Article Text

Abstract
Acute illnesses affecting the respiratory tract are common and form a significant component of the work of Sport and Exercise Medicine (SEM) clinicians. Acute respiratory illness (ARill) can broadly be classified as non-infective ARill and acute respiratory infections (ARinf). The aim of this consensus is to provide the SEM clinician with an overview and practical clinical approach to ARinf in athletes. The International Olympic Committee (IOC) Medical and Scientific Commission appointed an international consensus group to review ARill (non-infective ARill and ARinf) in athletes. Six subgroups of the IOC Consensus group were initially established to review the following key areas of ARill in athletes: (1) epidemiology/risk factors for ARill, (2) ARinf, (3) non-infective ARill including ARill due to environmental exposure, (4) acute asthma and related conditions, (5) effects of ARill on exercise/sports performance, medical complications/return-to-sport and (6) acute nasal/vocal cord dysfunction presenting as ARill. Several systematic and narrative reviews were conducted by IOC consensus subgroups, and these then formed the basis of sections in the consensus documents. Drafting and internal review of sections were allocated to ‘core’ members of the consensus group, and an advanced draft of the consensus document was discussed during a meeting of the main consensus core group in Lausanne, Switzerland on 11 to 12 October 2021. Final edits were completed after the meeting. This consensus document (part 1) focusses on ARinf, which accounts for the majority of ARill in athletes. The first section of this consensus proposes a set of definitions and classifications of ARinf in athletes to standardise future data collection and reporting. The remainder of the consensus paper examines a wide range of clinical considerations related to ARinf in athletes: epidemiology, risk factors, pathology/pathophysiology, clinical presentation and diagnosis, management, prevention, medical considerations, risks of infection during exercise, effects of infection on exercise/sports performance and return-to-sport guidelines.
- IOC
- Consensus
- Respiratory System
Statistics from Altmetric.com
Key points
Acute illnesses account for up to ~50% of all medical consultations at major sporting events, with ~50% of all acute illnesses involving the respiratory system.
Acute respiratory infections (ARinf) account for most of the acute respiratory illnesses in athletes and are caused primarily by viruses.
ARinf involve predominantly the upper airways and two clinical syndromes (ie, acute viral rhinitis/rhinosinusitis with or without systemic symptoms) are responsible for most ARinf in athletes.
Sport and Exercise Medicine clinicians can implement a practical clinical approach to the diagnosis, management, return-to-sport decision making and prevention of ARinf in athletes.
Introduction
The International Olympic Committee (IOC) Medical and Scientific Commission identified ‘protection of the health of athletes’ as an important focus involving prevention,1 management and safe return to sport (RTS) after acute illness in athletes. Management and prevention of acute illness in athletes forms a significant component of the work of Sport and Exercise Medicine (SEM) clinicians at international single-sport2–9 and multisport events such as the Olympics,10–14 Paralympic Games15–17 and Youth Olympics.18 19 Approximately 50% of all medical consultations at these events relate to acute illness in athletes, with the respiratory system consistently the most common organ system affected.4 7 8 11 12 20 21 Acute respiratory illness (ARill) can occur as a result of multiple causes, which can be broadly classified as non-infective or infective. In most studies to date,22 acute respiratory infections (ARinf) in athletes were diagnosed by history and clinical assessment without laboratory confirmation of an infection, or identification of a specific pathogen and are ‘suspected’ ARinf.4 7 8 10 12
The aim of this consensus statement is to provide the SEM clinician with an overview and practical clinical approach to ARinf in athletes. This document forms part 1 of a three-part series, with part 2 focusing on non-infective ARill in athletes23 and part 3 on SARS-CoV-2 infection in athletes.24 The specific focus of part 1 is to review clinically relevant aspects of ARinf in athletes. The first section of this manuscript proposes a set of definitions and classifications of ARinf in athletes to standardise future data collection and reporting. The remainder of this IOC consensus examines a wide range of clinical considerations related to ARinf in athletes: epidemiology, risk factors, pathology/pathophysiology, clinical presentation and diagnosis, management, prevention, medical considerations and risks of illness during exercise, effects of illness on exercise/sports performance and RTS decisions.
The work of this consensus group started in September 2019, before the COVID-19 pandemic. As the pandemic emerged in 2020, the work of IOC consensus group was expanded with the formation of subgroup 7, which was tasked to focus on SARS-CoV-2 infection in the athlete. The focus of this part 1 of the consensus was on all ARinf in athletes, but as new data on SARS-CoV-2 infection in athletes emerged from March 2020, several research findings that are generally applicable to ARinf were identified, and these are included in this part 1 consensus. As indicated, the specific work of subgroup 7 forms a separate IOC consensus on SARS-CoV-2 infection in athletes (part 3).
Methods
The process to generate this consensus statement involved several steps: (1) to identify SEM experts in the field, nomination forms (detailing key publications in the field, clinical experience and professional motivations) were widely distributed by the IOC Medical Commission and Scientific Department to all contacts in the IOC Research Centres for Prevention of Injury and Protection of Athlete Health, National Olympic Committee medical staff in past Olympic Games, and participants of past meetings and conferences such as the IOC World Conference on Prevention of Injury and Illness in Sport and IOC advanced team physician courses; (2) nominations were considered, and members then invited as either ‘core’ or ‘corresponding’ members (‘core’ members coordinated the preparation of specific consensus sections and ‘core’ and ‘corresponding’ members were involved with reviewing literature, collating data and conducting systematic and narrative reviews in six focus areas), the final ‘core’ group included representation from a former Olympic athlete (CM); (3) various areas of ARill were originally identified including ARinf and non-infective ARill such as acute asthma and related conditions, causes of nasal obstruction, and acute nasal/vocal cord dysfunction presenting as ARill; (4) each subgroup held online meetings to discuss broad content and formulate a systematic (with or without meta-analyses) or narrative review(s), and data from these reviews were incorporated into the main consensus documents; (5) the draft sections of the consensus documents were allocated to ‘core’ members. Initial draft sections of the consensus statements were reviewed internally before further discussion and finalisation of the consensus document at a meeting conducted in Lausanne, Switzerland on 11 to 12 October 2021. Final edits were completed in a 3-month period after the meeting, prior to submission of the manuscript.
Terminology, definitions and classification of ARinf in athletes
ARill in athletes, and specifically ARinf, can be categorised based on an anatomical and pathological classification. For the purposes of this consensus document, terminology and anatomical/pathological classifications of ARill and ARinf were agreed on by the consensus group early in the process and finalised after an online meeting in January 2021. Non-infective ARill was defined as an illness not caused by infection from a specific pathogen, by clinical diagnosis or laboratory investigation(s). There are several conditions that cause non-infective ARill and these are comprehensively reviewed in part 2 of the IOC Consensus statement on ARill in athletes.23
Anatomical classification of ARinf in athletes
Due to the structural and functional connection between upper and lower airways, there is a pathological continuum in many conditions causing ARill including allergy, asthma, infection and other inflammatory conditions related to pollution and chemical exposure.25 26 However, the terms ‘upper’ or ‘lower’ respiratory tract disease are still used commonly when referring to both non-infective and infective causes of ARill. In this context, ‘upper’ ARinf refers to symptoms, signs, and pathological features of infective conditions above and including the larynx (nose, sinuses, pharynx, larynx), while ‘lower’ ARinf refers to symptoms, signs, and pathological features of infective conditions below the level of the larynx (trachea, bronchi, lungs and pleura). The consensus group adopted use of the term ‘predominantly’ for upper or lower ARinf, based on the main clinical (cluster of upper or lower symptoms, signs) or pathological features involving the ‘upper’ or ‘lower’ airways.
Pathological classification of ARinf in athletes
Historically, in many studies reporting on ARill in athletes,22 the pathology could not be attributed specifically to an infection or a non-infective cause, and/or these details were not specified explicitly in the study design or methods section. When analysing data from these studies, the consensus group defined the ARill as an ‘undiagnosed’ ARill. In studies where an infection was reported, the infection was often not confirmed and/or the specific viral, bacteriological, or other pathogens causing the infection were not identified. In these cases, the consensus group classified the ARinf as ‘suspected’ rather than ‘confirmed’. For the purposes of this consensus statement, the following broad classification, and methods to diagnose ARinf used in studies to date, were agreed on and applied for this document (table 1). This table, featuring the methods to diagnose and classify ARinf, is adapted from two systematic reviews conducted by specific subgroups.22 27
Classification and methods to diagnose acute respiratory infection (ARinf) in athletes (adapted from Derman et al 22)
A ‘suspected’ ARinf was defined as ARill presenting with general symptoms and/or physical signs suggestive of an ARinf, but where the specific pathogen causing an infection was not confirmed by laboratory testing. In published studies of ARinf in athletes, the following methods were used to classify ‘suspected’ ARinf: (1) self-reported symptoms, coupled with an algorithm that was validated for the diagnosis of ARinf. The validated questionnaires included the Wisconsin Upper Respiratory Symptom Survey-21,28 the Jackson Cold Scale,29 or other questionnaires where the severity of the symptoms was scored to provide a quantitative assessment,30 31 (2) a review of self-reported symptoms of an ARinf by a physician, but without clinical or laboratory evaluation, or (3) clinical diagnosis of an ARinf by a physician, based on history and clinical examination.
A ‘confirmed’ ARinf was defined as an ARinf diagnosed by a physician with laboratory evidence confirming an infection. A ‘confirmed’ ARinf could then be further classified as either: (1) a confirmed ARinf but where the specific pathogen was not identified or (2) a confirmed ARinf where a specific pathogen (predominantly viral and less commonly bacterial) was identified by polymerase chain reaction (PCR) testing on specimens, culture of an organism from specimens, or serology (eg, rise in antibody titres) (table 1).
Pathology and pathophysiology of ARinf in athletes
Pathogens causing ARinf
ARinfs are mostly caused by different viruses, occasionally by bacteria, and rarely by other pathogens (eg, fungal).32 In the general population, a viral aetiology accounts for >80% of all upper ARinf.33–35 At least 10 different respiratory viruses species with hundreds of subtypes cause most ARinf in the general population (table 2), but there are many subtypes and serotypes.34 Clinically non-significant bacterial colonisation can also be combined with viral pathogen identification, as has been shown in 5% to 10% of adults with upper ARinf.35
More common pathogens (viral, bacterial) causing acute respiratory infection in the general population32 34
The specific pathogens causing ARinf in athletes have not been studied extensively, but the same pathogens cause ARinf in athletes as in the general adult population. Prior to the COVID-19 pandemic, rhinoviruses, non-SARS coronaviruses, influenza viruses and RS-viruses were identified as the most frequent pathogens causing ARinf in athletes, but only in a few studies.36–41 Since December 2019, the predominant pathogen causing ARinf in the general population was the novel coronavirus, SARS-CoV-2.
As in the general population, pathogens cannot be detected in all athletes presenting with symptoms of ARinf. Early studies conducted in Australia36 38 reported viral aetiology in one-third of athletes with symptoms of respiratory infection. In contrast, more recent studies from Finland showed a higher detection rate of viral causes (77%) in athletes with symptoms of ARinf.39 40 This higher detection rate, which is similar to reports in the general adult population, may be explained by several factors including: expected viral epidemics of winter season, winter sport disciplines, and methodological variations. In more recent studies four different multiplex PCR panels were used to identify pathogens.32 42 43 These studies indicate that athletes presenting with mild symptoms of respiratory infection are likely to have a viral aetiology. However, more prospective studies in larger athlete populations with a longer surveillance and follow-up time are needed. Bacterial causes of ARinf in athletes are described but are uncommon.44 As in the general population, the cause of ARinf in athletes has also been dominated by SARS-CoV-2 infection since December 2019.45–49
Pathophysiology of ARinf
Respiratory pathogens circulate commonly in all age groups by an efficient person-to-person transmission. The transmission pathways are dependent on the pathogen and include aerosol, droplet, as well as direct or indirect contact transmission.50 A detailed discussion of the pathophysiology of respiratory tract infection by viral and bacterial pathogens is beyond the scope of this consensus, and has been reviewed elsewhere.51 52 In general, on entry of the respiratory tract, viruses invade the respiratory epithelium, gain entry to the cells, elicit an inflammatory response, replicate, cause cellular death, and subsequently shed and transmit via respiratory secretions.51 53 Bacteria, such as those causing acute pharyngitis, attach to and, in the case of group A beta-haemolytic streptococcus, invade the mucosa of the respiratory tract, elicit an inflammatory response, cause cell death and may form an adherent exudate.51
The pathophysiological mechanisms responsible for the common general symptoms of ARinf are related to a non-specific acute phase response, as well as local tissue injury by the pathogen. In the early stages of the infection, the non-specific acute phase response results in the systemic release of several cytokines, which collectively are an important component of the host defence mechanism.52 Acute phase reactants (APR) are a heterogeneous group of plasma proteins that increase or decrease in concentration in response to inflammatory stimuli, including acute infection. APR such as C reactive protein (CRP) and procalcitonin (PCT) can be measured in the laboratory and are useful markers of inflammation associated with ARinf. Their response is proportional to the severity of the inflammatory stimulus of the ARinf.54 In most ARinf, inflammatory mediators such as prostaglandin and bradykinin are responsible for local symptoms (rhinorrhoea and nasal congestion), while cytokines are responsible for systemic symptoms (fever, chills, headache, myalgia).52 The clinical relevance of the acute phase response is that symptoms of ARinf caused by acute phase inflammatory mediators are non-specific and common to infections caused by different pathogens. As a result, symptoms of ARinf are generally non-specific and cannot be used to diagnose the underlying pathogen causing an ARinf. However, these symptoms (type, duration and severity) are related to the magnitude of the inflammatory response and can indicate the severity of the ARinf.54
Incubation period and infectiousness are two pathophysiological features of ARinf that have specific clinical relevance to the SEM clinician. The incubation period (defined as the time from pathogen exposure to onset of signs and symptoms) is pathogen-dependent, and varies from 1 to 14 days (eg, rhinovirus=1–3 days; adenovirus=7–13 days and SARS-CoV-2=2–14 days).33 55 56 Knowledge of the incubation period is important for the SEM clinician because it informs clinical decision making when controlling viral epidemics within teams.39 40
Until recently, viral shedding time was used to determine the duration of infectiousness, but this concept is changing due to the increased knowledge of SARS-CoV-2. Shedding time of respiratory viruses can range from a few days up to weeks, but the time of infectiousness during the detection of viral agent is often not known.57 The risk of viral transmission is highest during the first 3–4 days of the infection and in the case of SARS-CoV-2, up to 48 hours before the onset of symptoms. Infectiousness is an important determinant in decision making on the duration of quarantining infected athletes, and when an athlete can return to team practice, locker rooms and shared transportation.
Potential complications in other organ/organ systems, other than the upper respiratory tract, that can be associated with an ARinf
Although the majority of ARinf only result in pathology within the upper respiratory tract, there are potential regional systemic and complications in other organs/organ systems caused by respiratory viral pathogens causing ARinf (online supplemental table S1). The risk and type of complications vary according to the host and the pathogen.
Supplemental material
A systematic review of potential multiorgan complications of ARinf in athletes was commissioned and then undertaken by a subgroup of the IOC Consensus group. This review identified too few studies to analyse, therefore, data in this area are currently very limited. Although apparently very rare, particularly in younger populations, potential complications are of clinical relevance to athletes with ARinf because they can indicate more extensive or severe disease. This aspect was highlighted by studies during the recent COVID-19 pandemic indicating that, for example, reported cardiovascular complications such as myocarditis/pericarditis that can occur in athletes with SARS-CoV-2 infection. Initial studies, with small sample sizes in selected athletic cohorts, showed a high prevalence of myocarditis/pericarditis after SARS-CoV-2 infection,58 59 but in several larger studies this complication was found to be rare (<3% or less).60–62 Thus, although potential complications of ARinf affecting multiple organ systems are rare, the SEM clinician should consider these complications as they may predispose athletes to an increased risk of adverse medical events during return to full training and competition.
Incidence of ARinf in athletes
A systematic review and meta-analysis undertaken by a subgroup of the IOC Consensus group determined the incidence per 1000 athlete days of ARill, and specifically ARinf, in athletes.22 This review included subanalyses based on the anatomical and pathological classification of ARill, and specifically ARinf in athletes. Data included athletes at any level of performance (elite/non-elite), aged 15–65 years. Analysis was done from data in 124 original research articles (n=128 360 athletes) published between January 1990 and July 2020.
Incidence of ARinf in athletes
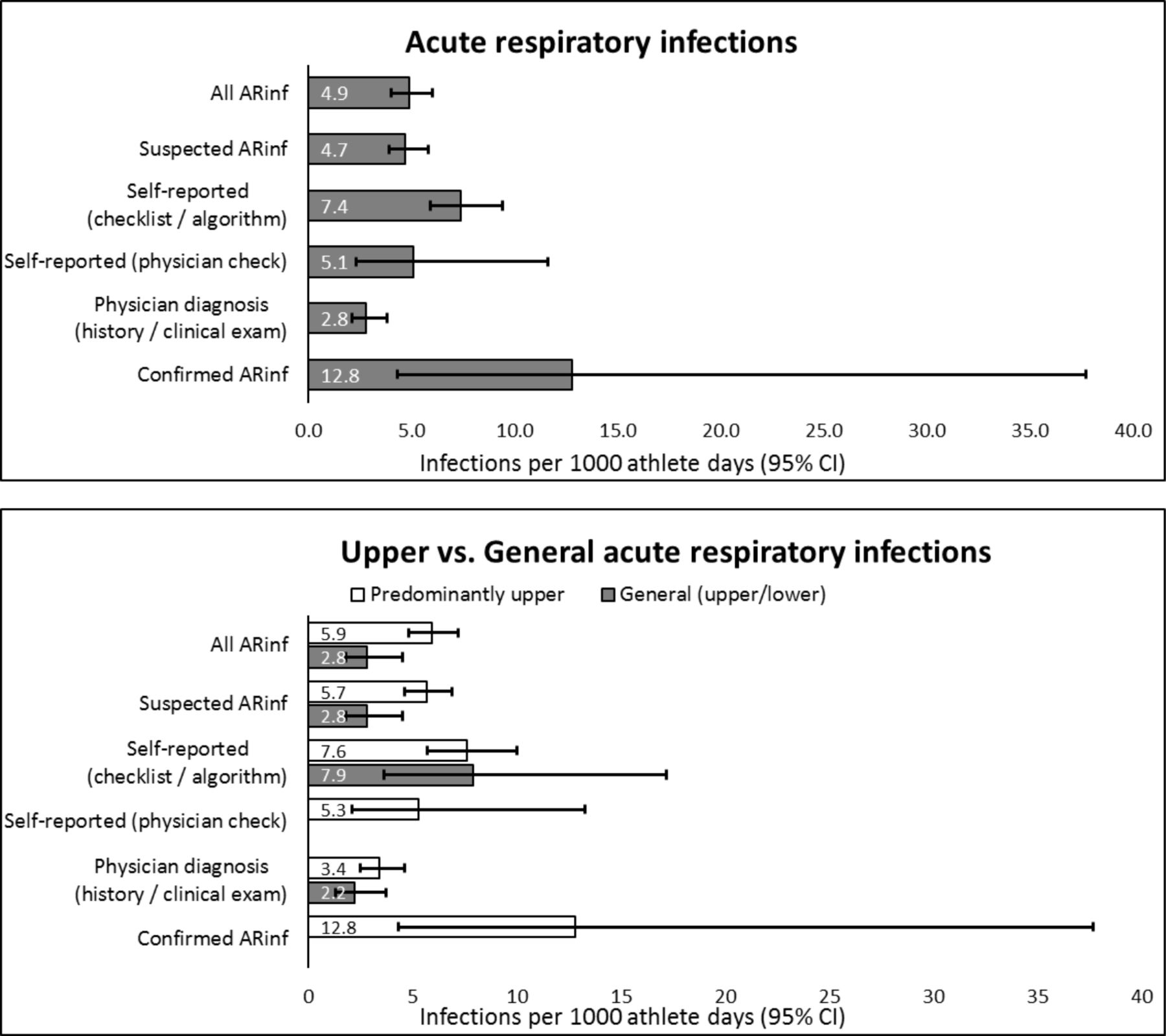
The incidence of ARinf by pathological and anatomical classification and by method of diagnosis is summarised in figure 1.

The incidence (per 1000 athlete days; 95% CIs) of acute respiratory infection (ARinf) by pathological and anatomical classification and by method of diagnosis (adapted from Derman et al 22).
The overall pooled incidence of all ARinf (both suspected and confirmed) in athletes was 4.9 per 1000 athlete days,22 and the incidence was twofold higher for predominantly upper ARinf (5.9 per 1000 athlete days) versus general (defined as combined upper and lower ARinf) ARinf (2.8 per 1000 athlete days). There was a higher incidence of ARinf in athletes with confirmed ARinf (pathogen identification) compared with all other categories of suspected ARinf. Studies in athletes with confirmed ARinf (pathogen identification)39 40 were conducted in a selected cohort of elite athletes during international winter sport competition and used a different more sensitive definition of ARinf (any symptom or viral pathogen that was detected). Although the incidence of ARinf was higher in these studies, there were wide 95% CIs, and this estimate was not significantly different from the incidence of ARinf in other studies.22 A higher incidence of ARinf in non-elite athletes (8.7 per 1000 athlete days) compared with elite athletes (4.2 per 1000 athlete days) was reported in the recent review. However, in a winter sport team setting, a seven-fold higher incidence of ARinf was evident in a group of elite athletes compared with age-matched controls exercising less than 6 hours per week and a control group of non-athletes.39 The study was conducted during a winter viral epidemic where athletes were asked to report even mild respiratory symptoms, which may explain the difference in findings.
Clinical point/s: How common are acute respiratory infections (ARinf) in athletes?
The general incidence of ARinf in athletes equates to ~1.8 ARinf per athlete per year (in comparison to ~2.3 in the general population).
There is a high incidence of predominantly upper ARinf.
Elite athletes have a lower incidence of ARinf than non-elite athletes.
The incidence of suspected ARinf is similar across methods of diagnosis, indicating that Sport and Exercise Medicine clinicians can confidently use validated questionnaires and checklists to screen athletes for suspected ARinf.
There appears to be a higher incidence of confirmed ARinf with pathogen identification compared with suspected ARinf, but this outcome requires confirmation in future studies with larger cohorts.
Risk factors associated with ARinf in athletes
A comprehensive review of the risk factors and biomarkers for both suspected and confirmed ARinf (n=24 studies) has been published by an IOC consensus subgroup.63 This review included 48 studies (19 390 athletes) and the majority (71%) of studies were self-reported ARill in athletes. Sub-analyses included the pathological classification of ARinf and methods used to diagnose suspected ARinf. A summary of risk factors with a strong positive association to a high incidence of confirmed ARinf or suspected ARinf is presented below.
Clinical point/s: What are the risk factors associated with acute respiratory infections (ARinf) in athletes? (strong positive associations)
Endurance sports versus other sports.
Winter vs other seasons.
Training variables (high intensity training, increased training load, training monotony, lack of tapering).
Training at altitude.
Competition periods.
Travel (during and following long-haul international travel).
Vitamin D deficiency.
While other possible risk factors for ARinf were identified in this review, conflicting evidence limited conclusions to be drawn, and further research is warranted.
Clinical presentation and diagnosis of ARinf in athletes
Introduction
Athletes with ARill who present with typical respiratory symptoms are traditionally categorised according to the predominant anatomical area affected: upper respiratory tract, lower respiratory tract/regional symptoms and systemic (whole body) symptoms. There is considerable overlap between symptoms of non-infective ARill and ARinf, but discrete symptoms and symptom clusters are more typical of ARinf than non-infective ARill (online supplemental table S2). Associated systemic symptoms, or other symptoms of multiorgan involvement, can also indicate ARinf rather than a non-infective cause of ARill (online supplemental table S2).
The clinical presentation of an ARinf is highly variable, and is influenced by several pathogen and host factors,64 and ranges in severity from mildly symptomatic to life-threatening and death.34 Explanations for the non-specific clinical presentation of ARinf include: (1) overlapping of some symptoms and clinical signs of ARinf and non-infective ARill, (2) the same pathogen can cause variable clinical presentations of ARinf in a group of athletes, (3) different pathogens can cause a similar ARinf clinical syndrome in the same athlete,34 and (4) many symptoms are the result of a non-specific acute phase response, which are common to all infections.52 Therefore, an ARinf caused by a specific pathogen cannot be diagnosed by typical symptoms and clinical signs (clinical syndrome) alone, and laboratory tests are required for formal identification.
Asymptomatic ARinf in athletes
Several pathogens can infect athletes, but the athlete may remain asymptomatic.64 For example, in a review of adult human influenza volunteer challenge studies in the general population, 30% of influenza virus infections were asymptomatic.65 In one study among athletes during the Nordic Ski World Championships, viral infections were asymptomatic in 8% of athletes of Team Finland, 19% of staff members and 22% of controls.39 Data from recent studies during the COVID-19 pandemic indicate that about 20% to 30% of SARS-CoV-2 infections in athletes are asymptomatic. Asymptomatic infections are important in the SEM context because: (1) there may be a risk, although likely to be very small, of adverse medical events during exercise, (2) the potential negative effect of asymptomatic ARinf on exercise/sports performance in athletes is unclear, but again is likely to be low and (3) there is a potential risk of transmission within teams and sports events.40 The importance of asymptomatic ARinf in transmission chains has been highlighted by the COVID-19 pandemic.
Clinical syndromes of ARinf
A clinical syndrome is defined as a combination of symptoms and signs (sometimes also referred to as a clinical phenotype) that together represent a disease process. Defining and diagnosing the clinical syndrome of ARinf, plotting the time course by monitoring the progress of the symptoms and signs, and knowing the pathogen, are all important in guiding the SEM clinician in management of athletes with ARinf. These parameters are relevant to identify potential detrimental effects of ARinf on exercise and sports performance and mitigate the risk of medical complications when resuming exercise training.
Symptomatic ARinf typically presents with mild, non-specific localised upper respiratory tract symptoms such as sore throat, sneezing, rhinorrhoea and nasal congestion/stuffiness.34 Cough and hoarseness are variable, and can indicate either upper or lower respiratory tract involvement. Primary symptoms can emerge initially or develop after several days.34 Both pathogen and host dependent symptoms of ARinf typically peak within 2–3 days after onset, are self-limited and resolve by 7–10 days in adults, both in the general population34 and in athletes.27 The duration of ARinf symptoms can be used as an indicator of severity of ARinf. Indicators of a more severe infection are: (1) regional symptoms (headache), (2) systemic symptoms (malaise, fever, myalgia and fatigue), (3) prolonged symptoms (lasting >7 days), (4) symptoms that increase rather than decrease in severity over time, (5) the development of new symptoms over time and (6) specific symptoms associated with multiorgan (non-respiratory) involvement.
Classification of clinical syndromes of ARinf
Clinical syndromes of ARinf can be based on a broad anatomical classification (predominantly upper or lower respiratory tract) and underlying pathology. Although this scenario is rapidly changing, most SEM clinicians do not yet have routine access to laboratory testing methods to identify specific pathogens causing ARinf to guide their clinical decision making. In this IOC consensus, we propose a classification of the clinical syndromes of ARinf in athletes, which has been adapted from Treanor.34 This classification is also based on a clinical presentation of an ARinf predominantly affecting the upper or the lower respiratory tract.
Clinical point/s: Classification of clinical syndromes of acute respiratory infections (ARinf) in athletes
Predominantly upper ARinf (>90% of all ARinf)
Acute rhinitis and/or additional features of rhinosinusitis and rhinopharyngitis without regional or systemic symptoms and signs (‘common cold’).
Acute rhinitis and/or additional features of rhinosinusitis and rhinopharyngitis with regional or systemic symptoms and signs (‘influenza-like’ syndrome).
Acute pharyngitis.*
Acute laryngitis.*
Acute laryngotracheobronchitis.*
Predominantly lower ARinf (<10% of all ARinf)
Acute tracheobronchitis.*
Acute bronchitis/bronchiolitis.*
Acute pneumonia.
Diagnosing the clinical syndromes of ARinf in athletes
Clinical diagnosis of a suspected ARinf (history and clinical examination)
Awareness of the current epidemics and a careful history of symptomatology with a clinical examination is recommended to identify the clinical syndromes of an ARinf. The case definition for each clinical syndrome as well as the broad clinical features of each clinical syndrome are summarised in table 3.
Case definitions and clinical features of acute respiratory infections (ARinf) clinical syndromes in athletes
Special investigations to confirm the diagnosis of an ARinf (no pathogen identified)
APRs are a heterogeneous group of plasma proteins that increase or decrease in concentration in response to inflammatory stimuli, including acute infections. There are several clinically important APR’s and their potential diagnostic value has been reviewed.54 66 Non-diagnostic specific markers of infection that the SEM clinician can consider as diagnostic markers are erythrocyte sedimentation rate (ESR), CRP and PCT. CRP is a better measure of the acute-phase response, more sensitive than ESR, and the preferred marker of infection. The clinical relevance of CRP is that, in response to ARinf, CRP concentration begins to rise after 12 to 24 hours and peaks within 2–3 days (50–100 mg/L). Extremely high increases in CRP (>500 mg/L) are more common in bacterial infections and severe systemic infections.54 Therefore, measurement of CRP concentration in an athlete with suspected ARinf can be useful to confirm the presence of an infection.
PCT is less commonly measured but can be a useful differential biomarker for bacterial (vs viral) ARinf. PCT has been used in the early identification of bacterial lower ARinf, and to stratify patients with a higher risk of complications.54 Finally, a full blood count (FBC) and differential white cell count can also be of value to distinguish non-infective ARill from ARinf in an athlete.54
Special investigations to identify the causative pathogen in ARinf
There are several methods to detect the pathogens causing the ARinf by collecting a nasopharyngeal mucosal sample with a flocked nasal swab, obtaining a sputum sample, or taking a blood sample for antibody testing.67 Viral and bacterial culture remains the ‘gold standard’ for pathogen identification. For viral diagnostics, the traditional diagnostic method of culture has, in the last two decades, largely been superseded by PCR tests.68 Antigen tests have proven to be useful in virus detection and control during the COVID-19 pandemic.69 However, antigen tests are not able to detect all respiratory viruses, and their sensitivity in adults may be as low as 30%.70 71 The commercial multiplex respiratory PCR tests are particularly useful as they can detect the genetic material (nucleic acids) of up to 16–18 respiratory viruses concurrently from a single mucus sample.72–74 Additionally bacterial targets such as Streptococcus pneumoniae, Mycoplasma pneumoniae, Chlamydia pneumoniae, Haemophilus influenzae are also included in some commercial PCR kits.75 76 It is important to note that a positive PCR test does not necessarily reflect active virus replication, and associations between viral load and infectiousness remain unclear.33 77 Sensitive and specific molecular test platforms, as well as fast, automated molecular point-of-care tests are becoming increasingly applicable for clinical use in SEM at international competitions such as the Olympic and Paralympic Games.39 40 78 The need for routine expensive comprehensive pathogen identification of ARinf is debatable as a specific therapeutic intervention is only available for influenza. However, the COVID-19 pandemic highlighted the importance of early recognition of symptoms, and early and precise viral pathogen identification so that athletes can be isolated quickly and quarantined to prevent spread of infection.39 40
Special investigations to assess for regional and systemic involvement (multiorgan involvement) of ARinf
In suspected cases of more severe and complicated ARinf, a range of special investigations can be considered to confirm the diagnosis of multiorgan involvement. The choice of special investigations will depend on the suspected involvement of the organ system/s involved. Some of the more common special investigations that the SEM clinician can consider in cases of moderate to severe ARinf in athletes are listed (online supplemental table S4). The consensus group recommends that confirmation of the diagnosis, determination of ARinf severity as well as management of regional and multiorgan complications, are best conducted in conjunction with specialist clinician colleagues.
Determining the severity of ARinf in athletes
There is substantial variability in the severity of illness when the same pathogen causes ARinf in multiple athletes, or when different pathogens cause ARinf in one athlete. The severity of an ARinf in athletes is dependent on numerous factors including the pathogen and host characteristics, which may be genetic or acquired. The following host (athlete) characteristics may predispose an individual to a more severe ARinf; older age, male sex, obesity and comorbidities (immune system dysfunction, immunosuppression, use of immune suppressive medications (eg, Transplant Games), hypertension, cardiovascular disease, cancer, chronic lung disease including asthma, diabetes mellitus) and Para athletes with spinal cord lesions and those of high needs. The risk of more severe ARinf is also related to vaccination status and exposure to a higher pathogen (viral) load.
Determination of what is considered a ‘more severe’ ARinf is derived from studies in the general population, particularly during the COVID-19 pandemic. In the general population, the definition of the ‘severity’ of an ARinf is based on parameters such as the presence or absence of severe symptoms (severe dyspnoea at rest), extremely low oxygen saturation, hospital admission, high care or intensive care unit admission, presence of respiratory distress requiring mechanical ventilation or death.79 However, most athletes with ARinf do not have extremely low oxygen saturation, do not require hospitalisation, and would be classified with an ARinf of mild to moderate severity. Currently, there are no validated tools, algorithms or scoring systems to differentiate severity of ARinf in athletes, who fall into the majority ‘mild to moderate severity’ category.
For the SEM clinician, it is important to assess the severity of ARinf in athletes in this ‘mild to moderate’ category of ARinf because this can: (1) influence the risk of medical complications during exercise after infection, which then guide clinical decision making in RTS following an ARinf, and (2) determine potential detrimental effects on exercise and sports performance post-infection. This IOC consensus group, by expert opinion, suggests that several parameters on clinical presentation (history and findings on clinical examination), as well as results of special investigations, can be useful indicators to stratify the severity of an ARinf in an athlete (table 4). We suggest that this clinical approach can be used in the initial assessment of athletes with ARinf and can form the basis of RTS decision making. However, we recognise that validation of these indicators has not been established fully, and further research is needed.
Indicators of the severity of an upper ARinf in athletes (history, physical examination and results of special investigations)
Principles of management of ARinf in athletes
The two most common clinical syndromes of ARinf that an SEM clinician will manage routinely are the ‘predominantly’ upper ARinf syndromes of: (1) acute rhinitis/rhinosinusitis/rhinopharyngitis (‘common cold’, ‘coryza’, ‘viral upper respiratory infection’) and (2) acute rhinitis/rhinosinusitis/rhinopharyngitis with systemic symptoms/signs (‘influenza-like’, ‘influenza’ syndrome). In this section, we focus on the principles of management of these two clinical syndromes. Other clinical syndromes of upper ARinf (acute laryngitis and tracheobronchitis) are less common and lower ARinf syndromes in athletes are rare.
There are seven main principles of management of ARinf that SEM clinicians can consider.
Clinical point/s: Seven principles of management of acute respiratory infections (ARinf) that Sport and Exercise Medicine clinicians can consider
General non-pharmacological treatment to support recovery and the immune response.
Nutritional, immune or probiotic supplementation.
Pharmacological treatment of symptoms.
Antiviral agents (for specific cases).
Antibacterial agents (for specific cases).
Management of the athlete with suspected multiorgan involvement or other complications (if present).
Decisions to allow an athlete with an ARinf to return-to-sport, including the initial decision to resume training (return-to-participation), and the subsequent decision to return to full exercise/sport performance.
These principles will be briefly reviewed, but a detailed summary, including the specific treatment, the advice/administration dose, as well as evidence of the effect of the treatment and potential side effects unique to upper ARinf in athletes, is presented in table 5.
A summary of the principles treatment of upper acute respiratory infection (ARinf) in athletes
General treatment to support recovery and the normal immune response
Rest/training reduction/restriction
In an athlete presenting with ARinf, one of the first management decisions the SEM clinician will make is whether rest, training reduction or restriction of training is required during the acute phase of the ARinf. The following recommendations are based on the severity classification of the upper ARinf (table 4). In mild/moderate ARinf, normal daily activity is generally allowed. In most cases symptoms of ARinf resolve within 1–3 days, but it is advisable to perform a daily checklist before either starting or resuming exercise training (checklist 1: table 6).
Checklists before starting or resuming exercise training in an athlete with acute respiratory infection (ARinf)
In general, once localised symptoms have either resolved or are very mild, and if there are no items flagged in the checklist, the athlete can be advised to perform an exercise challenge test (self-administered field test by the athlete/coach/support staff or a laboratory test). In severe ARinf, bed rest is recommended until regional and systemic symptoms have resolved, and there is no evidence of active multiorgan involvement, after which normal daily activity is allowed. For severe ARinf, the athlete is advised to consult an SEM clinician who will perform a checklist before giving advice of resuming exercise training (checklist 2: table 6). Based on the outcome of the checklist, a decision can be made to conduct an exercise challenge test.
General nutrition
It is well known that general nutritional status influences both their susceptibility to infection and response to infection.80 81 Thus, adequate energy availability as well as micro-and macronutrient intake are important for immune health in athletes with ARinf.80–82
Hydration
Maintenance of fluid intake during an ARinf is important to ensure that mucous membranes remain moist, to their defensive function and alleviate acute symptoms.82 However, there is no evidence to support increasing fluid intake beyond the maintenance of normal hydration.
Nasal saline irrigation
Nasal saline irrigation may relieve symptoms of ARinf, but data are limited.
Nutritional/immune supplements and/or probiotics
The use of specific nutritional or immune supplements as well as probiotics for athletes with ARinf is common and has a high cultural influence and community support. In general, scientific evidence to support the widespread use of these agents is lacking (table 5). Some studies report that nutritional supplements have some benefit in reducing the duration of symptoms or the recovery time of ARinf and these include zinc,83 84 Vitamin C and Vitamin D but only in vitamin deficient athletes. Although supplementation with herbal medicines is popular there is only low level evidence that some may be beneficial (table 5) including BNO1016, cineole and andrographis paniculata SHA-10 extract, pelargonium sidoides extract85 86 and Echinacea.87 Probiotics may help reduce the number of and the mean duration of upper ARinf,88 but the quality of the evidence is low. In summary, evidence for these therapies is generally of low quality, remains mixed and further studies are required.
Pharmacological treatment of symptoms
Treatment of symptoms is an important component of the clinical care of athletes with ARinf. Rhinorrhoea may impair athletes’ well-being and physical performance and swollen mucous membranes in the nasopharynx may give rise to obstruction and predispose athletes to secondary otitis media and/or sinusitis. There are several options for pharmacological treatment of symptoms of ARinf in athletes including analgesics, non-steroidal anti-inflammatory drugs (NSAIDs), mucolytics, corticosteroids, decongestants, antitussive agents, antihistamines, and combination drugs. Options for the pharmacological treatment of symptoms, and evidence for using these medications during the acute phase of upper ARinf, is summarised in table 5.
These treatments are frequently available as over-the-counter drugs in most countries, and therefore, are not well controlled by SEM clinicians and may cause side effects in athletes and can lead to doping violations. For example, NSAID’s can lead to gastric side effects, may increase risk of bleeding, can have renal side effects, and by masking symptoms can lead to a false positive perception of the clinical status of an athlete.
Antiviral agents
Antiviral treatment is available only for influenza viruses. SEM clinicians should be aware of the prevailing viral epidemics and can confirm influenza virus infection by PCR when suspected. In cases of confirmed influenza infection, antiviral treatment with oseltamivir or zanamivir should be started soon after the onset of the symptoms,89 but side effects of these drugs must be considered (table 5). If an athlete has been in close contact with influenza virus, prophylaxis treatment can be considered. Point-of-care-testing enables prophylaxis with oseltamivir for those predisposed to influenza virus infections, for example, living in same household or travelling in the same flight or carpool (https://www.cdc.gov/). Isolation of infected team members should be initiated after the onset of symptom/s and continued for 3–4 days, that is, the most infectious period.90
Antibacterial agents
Details about specific antibacterial (antibiotic) therapy for bacterial infections is beyond the scope of this consensus. In general, the place for general antibacterial agent use in athletes with upper ARinf is limited. Although antibiotics are widely used in the treatment of uncomplicated viral ARinf among athletes, they are not effective against viruses and can have negative side effects91 (table 5). It is recommended that antibiotic treatment is only considered in cases where there is clear identification of the (detected or suspected) infectious agent. In some cases of acute tonsillitis with an exudate, antibiotic treatment may be indicated if there is a strong clinical suspicion of a bacterial infection, but identification of a bacterial cause is still preferable. In most cases presenting as acute pharyngitis, a clinical diagnosis of a bacterial infection is almost impossible. Although antibiotics are only effective against bacteria, they are sometimes used to prevent bacterial superinfections (and re-infections).
Management of the athlete with suspected multiorgan involvement or other complications
An ARinf can lead to a variety of medical complications, even fatal, because of multiorgan involvement. Potential respiratory system complications or complications in other organs and organ systems (online supplemental table S1), and special investigations to diagnose these complications (online supplemental table S4) can be considered. Although these complications are rare, it is important that the SEM clinician considers them, particularly in athletes presenting with moderate or severe ARinf. Diagnostic work-up and management of athletes with suspected multiorgan involvement should be conducted in conjunction with appropriate specialist colleagues.
RTS considerations following ARinf in athletes
Terminology and key concepts related to the RTS decision
Traditionally, the point at which an athlete fully recovered from an injury or illness and returned to full participation at the pre-injury or illness level has been termed either return-to-play (RTP) or RTS. The first key concept is that the term RTP has mostly been used in the context of team rather than individual sports. In this consensus document, we agreed to use the term RTS because this term is more inclusive, is relevant to all sports, and was the recommended term by a 2016 consensus statement on RTS after injury.92
A second important concept is that RTS must be viewed as a continuum rather than a single time point at the end of recovery from an injury or illness. In the 2016 consensus on RTS, three time points of RTS on a continuum were suggested: return to participation, RTS and return to performance.92 These elements emphasise a graded, outcome-based progression to RTS that can be applied for any sport. For the purposes of this consensus, the following terminology and definitions will be used: (1) Return-to-participation (alternatively return-to-training) is defined as ‘the time point (day from onset of illness) when an athlete resumes with the first training/exercise session after an ARinf’, and (2) RTS is defined as ‘the time point (day) when an athlete has progressed to the same pre-illness level of sport participation (sport performance) or exercise type, intensity, duration and frequency (exercise performance)’. The RTS process may progress rapidly from return-to-participation to RTS (from 1 day to a few days) or evolve gradually and progressively over a longer time (few days to weeks). The rate of progression depends on several factors, including the severity of the ARinf, evidence of associated medical complications in other organ systems, normal responses to progressive increases in training load, and the presence of other modifiers that are part of a complex decision-making process and framework for RTS decisions.
The third concept is that the consensus group broadly adopts the Strategic Assessment of Risk and Risk Tolerance (StARRT) framework for RTS decisions.93 The principle of the StARRT framework is that the RTS decision making process involves three important steps: (1) assessment of health risk, (2) assessment of activity risk, and (3) assessment of risk tolerance through modifiers such as the need/desire for an elite athlete to progress to RTS more rapidly.93 The final general concept is that, as for injuries, the final clearance to RTS after an ARinf is a shared-decision-making process that considers physical, psychological and social factors (biopsychosocial model).92
The scientific basis for RTS decisions after an ARinf in athletes
Even though the RTS clinical decision-making process is very common and important for the SEM clinician, there is little research available to support a sound scientific approach to RTS after an ARinf. Historically, RTS decisions following an ARinf were guided by expert opinion to follow the ‘neck check’ rule.94 95 Subsequently, other RTS guidelines have been published,96 97 including several recently published expert opinions that mainly focused on cardiovascular concerns following SARS-CoV-2 infection in athletes.62 98–103 These ‘expert opinions’ were initially based on no data to support the guidelines, but recently some data became available.104–106 The more recent guidelines were only for athletes with SARS-CoV-2 infection and did not focus on all ARinf (irrespective of the pathogen responsible for the ARinf). They have not consistently considered the key concepts and the three steps in the RTS decision making process, as discussed above.
A systematic review with a meta-analysis was commissioned for this consensus statement to evaluate the scientific evidence for RTS decision making after ARill. Specifically, the aims were to determine the days until RTS after ARill, % of time loss ARill (ARill resulting in >1 day lost from training/competition), and symptom duration (days) of ARill in athletes.27 This review included published studies up to August 2021 before any data on SARS-CoV-2 in athletes became available, identified a total of 54 studies representing 31 065 athletes. Only four studies reported actual days until RTS following ARill, ranging from 0 to about 8 days. The mean symptom duration for all ARill was 7 days. Notably the pooled frequency (%) of ARill resulting in >1 day lost from training/competition was ~20% indicating that in most cases athletes continued training or competing. Consequently, athletes and coaches can be reassured that most ARill either do not interfere with training, or only result in a short period of interrupted or no training. This is consistent with the observation that most (>80%) ARinf are mild, self-limiting and of short duration. Future studies are needed to obtain detailed clinical, laboratory and specific pathogen data on ARinf to customise RTS. The remaining 20% of athletes who have more moderate or severe disease may be at increased risk of adverse medical events during exercise when they RTS.
Guidelines for RTS of an individual with ARinf
We recommend a stepwise RTS clinical decision-making process that can be applied to all athletes with ARinf, irrespective of the pathogen involved. The recommendations are based on the StARRT framework93 and involves the following four stepwise assessments: (1) severity of the ARinf based on symptoms, (2) health risk based on history, clinical assessment and special investigations (where indicated), (3) activity risk (risk of adverse medical event during exercise) and (4) risk tolerance. This stepwise assessment and decision making algorithm is summarised in figure 2.

{kind=link}
{kind=link}
Summary of the RTS clinical decision-making process for athletes with acute respiratory infection (Arinf). *Reassignment of severity categories can take place after clinical assessment and special investigations (criteria in table 4). Strategic Assessment of Risk and Risk Tolerance framework for return-to-play decision making.93 CPET, cardiopulmonary exercise testing; CRP, C reactive protein; RTS, return-to-sport; SEM, sport and exercise medicine.
Step 1: assessment of infection severity based on symptoms
The purpose of the initial assessment of ARinf severity, based on symptoms, is to determine the degree to which detailed subsequent assessments of risk, activity risk and risk tolerance should be undertaken. The principle is that not all athletes with ARinf require a full medical assessment and a battery of special investigations. For example, asymptomatic and minor ARinf are successfully self-managed by many athletes and coaches. Recently, during the COVID-19 pandemic, most guidelines recommend a RTS decision tree should be based on an initial determination of severity of ARinf.62 98–103 However, there is no consensus on a severity classification to use in athletes with ARinf. We propose criteria to classify the severity of ARinf in athletes based on their initial presenting symptoms into four categories: (1) asymptomatic ARinf (positive test or high risk of exposure but no symptoms), (2) mild ARinf, (3) moderate ARinf and (4) severe ARinf (table 4: symptoms). Based on this classification, further decision making on RTS (steps 2–4) is recommended (figure 2).
Step 2: assessment of health risk (‘tissue health’)
The purpose of the assessment of risk is to determine the risk of an adverse medical event when exercise continues during an ARinf or resumes after an ARinf. The elements of the assessment are the medical history, findings on a clinical assessment, and results of selected special investigations. It is criteria-based and the need for the elements of the assessment are based on the severity of the ARinf, and individual athlete risk factors associated with more severe ARinf.
Asymptomatic and mild ARinf
In the case of athletes with asymptomatic or mild ARinf, we recommend that the assessment of health risk be self-administered or administered by the coach/support staff. Athletes with asymptomatic or mild ARinf are encouraged to complete a daily checklist (table 6: checklist 1) before proceeding to step 2 (assessment of activity risk). If no chronic conditions or no symptoms in the checklist are present, the athlete can continue with a self-administered or coach-administered exercise challenge test. If chronic conditions or symptoms in the checklist are present, it is recommended that the athlete consult with a physician or healthcare professional to reassess the severity of the ARinf and be fully evaluated for moderate or severe ARinf.
Moderate or severe ARinf
The RTS process for moderate or severe ARinf should be under the care of a physician or other healthcare professional. A more detailed history and a full clinical assessment can be considered before return-to-participation for all athletes with moderate ARinf. In cases of severe ARinf a more detailed history and a full clinical assessment by a physician is strongly recommended. Special investigations/laboratory tests are generally not required for athletes with mild ARinf (except on an individual basis for athletes with risk factors that are associated with more severe ARinf). Basic laboratory tests for non-specific systemic involvement (eg, CRP and FBC) can be considered in athletes with moderate ARinf, while more extensive special investigations/laboratory tests are recommended in severe ARinf. The types of investigations are determined by the suspected organ involvement (online supplemental table S4). On completion of the risk assessment, the physician can re-assign the risk category (figure 2).
After the risk assessment, as for asymptomatic or mild ARinf, we recommend that the physician or healthcare professional perform a checklist before an athlete performs the exercise challenge test (table 6: checklist 2). If no abnormalities are identified by these checklists, the athlete can undergo a supervised laboratory-based exercise challenge test.
Step 3: assessment of activity risk (risk of adverse medical event during exercise)
The assessment of activity involves: (1) determining the physiological demands that exercise/sport will place on organ systems when training resumes and (2) a continual assessment of the response of the athlete as training progresses. The first step in the assessment of activity risk is to perform a graded exercise challenge test. The specific outcomes are to determine if there are any abnormal symptoms, clinical signs or laboratory-measured responses to the exercise challenge (during, immediately after or for 24 hours after the test).
Asymptomatic and mild ARinf
In cases of asymptomatic or mild ARinf, the exercise challenge test may be a sport-specific field (or laboratory) test that is conducted either by the athlete, or in conjunction with the coach/strength and conditioning staff (box 1).
Guidelines to performing an exercise challenge test in an athlete after an acute respiratory infection (ARinf)
1. Self-administered or coach/support staff administered exercise challenge test
This test can be administered by the athlete themselves or a coach/trainer/support staff.
Always start by performing a pre-exercise checklist based on symptoms (table 6—checklist 1).
Select a suitable field-based test (eg, a standard warm-up exercise session, standard walk/jog/cycle/swim).
Perform the exercise test as follows:
Choose a moderate exercise intensity (60%–70% of normal exercise intensity).
Assess your response (how you feel) after 10–20 min of exercise.
Monitor for symptoms during exercise.
Discontinue the exercise challenge test if any of the following symptoms develop during exercise (excessive fatigue/tiredness, shortness of breath/breathlessness, chest pain/discomfort, dizziness, palpitations/racing heart (faster than normal, eg, on heart rate monitor), muscle/joint pain, higher level of effort for the same past exercise load and ‘not feeling well’)—consult with a medical doctor if any these symptoms develop.
Monitor for the same symptoms as above (with the addition of very dark brown/red urine after exercise) immediately after exercise and 24 hours after exercise - consult with a medical doctor if any of these symptoms develop.
2. Laboratory-based exercise challenge test
The laboratory test is administered by a health professional in a laboratory setting under supervised conditions.
The health professional first performs the pre-exercise checklist based on symptoms, clinical signs and the results of special investigations (table 6—checklist 2).
Select a suitable standardised laboratory test (eg, Modified Bruce protocol).
Select the special investigations to be performed before, during and/or after the exercise challenge test.
Rating of perceived exertion (RPE), rating of perceived breathlessness (RPB), heart rate and blood pressure response to exercise—recommended.
Exercise ECG: moderate ARinf (based on clinical suspicion); severe ARinf (recommended).
Pre-exercise and postexercise pulmonary function testing (decision based on clinical suspicion).
Other special investigations—based on clinical suspicion.
Perform the exercise challenge test as follows:
Perform measurements at rest and start at the first stage of the exercise test protocol.
Monitor for the development of abnormal symptoms during exercise at the end of each stage and discontinue the exercise test if any of the following symptoms develop (excessive fatigue/tiredness, shortness of breath/breathlessness, chest pain/discomfort, dizziness, palpitations/racing heart, excessive cough, wheeze, stridor, muscle/joint pain, higher level of effort for the same past exercise load and ‘not feeling well’).
Monitor for the development of abnormal clinical signs during exercise at the end of each stage and discontinue the exercise test if any of the following clinical signs develop (abnormal heart rate and blood pressure response, very high respiratory rate, inappropriately high RPE and RPB).
Monitor for the same symptoms, signs and for a prolonged heart rate recovery after exercise.
Monitor for abnormalities when special investigations (ECG, pulmonary function testing) are done during and after exercise.
Monitor for symptoms (above), with the addition of dark urine in the 24 hours after exercise.
Re-assess the athlete if any abnormal symptoms, clinical signs or special investigations develop or are evident during, immediately after or 24 hours after exercise.
After the exercise challenge test, the athlete (coach or trainer) must perform a postexercise checklist (table 7: checklist 3). If there are no abnormal responses during or after exercise, the athlete can progress with increased training load (increased training frequency, intensity and duration), while self-monitoring for the same abnormal responses during and after each exercise training session (table 7: Checklists 3).
Checklists after an exercise/training session before the training load (intensity, duration, frequency) can increase in athletes with an acute respiratory infection (ARinf)
If there are abnormal responses during or after the exercise challenge test, or any subsequent exercise sessions at higher training loads, then the athlete should stop training and consult a physician or healthcare professional who will reassess the ARinf.
Moderate or severe ARinf
In cases of moderate ARinf, the recommendation is to either advise that the athlete performs a self-administered exercise challenge test or performs an exercise challenge test in a laboratory setting under supervision of trained medical staff (box 1). The choice would be based on the decision by the physician or healthcare professional. In cases of severe ARinf, the recommendation is to perform an exercise challenge test in a laboratory setting under supervision of trained medical staff (box 1). In moderate or severe ARinf either the athlete or the physician or qualified healthcare professional must complete a checklist (table 7: checklist 3 for the athlete, and checklist 4 for the SEM clinician) to determine whether the response to the exercise challenge test was normal. If there are no abnormal responses during or after exercise, the athlete can progress with increased training load (increased training frequency, intensity and duration), while self-monitoring for the same abnormal responses during and after each session (table 7: checklists 3 and 4). Again, if there are abnormal responses during or after the exercise challenge test, or any subsequent exercise sessions at higher loads, then the athlete should stop training and a physician or healthcare professional should re-assess the ARinf.
Assessment of activity risk is ongoing as training load progresses from return-to-participation/training to full return-to-performance and is mainly outcome based. The main outcome is to not only monitor for any abnormal responses to the exercise test (during, immediately after or 24 hours after the test), but also to determine if: (1) the athlete’s adaptation to training is as expected, or (2) there are other barriers to progression such as fatigue, soreness, or musculoskeletal injury. In general, a more rapid progression, with no abnormal responses, is likely in cases of asymptomatic ARinf or mild ARinf, while the rate of progression may be slower in cases of moderate/severe ARinf.
Step 4: assessment of risk tolerance
Continuous assessment of risk tolerance modifiers (eg, internal (self) or external pressures on the athlete, travel, timing of competitions, masking of symptoms, and conflict(s) of interest) is performed as the athlete progresses from return-to-participation to return-to-performance, completing the final RTS decision.
The final RTS decision is taken only when the risk assessments (steps 2 and 3) are below an acceptable risk tolerance threshold (step 4). At this point, the athlete is finally cleared for full RTS at the preillness training or competition level.
RTS considerations following ARinf in the team setting
As ARinf is a communicable disease, the physician must consider the risk not only from an individual but from a team perspective. A team environment, with locker rooms, meal sharing, shared equipment and accommodation is comparable to living in a family setting. In the family setting there are data that 20%–50% of susceptible members can become infected after exposure to viral ARinf such as rhinovirus, adenovirus and SARS-CoV-2. In general, viral transmission is most likely during the first 3–4 days of the infection, and isolation in the beginning of the symptomatic infection is recommended. Additional mitigation strategies, such as social distancing, and use of face masks and rigid hand hygiene can reduce the risk of viral transmission within teams. Knowledge of the specific virus, the viral shedding time and the transmission route helps to determine quarantine protocols, especially in the professional/elite sports environment and major competitions.
Effects of ARinf on exercise and sports performance
Improved understanding of the consequences of ARinf on an athlete’s performance informs prevention, treatment, and medical care, and RTS. The potential effects of ARinf on exercise and sport performance can influence the progression from return-to-participation/training to full RTS. For this consensus, a systematic review by a subgroup of the IOC consensus group was commissioned to determine the effects of ARinf on exercise and sports performance in athletes.107
Acute and longer-term effects of ARinf on exercise and sports performance
Initial studies point towards a decrement in performance following an ARinf, with impairments to muscular, nervous system and cardiorespiratory capacities, reflecting muscle protein catabolism caused by illness. Impaired coordination ability and speed in the performance of motor skills, reductions in submaximal force generation, slower reaction time, and decreased attention and vigilance, have been reported during allergic rhinoconjunctivitis108 and respiratory infections.109 However, some physiological attributes, including pulmonary function and VO2max, seem to be robust in the presence of mild ARinf particularly when localised to the upper respiratory region. ARinf that causes moderate to severe symptoms is associated with a higher risk of negatively affecting performance compared with mild ARinf. Performance might also be influenced by the loss of training time due to the illness and this might constitute a major determinant of performance of athletes in elite competition.110
Studies show the acute effects of ARinf on sports performance parameters can reduce the likelihood to start a race if an athlete had a recent ARinf (8–12 days prior to a race),111 compromise self-reported training ability and training capacity,112 and impair running kinematics (measured stride length, stride frequency and joint angles).113
Reduced training load, training mileage and a reduction in sports performance points have been reported over several months following ARinf. Time lost to acute illness in training and competition success is a primary indicator of the effect of ARinf on sports performance. The likelihood of achieving success was increased by sevenfold in athletes able to complete >80% of planned training weeks.110 Every week containing one or more days of modified training reduced the chances of achieving a key sports performance goal by 26%. Similarly, time-loss from training costs the recreational athlete highly anticipated participation in events, races, leagues, or competitions. Regardless of clinical significance, effects on performance including time lost due to acute illness, and an athlete’s subjective (perceptual) experience of an acute illness, may be just as detrimental to sports performance outcomes as physical impairments.
Other indirect effects of ARinf on exercise and sport
The negative effects of ARinf on exercise and sports performance could be indirect in nature. For example, nasal congestion can disrupt sleep, impair coordination and visual coordination. Other indirect effects of ARinf include tiredness, fatigue, and impaired quality of life. Furthermore, adverse effects caused by commonly used medications (antihistamines or anticholinergic agents) might impair exercise performance. Physicians should consider a broad range of clinical effects, and together with the athlete and coach, consider other practical, sporting and lifestyle issues that could influence management of an ARinf, and the time course of RTS.
Prevention of ARinf in athletes
Prevention of ARinf requires a multifaceted approach that minimises the risk of infection in an individual, the team and the people that they interact with, for example, team or technical support staff, media and spectators, within the environment which they are living in at that time. This is achieved through multiple measures including general and specific education and health promotion, individualised risk assessment and introduction of specific strategies to reduce risk, minimise symptom duration and reduce risk of spread to others. Some of the measures will be specific to the environment the individual is operating in (eg, training, travel or competition), and others will be generic recommendations of vaccination,114 hand hygiene,115 116 cough etiquette, use of face masks,117 promoting a resilient immune system (eg, nutrition, recovery and sleep hygiene) and early reporting of symptoms.
The prevention of ARinf is related to the risk factors associated with ARinf. For this consensus a systematic review by a subgroup of the IOC consensus group was commissioned to review strategies for the prevention of ARinf in athletes. However, this review identified only a few articles that could be considered. A summary of the risk categories with the specific risk factors, and the possible prevention measures for ARinf in athletes is summarised in table 8. From this list, an SEM clinician can advise a spectrum of preventive measures based on several risk factors applicable and the prevailing situation combined the individual athlete’s situation.
A summary of risk factors associated with ARinf in athletes with prevention measures that can be considered
Summary and future directions
The aim of this consensus was to provide the SEM clinician with an overview and practical clinical approach to ARinf in athletes. In summary, ARinfs in athletes are common, accounting for >50% of all illness-related consultations of an SEM clinician at major sports tournaments. Viral pathogens cause most ARinf, which present with several clinical syndromes, mostly as upper respiratory ARinf with or without systemic symptoms. Most ARinf in athletes (>80%) can be classified as mild, and do not have more than a short, transient and uncomplicated clinical course, which does not pose an increased risk for medical complications when exercise training continues or resumes. These asymptomatic or mild ARinf do not negatively affect exercise or sports performance. A small % of ARinf have a moderate to severe clinical presentation characterised by whole body and multiple symptoms, a more prolonged time course, and can be associated with regional respiratory complications or systemic multiorgan involvement. In these subgroups, there is in increased risk of medical complications as exercise training resumes after moderate to severe ARinf, which can also negatively affect exercise and sports performance. Although these complications and risks are rare, they need to be identified in athletes during the RTS process after ARinf. This process forms the basis of recommending a stepwise approach to RTS by risk stratifying athletes with ARinf, and then directing further more detailed assessment (clinical and by special investigations) to identify potential risk.
In this consensus, we suggest a practical stepwise clinical approach for this RTS process. Two novel and important contributions to this process are: (1) the recommendation that an exercise challenge test (self-administered or laboratory based) is performed before starting moderate- to high-intensity exercise training following an ARinf and (2) a recommendation for ongoing monitoring of symptoms and signs or abnormal training adaptation during the progressive RTS process. A further novel approach that we strongly advise is that athletes, coaches and medical staff be educated to (1) safely self-implement an exercise challenge test for asymptomatic or mild ARinf and (2) conduct ongoing self-monitoring during the RTS process, irrespective of the severity of ARinf.
Finally, we offer the following recommendations for future research and studies in this important field:
Consider using a standardised approach in future epidemiological and clinical studies: (1) the suggested classification system of ARinf, (2) definitions of the clinical syndromes of ARinf and (3) the classification of severity of ARinf.
Consider determining/documenting the specific pathogen responsible for ARinf in athletes. The use of scientific diagnostic methods to distinguish ARinf from ARill will enhance the quality of the current literature. This information will identify whether specific pathogens causing ARinf in athletes differ with respect to incidence, risk factors for ARinf, clinical presentation, pathology, illness severity, risk of multiple organ involvement, risk of medical complications during exercise, potential negative effects of pathogens on exercise and sport performance, and pathogen-specific RTS guidelines.
Conducting studies to:
Validate and/or refine the proposed severity classification of ARinf in athletes.
Determine the effects of asymptomatic ARinf in athlete.
Quantify the effects of ARinf (pathogen specific) on exercise and sports performance.
Validate and/or refine the suggested RTS guidelines, including the efficacy of athlete/coach and support staff education.
Evaluate the efficacy of various prevention strategies and treatment options for ARinf in athletes.
Identify if there are any longer-term health and performance consequences of pathogen specific ARinf in athletes.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
The core members of the IOC consensus group and authors of this manuscript acknowledge the following subgroup corresponding members of the IOC consensus group on Acute Respiratory Illness in Athletes, who contributed to the generating and publishing review material that formed part of this consensus statement: Marelise Badenhorst, Maaike Eken, Josu Gomez-Eceiza, Jane Fitzpatrick, Maree Gleeson, Lovemore Kunorozva, Katja Mjosund, Margo Mountjoy, Christopher Carlsten, Beat Villiger, Oliver Price, Vibeke Backer, Bruno Chenuel, Kjell Larsson, Carolette Snyders, Kelly Kaulback, Tod Olin, Thomas Halvorsen, Harald Hrubos-Strom.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @paolo_emilio, @VBougault, @wderman, @NIL don't use twitter, @TSoligard, @SportswiseUK
Contributors All authors contributed to the initial draft and final version of the paper. All authors confirmed the final version to be published.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared except for the following: RB who works as Director for the IOC Medical and Scientific Department, International Olympic Committee, Lausanne, Switzerland. LE who works as Head of Scientific Activities for the IOC Medical and Scientific Department, International Olympic Committee, Lausanne, Switzerland. UE who is the Chair of the Medical and Scientific Department, International Olympic Committee, Lausanne, Switzerland. TS who works as Scientific Manager for the IOC Medical and Scientific Department, International Olympic Committee, Lausanne, Switzerland.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.