Article Text

Abstract
Objective To identify and quantify potential risk factors for osteoarthritis (OA) following traumatic knee injury.
Design Systematic review and meta-analyses that estimated the odds of OA for individual risk factors assessed in more than four studies using random-effects models. Remaining risk factors underwent semiquantitative synthesis. The modified GRADE (Grading of Recommendations Assessment, Development and Evaluation) approach for prognostic factors guided the assessment.
Data sources MEDLINE, EMBASE, CENTRAL, SPORTDiscus, CINAHL searched from inception to 2009–2021.
Eligibility Randomised controlled trials and cohort studies assessing risk factors for symptomatic or structural OA in persons with a traumatic knee injury, mean injury age ≤30 years and minimum 2-year follow-up.
Results Across 66 included studies, 81 unique potential risk factors were identified. High risk of bias due to attrition or confounding was present in 64% and 49% of studies, respectively. Ten risk factors for structural OA underwent meta-analysis (sex, rehabilitation for anterior cruciate ligament (ACL) tear, ACL reconstruction (ACLR), ACLR age, ACLR body mass index, ACLR graft source, ACLR graft augmentation, ACLR+cartilage injury, ACLR+partial meniscectomy, ACLR+total medial meniscectomy). Very-low certainty evidence suggests increased odds of structural OA related to ACLR+cartilage injury (OR=2.31; 95% CI 1.35 to 3.94), ACLR+partial meniscectomy (OR=1.87; 1.45 to 2.42) and ACLR+total medial meniscectomy (OR=3.14; 2.20 to 4.48). Semiquantitative syntheses identified moderate-certainty evidence that cruciate ligament, collateral ligament, meniscal, chondral, patellar/tibiofemoral dislocation, fracture and multistructure injuries increase the odds of symptomatic OA.
Conclusion Moderate-certainty evidence suggests that various single and multistructure knee injuries (beyond ACL tears) increase the odds of symptomatic OA. Risk factor heterogeneity, high risk of bias, and inconsistency in risk factors and OA definition make identifying treatment targets for preventing post-traumatic knee OA challenging.
- anterior cruciate ligament
- meniscus
- risk factor
- osteoarthritis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What are the findings?
Anterior cruciate ligament (ACL) tears with a medial meniscal injury and/or meniscectomy, and isolated meniscal injuries are associated with an increased risk of structural knee osteoarthritis (OA).
Little is known about the risk factors for symptomatic or structural knee OA after non-ACL tear-related knee injuries, or after an ACL tear beyond meniscal injury or meniscectomy.
It is unclear if there are modifiable risk factors after a traumatic knee injury that can be targeted to prevent symptomatic or structural OA.
How might it impact on clinical practice in the future?
Non-modifiable risk factors: There is moderate-certainty evidence that the odds of symptomatic knee OA increased with various single (cruciate ligament, collateral ligament, meniscus, chondral, fracture or dislocation) and multistructure knee injuries (ACL with meniscal injuries and patellar dislocation with chondral injuries).
Modifiable risk factors: It is challenging to identify ‘treatment targets’ to prevent symptomatic or structural knee OA after a traumatic knee injury due to the heterogeneity in potential risk factors assessed, low-certainty of evidence, and inconsistency in how risk factors and osteoarthritis have been operationalised, measured and analysed.
In the absence of high-certainty evidence for modifiable risk factors for OA after traumatic knee injury, efforts to prevent post-traumatic OA should focus on implementing evidence-based injury prevention programmes and addressing modifiable risk factors for non-traumatic OA (eg, minimise unhealthy adiposity and quadriceps weakness) after a wide range of knee injuries.
Background
Osteoarthritis (OA) is the most common joint condition. It affects more than 300 million people worldwide and is a leading cause of pain, disability and socioeconomic costs.1 2 Post-traumatic OA accounts for at least 12% of OA cases, or 36 million people globally, and commonly involves the knee joint.3
Despite the large burden of OA, there is no cure.4 This leaves prevention as the primary means available to curb the OA epidemic.5 OA prevention can take many forms.6 In the context of post-traumatic knee OA, primary prevention strategies aim to prevent knee joint injuries in susceptible groups; secondary prevention strategies aim to delay or halt the onset of OA after joint injury; while tertiary prevention aims to improve pain and function in those with OA.
Although there is high-level evidence to guide primary7 and tertiary prevention8 of post-traumatic knee OA, considerable gaps remain in our understanding of how to delay or halt the development of OA after a traumatic knee joint injury.9 10 Secondary prevention of post-traumatic knee OA is contingent on knowing who is at risk (target population), identifying modifiable risk factors (treatment targets) and implementing interventions that mitigate these modifiable risk factors (treatments).11 A 2015 systematic review narratively summarised the risk factors for structural tibiofemoral and/or patellofemoral OA after anterior cruciate ligament (ACL) injury.12 It is unknown if these findings extend to other knee injuries, to symptomatic knee OA, or if studies reported since 2015 can address the inconclusive findings.
The primary objective of this research was to identify and quantify the magnitude of potential modifiable and non-modifiable risk factors for symptomatic and structural knee OA following traumatic knee injury. This review is one of seven informing an evidence-based consensus (OPTIKNEE) developing recommendations to guide rehabilitation to prevent post-traumatic knee OA.
Methods
Registration
This review was registered on the Open Science Framework on 7 August 2020 (https://osf.io/bkhr5/).
Framework
The Cochrane Handbook,13 Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines14 and PRISMA-Search extension15 informed the conduct and reporting of this review.
Data sources and search
Relevant studies were identified by searching five databases (Medline-Ovid, EMBASE-Ovid, CENTRAL-Ovid, SPORTDiscus-EBSCOhost, CINAHL-EBSCOhost). Search strategies consisted of medical subject headings and text words related to traumatic knee injury, risk or prognosis, and knee OA with limits for study design and English language. The Medline search strategy was developed in consultation with a health sciences librarian and adapted for other databases. All search strategies are presented in the online supplemental file. Searches were documented and reference lists of identified systematic reviews and included studies hand-searched to identify additional relevant records. Records were transferred to a reference management software (EndNote V.X1).
Supplemental material
Eligibility
Randomised controlled trials (RCTs) and cohort studies (prospective and retrospective) that assessed a potential risk factor for an outcome of symptomatic or structural knee OA over a minimum 2-year period after a traumatic knee injury in persons with a mean age at injury ≤30 years were included. Traumatic knee injury was defined as an isolated or combined traumatic tibiofemoral or patellafemoral (eg, ligament, meniscal, cartilage, subluxation, dislocation, fracture) injury. Symptomatic OA outcomes could include symptomatic radiographic OA, physician diagnosis, diagnostic code, endorsed evidence-based criteria16–18 or arthroplasty. Structural OA outcomes could include radiographic or MRI-based definitions. A minimum 2-year follow-up period was chosen as radiographic OA can be present 2 years following knee trauma.19 To maximise relevance to current day surgical and rehabilitation procedures, only studies published after 1999 were included. A mean age of injury ≤30 years was chosen to minimise the inclusion of degenerative meniscal lesions.20 Only studies measuring a risk factor(s) prior to an OA outcome, including exposed and unexposed participants, and compared OA prevalence between levels of risk factor exposure were included.11 Studies reporting data from the same cohort were included if they assessed different risk factors or reported estimates at different follow-up periods. We excluded studies that did not report knee trauma, including participants with OA at baseline, or did not operationalise OA unless data that allowed us to apply a definition were provided.
Study selection
After duplicate removal (EndNote V.XI), records were imported into a screening and data extraction platform (Covidence, Veritas Health Innovation). The authors (JML, JBT, LKT, BLvM, MvM, JLW) independently screened titles and corresponding abstracts in duplicate to determine potentially relevant records, followed by full-text review to determine final record selection. Disagreements were resolved through consensus or third author when needed. All decisions and inclusion and exclusion reasons were recorded (Covidence).
Data extraction
The authors (JML, JBT, LKT, ML, MvM, BLvM, MM, JLW) independently performed data extraction, in duplicate using a structured data extraction form (Covidence). Data extraction was guided by prognostic factor review recommendations21 and included study information (first author, publication date, title, location, design, aim, population, recruitment methods, inclusion and exclusion criteria, primary exposure and outcome variables, statistical tests, funding sources, conflicts of interest); participant characteristics (sample description, primary injury, time from injury to baseline, sex, age at injury, body mass index (BMI) at injury); treatment approach; follow-up duration (start and end date); risk factor(s) assessed and comparison condition; study attrition by exposure status; OA definition (method, definition, joints assessed); and results including number of total, exposed, unexposed participants, OA prevalence, unadjusted and/or adjusted estimate of OA odds or risk for each risk factor (OR, risk ratio (RR), HR with 95% CIs). When studies reported univariable and multivariable estimates, only multivariable estimates were extracted.
Risk of bias
The authors (JML, JBT, LKT, ML, BLvM, MvM, JLW) independently assessed risk of bias across included studies in duplicate using the Quality in Prognosis Studies (QUIPS) tool.22 Disagreements were resolved through consensus or third author when needed. The potential for selection, attrition and measurement bias for both risk factors and OA outcome, and bias due to confounding and statistical analysis were categorised as low, moderate or high based on signalling questions.21 22 Signalling question criteria (online supplemental file) were agreed on ‘a priori’ and operationalised based on expert knowledge, comparable reviews23 24 and domain-specific guidance (eg, missing data).21 22 25
Data synthesis
Data synthesis involved four steps. First, unique potential risk factors were identified and categorised by demographics, injury or treatment type. Second, matrices of potential risk factors for symptomatic and structural OA stratified by injury type and follow-up length were created. Third, univariate OR (95% CI) of OA for potential risk factors assessed in studies that only reported a p value when raw data was available were calculated. If necessary, accepted definitions of structural OA were applied to data where authors had not operationalised OA, but raw data were available (ie, KL Grade ≥2,26 Ahlback ≥1,27 Fairbanks ≥2,28 IKDC≥Grade B29 and patellofemoral joint osteophyte grade ≥1).26 Lastly, quantitative (meta-analysis) or semiquantitative synthesis was conducted, and certainty of evidence ratings assigned. Meta-analyses were performed for individual potential risk factors where there are more than four studies with OR (95% CI) of symptomatic or structural knee OA. Semiquantitative analyses were performed for potential risk factors with insufficient data for meta-analysis.30 Certainty ratings were generated by one author (JML), checked for accuracy by the lead author (JLW) and discrepancies resolved by consensus.
Quantitative synthesis
Statistical analyses were performed in R V.4.1.0 (R Core Team, Austria) using the ‘meta’ and ‘tidyverse’ packages. The pooled relative odds of OA for a given risk factor was estimated using a logarithmic transformed inverse variance-weighted (restricted maximum likelihood) random effects models with results back transformed and presented as ORs (95% CI). If possible, analyses were stratified by overall knee joint and joint compartment (total joint, tibiofemoral, medial tibiofemoral, lateral tibiofemoral, patellofemoral) OA; injury type (isolated ACL tear, ACL tear with concomitant injury, non-ACL-related injury); and follow-up time. Random effects models were chosen given the large expected heterogeneity in the methods used to assess and compare individual risk factors; length of time between injury and OA; and OA definition. Heterogeneity was assessed as the between-study variance (Tau2) and proportion of variance attributable to between-study inconsistency (I2). 31 32 When a risk factor was presented as both continuous and dichotomous variables across studies, the dichotomous scale was transformed to a continuous variable following Cochrane Handbook13 guidance if possible. In cases where a risk factor was assessed at various timepoints in the same cohort, only estimates from the furthest timepoint were included. ORs were chosen as the effect estimate as most studies in this field use logistic regression and do not present data required to recalculate risk or HR (95% CI).
After meta-analyses, the overall certainty of evidence for estimates of individual risk factors was rated as ‘high,’ or downgraded to ‘moderate’, ‘low’ or ‘very low’ using the modified GRADE (Grading of Recommendations Assessment, Development and Evaluation) approach for prognostic factor reviews.30 Briefly, the certainty of evidence was assessed across six domains including phase of investigation (strength of prognostic factor study design on a continuum from identifying, to confirming or understanding a prognostic pathway)33; methodological weaknesses (risk of bias based on QUIPs); heterogeneity of results (inconsistency in sample and methods); generalisability of findings to the target population (indirectness); estimate precision (95% CI width); and risk of publication bias.30
Semiquantitative synthesis
Semiquantitative synthesis30 involved rating the certainty of evidence for potential risk factors using the same modified GRADE approach30 adapted for non-pooled data (see online supplemental file).33 34 All domain ratings were considered when assigning an overall rating30 and a corresponding statement of certainty in the direction (considering consistency across studies), and magnitude of the risk factor and OA relationship was generated.
Patient and public involvement
Two individuals with lived experience of ACL tear (and ACLR) and four clinicians (physiotherapists, orthopaedic surgeons) contributed to the priority theme setting of this review through the OPTIKNEE consensus. A patient partner (MM) was involved in the design, execution and dissemination of this study (see the Contributions section).
Results
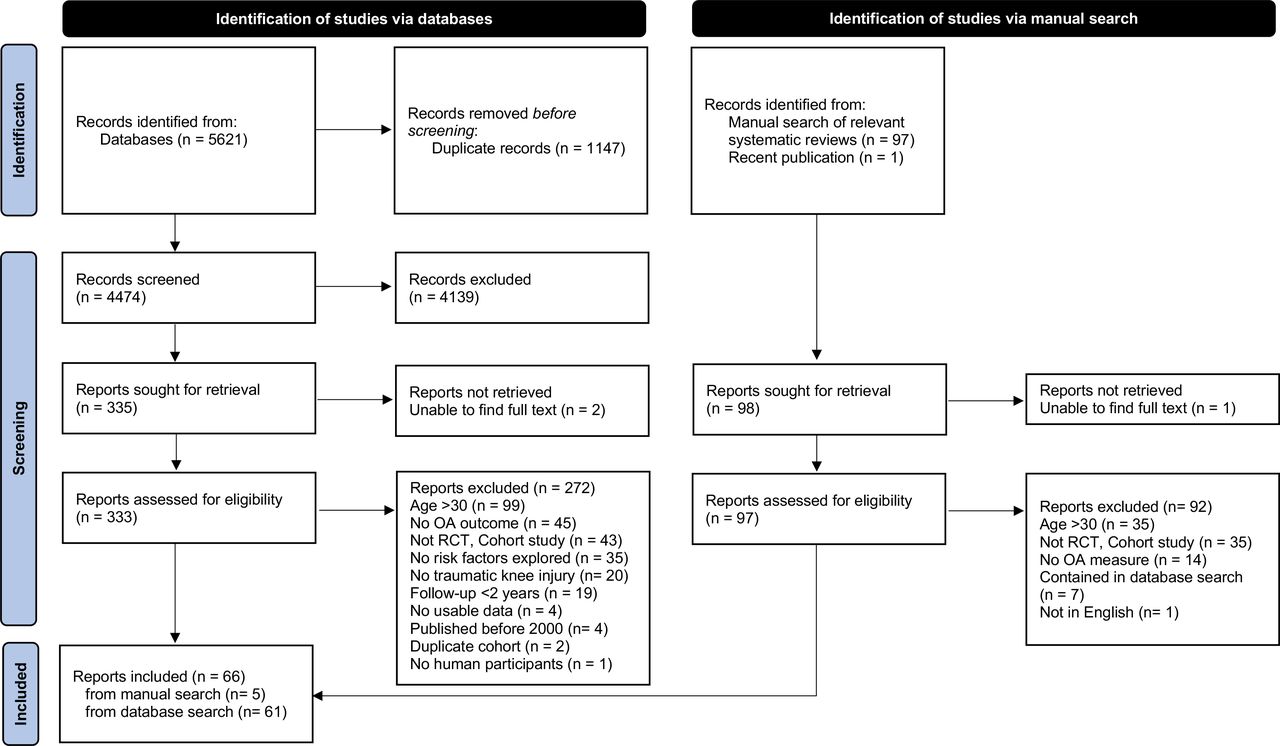
Sixty-six studies were included in the review (figure 1). These studies were published between 2000 and 2021, and included at total of 873 785 participants (73 852 with ACL-related injuries, 11 982 with non-ACL-related injuries and 787 951 uninjured) from 48 unique cohorts.

PRISMA flowchart. OA, osteoarthritis; PRISMA, Preferred Reporting Items for Systematic reviews and Meta-Analyses; RCT, randomised controlled trial.
Study characteristics
Included studies are summarised in the online supplemental file. Twenty-four were RCTs,35–58 17 were prospective cohort studies29 59–74 and 25 were retrospective cohort studies.28 75–98 Fifty-eight (89%) of the studies assessed participants with an ACL tear (with and without concomitant injuries),29 35–44 46–71 73–89 91 92 94 98 three (5%) considered multiple knee injuries,72 93 97 two (4%) meniscal injuries only,28 90 one (2%) cartilage injuries only45 and one (2%) patellar dislocations only.96 Only eight (12%) of the studies assessed risk factors for symptomatic OA (four ICD-9 or 10 diagnostic codes for OA, two physician chart, one symptomatic radiographic, one KOOS (Knee Injury and Osteoarthritis Outcome Score)).37 80 88 90 93 95–97 In contrast, 50 (76%) assessed risk factors for structural OA alone (49 radiographs, 1 MRI),28 29 35 36 38–60 62–64 68–73 75 76 78 79 81–84 86 87 91 92 94 98 and 8 (12%) assessed risk factors for both (eight symptomatic radiographic).61 65–67 74 77 85 89 Radiographic definitions of OA were based on a variety of grading systems including the KL (n=29),35 38 39 45–49 54 56 57 59 61 65–67 70 71 74 77 79 80 83–87 89 98 IKDC (n=15),29 51–53 58 60 62 68 69 75 76 78 91 92 94 Ahlback (n=10),28 36 39–43 49 55 59 OARSI Atlas (n=5),37 44 63 64 73 81 Fairbank (n=4),28 36 39 82 Iwano (n=2)40 96 and modified Ahlback and Fairbank (n=1)50 approaches, while the MRI definition was based on MOAKS (n=1)72 grading. Follow-up times ranged from 2 to 37 years, with 40 (61%) having a 6–15 year follow-up (figures 2 and 3).

Overview of potential risk factors for symptomatic knee OA by follow-up time and knee injury type. To provide an overview of what potential risk factors have been assessed at what timepoints, cohort studies that assessed a risk factor at multiple follow-up points are represented more than once. Apparent redundancies in risk factors are based on differences in definitions use across included studies (eg, terminology used to describe injuries that involved more than one structure). ACL, anterior cruciate ligament; ACLRc, ACL tear reconstruction; ACLRp, ACL tear repair; Ant, anterior; BMI, body mass index; Ext, extension; Flex, flexion; fu, follow-up; Knee injury, inclusive of several injury types; OAT, osteochondral autograft transfer; PF, patellofemoral; ROM, range of motion; RTS, return to sport; TF, tibiofemoral joint; yrs, years. 1Rehabilitation information provided. 2Intervention no reported. 3Past, present or future. 4Present or future. 5Serum.

Overview of potential risk factors for structural knee OA by follow-up time and knee injury type. To provide an overview of what potential risk factors have been assessed at what timepoints, cohort studies that assessed a risk factor at multiple follow-up points are represented more than once. ACL, anterior cruciate ligament; ACLRc, ACL tear reconstruction; ACLRp, ACL tear repair; Ant, anterior; BMI, body mass index; Ext, extension; Flex, flexion; Knee injury, inclusive of several injury types; OAT, osteochondral autograft transfer; ROM, range of motion; RTS, return to sport; TF, tibiofemoral joint; yrs (years). 1Rehabilitation information provided. 2Intervention no reported. 3Past, present or future. 4Present or future. 5Serum.
Risk factors
Across included studies, 81 unique potential risk factors were identified including 46 for symptomatic OA and 62 for structural OA, spanning 10 broad categories (figures 2 and 3). Categories included demographics (n=19)38 54 59 60 66 67 69 74–76 78 80 81 83 84 89 94–96; follow-up time (n=5)38 54 75 84 89; injury type (n=22)29 41 51 59 64–68 70–72 76 81 84 88 89 93 95–98; treatment approach (n=14)44 50 61 64 71 72 74 80 83 85 87 88 95 98; surgery type (n=30)28 29 38 40 44 45 50 51 53 59 61 64 69 71 72 74–76 78 80 81 83–85 87 88 90 95 96 98; ACL reconstruction (ACLR) surgical technique (n=9)37 40–43 47 48 50 55; ACLR graft choice (n=20)35 36 38 39 46 49 51–53 56–58 62 66 81 86 91 92 94 95; post-ACL injury or ACLR status (n=17)29 38 59 62 66 69 71 73 74 76–82 89 91 94; joint morphology (n=2)75 96; and biomarkers (n=1).63 Twenty-seven (59%) of the 46 potential risk factors for symptomatic OA and 39 (63%) of the 62 potential risk factors for structural OA were assessed in only one study. Further, 13 (81%) and 34 (57%) of the studies assessing symptomatic and structural knee OA considered multiple potential risk factors, respectively.
Odds and risk of osteoarthritis
With respect to potential risk factors for symptomatic OA, nine (14%) studies estimated or provided data to calculate OR (95% CI), one (1.5%) reported RR (95% CI), and eight (12.5%) reported HR (95% CI; see online supplemental file). In contrast, for potential risk factors for structural OA, 55 (92%) studies estimated or provided data to calculate OR (95% CI), while two reported RR (95% CI; see online supplemental file).
Risk of bias
The results of the risk of bias assessment are summarised in table 1. Only four studies (6%)44 88 90 97 were judged to be at low risk of bias across all domains. Most studies were judged to be at high risk of bias due to participant attrition (n=42, 64%) and inadequate control of confounding (n=32, 49%). Thirty-eight (58%) studies were judged to have low risk of bias in risk factor measurement.
Chronological summary of risk of bias assessment (QUIPS)
Meta-analyses
Across all potential risk factors, 6 (15%) for symptomatic OA and 16 (26%) for structural OA were assessed in more than four studies. Of these, none of the risk factors for symptomatic OA, and only 10 for structural OA (ie, sex, rehabilitation for ACL tear, ACLR for ACL tear, ACLR age, ACLR BMI, ACLR graft source, ACLR graft augmentation, ACLR with cartilage injury, ACLR plus partial meniscectomy and ACLR plus total medial meniscectomy) were eligible for meta-analysis. Ineligibility was due to insufficient data, or heterogeneity in the reported statistic (ie, OR, RR, HR), comparison condition or joint compartment assessed.
GRADE ratings suggested very-low certainty evidence that the odds of structural knee OA were increased after ACLR with concomitant cartilage injury (OR 2.31, 95% CI 1.35 to 3.94, I2=58%), ACLR with partial meniscectomy (OR 1.87, 95% CI 1.45 to 2.42, I2=44%) and ACLR with total medial meniscectomy (OR 3.14, 95% CI 2.20 to 4.48, I2=0%). No other statistically significant associations were found. Figure 4 summarises the pooled estimated OR (95% CI) and heterogeneity of meta-analyses (individual analyses in the online supplemental file), while table 2 summarises the GRADE rating, overall confidence and direction and magnitude for each risk factor. Potentially important heterogeneity was present for five of ten potential risk factors. Overall, the evidence for all meta-analyses was judged as ‘very-low certainty’ due to lower strength of study design (phase I and phase II studies), very serious risk of bias (8/10), inconsistency (5/10), indirectness (5/10), imprecision (4/10), publication bias (5/10) or no upgrading factors (5/10 studies).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plots for risk factor meta-analyses for structural knee OA (stratified by joint compartment). Odds (OR, 95% CI) of structural knee OA by risk factor both stratified by joint compartment (ie, unspecified knee joint compartment, total tibiofemoral joint compartment, medial tibiofemoral joint compartment) and combined across joint compartments. ‘Unspecified joint compartment’ was used when it was not clear which knee joint compartment(s) were assessed. Follow-up is presented in year range. ACLR, anterior cruciate ligament reconstruction; ACL, anterior cruciate ligament; BMI, body mass index; NA, I2 could not be calculated based on one study; yrs, years. 1Reference group is female sex. 2Samples include ACL injured persons only. 3Rehabilitation for ACL tear is stratified by comparison condition (ie, rehabilitation or delayed ACLR) not joint compartment thus estimates represent OA in any knee compartment. Frobell et al,44 Kvist et al 61 and Neuman et al 64 assessed tibiofemoral and patellofemoral OA with the tibiofemoral estimates included in meta-analyses, Meuffels et al 87 assessed tibiofemoral OA (based on radiographic views reported), Wellsandt et al 71 assessed tibiofemoral OA but only report medial tibiofemoral compartment estimates, while Kessler et al 83 did not specify joint compartment. 4Reference is no ACLR. 5Odds for every 1 year increase in age. 6Odds for everyone one kg/m2 increase in BMI. 7Reference is semitendinosus tendon autograft. 8Reference is ACLR or ACL repair with no graft augmentation. 9Reference is no cartilage injury or less severe cartilage injury at ACLR.10Reference is ACLR with no meniscectomy.11Reference is ACLR with no total medial meniscectomy.
Summary of evidence of risk factors for structural knee OA (meta-analysis)
Semiquantitative analyses
The results of the semiquantitative analyses for symptomatic and structural OA are summarised in tables 3 and 4, respectively. Potential risk factors for symptomatic OA were mostly assessed in phase II (confirmatory) and phase III (explanatory) studies with large sample sizes, and low-to-moderate risk of bias resulting in certainty of evidence ratings spanning high (27%), moderate (7%) low (22%) and very low (44%). In contrast, risk factors for structural OA were mostly assessed in phase I (exploratory) and phase II (confirmatory) studies with relatively smaller samples, higher risk of bias and conflicting results leading to certainty of evidence ratings of moderate (8%), low (16%) and very low (76%).
Summary of evidence of risk factors for symptomatic knee OA (semiquantitative synthesis)
Summary of evidence of risk factors for structural knee OA (semiquantitative synthesis)
After assessing GRADE domains, there was moderate-certainty evidence that the risk of symptomatic OA was increased with cruciate ligament, collateral ligament, meniscal, chondral, tibiofemoral fractures, tibiofemoral or patellar (and recurrent) dislocations, and multistructure injuries (including patellar dislocations with chondral injuries). Further, there was moderate-certainty evidence that an ACL tear with any concomitant injury increases the odds of structural OA.
Discussion
There is moderate-certainty evidence that the risk of symptomatic knee OA was increased after various types of single (cruciate ligament, collateral ligament, meniscus, chondral, fracture or dislocation) and multistructure injuries (ACL with meniscal injuries, patellar dislocation with chondral injuries). There is also very-low certainty evidence that the odds of structural knee OA was increased after a cartilage injury (OR 2.31), partial meniscectomy (OR 1.87) and medial meniscectomy (OR 3.14) at ACLR. These findings clearly identify the target population for secondary prevention of symptomatic and structural post-traumatic OA as persons with a wide range of tibiofemoral and patellofemoral joint injuries with priority given to specific multistructure injuries (ACL tear with concomitant injury and patellofemoral dislocation with chondral defect). Unfortunately, no treatment targets for secondary prevention of symptomatic and structural post-traumatic OA were identified due to heterogeneity in potential risk factors assessed and comparator groups, high risk of bias and inconsistency in how potential risk factors and OA were defined, measured and analysed.
Based on very-low certainty evidence, we were able to estimate the magnitude of non-modifiable risk factors reported on narratively in a past systematic review,12 including increased odds of structural knee OA related to ACLR with cartilage injury (twofold), partial (twofold) or total (threefold) meniscectomy. Despite similarities in the direction of findings, the certainty of supporting evidence between our and the past review differ. This discrepancy may reflect differences in design, methods of assessing certainty of evidence, risk factor groupings, and distinction between symptomatic and structural OA across studies. Our findings are also consistent with Poulsen et al 99 who identified increased odds of radiographic, symptomatic or self-reported OA with ACL tears (fourfold), meniscal injuries (sixfold) or combined ACL tears and meniscal injuries (sixfold).
Building on these past reviews, we identified moderate-certainty evidence that the odds of symptomatic OA are elevated not only by ACL tears (with or without concomitant injuries), but with collateral ligament, meniscal, chondral, dislocations, fractures and multistructure injuries as well. Given that some non-ACL injuries (ie, collateral ligament injuries) have a similar prevalence as ACL tears and are associated with a fivefold increased risk of symptomatic OA at 11 years,97 it could be argued they are an important focus for primary (injury) prevention and that we need to expand our current paradigm about the ‘target population’ for secondary prevention. Finally, we identified that male sex at ACL tear, older age at ACLR, higher BMI at ACLR, rehabilitation for ACL tear, ACLR for ACL tear, ACLR autograph choice, and ACLR augmentation do not change the odds of structural OA.
An important finding of this review is the high risk of bias that exists in the evidence-base underpinning prognosis after knee trauma, particularly in relation to attrition (selection bias) and controlling for confounding. Contributing to this are the large number of exploratory studies aimed at ‘identifying associations’ between a mosaic of potential risk factors and an equally diverse set of possible outcomes (one of which is OA). Typically, these studies do not account for confounding or multiple comparisons and only report p values or estimates of OA when the relationship is statistically significant (ie, reporting bias). Another common limitation saturating the evidence-base is the interpretation of coefficients included in regression models to control for potential confounding as if they were the primary risk factor of interest.100
From year 2000 to present, there appears to have been improvements (table 1) in reporting and reducing measurement bias for outcome variables, bias in statistical analysis and bias in confounding. Despite this, risk of bias related to participant attrition and its reporting persist. Transparent reporting of attrition is vital to ensure that future studies to confirm or explain the relationship between a risk factor and OA are adequately powered to detect changes at distant time points. Disguising attrition rates, or the forces driving attrition, only serves to weaken the field of study.
Recommendations for future research
The inability to identify treatment targets (modifiable risk factors) for preventing symptomatic knee OA after trauma, despite the extensive resources invested in the 66 studies included in this review, is nothing short of depressing. There is an urgent need to move beyond studies that ‘explore or identify’ the relationship between potential risk factors and structural OA, towards studies specifically designed to test independent associations between a risk factor and symptomatic OA, or explain the prognostic pathway with adequately powered statistical models built around the primary risk factor of interest. This might be best facilitated by involving an epidemiologist and/or a statistician. It is also important to recognise that unlike non-modifiable risk factors, high-certainty evidence for a modifiable risk factor can only come from an RCT (or meta-analyses of RCTs) showing that an intervention capable of modifying the risk factor reduces the incidence of OA.
Fewer than 25% of the included studies assessed risk factors for symptomatic OA. Given that it is the pain, disability and loss of quality of life associated with OA that drive the substantial personal and societal burden (healthcare use and workforce disability) of this condition, it is vital that future studies look beyond structural (ie, radiographic) definitions and focus on the ‘illness’ of OA. Similarly, only 13% of the studies we identified considered knee injuries beyond ACL tears. A broader consideration of traumatic knee injury, beyond ACL tear is needed to understand how to best tailor prevention strategies.
Despite identifying >80 unique potential risk factors, there was an obvious paucity of socioeconomic (eg, education and literacy, employment status, income, access to health services), sociocultural (eg, ethnicity, gender, childhood experiences) and ecological (eg, physical environment, climate, population density) factors in the evidence-base. As many of these factors are known determinants of health, it is reasonable they may influence the development of symptomatic OA after knee trauma and should be prioritised.
Given the challenges of retaining participants over many years, it is essential that future studies adjust for realistic attrition ‘a priori’. Similarly, there is an urgent need for consensus on definitions of early (in the lifespan) symptomatic and structural OA, early-stage (in the course of the illness/disease) symptomatic and structural OA,101 and how to operationalise, measure and handle key modifiable risk factors to enable future meta-analyses. Consensus on OA definitions102 and important modifiable risk factors are also needed to facilitate their inclusion in administrative datasets to allow for population level analyses.
Methodological (PROGRESS 2)11 and reporting (CONSORT,103 STROBE)104 guidelines exist and should be consulted during future study design. When reported, structural OA should be evaluated and presented for the total knee complex and for individual tibiofemoral and patellofemoral compartments to facilitate more precise data pooling. Particular attention should be paid to best practice for dealing with missing data, reporting selection bias (comparison of those lost to follow-up to those retained) and not categorising continuous variables in arbitrary, uninformative groupings. Presenting data in interpretable figures, including frequency with a denominator, and online supplemental files will facilitate future meta-analyses.
Clinical implications
Efforts to prevent symptomatic and structural OA after knee trauma should target people with a wide range of single and multistructure tibiofemoral and patellofemoral joint injuries. Although no clear treatment targets for preventing symptomatic or structural knee OA after knee trauma exist, efforts to reduce the burden of post-traumatic knee OA should not be abandoned. A logical and pragmatic approach would be to implement evidence-based injury prevention programmes to reduce the incidence of all knee trauma and target known independent modifiable risk factors for knee OA in general (as they will likely compound risk after trauma) following a wide range of knee injuries (not just ACL tears).6 105 This should include physical activity and exercise-therapy strategies to minimise unhealthy adiposity106–108 and quadriceps weakness.109
Another important clinical implication of this review relates to managing expectations about potential risk factors commonly cited as having either a protective or harmful effect for post-traumatic knee OA where evidence suggests otherwise. For example, the perceived value of early ACLR for reducing the risk for OA, and perceived harmful effect of late ACLR,110 rehabilitation only, or returning to pivoting sports after ACL tear.111
Strengths and limitations
Every effort was made to follow best practice for systematic reviews and meta-analyses for prognostic factors, and grading risk of bias and certainty of evidence. We developed a comprehensive search strategy in consultation with a librarian scientist and performed extensive searches without limiting the types of potential risk factors or knee injuries included. These efforts resulted in the most extensive synthesis, analysis (quantitative and qualitative) and presentation of potential risk factors for OA after knee trauma to date.
We acknowledge that our meta-analyses combined data across a range of follow-up times with significant heterogeneity. By including data from early timepoints when structural changes and/or symptoms are less prevalent, it is possible that the odds of OA are underestimated. With respect to heterogeneity, we have been transparent about the source and based our interpretations on 95% CI, not p values. Despite an ‘a priori’ decision tree, discussing unforeseen decisions among the research team, our semiquantitative synthesis is dependent on the judgement of the research team and prone to investigator bias. This may have resulted in more downgrading of evidence in an attempt to avoid overstating findings without supporting quantitative estimates. In contrast, the conservative nature of our QUIPS signalling questions and criteria for semiquantitative application of GRADE may have elevated the certainty of evidence ratings. Although we excluded studies published prior to 2000, some of the procedures (ie, ACL tear diagnosis with arthroscopy, open ACLR, ACL repair, total meniscectomy, prolonged knee immobilisation) in studies with longer follow-up periods are not common today and may have influenced the odds of OA. Finally, despite attempts to group studies into similar treatment groups, heterogeneity (ie, ACLR, ACL repair with or without augmentation) within samples must be acknowledged.
Conclusion
There is moderate certainty of evidence that the risk of symptomatic knee OA is increased after various single and multistructure knee injuries. Similarly, there is very-low certainty evidence that the odds of structural OA is increased with cartilage injury, partial meniscectomy and medial meniscectomy at ACLR. In contrast, no modifiable risk factors, or treatment targets, for symptomatic or structural knee OA after knee trauma were identified. Consensus on how to operationalise and handle potential risk factors, comparator groups and osteoarthritis are needed to inform strategies to prevent post-traumatic knee OA.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
JLW is supported by a Michael Smith Foundation for Health Research a Scholar Award (SCH-2020-0403) and an Arthritis Society STAR Career Development Award (STAR-19-0493). JML is supported by the Arthritis Society. LKT is supported by a Canadian Institutes of Health Research Fellowship. AGC is supported by a National Health and Medical Research Council (NHMRC) of Australia Investigator Grant (GNT2008523). The authors would like to acknowledge librarian scientist Wichor M. Bramer, PhD (Erasmus MC) who performed the database searches, librarian scientist Charlotte Beck (UBC) who assisted in translating the MEDLINE search strategy into SPORTDiscus and other OPTIKNEE review leads Bjørnar Berg, Stephanie Filbay, Pætur Holm, Erin Macri, Britt Elin Øiestad, May Arna Risberg, and Anouk Urhausen for their methodological input.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @jwhittak_physio, @JayLos18, @jbthorlund, @LKTphysio, @bellevanmeer, @agculvenor, @ewa_roos, @mvanmiddelkoop
Contributors AGC, JLW, ER and KMC were involved in priority theme setting. JLW coordinated the study. JLW, MvM, KMC, AGC, ER, JBT, CBJ, LKT, MM and BvM were involved in the design of the study. JLW, MvM, JML, JBT, LKT and BvM screened title and abstracts as well as full-text records. JLW, JML, JBT, LKT, MvM and ML performed data extraction and risk of bias assessment. MM contributed their lived experience to the design of (risk factors of interest), conduct (data extraction-author, year, country of publication, sample characteristics), and write-up (identification of key messages such as a focus on symptomatic versus structural OA). JLW and JML performed statistical analysis in conjunction with CBJ. JLW and JML wrote the first draft of the manuscript. All authors contributed to reviewing, editing and revising the manuscript and approved the final submitted version. JLW is the guarantor.
Funding Initial priority theme setting for the OPTIKNEE consensus (https://bit.ly/OPTIKNEE) was supported by a Canadian Institutes of Health Research Planning and Dissemination Grant (principal investigator JLW #161821) and a La Trobe University Research Focus Area Collaboration Grant (principal investigator AGC). The funders had no role in any part of the study or in any decision about publication.
Competing interests JLW and AGC are associate editors of the British Journal of Sports Medicine (BJSM). JLW is an editor with the Journal of Orthopaedic and Sports Physical Therapy. KMC is a senior advisor of BJSM, project leader of the Good Life with Osteoarthritis from Denmark (GLA:D) – Australia a not-for profit initiative to implement clinical guidelines in primary care, and holds a research grant from Levin Health outside the submitted work. CBJ an associate editor of Osteoarthritis and Cartilage. JBT holds a research grant from Pfizer outside the submitted work. ER is deputy editor of Osteoarthritis and Cartilage, developer of Knee injury and Osteoarthritis Outcome Score (KOOS) and several other freely available patient-reported outcome measures, and founder of the GLA:D). All other authors declare no competing interests.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.