ability of these services to be implemented in a real-world setting.
Attendance to videoconferencing exercise interventions across trials was 70%. Among the listed trials, reporting of attendance varied widely. Including data from author contacts, 24 trials had an attendance measure and 8 (26% of total trials) provided mean and SD. In addition, no trials reported adherence to exercise prescription during the session. This inability to verify that participants completed the prescribed intervention makes it difficult to determine whether the adherence to exercise training was associated with change in effectiveness outcomes. Adherence to telehealth interventions has been flagged as a potential barrier to implementation among health professionals.92 Future studies should emphasise the monitoring and reporting of attendance and adherence data to better understand the relationship between the intervention and outcomes.
Within the listed studies, generally positive satisfaction rates were reported for videoconferencing. Convenience, usefulness and ease of access to technology were driving factors for the high satisfaction rates observed. Sources of dissatisfaction can relate to the presence of technical issues within session. Positive satisfaction rates for telerehabilitation are consistent throughout the literature, with ease of use and decreased cost/time burden increasing engagement.93 Although not all trials measured satisfaction rates in this review (n=17, 53%), it can be suggested that videoconferencing may be an effective and satisfying modality of exercise for patients with chronic disease. Further investigation into this observation is recommended.
Future directions
Due to the highly accessible nature of videoconferencing technology, the potential for integration into patient care is substantial. However, future studies need to investigate the effectiveness of these interventions with more robust methodology. Future studies should employ appropriate assessor blinding, be adequately powered, include comparator groups and use intention-to-treat analysis to increase the validity of the observed results. Adequate monitoring and reporting of attendance and adherence to exercise prescription should also be encouraged. Future studies should also emphasise the reporting of the magnitude and nature of technical issues present in session. This is because both health professional and patient acceptance of technology are influenced by the presence of technical issues.
The main limitations of this review were due to the number, quality and types of trials that were included. Only 12 comparator trials including 757 individuals that met the inclusion criteria have been conducted. Of these only eight are randomised controlled trials with 463 participants. Although separated from the comparator trials, the inclusion of single-arm studies is another limitation as they are subject to regression to the mean and time trends. As patient data sets could not be accessed as part of this review, normality of individual data could not be assessed. Due to the sample sizes of trials included in the meta-analyses, small-sample bias may have been present.94 The quality of the trials was demonstrated with moderate risk of bias (Downs and Black score=16.3/28) and moderate/low certainty rating identified through GRADE analysis. While the quality of trials was generally low, our sensitivity analysis showed that no study significantly influenced the results of the meta-analysis. Although SMD allowed for the comparison of multiple outcome measures across different scales, its use is a limitation. The SD of a measure will often vary over different populations, making the generalisability of SMD problematic. This could have resulted in confounding and potentially distorted the observed results in the meta-analyses.95 96
Conclusion
Videoconferencing exercise interventions appear to be an effective and feasible modality of exercise delivery for improving markers of exercise capacity and quality of life in patients with chronic disease. Importantly, sessions led by videoconferencing resulted in comparable improvements in outcomes to in-person exercise interventions. This suggests that videoconferencing is a suitable and accessible alternate delivery modality for exercise training. However, studies with more robust methodology need to be conducted to verify these findings. Future studies should also emphasise adequate reporting of exercise adherence and technical issue data. Implementing these measures will reduce the risk of methodological bias and provide a more accurate understanding of the benefits of videoconferencing exercise interventions for patients with chronic disease.
Key messages
What is already known on this topic
Exercise interventions in several chronic disease groups delivered in-person have a beneficial impact on a vast range of medical and patient-reported outcomes.
Previous literature suggests that telehealth may be an effective alternate to traditional exercise services in chronic disease.
What this study adds
Videoconferencing exercise interventions are feasible and effective for improving exercise capacity and quality of life for patients with chronic disease.
More robust trials are needed to verify these findings. Emphasis must be placed on exercise adherence and technical issue reporting.
How this study might affect research, practice and/or policy
High levels of patient satisfaction, coupled with low rates of technical issues, emphasise the ability of videoconferencing exercise interventions to meet the demands of an evolving healthcare system and to better support patient preference.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
The authors thank Dr Jaimon Kelly (ORCID: 0000-0003-0232-5848) for his expert input with the GRADE analysis, and Prof Norman Morris (ORCID: 0000-0003-4054-4662) for his advice on the review methodology.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @Riley_Brown96
Contributors RCCB contributed to the design of the study, was responsible for the collection, analysis and interpretation of the data, and oversaw the writing of the manuscript. JSC contributed to the design of the study and the interpretation of data and provided feedback on drafts of the manuscript. KJR contributed to the collection of data. IJH provided feedback on drafts of the manuscript. SEK contributed to the design of the study, the analysis and interpretation of data, and provided feedback on drafts of the manuscript. All authors read and approved the final manuscript.
Funding In-kind contributions were received from The University of Queensland and the Department of Nutrition and Dietetics for the completion of this review. No external sources of funding were used to assist in the preparation of this article. SK is supported by the National Health and Medical Research Council of Australia via an Early Career Research Fellowship (122190).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.