Article Text

Abstract
Objective To quantify the association between physical activity and risk of SARS-CoV-2 infection, COVID-19-associated hospitalisation, severe illness and death due to COVID-19 in adults.
Design A systematic review and meta-analysis.
Data sources Three databases were systematically searched through March 2022.
Eligibility criteria for selecting studies Peer-reviewed articles reporting the association between regular physical activity and at least one COVID-19 outcome in adults were included. Risk estimates (ORs, relative risk (RR) ratios or HRs) were extracted and pooled using a random-effects inverse-variance model.
Results Sixteen studies were included (n=1 853 610). Overall, those who engaged in regular physical activity had a lower risk of infection (RR=0.89; 95% CI 0.84 to 0.95; I2=0%), hospitalisation (RR=0.64; 95% CI 0.54 to 0.76; I2=48.01%), severe COVID-19 illness (RR=0.66; 95% CI 0.58 to 0.77; I2=50.93%) and COVID-19-related death (RR=0.57; 95% CI 0.46 to 0.71; I2=26.63%) as compared with their inactive peers. The results indicated a non-linear dose–response relationship between physical activity presented in metabolic equivalent of task (MET)-min per week and severe COVID-19 illness and death (p for non-linearity <0.001) with a flattening of the dose–response curve at around 500 MET-min per week.
Conclusions Regular physical activity seems to be related to a lower likelihood of adverse COVID-19 outcomes. Our findings highlight the protective effects of engaging in sufficient physical activity as a public health strategy, with potential benefits to reduce the risk of severe COVID-19. Given the heterogeneity and risk of publication bias, further studies with standardised methodology and outcome reporting are now needed.
PROSPERO registration number CRD42022313629.
- Covid-19
Statistics from Altmetric.com
Disclaimer: this video summarises a scientific article published by BMJ Publishing Group Limited (BMJ). The content of this video has not been peer-reviewed and does not constitute medical advice. Any opinions expressed are solely those of the contributors. Viewers should be aware that professionals in the field may have different opinions. BMJ does not endorse any opinions expressed or recommendations discussed. Viewers should not use the content of the video as the basis for any medical treatment. BMJ disclaims all liability and responsibility arising from any reliance placed on the content.
WHAT IS ALREADY KNOWN ON THIS TOPIC
Regular physical activity has a protective effect against severity of respiratory infections.
Regular physical activity is associated with a multitude of beneficial health effects, including the reduction of the incidence of risk factors for adverse COVID-19 outcomes (ie, obesity, type 2 diabetes).
WHAT THIS STUDY ADDS
Regular physical activity is related with lower risk of SARS-CoV-2 infection and lower likelihood of adverse COVID-19 outcomes (including hospitalisation, severity and mortality), although due to limitations of the studies, our findings need to be interpreted with caution.
Greatest benefit is provided by achieving at least 500 metabolic equivalent of task (MET)-min per week of physical activity, which is equivalent to 150 min of moderate-intensity or 75 min of vigorous-intensity physical activity per week.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
These findings may help guide physicians and healthcare policymakers in making recommendations and developing guidelines with respect to the degree of physical activity that can help reduce the risk of adverse COVID-19 outcomes at both the individual and the population level, especially in high-risk patients.
Introduction
SARS-CoV-2, the causative agent of COVID-19, was detected in 2019 in Wuhan (Hubei, China). Declared a pandemic by the WHO in March 2020, COVID-19 has brought devastating human and economic consequences.1 2 Researchers worldwide are continuing to undertake research to understand the factors contributing to virus-related morbidity, hospitalisation and mortality, to inform clinical decisions and public health strategies. Several risk factors for increased disease severity have already been identified including personal characteristics such as age, sex and race as well as health conditions including diabetes, obesity, hypertension and respiratory illnesses.3
It is well known that regular physical activity exerts a multitude of beneficial health effects, including reducing the incidence of the aforementioned risk factors for increased severity of COVID-19.4 5 Perhaps more importantly is the ability of physical activity to both enhance immune defence and mitigate the deleterious effects of stress on immunity during the COVID-19 pandemic.6 Previous studies have suggested that sufficient physical activity has a protective effect against both the infectivity and severity of respiratory infections7–9 due, at least in part, to its immunological benefits.8
The link between regular physical activity and COVID-19 outcomes is poorly understood but likely involves both metabolic and environmental factors.10 A growing body of evidence from several studies has suggested that increased physical activity may modulate the disease course and reduce the development of negative outcomes in confirmed cases of COVID-1911; however, there has been no attempt to systematically evaluate and meta-analyse the current evidence on the effect of habitual physical activity on COVID-19 outcomes. Additionally, these studies varied with respect to sample size, ethnicity and other characteristics, leading to inconsistencies with respect to their interpretation. Accordingly, the aim of the present study was to quantify the association between physical activity and risk of SARS-CoV-2 infection, COVID-19-associated hospitalisation, severe illness and death due to COVID-19 in adults.
Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines12 and The Meta-analysis Of Observational Studies in Epidemiology guidelines13 were followed. This meta-analysis was registered in the International Prospective Register of Systematic Reviews (PROSPERO).
Eligibility criteria
To be eligible for inclusion in the present meta-analysis, studies had to meet the following criteria: (1) participants: adults aged 18 years and older with and without a diagnosis of COVID-19 disease (ie, as tested using real-time reverse transcriptase-PCR assay on nasal and pharyngeal swabs), (2) exposure: physical activity assessed with questionnaires or objective-measure devices (ie, accelerometers, heart rate monitors, smart devices), (3) outcomes analysed: SARS-CoV-2 infection, hospitalisation due to COVID-19, severe COVID-19 (eg, due to intensive care unit (ICU) admission, administration of invasive ventilation) and death due to COVID-19 and (4) study design: case–control, cross-sectional, prospective and retrospective cohort studies. Studies were excluded if they did not report data regarding the variables of interest and/or data for HRs, relative risk (RR) or ORs and 95% CIs, and studies that included self-reported COVID-19 infection or already hospitalised patients.
Information sources
Two authors (YE and AG-H) independently searched PubMed, Web of Science and SportDiscus databases for studies listed between November 2019 and March 2022. The search had no language restriction. We also searched and reviewed the references cited within the retrieved relevant reports for any additional studies. A professional librarian was consulted to verify the quality of the search strategy.
Search strategy
The following string of terms was used: ‘physical activity’, ‘COVID-19’, ‘SARS-CoV-2’, ‘mortality’, ‘hospitalization OR ‘hospitalisation’, ‘infection’, ‘severe COVID-19’. Reference lists of eligible studies were manually examined for further identification of relevant articles and included if appropriate. Any disagreement was resolved by consensus with a third author (RR-V). Full search strategies for all databases are shown in online supplemental emethod 1.
Supplemental material
Selection process
After removing duplicates and reviewing the title and abstract of potential studies, two authors (YE and AG-H) systematically assessed the full text of identified manuscripts for eligibility.
Data collection and data items
The following data were extracted from each study by two authors (YE and AG-H), using a Microsoft Excel spreadsheet specifically designed for the present study: (1) study characteristics (ie, first author’s name, publication year, country and sample size), study design (ie, case–control, cross-sectional, prospective and retrospective cohort studies) and duration of follow-up (where applicable), (2) participants’ information (ie, sex, age, number of events (eg, hospitalisation, severe COVID-19)), (3) physical activity assessment details (ie, self-reported, objective-measured, definition) and (4) statistical analysis and study results (ie, confounding factors, outcome of interest and main results as RR, HR or OR and the corresponding 95% CI was recorded).
Quality assessment
The quality of included studies was evaluated according to the Quality Assessment Tool for Observational Cohort and Cross-sectional Studies (14 items) and the Quality Assessment of Case-Control Studies (12 items). Each item of methodological quality was classified as ‘yes’, ‘no’ or ‘other’ (CD, cannot determine; NA, not applicable; NR, not reported).14
The Grading of Recommendations, Assessment, Development and Evaluation (GRADE) approach was used to evaluate the quality of the evidence and grading strength of recommendations.15
Effect measures
For the meta-analysis, RR and OR with associated 95% CIs were collected from studies for each COVID-19 outcome, if available. When the RR was not provided, it was calculated from adjusted OR when possible using the method of Zhang and Yu.16 Because these transformations can underestimate the variance of the RR derived from the OR and produce a biased estimate when confounding is present,17 18 we performed a sensitivity analysis that excluded seven studies for which this transformation had been applied.
Synthesis methods
All analyses were performed using STATA (V.17.0, STATA Corporation, College Station, Texas) and all p values were two sided with a significance level of 0.05. Meta-analysis was performed using the random-effects inverse-variance model with the Hartung-Knapp-Sidik-Jonkman adjustment.19 RR values were pooled when comparing the inactive (reference group) versus active categories in relation to COVID-19 outcomes. When studies presented several statistical risk-adjustment models, only the RR associated with the statistical models that contained the highest number of additional covariates was considered. Studies reporting risk estimates relative to the highest category of physical activity20 21 were recalculated to set the lowest physical activity category as the referent.22
To examine the percentage of variation within studies as a consequence of heterogeneity and not explained by chance, the heterogeneity index (I2) was used and was estimated from the Cochran Q statistic. Cut points for low, moderate and high degrees of heterogeneity were I2 values of 25%, 50% and 75%, respectively.23
Potential small-study effects due to publication bias were examined using the Luis Furuya-Kanamori (LFK) index and the Doi plot. Values of –1, between –1 and –2, and >–2, were considered to represent no, minor and major asymmetry, respectively.24
A sensitivity analysis was conducted to assess the robustness of the summary estimates and to determine whether a particular study accounted for the inconsistency. To examine the effects of each result from each study on the overall results, results were analysed with each study removed from the model once.
Whenever possible, a subgroup analysis was conducted according to the design of the study (cross-sectional and case–control or prospective and retrospective studies) and type of physical activity assessment (subjective or objective).
For the dose–response meta-analysis, we computed study-specific slopes (linear trends) and 95% CIs from the natural logs of the RR and CIs across categories of physical activity using the method of Greenland and Longnecker.25 Only studies with three or more quantitative physical activity levels were included in these analyses. A potential non-linear dose–response relationship between physical activity and COVID-19 outcomes was examined by using restricted cubic splines with 3 knots at 10%, 50% and 90% percentiles of the distribution.26
In preparation for the dose–response meta-analysis, we standardised domain-specific physical activity measures to total metabolic equivalent of task (MET) min of physical activity per week as follows: (1) the mean physical activity in each category was assigned to the corresponding RR for each study, (2) for studies that reported ranges of physical activity, we estimated the midpoint for each category by calculating the average of the lower and upper bounds, (3) when the highest or lowest category was open ended (eg, ≥1 500 MET-min/week), we multiplied or divided the reported upper boundary by 1.25 and used this value (1 875 MET-min/week in the example), (4) for studies that reported physical activity categories as sufficient/insufficient,20 or consistently active/inactive,21 some activity or low, moderate and high,27 28 we take into account the following cut-offs: inactive/none/low (0 MET-min/week), insufficiently active/insufficient/moderate/some activity (0–<500 MET-min/week), active/sufficient/high (500–<1 000 MET-min/week) and highly active (more than 1000 MET-min/week) and (5) for studies that reported physical activity by frequency per week,29 30 we converted the frequencies to minutes per week by assigning a dose of 45 min/session at moderate intensity (ie, 4 MET).31
Results
Study selection
The electronic search strategy retrieved 4 063 studies. After removing duplicates and screening titles, 291 studies were assessed for eligibility based on full text. A total of 16 studies were included in the present meta-analysis.10 20 21 27–30 32–40 The PRISMA flow diagram illustrating the number of studies excluded at each stage of the systematic review and meta-analysis is shown in figure 1. A reference list of excluded articles and reasons for exclusion based on the full text is detailed in online supplemental emethod 2.
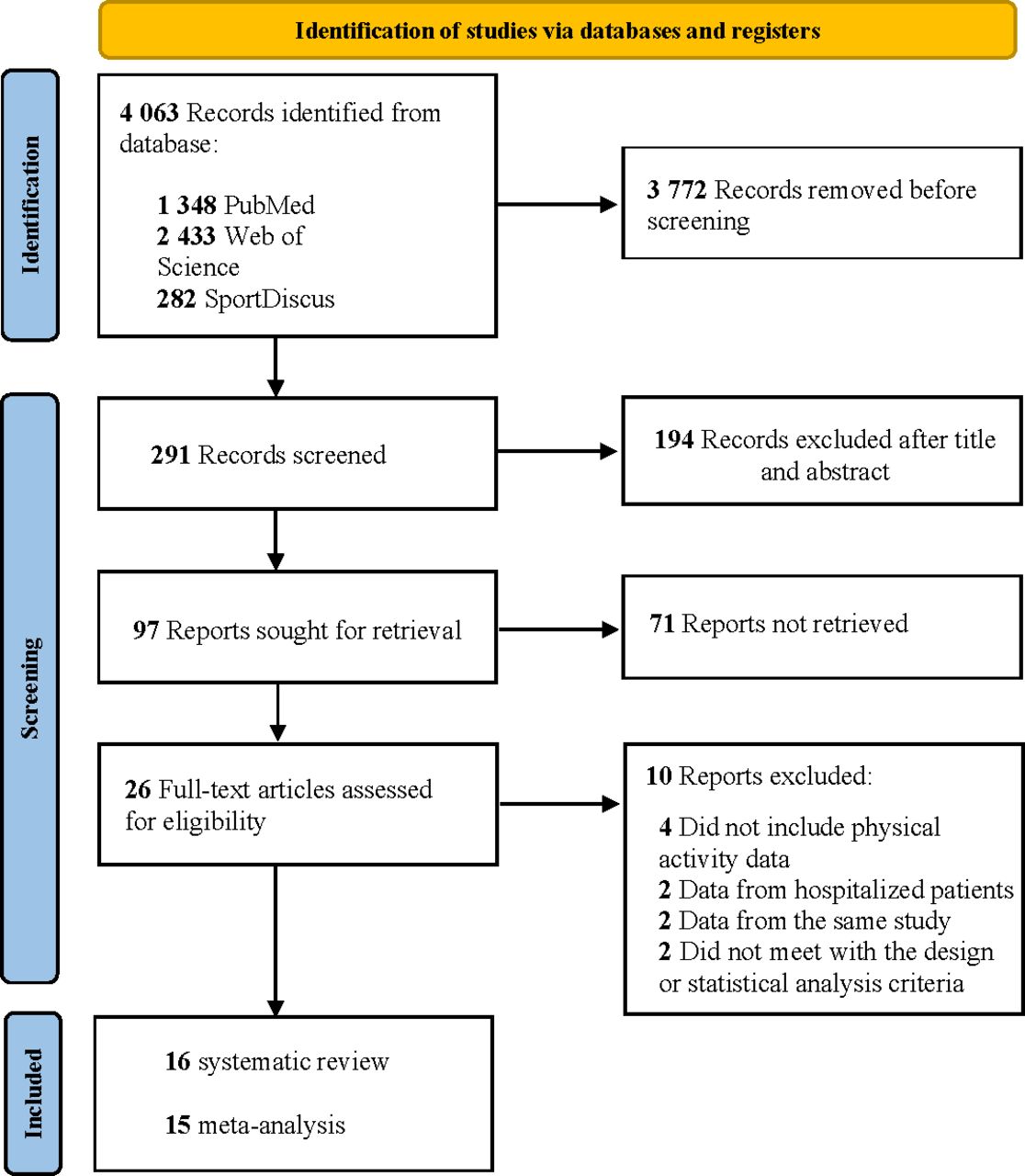
PRISMA flow diagram. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Study characteristics
The main characteristics of the included studies are described in online supplemental etable 1. Sixteen studies fulfilled eligibility criteria and were included in the systematic review, including 1 853 610 participants (53% women, mean age 53.2 years). To avoid double counting, when two studies analysed the same variables using data from the same source and similar physical activity assessment (questionnaires or accelerometers),20 28 32 33 we only included those studies with the larger sample size.33 Study designs included cross-sectional studies,29 34–36 38 case–control studies,37 39 40 prospective cohort studies10 20 21 28 32 33 and retrospective observational studies.21 27 Studies were conducted in South Korea,37 England,20 Iran,36 Canada,34 UK,28 32 33 USA,21 Spain,29 Brazil,38 Palestine,35 South Africa27 and Sweden,39 or involved different countries.30 40 The main outcomes of the included studies were hospitalisation for COVID-19,20 21 27 30 32–35 38 39 severe illness10 21 27 29 32 34 36 38 40 and COVID-19 mortality.10 21 27 28 33 37 39 Also, one study defined severe COVID-19 illness as either hospital admission, admission to ICU and/or death due to COVID-19.39
Sources of information included the Korean National Health Insurance Database,37 Health Profile Assessment database,39 UK Biobank,20 28 32 33 Discovery Health and Vitality Client Data,27 Electronic health records of Kaiser Permanente South California,21 the Survey of Health, Ageing and Retirement in Europe,30 data from the COVID-19 Host Genetic Initiative40 and participant responses from independent surveys.29 38 Clinical data including hospitalisation cases, use of ICU or ventilation were extracted from medical records in most studies10 20 21 27 28 32 33 36 37 39; however, three studies used self-reported hospitalisation data.29 30 34 35 38 Data on mortality from COVID-19 were extracted from death certificates through linkage with National Registers10 28 32 33 37 39 or from medical registers.21 27 One study specified that COVID-19 mortality as the primary cause of death was determined from the presence of ICD-10 codes U07.1 or U07.2,28 and another study defined COVID-19 mortality as the termination of isolation due to death.37 Estimations of total events included 134 639 positive cases, 20 984 hospitalisations for COVID-19, 7 009 cases of severe illness for COVID-19 (including ICU and/or ventilation use) and 2 878 COVID-19-related deaths.
Physical activity was self-reported in most studies,10 20 21 28–30 34–39 although three studies directly measured physical activity through accelerometers,32 33 40 or smart devices, clocked gym attendance or recorded mass sports event participation.27 Most studies grouped physical activity level according to self-reported variables such as MET-min/week,10 28 36 37 time spent during the week,27 30 33 34 39 physical activity intensity29 or meeting physical activity guidelines.20 21 38 One study did not report the method of classification of physical activity.35
Study quality
All observational cohort and cross-sectional studies met at least 7 out of 14 items included in the Quality Assessment Tool for Observational Cohort and Cross-sectional Studies and were considered to have fair-to-good methodological quality. The average score of observational cohort and cross-sectional studies was 10.31/14, and case–control studies had 9.7/12 on average (online supplemental etable 2).
Regarding the GRADE assessment, the overall quality of the evidence for the association between physical activity and SARS-CoV-2 infection and COVID-19 hospitalisation was low, and for physical activity and severe COVID-19 illness and death due to COVID-19 was moderate. The dose–response gradient associated with physical activity and risk for having severe COVID-19 illness and mortality due to COVID-19 was deemed a relevant reason to upgrade the quality of evidence for those outcomes. An overview of each GRADE domain for each COVID-19 outcome is summarised in online supplemental etable 3.
Synthesis of results
Adults who engaged in regular physical activity had a lower risk of SARS-CoV-2 infection (RR=0.89; 95% CI 0.84 to 0.95, p=0.014; I2=0%), hospitalisation (RR=0.64; 95% CI 0.54 to 0.76, p<0.001; I2=48.01%), severe COVID-19 illness (RR=0.66; 95% CI 0.58 to 0.77; p<0.001; I2=50.93%) and death due to COVID-19 (RR=0.57; 95% CI 0.46 to 0.71; p=0.001; I2=26.63%) when compared with adults who were classified as inactive (figure 2).
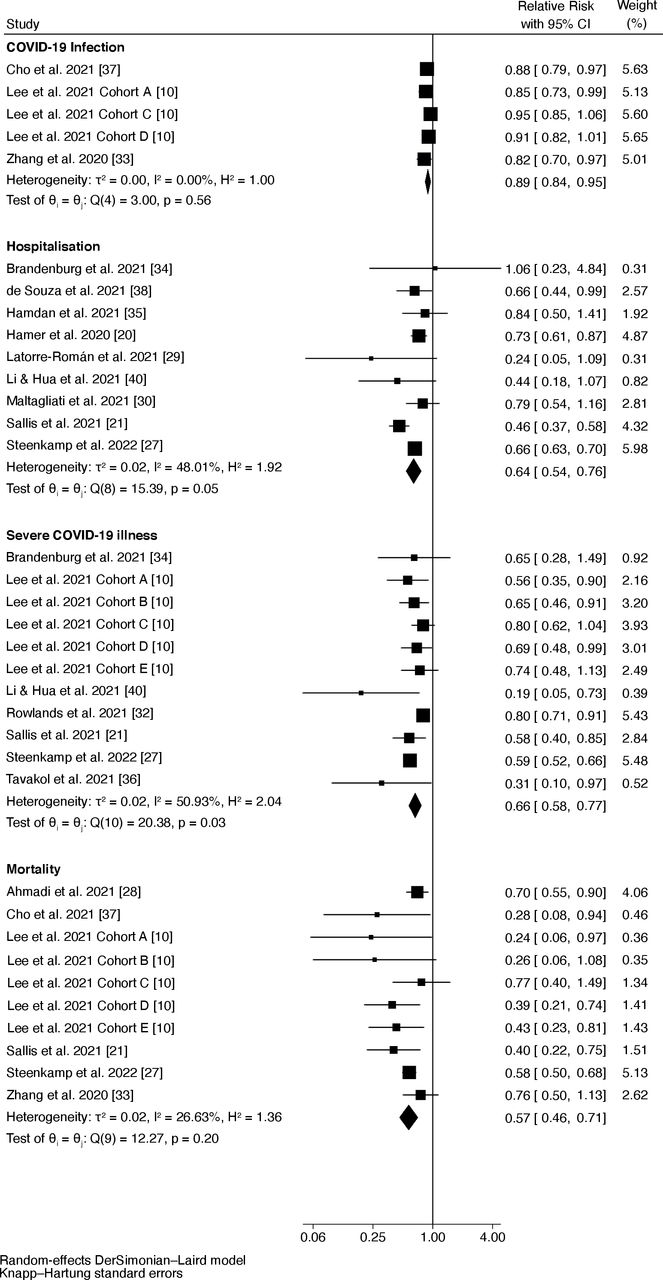
Forest plot showing the relative risk of COVID-19 infection, hospitalisation, severe COVID-19 and death due to COVID-19 comparing physically active and inactive adults.
The LFK index for the Doi plots showed minor asymmetry in hospitalisation (LFK=−1.02) (online supplemental efigure 1), and major asymmetry indicating risk of publication bias in COVID-19 infection (LFK=−2.39) (online supplemental efigure 2), severe COVID-19 illness (LFK=−3.49) (online supplemental efigure 3) and mortality (LKF index=−4.74) (online supplemental efigure 4).
Sensitivity analyses confirmed that overall findings remained once each study was individually excluded (online supplemental efigure 5 to 8).
Subgroup analysis according to design, physical activity assessment and measure outcome is shown in online supplemental etable 4. Overall, physical activity was related with lower risk of SARS-CoV-2 infection, hospitalisation and death due to COVID-19 independent of design and instrument used. Physical activity assessed objectively was related with lower risk of severe COVID-19 illness (RR=0.65; 95% CI 0.24 to 1.75, p=0.200; I2=88.5%), but not significantly. A sensitivity analysis that excluded the studies where only OR instead of RR were presented had little effect on the results and lower heterogeneity (COVID-19 infection RR=0.91; 95% CI 0.80 to 1.06, p=0.115; I2=0%; hospitalisation, RR=0.66; 95% CI 0.62 to 0.71, p<0.001; I2=0%; severe COVID-19 illness, RR=0.64; 95% CI 0.55 to 0.75, p<0.001; I2=17.39%; death due to COVID-19, RR=0.61; 95% CI 0.47 to 0.80, p=0.003; I2=61.30%).
Finally, the results indicated a non-linear dose–response relationship between physical activity presented in MET-min/week and severe COVID-19 illness (figure 3A) and COVID-19-related death (figure 3B) (p for non-linearity <0.001), but not for infection (p=0.344) and hospitalisation (p=0.122). Non-linear associations were observed in both analyses with a flattening of the dose–response curve at around 500 MET-min/week.

{kind=link}
{kind=link}
{kind=link}
Non-linear relationship between physical activity and severe COVID-19 illness (A) and death due to COVID-19 (B).
Discussion
Our analysis reveals that individuals who engage in regular physical activity have a lower likelihood of SARS-CoV-2 infection, COVID-19 hospitalisation, severe COVID-19 illness and COVID-19-related death than physically inactive individuals, independent of design and instrument used. We also found that the greatest benefit is provided by achieving at least 500 MET-min/week of physical activity.
The immunoregulatory effects of physical activity are well known.8 We found evidence of the association between regular physical activity and an 11% lower risk of COVID-19 infection. This finding is consistent with that of Cunningham41 at the US county-level, who found that physical activity negatively associated with COVID-19 cases per 100 000 county residents. Our results also support the findings of other studies in this area linking physical activity with infectious diseases. For example, a recent systematic review and meta-analysis reported that engaging regularly in moderate-to-vigorous physical activity is associated with 31% lower prospective risk of infectious disease and 37% lower risk of infectious disease-related mortality.9 Also, participating in physical activity has been reported to reduce the incidence of community-acquired pneumonia and the risk of acute respiratory infections (eg, upper respiratory tract infection).42
Our meta-analysis also suggests that adults who engage in regular physical activity have lower risk of COVID-19 hospitalisation and severe COVID-19 illness than those who are physical inactive. According to the available scientific evidence from other viral infections, a possible explanation for these results is that physically active people will have less severe symptoms, shorter recovery times and may be less likely to infect others they come into contact with.43 A previous meta-analysis conducted by Fierens and Goossens44 found that exercise had a significant effect on the severity of symptoms and number of symptom days, confirming our findings. Lee et al 10 reported an interesting finding in their nationwide cohort study: the length of hospital stay was shortened by approximately 2 days in patients participating in both aerobic and muscle strengthening, or with 500–1000 MET-min/week. This also accords with our dose–response analysis, which showed a non-linear relationship between physical activity and severe COVID-19 illness with a flattening at around 500 MET-min/week. Another clinically relevant finding reported by Steenkamp et al 27 was the greater protective effect of physical activity against essential hypertension, diabetes mellitus, chronic renal failure, HIV and rheumatoid arthritis; even those who were in the moderate activity group (ie, 60–149 min/week) had a significantly lower risk of hospitalisation, ICU admission and ventilation compared with peers in the low activity group.
We also found that a high physical activity level was a protective factor for COVID-19 mortality. In accordance with the present results, previous studies have demonstrated that physical activity reduces the influenza-associated mortality.45 The aforementioned immunological benefits of physical activity and exercise may prevent infection, associated severity and death due to COVID-19.8 46 Also, as mentioned, previous studies have demonstrated how physical activity is linked to improved immune markers in several diseases related to COVID-19, including obesity, cardiovascular disease and diabetes,4 5 which are known predictors of severe COVID-19 illness and mortality.3 In this sense, Hamrouni et al 47 provided evidence suggesting that a high physical activity level (ie, ≥600 MET-min/week) may attenuate the COVID-19 mortality risk associated with obesity but may not completely negate the higher risk. Regarding the dose–response analysis, our findings also showed a non-linear relationship between physical activity and death due to COVID-19 with a flattening at around 500 MET-min per week. Therefore, consistent with the literature,48 49 our study confirms the public target range of 500–1000 MET-min per week of physical activity, which is equivalent to 150–300 min of moderate-intensity or 75–150 min of vigorous-intensity physical activity per week.
Several mechanisms have been suggested for the putative protective effects of physical activity in the immune system. For example, in animal models, moderate-intensity exercise seems to be associated with (1) increased leucocyte function, (2) enhanced chemotaxis, degranulation, cytotoxic activity and phagocytosis and (3) reduced cellular inflammation and oxidative stress.50 In healthy humans, physical activity has been linked to reduced systemic inflammation, enhanced natural killer cell cytolytic activity, increased T-cell proliferative capacity, lower circulatory levels of inflammatory cytokines (ie, decreased ‘inflamm-ageing’) and increased neutrophil phagocytic activity, which can all enhance viral control.8 51 Thus, regular moderate-intensity exercise may be effective in enhancing anti-inflammatory responses, which could help to revert lymphocytopenia in patients with COVID-19.52 However, in vitro and individual-level studies are required to verify or refute this hypothesis. Another possible explanation for our findings is the level of cardiorespiratory and muscular fitness of the individuals, as both likely play a pivotal role in explaining the protective effect of physical activity on COVID-19 hospitalisation,30 39 53 severity39 and mortality.53 54 Furthermore, individuals from lower socioeconomic status and low-income or middle-income countries may face additional difficulties in engaging in regular leisure physical activity compared with those from higher socioeconomic backgrounds (ie, limited resources, living in neighbourhoods with less access to parks or with less walkability, paying the costs of participating in registered sports or membership in sport clubs),55 which may place an even greater pandemic burden on these marginalised groups. The challenge is to ensure equitable access to physical activity to ensure better health outcomes for all.
Several limitations must be considered when interpreting our results. The main limitation is that the pooled estimates could be confounded as the results of individual studies are subjected to uncontrolled confounding in practice and the set of adjusted variables often vary over studies reporting adjusted RR/OR. Also, the adjustment for covariates of some individual studies could have been not sufficient, and, therefore, confounding bias should be adjusted using external estimates of confounding.56 Second, most of the participants included in the 16 studies were mainly exposed to the infectious Beta and Delta variants, before the Omicron variant became prevalent globally. Therefore, further studies with these new variants are warranted to confirm our findings as well as studies analysing vaccination impact and use of new treatments. Third, most of the studies used self-reported questionnaires to determine physical activity levels, which may lead to misclassification (ie, an underestimation of the magnitude of true association) and used different definitions to determine physical activity levels. Also, most of the studies obtained data on physical activity status at a single point and collected only leisure-time activities, and not household and occupation-related physical activities, which may impact the magnitude of true associations. Fourth, most of the study designs (ie, cross-sectional and case–control studies) of the included studies prevent the drawing of causal inferences and can be more susceptible to bias (eg, selection bias, information bias). In addition, other potential sources of bias might have been differences in social status or collinearity of risk factors. Also, even representative studies could be biased. For example, the UK Biobank is poorly representative as the response rate was very low and the sample are more affluent and healthier than the average British population. Fifth, only one study excluded patients who had been vaccinated against COVID-19 (either partially or fully vaccinated)27; the remaining studies did not report this information. However, based on the date of data collection, we would speculate that it was before vaccines were widely accessible. Sixth, no study accounted for factors such as social distancing, mask wearing and hand washing, but individual hygiene (ie, hand washing) may serve as an important predictor of COVID-19. Also, the presence of publication bias with the possibility that selective reporting may have further undermined the generalisability of our findings. Seventh, dose–response analysis using mean/midpoints can result in distorted dose–response curve and power/precision loss.56 Eight, the protective benefits of physical activity relative to COVID-19 outcomes may have not been adequately represented, since most studies were adjusted for confounders associated with severe COVID-19 (ie, obesity, hypertension, diabetes). This may have diluted the overall protection of physical activity, which involves the prevention of chronic conditions. Finally, although the correction method proposed by Zhang and Yu16 is often cited and used in practice, simulations suggest that 95% CI obtained using this method suffer from poor coverage, since that they are too narrow and type I error is inflated (too high).57 Additionally, several authors have pointed out that such simple correction methods produce biased RR.17 18
Conclusion
We report the importance of physical activity in lowering the risk of infectivity, hospitalisation, severity and mortality of COVID-19. Greatest benefit is provided by achieving at least 500-MET min/week of physical activity, which is equivalent to 150 min of moderate-intensity or 75 min of vigorous-intensity physical activity per week. However, it is important to bear in mind limitations of the present study (eg, observational designs, subjective tools to assess physical activity, publication bias) when interpreting the results. These findings may help guide physicians and healthcare policymakers in making recommendations and developing guidelines with respect to the degree of physical activity that can help reduce the risk of infectivity, hospitalisation, severity and mortality of COVID-19 at both the individual and the population level,58 especially in high-risk patients. More epidemiological studies with detailed quantification of physical activity and sample size will help establish more precise information regarding this association.59 Given the heterogeneity and risk of publication bias, further studies with standardised methodology and outcome reporting are warranted.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
Antonio García Hermoso had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Also, Antonio García Hermoso is the responsible for the data analysis.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors AG-H and YE conceptualised and designed the study, drafted the initial manuscript, and reviewed and revised the manuscript. RR-V and YE designed the data collection instruments, collected data, carried out the initial analyses and reviewed and revised the manuscript. MI and AG-H conceptualised and designed the study, coordinated and supervised data collection, and critically reviewed the manuscript for important intellectual content. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work. AG-H is responsible for the integrity of the work as a whole.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors. MI and RRV were funded in part by a research grant PID2020-113098RB-I00 of the Spanish Ministry for Science and Innovation (State Scientific, Technical and Innovation Research 2017-2020).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.