Article Text

Abstract
Introduction Primary cam morphology is highly prevalent in many athlete populations, causing debilitating hip osteoarthritis in some. Existing research is mired in confusion partly because stakeholders have not agreed on key primary cam morphology elements or a prioritised research agenda. We aimed to inform a more rigorous, inclusive and evidence-based approach to research on primary cam morphology and its natural history by working towards agreement on a set of research priorities for conditions affecting the young person’s hip.
Methods An international expert panel—the Young Athlete’s Hip Research (YAHiR) Collaborative—rated research priority statements through an online two-round Delphi exercise and met online to explore areas of tension and dissent. Panellists ranked the prioritised research statements according to the Essential National Health Research (ENHR) ranking strategy. Reporting of results followed REPRISE (REporting guideline for PRIority SEtting of health).
Results A diverse Delphi panel (n=65, Delphi rounds 1 and 2; three ENHR strategy surveys: n=49; n=44; n=42) from 18 countries representing six stakeholder groups, prioritised and ranked 18 of 38 research priority statements. The prioritised statements outlined seven research domains: (1) best practice physiotherapy, (2) rehabilitation progression and return to sport, (3) exercise intervention and load management, (4) primary cam morphology prognosis and aetiology, (5) femoroacetabular impingement syndrome prognosis and aetiology, (6) diagnostic criteria, and (7) screening. The panel recommended areas of tension and dissent for the research community to focus on immediately.
Conclusion While informing more rigorous, inclusive and evidence-based research, this consensus is a roadmap for researchers, policy-makers and funders to implement research dedicated to reducing the cost and burden of hip disease related to primary cam morphology.
- hip
- groin
- research
- consensus
- osteoarthritis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Primary cam morphology is mostly a benign bony prominence that develops at the femoral head–neck junction of the hip. It is, however, highly prevalent in many athlete populations1–3 and causes debilitating hip osteoarthritis in some,4 thus placing existing and potential athlete-patients at risk of future hip disease.
Two aspects relevant to research focus and quality, highlighted in the introduction of a linked paper (Oxford consensus study, part 1) underpinned the work reported in this paper. First, clinicians and researchers cannot predict with accuracy who will develop primary cam morphology, whose primary cam morphology will be inconsequential and who will end up with a total hip replacement—research into risk factors for aetiology and poor outcomes of primary cam morphology is needed. Second, existing research is mired in confusion partly because clinicians, athletes, patients and researchers have not agreed on a conceptual or operational definition of primary cam morphology, key terminology or a taxonomy of subtypes.5
We reported in a linked paper (Oxford consensus study, part 1) how an international group of clinicians, athletes, patients and researchers—representing the Young Athlete’s Hip Research (YAHiR) Collaborative—engaged with, challenged and improved four key areas on primary cam morphology and its natural history. The four key areas identified for further attention by a preliminary concept analysis5 were the following: (1) a new conceptual definition for the morphology based on five defining attributes; (2) more consistent terminology commending the important (although from a small and select expert panel) Warwick Agreement6; (3) taxonomy distinguishing between primary and secondary cam morphology and (4) challenges of operationalising the hip morphology. However, agreement on a prioritised research agenda for the field, the focus of this paper, is lacking.
The problem of largely investigator-driven health research agendas, marginalising the voices of other stakeholders including patients, caregivers and the community, has fuelled a mismatch between the interests of patients and researchers, and a possible misdirected allocation of limited resources.7–9 This spotlighted the need for transparent research priority setting with stakeholders.7 10–17
The Warwick Agreement expert panel, including one patient, prioritised and ranked 23 femoroacetabular impingement (FAI) syndrome research questions in 2016,6 while more recent consensus statements on hip-related pain18–21 and FAI imaging22–24 proposed and discussed, without prioritising or ranking, additional research topics.
Research partnerships with athletes, patients, researchers and clinicians should agree on a prioritised research agenda for conditions affecting the young person’s hip. If not, crucial questions will remain unanswered, scarce resources will continue to be directed to areas with low or no impact, and research waste will continue.
Here we report on our aim to inform a more rigorous, inclusive and evidence-based approach to research on primary cam morphology and its natural history. The specific objectives of the research were to:
Ascertain the level of agreement among experts on definitions, terminology, taxonomy and imaging outcome measures for research on primary cam morphology.
Work towards agreement (and highlight residual disagreements) on a set of research priorities on conditions affecting the young person’s hip, focusing primarily on primary cam morphology and its natural history.
Hold two education events to engage stakeholders, disseminate the latest evidence and stimulate debate.
Oxford-Aspetar-La Trobe Young Athlete’s Hip Webinar Series.
Young Athlete’s Hip Research Collaborative Symposium.
We report the results of objective 2 and our dissemination strategy (objective 3) in this paper and that of objective 1 in a linked paper (Oxford consensus study, part 1).
Methods
This methods section focuses on objectives 2 and 3 of the Oxford consensus study while a linked paper (Oxford consensus study, part 1) describes the methods to achieve objective 1. Online supplemental file 1 describes and elaborates on the combined Methods for parts 1 and 2 of the Oxford consensus study.
Supplemental material
We held a sequential, two-round online Delphi survey and two synchronous online mixed stakeholder group meetings (Interacting Group Process) to explore the level of agreement among a panel of experts on primary cam morphology definitions, terminology, taxonomy and imaging outcome measures for research, and to work towards agreement on a set of research priorities on conditions affecting the young person’s hip. The prioritised research statements were further ranked according to the Council on Health Research for Development’s Essential National Health Research (ENHR) ranking method.
Study design: Delphi method and research priority setting process
Delphi method: For this three-stage consensus study (figure 1), an experienced steering committee managed the design, conduct and dissemination rigour. A two-round Delphi method was used to prioritise the research statements (domain 5 of the Delphi method). We modified the classical Delphi method slightly by replacing an open qualitative first round with a preselected list of statements based on a literature review and synthesis of steering group members’ knowledge.25–27 Three online Microsoft Forms surveys followed to further rank the prioritised statements according to the Council on Health Research for Development's ENHR strategy for research priority setting.28

Oxford consensus study flow chart. Stage 1: prepare for Delphi method; stage 2: Delphi method online rounds; stage 3: virtual discussion meetings and ENHR strategy for research priority setting. *Essential National Health Research; **Mini-module adapted from Ref. 28.
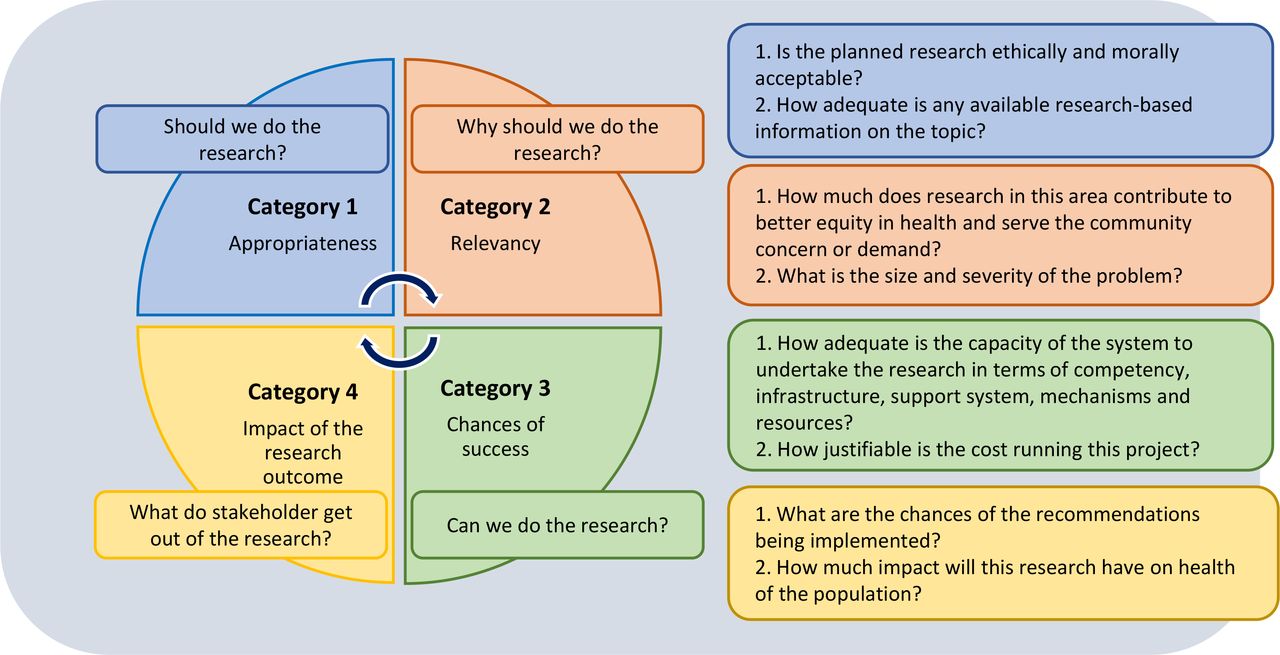
Research priority setting—ENHR strategy to rank the prioritised statements: We adapted the ENHR ‘mini-module’, asking the Delphi panel to apply a 0 to 3 Likert Scale score to category 1 criteria, and 1 to 3 Likert Scale for remaining six criteria. A maximum three points per criterium resulted in an equal weighting of six points per category (figure 2 and online supplemental files 8a, 8b and 8c and 9). We shared and discussed the ENHR ranking strategy results with Delphi panel members during optional online meetings. Our research priority setting project will be registered on the Ludwig Boltzmann Gesellschaft Open Innovation in Science Center’s worldwide Priority Setting Database of research priority setting projects, adding rigour and transparency.29
Supplemental material
Supplemental material
Supplemental material
Supplemental material
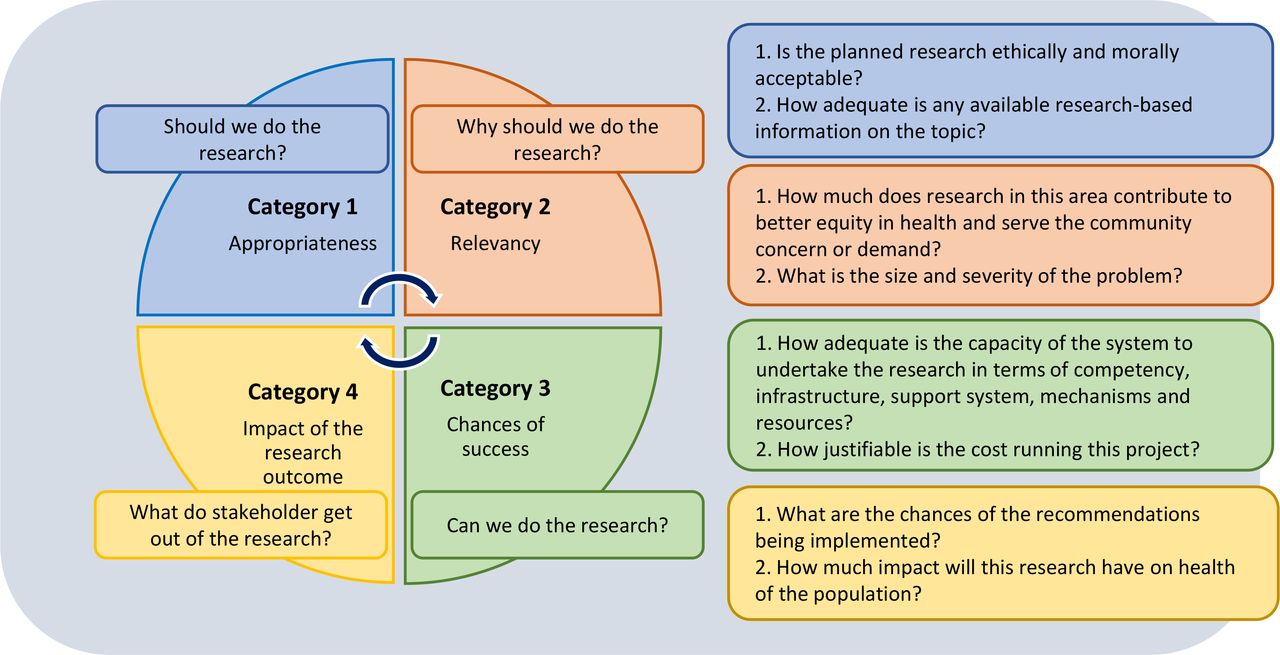
Four categories (and two criteria for each) of the Essential National Health Research ranking strategy.28 We applied a 0 to 3 Likert Scale score to category 1 criteria, and 1 to 3 Likert Scale score for the remaining six criteria. A maximum three points per criterium resulted in an equal weighting of six points for each category.
The Delphi and ENHR exercises allowed panel members to participate anonymously, reducing the potential influence of dominant individuals.30 Reporting of results followed the 31-item REporting guideline for PRIority SEtting of health (REPRISE)7 (online supplemental file 2) and the Conducting and REporting DElphi Studies (CREDES)31 (online supplemental file 3).
Supplemental material
Supplemental material
Stage 1: planning
Steering committee: The study steering committee included members of the YAHiR Collaborative and aimed for a robust Delphi method and ENHR ranking process. Interpreting ‘diversity’ as more than representation of certain demographic groups, the steering committee ensured a diverse (eg, sex/gender, country of residence, profession), informed (knowledgeable about primary cam morphology and its natural history) and representative of previously minoritised groups relevant to this research field (eg, participants from the Global South, patient and public representatives and women) international Delphi panel. By prioritising anonymity and access to adequate topic-specific resources, the online Delphi method and ENHR ranking strategy supported a more equitable and inclusive process (online supplemental file 4: steering committee terms of reference).
Supplemental material
Delphi and ENHR ranking panel: We describe in a linked paper and online supplemental file 1, how the ‘closeness continuum’ was adapted and applied to purposively recruit a maximum variation sample of 73 experts for this study, based on the steering committee’s judgement and knowledge of the context.32 With steering committee oversight, the lead author invited all potential participants. Participants were not reimbursed.

Revised Bloom’s taxonomy of cognitive process action verbs informing our dissemination strategy.36
Definition of consensus
Sample size: The Delphi study steering committee oversampled to compensate for possible attrition over rounds (at a rate of 25% per round). As consensus is normally achieved in an average of three rounds, the steering committee aimed to recruit a starting sample of 50 to 100 panel members.
Patient and public involvement (PPI): We involved patient and public partners in the planning, delivery and dissemination phases of the Oxford consensus through the YAHiR Collaborative’s PPI group. The latter group was represented in the Delphi study steering committee. We supplied all members of the PPI group with a glossary, mentored them on definition use and content (during individual and one PPI group online meetings) and invited them to weigh in on each Delphi round as well as in ENHR ranking surveys.33 They had access to the recordings of the Oxford-Aspetar-La Trobe Young Athlete’s Hip Webinar Series, providing a good knowledge base including the current evidence, and issues, allowing an informed assessment. Members of the PPI group lead and actively participated in the mixed stakeholder group discussions following the Delphi rounds (stage 3 below).
Delphi software: We used DelphiManager, ‘a web-based system designed to facilitate the building and management of Delphi surveys’ for the Delphi rounds and Microsoft Forms for the ENHR research ranking exercise.34
Ethical considerations: Research participants provided informed online consent for the study as part of the DelphiManager surveys and their identities kept anonymous during the online Delphi and ENHR ranking rounds. The University of Oxford’s Medical Sciences Interdivisional Research Ethics Committee (MS IDREC) provided ethics approval (R73576/RE001).
Statement preparation: We created an extensive list of statements and conceptual framework of all the potential future research priorities for primary cam morphology and its natural history. We based the initial statement list on a concept analysis of primary cam morphology,5 the early results of a qualitative study to explore stakeholder perspectives on factors contributing to high-quality research on how primary cam morphology develops, the Lisbon Agreement on Femoroacetabular Imaging22–24 and the research recommendations of recent (since January 2016) consensus recommendations on research in the field.6 18–24 Members of the Delphi study steering committee independently reviewed the statements, followed by an iterative, asynchronous online process to review, discuss, modify and approve the final statements. The steering committee provided additional descriptive information ('Help Text') where appropriate and asked stakeholders, including members of the PPI group, to provide feedback on the draft Delphi survey. Stakeholders examined the survey’s face validity (eg, comprehensibility and acceptability) and refined language, formatting and layout.
Panel information pack and training: All panel members had access from the outset of the project and throughout the Delphi process to the course material, including recorded presentations, of the first eight webinars of the Oxford-Aspetar-La Trobe Young Athlete’s Hip Webinar Series (online supplemental file 5). Panel members had full-text access to five recent consensus statements,6 18–21 and a summary of their research recommendations is described in online supplemental file 6. Completion of the webinars and/or reading of the consensus statements were not required.
Supplemental material
Supplemental material
Consensus definition: The steering committee agreed on a consensus definition prior to the Delphi rounds (table 1).
Stage 2: online Delphi rounds
The consensus process involved a sequential, two-round Delphi survey.
Round 1: Invited participants provided informed consent and registered for the study in one of the six stakeholder groups. The statements were presented in a sensible and logical order in five questionnaire domains (definitions, terminology, taxonomy, imaging outcomes and research priorities).
Panel members scored each statement using a 9-point Likert Scale ranging from 1 ('not important/disagree') to 9 ('critical/agree'), based on the Grading of Recommendations Assessment, Development and Evaluation scale for scoring the importance of including the item in the final list of statements.35 Round 1 included free-text sections allowing participants to propose new or modified statements and provide general study feedback. The steering committee reviewed, discussed and considered the proposed new statements or statement modifications suggested by participants in round 1 and resolved any uncertainties. All statements were kept unchanged for round 2.
Round 2: Participants had access to the visual distribution (histograms) of round 1 scores for each statement stratified by stakeholder group. Panel members saw their score and then rescored (or not if they chose to defend their outlying score) each statement on a scale of 1 to 9 based on the average scores of the group. We documented changes in scores from round to round, and panel members could provide reasons when their score boundaries changed between round 1 and round 2, for example, to defend their outlying score(s) (online supplemental file 7).
Supplemental material
The steering committee and Delphi panellists explored and discussed reasons for outlying scores, disagreement and dissent (including statements with overall consensus) during the online Interacting Group Process (stage 3). The steering committee considered further Delphi rounds (applying the same criteria). However, the two Delphi rounds resulted in high consensus and surfaced important disagreements and areas of dissent to proceed to online consensus discussions, including how to implement the study’s findings.
Stage 3: online Interacting Group Process and research priority setting using the ENHR ranking exercise
Interacting Group Process—online mixed stakeholder group discussion meetings: Facilitated by Delphi steering committee and PPI group members, Delphi panellists discussed all discordant items as well as areas of tension and dissent, during two online mixed stakeholder group meetings, based on the Interacting Group Process. The second meeting, reported in this paper, discussed research statements prioritised after the two Delphi rounds. The first meeting discussed the Delphi round results for the first four domains: definitions, terminology, taxonomy and imaging outcomes (Oxford consensus study, part 1). To create a safe space for panellists to share their views, the steering committee facilitated discussions in small zoom breakout rooms that were not recorded. Group leads documented the discussions in a field diary and maintained speaker anonymity.
Research priority setting—ENHR strategy: An online Microsoft Forms survey process followed to further rank the prioritised statements according to the ENHR strategy for research priority setting as described earlier (online supplemental files 8a, 8b and 8c).28
Feedback: Following the ENHR ranking exercise, panellists were able to attend one of six optional, time-zone friendly online feedback-and-discuss meetings.
Data analyses
Delphi method: We describe detailed data analysis, including descriptive statistics, qualitative analysis of panellist feedback and dissent analysis in a linked paper (Oxford consensus study, part 1) and online supplemental file 1. We applied outlier, bipolarity and stakeholder group analysis to explore possible dissent (dissent analysis).
ENHR ranking exercise: We created Excel spreadsheets of panellists’ ranking-question scores and qualitative feedback (using three Microsoft Forms surveys) for each of the 18 Delphi method-prioritised research statements. We calculated mean scores for the eight ranking criteria (0 to 3 Likert Scale score to category 1 criteria and 1 to 3 Likert Scale for the remaining six criteria). A maximum three points per criterium resulted in an equal weighting of six points for each of the four categories (figure 2). The final statement ranking score was calculated by adding the mean criterium scores (maximum ranking score per research statement=24).
Dissemination and implementation
To fulfil objective 3 of the Oxford consensus study, we applied the revised Bloom’s taxonomy36 (figure 3) to develop two education events aimed at early dissemination and implementation: Oxford-Aspetar-La Trobe Young Athlete’s Hip Webinar Series (online supplemental file 5), and YAHiR Collaborative’s Young Athlete’s Hip Symposium and Research Meeting (22–23 September 2022 at Worcester College in Oxford—online supplemental files 13a and 13b). The revised Bloom’s taxonomy, a tool to create education that encourages critical thinking, emphasises verbs—the basis of the cognitive process.36
Supplemental material
Supplemental material
Results
Of the 73 experts invited to participate in this study, 65 completed rounds 1 and 2 of the Delphi exercise. The Delphi panel from 18 countries represented six stakeholder groups—26 were female (table 2). The Delphi panel scored 85 statements (12 definition, 19 terminology, 4 taxonomy, 12 imaging outcome and 38 research statements) and reached consensus on 43 of 85 (51%) statements in round 1, and 53 of 85 (62%) statements in round 2. Results of the Delphi rounds for the definition, terminology, taxonomy and imaging outcomes domains (domains 1 to 4 of the Delphi method; objective 1) are reported in a linked paper (Oxford consensus study, part 1).
Demographic characteristics of Delphi panel and Essential National Health Research (ENHR) ranking exercise participants
Here, we report the results of our strategy working towards agreement on a set of research priorities on conditions affecting the young person’s hip, focusing on primary cam morphology and its natural history (objective 2; Delphi domain 5 and ENHR ranking strategy). This results section includes three key elements: (1) quantitative results (online supplemental files 7, 8a and 8b), (2) qualitative analysis supported by quotations of panellists’ feedback selected from across the Delphi database (online supplemental file 10) and (3) dissent analysis (online supplemental file 9). Through this comprehensive approach to results, we illuminate the quantitative and qualitative strengths of the Delphi method. To facilitate readability, we colour-coded tables 3 and 4 and crafted a separate infographic paper summarising the 18 prioritised research statements in seven research domains.
Supplemental material
Supplemental material
Results of two Delphi survey rounds and ENHR* ranking exercise showing the level of agreement and ranking of 18 prioritised research priority statements on conditions affecting the young person’s hip†
Results of two Delphi survey rounds showing the level of agreement on 20 non-prioritised research priority statements on conditions affecting the young person’s hip*
The results of the Interacting Group Process discussions are summarised in box 1 and online supplemental file 12. We also report two education events to engage stakeholders and disseminate research results (objective 3).
Supplemental material
Interacting Group Process: mixed stakeholder group discussion summary—research priority domain
While prospective cohort studies on primary cam morphology aetiology and prognosis are already prioritised, authentic collaboration on large multicentre studies, using similar methods to allow data sharing, should (1) ‘involve patient and the public in everything’, (2) focus on ‘agreeing a standard set of variables’ (outcomes, interventions, assessments), and (3) ‘ask very specific questions’ using ‘clear methods’. Discussion groups raised six challenges to authentic collaboration (with possible solutions for some). First, authorship position, when publishing results, is often contested. Second, it is difficult to getting started with data sharing—larger/established research groups should lead. Third, early career researchers, especially from low/middle-income countries or resource poor settings, are sometimes not taken seriously enough. Fourth, equitable approach to funding division, although important, is difficult, especially dividing financial support across countries. Fifth, standardising of processes can be difficult for lower income countries or institutions. Last, funders should target grants to support collaborative projects.
The panel agreed that primary cam morphology screening as part of research to inform our knowledge ‘is fine, but screening as part of routine clinical practice is likely not fine and may lead to overmedicalisation’. Risks of screening for primary cam morphology include ‘overtreatment in a condition that we know is often asymptomatic’. The panel questioned the need to screen ‘for a condition that we have already agreed is a ‘normal physiological response’. A biostatistician panel member commented on the importance of the WHO’s Wilson-Junger criteria to inform whether screening is appropriate or not. Warning that screening in younger cohorts (8 to 18 years) should ‘be carefully managed from an ethical perspective’, the panel recommended ‘qualitative studies’ to investigate ‘the potential nocebo impact of any diagnostic labelling’. It is also important to note the lack of scientific evidence to support ‘advising younger individuals that they should limit participation in certain sports based on screening results’. Screening results might provide a basis ‘to offer preventative support at an earlier stage to a small percentage of those with cam [morphology] who go on to develop significant hip problems later in life’.
Stakeholder groups discussed eight factors that will facilitate athlete/participant compliance in long-term follow-up studies: (1) involve stakeholders in study designs; (2) focus on language—‘let’s figure out how to keep your hip healthy’; (3) address a large qualitative research void with respect to compliance in prevention/cohort studies; (4) recruit full teams not individuals; (5) demonstrate [to athletes, coaches and managers] that performance improves—focus on performance development over hip health to get better buy-in from athletes, coaches, and parents; (6) foster wider organisational buy-in and involve policy-makers in priority setting; (7) consider how much is asked from participants—balance how much we measure to reduce the burden, and (8) create a core outcome set for these areas to support streamlined research studies and participant burden.
Discussing the feasibility of load management studies during growth, discussion groups stressed the importance of involving ‘methodology experts’ (eg, study design and training-load monitoring) and the target group in the development of any research. Load management studies on primary cam morphology development during growth may not be the right priority for new research. Patient buy-in is likely to be low—‘elite sports children may be unwilling to reduce participation in their preferred sport’ and more attention needs to be given to context: ‘optimal study designs may not be generalisable to suboptimal context’.
Warning ‘not to focus on cam morphology as a problem’, stakeholder groups mentioned seven critical elements of effective physiotherapy/rehabilitation (best practice physiotherapy) for patients with FAI syndrome: clinicians should (1) apply a ‘holistic approach to rehabilitation’ that uses the ‘same language’; (2) deal with ‘patient expectations, especially time: lifelong’; (3) address ‘fear of movement’; (4) modify ‘what the patient do’; (5) consider ‘who the advocate for the athlete/patient should be’; (6) deliver ‘treatment programmes’ of ‘at least 6 months in duration’, and (7) develop treatment programmes with ‘exercise interventions’ as the ‘foundation, with potential room for manual therapy’. Finally, the field ‘needs individual participant data studies with subgroup analysis to inform this [best practice physiotherapy], as much of the therapy approaches that “work” has been mixed methods so likely needs to be teased out as to which factors offer the greatest benefit’.
An ex-elite athlete panellist spotlighted Return-to-Sport challenges mentioning ‘major anxiety’ as a result of ‘worries about Return-to-Sport (RTS) (which was my living)’.
A patient–clinician panel member commented on their ‘lived experience as a patient with FAI/labral tear’, emphasising that ‘all healthcare providers have to be on the same page when it comes to expectations and treatments’. Patients ‘struggle with learning how to ultimately keep their hip happy’. This panel member emphasised three RTS aspects from a patient’s perspective and relevant to a multidisciplinary team approach. Clinicians should encourage and support patients to (1) work with a strength and conditioning coach ‘who helped me really get over the fear that loading my hip would make it worse’; (2) work with a sports psychologist ‘to work through catastrophising thoughts I had about my hip imaging results’, and (3) identify ‘all lifestyle factors and training factors that will impact the hip: frequency of sport/running, duration, intensity, sleeping, nutrition, strength training’.
Stakeholder groups commented on six additional factors that may influence RTS: (1) ‘Athlete expectations: what has the athlete been told about their condition and their potential prognosis by a healthcare practitioner. Does the athlete expect or feel that X intervention is the “only way” to allow them to RTS? Are we honest with athletes about the potential that they may not return to their previous playing levels due to the current status of their injury/pain/hip? (2) Quality of intervention: we still do not have a “best practice” method/guide for hip interventions in cam morphology and FAI syndrome. The treatment that an athlete receives, surgical or non-surgical, may have a large influence on them returning to sport; (3) Stage of career: as indicated in an earlier comment—considering the stage of the athlete’s career may influence RTS. Older athlete towards the end of their career may not “want to return to sport” to preserve long-term health and quality of life; (4) Sport type: individual versus team. Knowledge of an individual’s sport may have a large influence on their RTS. Often team sport athletes may be able to gradually RTS or have their load managed. In individual sports this may not be possible and there may be more pressure to RTS when they are not necessarily ready; (5) Contract status: in professional athletes, an athlete’s contract status or endorsements may influence their RTS timeframe; (6) Support structures: the support structures and expertise available may influence an athlete’s RTS’.
While there is a ‘need for clarity around the definition of “return to sport”—as return to sport is often very different than return to performance’, stakeholder groups warned that ‘the current binary (yes or no) method of outlining RTS may not be fit for purpose’. They suggested the possibility of ‘a sliding scale or some type of Likert Scale that assesses athletes’ confidence/happiness with playing status pre/postintervention’.
Finally, stakeholder groups emphasised ‘the need for qualitative research in the area to ascertain players’ perspectives about RTS’.
The importance of qualitative research was spotlighted by a patient-panellist’s Delphi round 1 recommendation to add a research priority statement ‘on how diagnosis, rehab, return to sport impacted the mental health of young athletes (and others)’. Stakeholder groups emphasised ‘considering all the aspects in anything that is labelled and how the label may impact growth and bias later’. Differentiating between primary and secondary cam morphology is therefore important ‘as an aid for better definition and intervention as the science evolves’. It is ‘super important in this population to understand a patient’s journey from diagnosis through treatment’. Athlete-patients are interested in what primary cam morphology and/or FAI syndrome means for their hip ‘long term’: ‘Can we rehab or is surgery required?’; ‘How it will impact my career, life, both and do I need it fixed or not?’ Stakeholder groups suggested researchers should ‘embed what is important to patients or those with the morphology’, ‘work in coproduction’ on ‘experience videos’ and ‘frameworks, maybe starting with safeguarding or prevention’. In addition, stakeholder groups recommended ‘peer focus groups with young people, explaining the science and giving them the problems to ‘solve for science’ along with scenarios, risk communication, discuss pre-emptive or interventional screening and explain differences noting prostate, breast, lung screenings and costs’.
The groups highlighted involving parents and coaches as ‘it is difficult for athlete-patients to rest/commit to physiotherapy especially when being pushed by parents/coaches’. It is also difficult to motivate patient-athletes to continue with exercise-based rehabilitation after 3–4 months especially with ‘regional differences between effective physio/rehab/surgery’ and systems, for example ‘pay for service and how that affects treatment decisions’.
The Delphi panel reached consensus to prioritise 14 of 38 research statements in Delphi round 1 and 18 in round 2 (table 3). Twenty research statements were not prioritised (table 4). Panellists listed reasons for score boundary changes between rounds 1 and 2 for each statement (online supplemental file 7); statement 56 (table 3) did not reach stability. The four highest ranked research statements following the Delphi rounds described studies to investigate primary cam morphology aetiology and prognosis (statements 49, 48, 50 and 54; >90% Delphi panellists agreed that these statements were ‘critical’ and 0% that it was ‘not important’). This changed after the online Interacting Group Process discussion (six mixed stakeholder groups (n=41) of five to eight panellists each) and the ENHR ranking exercise (three ENHR strategy surveys: n=49; n=44; n=42). We present the average criterium question scores for 18 prioritised statements in online supplemental files 9 and 11. Figure 4 presents the median, IQR, minimum, maximum and outlier statements for the eight criteria used to rank research statements.

Box plots of pooled Essential National Health Research (ENHR) strategy for research priority setting ranking data (18 prioritised statements) for each category question showing the third quartile (Q3) and first quartile (Q1), median, range and outliers. Statement 51 (mean score 1.8) was the only outlier in category 2 (Relevancy), criterium question 2 (C2Q2). Category 3 (the chance of success), criterium question 1 (C3Q1) had four outliers: the mean scores were high for statement 68 (mean score 2.4), statement 55 (mean score 2.3) and statement 69 (mean score 2.2) and low for statement 51 (mean score 1.6). C1Q1 and C1Q2: Category 1 Questions 1 and 2; C2Q1 and C2Q2: Category 2 Questions 1 and 2; C3Q1 and C3Q2: Category 3 Questions 1 and 2; C4Q1 and C4Q2: Category 4 Questions 1 and 2.
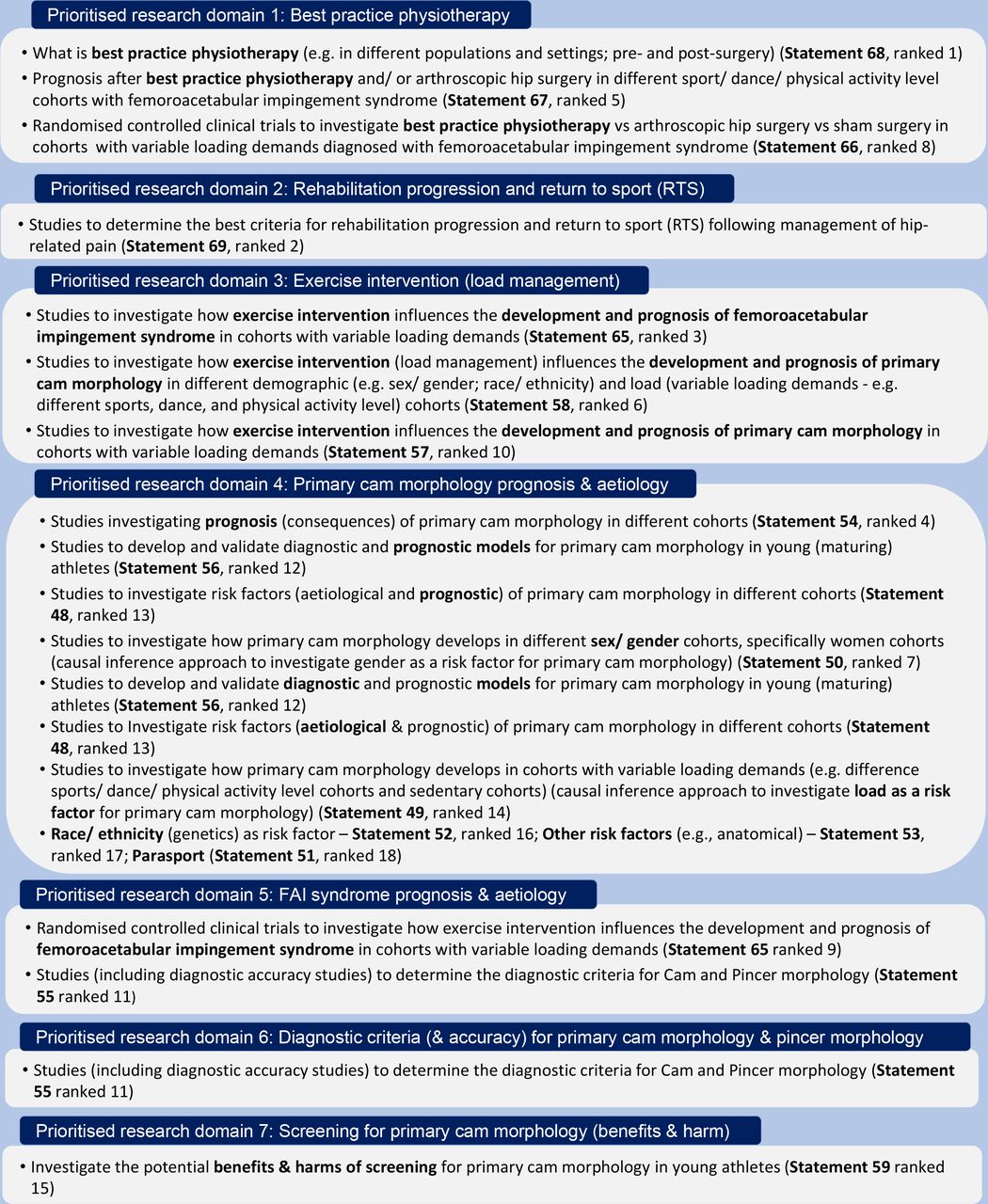
The 18 prioritised and ranked research statements, highlighted in green in table 3, outlined seven research domains: (1) best practice physiotherapy, (2) rehabilitation progression and RTS, (3) exercise intervention and load management, (4) primary cam morphology aetiology and prognosis, (5) FAI syndrome aetiology and prognosis, (6) diagnostic criteria, and (7) screening. These are medium-term to long-term research priorities (figure 5). A related infographic paper presents the prioritised research domains in the context of primary cam morphology’s natural history.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Research priorities on conditions affecting the young person’s hip, focusing primarily on primary cam morphology and its natural history (18 statements in seven domains prioritised following two Delphi rounds and further ranked according to the Council on Health Research for Development's Essential National Health Research (ENHR) strategy for research priority setting).
The Delphi panel prioritised research on best practice physiotherapy, including (1) what it is (statement 68); (2) prognosis after best practice physiotherapy and/or arthroscopic hip surgery in patients with FAI syndrome (statement 67) (however, current methods to capture outcomes are ‘controversial’), and (3) trials comparing best practice physiotherapy with arthroscopic hip surgery and sham surgery in patients with FAI syndrome (statement 66). Acknowledging the fact that ‘we already have three trials’, the panel commented on the ‘need to establish what best practice physiotherapy is’ before comparing it with other interventions. What best practice physiotherapy is, is also important for athlete-patients: ‘my experience of physiotherapy as an elite athlete was very mixed—some good, some poor’.
An ex-elite athlete panel member contextualised the importance of studying ‘best criteria for rehabilitation progression and Return to Sport (RTS) following management of hip-related pain’, (statement 69): ‘worries about RTS caused major anxiety for me’ as ‘sport was my living’.
The panel recognised the size and cost of RCTs to investigate how exercise intervention influences the development and prognosis of primary cam morphology (statements 57 and 58) and FAI syndrome in cohorts with variable loading demands (statement 65). To address these challenges, they emphasised ‘pooling of resources/skills’, and ‘to start with one sport/cohort and do this well before extending outwards’. In addition, it is ‘very hard to get people to change behaviour regarding sports activities’. Although prioritised, there are at least four challenges to plan and do ‘cohort studies to investigate how exercise intervention influences the development and prognosis of primary cam morphology in cohorts with variable loading demands’ (statement 57). First, to date, exercise interventions ‘are ill-defined’. Second, cohort studies might not be the best study design ‘to study the effects of interventions’. Third, ‘variable-loading demands’ may be ‘difficult to determine’ in some sports. Finally, it is necessary to ‘consider load outside of the structured sporting environment’.
The Delphi panel prioritised prospective cohort studies to investigate primary cam morphology and FAI syndrome risk factors (aetiological and prognostic). Acknowledging the importance of prospective research on aetiological risk factors for primary cam morphology (statements 48 and 53), the panel also prioritised cohort studies on how the morphology develops in different sex/gender (statement 50), race/ethnic (statement 52) and variable load demand cohorts (statement 49), including parasport (statement 51), especially ‘multicentre studies that would really improve knowledge and patient care’.
Primary cam morphology prognosis studies (statements 48 and 54) are ‘vitally important’; however, panellists acknowledged four challenges. First, these studies are ‘really difficult’ to plan and execute. Second, ‘funding is always an issue’. Third, these are long studies and, therefore, have a ‘lower chance of success’. Finally, scientific evidence is lacking ‘for interventions to modify disease trajectory’.
While prioritising ‘studies to develop and validate diagnostic and prognostic models for primary cam morphology in young (maturing) athletes’ (statement 56), panellists commented that ‘the field is not ready’ yet and that ‘identification of risk factors (eg, explanatory analyses)’ should be prioritised. Another panellist, ‘considering agreement on cam morphology being a finding and not a diagnosis’, suggested rephrasing the statement to ‘develop and validate measurement methods and prognostic models’.
Panellists emphasised two important considerations for ‘prospective cohort studies investigating risk factors for the development and prognosis of femoroacetabular impingement (FAI) syndrome in different cohorts’ (statement 64): ‘the impact on stakeholders and their involvement’, and whether agencies/governments will ‘see this as a priority for funding’.
The panel emphasised five important considerations for primary cam morphology and FAI syndrome risk factor research. First, it is crucial, ‘to ensure there is more research in this space around females given the lack of current data’. Second, race/ethnicity is a ‘hot topic right now’ and ‘a difficult construct, especially when treated categorically’. Resources are required ‘to adequately sample diverse populations’. Third, research on variable loading demands is challenging. It should focus on ‘the effect of different loading patterns as it may be possible to modify loading in specific athletic populations’. However, it is difficult ‘to accurately capture’ training loads and ‘tough’ to get stakeholder ‘buy-in’. For example, there is ‘no way’ to convince disciplines such as dance ‘to change something in terms of load to prevent the development of health problems’. Fourth, parasport, although ‘incredibly important’, is a ‘difficult population to study because infrastructure to support is not as strong’, and large enough sample sizes is a ‘big challenge’. Finally, it is crucial to consider available data for example, Generation R Study in the Netherlands, ‘a prospective general population study in children on which we have prospective follow-up imaging data of the hip of around 3000 children at ages 9, 13 and 17 years (the latter is ongoing)’.
Research to determine diagnostic criteria for cam and pincer morphology, including diagnostic accuracy (statement 55), although prioritised by the panel, ‘may focus too much on a dichotomous view’ rather than ‘degrees (literally) of risk’. While agreeing ‘consensus is needed regarding a gold standard diagnostic tool if possible’, this research needs to be ‘carefully developed/investigated’ to focus on ‘imaging outcomes’ that are ‘correlated with clinical outcomes’. A panellist questioned whether ‘a set of very clear diagnostic criteria’ is possible ‘as FAI syndrome is a complex 3D dynamic problem’.
Studies to investigate the potential benefits and harms of screening for primary cam morphology in young athletes (statement 59) ‘isn’t as important as some of the other research priorities’; however, this research ‘should be taken very seriously and involve all stakeholders’.
Dissent analysis (online supplemental file 11). Outlier analysis: 2 outliers for 16 of 38 research priority statements did not influence group consensus or non-consensus. Bipolarity analysis: There was no bimodal distribution in the overall scoring of research priority statements. Stakeholder group analysis: The average round 2 scores were significantly different for the physical therapist stakeholder group compared with the radiologist stakeholder group for statements 61, 74 and 75; for the physical therapist stakeholder group compared with researcher stakeholder group for statements 58, 61, 65, 68, and 74, and physician stakeholder group compared with radiologist stakeholder group for statements 61 and 74.
Results of the online Interacting Group Process are summarised in box 1 and online supplemental file 12.
Dissemination and implementation
This study informed the design of two educational events to engage stakeholders, disseminate the latest evidence and stimulate debate: the Oxford-Aspetar-La Trobe Young Athlete’s Hip Webinar Series (online supplemental file 5) and the YAHiR Collaborative’s Young Athlete’s Hip Symposium and Research Meeting (online supplemental file 13a and 13b) a 2-day event at Worcester College, Oxford (22–23 September 2022). The Symposium on 22 September focused on dissemination and discussion of the Oxford Delphi consensus studies, while the Research Meeting on 23 September 2022 discussed plans and strategies to implement and evaluate the impact of the prioritised research agenda.
Discussion
An international Delphi panel of expert clinicians, athletes, patients and their representatives, and researchers—representing the YAHiR Collaborative—agreed on set of research priorities on conditions affecting the young person’s hip focusing on primary cam morphology and its natural history, reported here following REPRISE guidelines.7 They outlined seven research domains: (1) best practice physiotherapy, (2) rehabilitation progression and RTS, (3) exercise intervention and load management, (4) primary cam morphology aetiology and prognosis, (5) FAI syndrome aetiology and prognosis, (6) diagnostic criteria, and (7) screening. This consensus serves as a roadmap for researchers, policy-makers and funders to prioritise research dedicated to reducing the cost and burden of conditions affecting the young person’s hip, including hip disease related to primary cam morphology.
In what follows, we discuss the Delphi panel’s opinions on a prioritised research agenda and summarise how agreement and areas of tension and dissent might inform future work—a more rigorous, inclusive and evidence-based approach to research on primary cam morphology and its natural history. This consensus builds on recent consensus statements6 18 19 21–24 and a primary cam morphology concept analysis5 and consensus (Oxford consensus study, part 1).
Best practice physiotherapy is central to the treatment of hip-related pain in active adults, crucial to the understanding of effective treatment options for FAI syndrome, yet elusive and contested. The panel recommended research to (1) clarify what best practice physiotherapy is, (2) illuminate how it influences FAI syndrome prognosis and (3) reinvestigate its position as an effective treatment option compared with hip arthroscopy in patients with hip-related pain. First, practitioners and patients are confused by an elusive definition for best practice physiotherapy. A recent consensus on physiotherapist-led treatment for young to middle-aged active adults with hip-related pain recommended treatments that are exercise-based of at least 3 months duration and recommended further research to investigate optimal frequency, intensity, time, type, volume and progression of exercise therapy.18 Second, heterogeneous physiotherapist-led interventions might improve pain and function when compared with other non-surgical treatments or sham treatments in young and middle-aged adults with hip-related pain (including FAI syndrome); however, no high-quality trials exist to cement its superiority.37 Finally, the only three RCTs comparing hip arthroscopy with prescribed physiotherapy38–40 were compromised by out-of-date exercise therapy programmes.41 New trials should do better.
The panel prioritised studies to determine best criteria for rehabilitation progression and RTS following management of hip-related pain. Such a study recently investigated RTS after criteria-based rehabilitation for acute adductor injuries.42 RTS is complex, sport-specific, multifactorial (depending, eg, on the intervention) and an exercise in risk management.43–49 The Delphi panel emphasised six considerations for rehabilitation and RTS studies, including (1) athlete expectations, (2) intervention quality, (3) career stage, (4) type of sport, (5) athlete contract status, and (6) athlete support structures.
The panel prioritised studies to investigate the role of exercise intervention (load management) on the development and prognosis of (1) FAI syndrome and (2) primary cam morphology. This should involve different demographic and load cohorts and include studies to develop and validate diagnostic and prognostic models for primary cam morphology in young athletes. While these studies should involve different sport, dance and physical activity cohorts, the panel highlighted the importance of prioritising prospective research in girls’/women’s sport. To date, few prospective cohort studies investigated how [primary] cam morphology develops in athletes. However, none involved girls/women athletes, and only one involved a control group.50–54 Finally, load intervention studies involving maturing athletes are easier said than done; they ‘may be unwilling to reduce participation in their preferred sport’.
Diagnostic criteria for cam and pincer morphology are contested. The results of a recent systematic review to determine the diagnostic accuracy of clinical tests for cam or pincer morphology in individuals with suspected FAI syndrome were inconclusive due to high risk of bias and low statistical precision of included studies.55 There is to date no agreement on a radiographic definition of cam or pincer morphology. This Delphi panel agreed that an alpha angle threshold of ≥60 degrees to classify cam morphology (Oxford consensus study, part 1), recently proposed in a systematic review56 and another consensus,22 is appropriate; however, further research should verify this.
Screening for primary cam morphology is contentious. The panel acknowledged the risk of harm—overdiagnosis and overtreatment—of ‘a normal finding’, prevalent in many athletes. Screening might benefit ‘a small percentage of those with primary cam morphology who go on to develop significant hip problems later in life’, offering them ‘preventative support at an earlier stage’. The WHO’s Wilson-Junger criteria should inform whether screening is appropriate or not.57
Although the Delphi panel did not prioritise qualitative or mixed-methods studies to ‘explore perspectives/preferences/attitudes/concerns/experiences of primary cam morphology and FAI syndrome stakeholders’ (statements 61 and 74), mixed stakeholder groups highlighted the importance of ‘understanding a patient’s journey’. They emphasised the importance of involving stakeholders in coproduction—especially athletes, parents and coaches. Stakeholder discussions underscored the fertile ground for coproducing qualitative research, especially with minoritised populations, to address pertinent questions.58 Taking an evidence-based research approach, these studies should build on the results of systematic reviews and qualitative evidence synthesis relevant to the specific question.59
How agreement on a prioritised research agenda advances research on primary cam morphology and its natural history?
Strong consensus on primary cam morphology’s conceptual and operational definitions, taxonomy and terminology reported and discussed in a linked paper (Oxford consensus study, part 1) empowers researchers and their patient and public partners to do more rigorous research—research that is more credible, consistent, replicable, valid, and of higher quality.8 60 61 Combining rigorous research with consensus on a prioritised research agenda catalyses focused, high-quality research that is systematic in its inquiry, employs appropriate design and asks challenging questions that matters.62 This consensus informs future research priorities, illuminating challenging questions that are relevant to the minoritised, including athletes and athlete-patients. It also invites authentic collaboration, setting the scene for a more inclusive approach to research.
Inclusive primary cam morphology research, adapting Walmsley and Johnson’s (2003, p. 16) core criteria for inclusive research, should ‘address issues which really matter … and which ultimately leads to improved lives for them’, ‘access and represent’ the patient’s views and experiences and reflect that patients ‘need to be treated with respect by the research community’.63 Research on primary cam morphology and its natural history continue to minoritise important patient-athlete populations—women, children and parents, para-athletes and athletes from the Global South. Patient partners are to a large extent absent from the research process. It is worth emphasising the difference between doing inclusive research, ‘a thing with criteria that define it’ and ‘doing research inclusively’.64 The latter emphasises doing—a fluent and developmental process. Doing primary cam morphology research inclusively means the minoritised, including athletes and athlete-patients are not merely ‘involved’ at every stage of research, but in charge as partners with power—exerting some control over all decisions. This is doing research that aims for the top rungs of Arnstein’s ladder of citizen participation—partnership, power and control.65 66 Mere involvement of patients risks non-participation (eg, manipulation as members of ‘advisory boards’) or tokenism67 (being assigned but informed, or consulted and informed, or placated—pacified by the veneer of involvement). Practically, this means the minoritised should be involved in and in charge of the process of research on primary cam morphology and its consequences, including crafting and disseminating new knowledge—a process that demedicalises and empowers. This inclusive partnership provides a powerful foundation for evidence-based research.
Evidence-based research uses ‘prior research in a systematic and transparent way to inform a new study so that it is answering questions that matter in a valid, efficient and accessible manner’, minimising clinical health research that is unnecessary, irrelevant, unscientific, wasteful and unethical.68–70 However, Anjum et al (2020) appealed to the Evidence Based Medicine community to expand their notion of ‘evidence’. First, as ‘evidence is typically evidence of causation’, evidence-based researchers ‘need to tackle the problem of causation head on’ to better understand ‘what is meant by “evidence,” what is the “best available evidence” and how to apply it in the context of medicine’. Second, researchers should appreciate that multiple methods are needed to establish causation—not only the statistical approaches of randomised controlled trials and systematic reviews of trials. Third, researchers should use different types of evidence (eg, case studies and case reports) to inform ‘causal evidence’. Last, researchers should use patient narratives and phenomenological approaches as tools to look beyond evidence such as symptoms and outcomes.71 Researchers should also specify their causal intent, when relevant, and use language consistent with that intent when reporting their studies.72 Consensus on a prioritised research agenda on conditions affecting the young person’s hip, underpinned by an evidence-based approach to research, applying a more inclusive lens to the notion of ‘evidence’ (and knowledge coproduction), is a strong foundation for higher research value and less research waste. However, an important step is effective dissemination and implementation of the prioritised research agenda.
The YAHiR Collaborative values transparent and reproducible research, central to the aim of this study to inform a more rigorous, inclusive and evidence-based approach to research on primary cam morphology and its natural history. We invite scrutiny and critique, foster equal opportunities and share study data as open access published manuscripts and supplementary files (Oxford consensus studies, parts 1 and 2) or documents associated with an Open Science Framework–registered study project. We invite readers to engage with the material, participate in the dissemination and collaborate to cocreate knowledge that matters. Open science aims to make scientific knowledge (in different languages) openly available, accessible and reusable for everyone. Our approach reinforces quality and integrity, collective benefit, equity and fairness, diversity and inclusiveness—the core values of open science.73
Dissemination and implementation
Collaborative work to disseminate and implement the findings of this study was essential, not only to the ethical conduct of future research but also to coproduce new knowledge.74
Oxford-Aspetar-La Trobe Young Athlete’s Hip Webinar Series
This Delphi study was a catalyst for authentic involvement of Patient and Public partners. We codesigned and codelivered, with members of the Patient and Public Involvement Group, Webinar 9 of the Oxford-Aspetar-La Trobe Young Athlete’s Hip Webinar Series. The process emphasised collaborative and inclusive work beyond ‘involvement’—PPI colleagues took charge. We disseminated the early study results in Webinar 10 (agreement on primary cam morphology definition, terminology, taxonomy and imaging outcomes) and Webinar 11 (prioritised research agenda). These webinars were recorded and online access were provided to registered webinar participants, and the Oxford Delphi consensus panel.
Young Athlete’s Hip Research Collaborative Symposium and Research Meeting
The YAHiR Collaborative’s 2-day Symposium and Research Meeting (22-23 September 2022) built on the webinar series. The focus of the meeting was to disseminate and discuss the results of the Oxford Consensus Study among all stakeholders (athletes, patients, parents and coaches, clinicians and researchers), deliberate areas of ongoing tension and dissent and collaborate to implement the consensus by developing and curating resources, as well as sharing and aggregating large datasets. The results of the Research Meeting will be reported in a seperate paper.
Strengths and limitations
We discussed strengths and limitations to the Delphi method in a linked paper (Oxford consensus study, part 1). We anticipated survey fatigue—not completing the survey or reluctance to participate when faced with extensive and complicated surveys—as a possible major limitation.75 The Delphi and ENHR ranking exercise surveys were long and potentially complicated. We introduced four measures to mitigate participant fatigue. First, we structured the Delphi survey in five domains. Second, we invested time to optimise statement wording and kept the statements and survey structure the same for both Delphi rounds. Third, we authentically engaged participants, including PPI group members, through a webinar series described above, and additional online information and discussion sessions. Last, we divided the 18 research statements for the ENHR ranking strategy between three surveys of five to seven statements per survey. All 65 participants completed the two Delphi rounds and more than 40 the three ENHR surveys. A major strength is the large, international panel representing six stakeholder groups, including a PPI group. Although some statements (and domains, eg, imaging outcomes) required technical knowledge, potentially limiting some panellists’ ability to answer, we invested time to share relevant knowledge and allowed the option ‘not able to score’. Acknowledging that a spectrum of expertise is key to inform a group’s opinion, we applied the more inclusive ‘closeness continuum’ to expertise.32
Research priorities are based on this diverse international Delphi panel’s opinion. Despite progress on diversity, equity and inclusion, including actively involving a PPI stakeholder group (also as coauthors), we acknowledge that more could be done. Another panel, more representative of communities that are not widely represented in the hip-and-groin research field (our Delphi panel only involved three participants from Africa, all from the same country), might have different opinions. Although all panel members completed the two Delphi rounds, panel attrition resulted in an ENHR ranking exercise panel dominated by physical therapists. This might have skewed ranking results towards research questions important to this stakeholder group.
Finally, many research statements included a method clause and referred to ‘physiotherapy’ as treatment. Panellists might have scored research topic/question-specific statements without referring to method (eg, RCT, cohort study) differently. We acknowledge our implicit bias that only physiotherapists could deliver ‘physiotherapy’ or ‘personalised hip therapy’. This is not the experience for everyone. ‘Clinician-led progressive exercise rehabilitation’ might have been a better phrase than ‘best practice physiotherapy’. Equally, ‘physiotherapist-led treatment’ might have been a better phrase to reflect contemporary physiotherapy practice. This is an important topic for further scrutiny with clinicians, researchers and patient partners.
Conclusion
Building a more rigorous, inclusive and evidence-based research ecosystem is essential, but it is also a deliberate, disruptive and daunting task. A diverse Delphi panel of 65 stakeholders representing six stakeholder groups agreed on the first ranked set of research priorities on conditions affecting the young person’s hip, focusing on primary cam morphology and its natural history. Although the 18 research priorities identified signal possible gaps in the current evidence base, researchers, PPI partners and clinicians should spotlight these gaps through an evidence-based approach to future research. While informing more rigorous, inclusive and evidence-based research, this consensus is a roadmap for researchers, policy-makers and funders to implement research dedicated to reducing the cost and burden of conditions affecting the young person’s hip, including hip disease related to primary cam morphology.
Ethics approval
This study involves human participants and was approved by the University of Oxford’s Medical Sciences Interdivisional Research Ethics Committee (MS IDREC)—R73576/RE001. Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @DrPaulDijkstra, @Seaniemc89, @clare_ardern, @JoanneLKemp, @AndreaBMosler, @blazey85, @TO_dpr, @azizfar, @aserner, @rwilly2003, @oke_jason, @KarimKhan_IMHA, @trishgreenhalgh
Collaborators Young Athlete’s Hip Research (YAHiR) Collaborative: Rintje Agricola; Thor Einar Andersen; Olufemi Ayeni; Ian Beasley; Mario Bizzini; Marco Cardinale; Tafadzwa Chiokwindo; Richard de Villiers (deceased); Lars Engebretsen; Tom Entwisle; Emin Ergen; Scott Fernquest; Celeste Geertsema; Mo Gimpel; Fares Haddad; David Hanff; Joshua Heerey; Per Holmich; Franco Milko Impellizzeri; Julie Sandell Jacobsen; Christa Janse van Rensburg; Ara Kassarjian; Vikas Khanduja; Stephanie Kliethermes; Cara Lewis; Travis Maak; Susan Mayes; Inger Mechlenburg; Nonhlanhla Mkumbuzi; Sofie Nelis; Antony Palmer; Theodora Papadopoulou; Marc Philippon; Lauren Pierpoint; Lindsey Plass; Noel Pollock; Michael Reiman; Nia Roberts; Nikki Rommers; Nisrine Sawaya; Toni-Jane Snoxell; Jomar Souza; Louise Strickland; Tina Taseska; Kristian Thorborg; Jane Thornton; Johannes Tol; Larissa Trease; Pim van Klij; Pieter Volcke; Adam Weir; Fiona Wilson and Mara Yamauchi.
Contributors HPD proposed the idea of a Delphi consensus study on the topic, planned and coordinated the study as part of his DPhil Evidence-Based Health Care studies. TG, MC, JLO, KMK and SG-J supervised the lead author’s DPhil studies and provided oversight to the study with other members of the Delphi Study Steering Committee (SMA, CLA, JLK, ABM, AP, PB, AS). All Steering Committee members contributed to, revised and refined the list of Delphi statements. AP co-led the Patient and Public Involvement Group with HPD, and with DPR and RWW facilitated an authentic patient’s voice throughout. AF, with oversight by JLO, contributed to the statistical analysis of the study. Although EM and VM contributed to all stages of the Delphi study, their focus was on the imaging and research priorities domains. CLA and KMK cochaired with HPD the Interactive Group Process, while ABM, AP, JLK, SG-J, DPR, SMA, EM, PB, RWW, AS and MC acted as group leads for the six small multistakeholder groups. HPD wrote the first draft of the manuscript; all listed authors contributed to reviewing, editing and revising the manuscript and have read and agreed to the submitted version of the manuscript. The Young Athlete’s Hip Research (YAHiR) Collaborative listed as 'Collaborators' were all Delphi panel members and contributed to the online Interactive Group Process and the ENHR ranking exercise.
Funding The lead author received a Kellogg College, Oxford Research Support Grant to the value of £1000.
Competing interests HPD is an associate editor for BJSM; CLA is Editor-in-Chief for Journal of Orthopaedic & Sports Physical Therapy (JOSPT); JK is an editor for BJSM; ABM is a BJSM deputy editor; AP is an editor at BMJ; KMK was editor-in-chief for BJSM from 2008 to 2020 but holds no position with BJSM or BMJ Group at present (June 2022).
SM, PB, DR, AF, AS, EM, VM, RWW, JLO, SG-J, MC and TG declare no competing interests.
Young Athlete’s Hip Research (YAHiR) Collaborative collaborators: Jane Thornton (JT) and NM are BJSM editors; KT and FW are BJSM deputy editors; LE is BJSM IPHP editor; Johannes Tol (JT), CJvR, SK, and AW are BJSM associate editors.
Provenance and peer review Not commissioned; externally peer reviewed.
Author note Equity, diversity and inclusion: The Oxford consensus steering committee (HPD, SMA, CLA, JLK, ABM, AP, PB, AS, JLO, KMK, SG-J, MK, TG), 5 women and 8 men were English-speaking (as a first or second language) white academics (11 with PhDs); 4 were physicians, 6 allied healthcare practitioners and 3 health researchers. AP represented the Young Athlete’s Hip Research (YAHiR) Collaborative’s Patient and Public Involvement Group. One resided in the Global South. Interpreting ‘diversity’ as more than representation of certain demographic groups, the steering committee ensured a diverse and informed Delphi panel, representing six multiprofession stakeholder groups, including previously minoritised groups relevant to this research field (eg, women, athletes, patients and the community, participants from the Global South). This study’s online Delphi method, with a specific focus on anonymity and access to adequate topic-specific resources, supported a more equitable and inclusive process. First, the study’s online Delphi method was more equitable (as opposed to an in-person meeting) as traditionally under-represented groups had similar opportunities to participate—levelling the playing field (they did not need to travel and could share their opinion in a ‘safe space’). Second, the study’s online Delphi method was more inclusive (referring to a positive and supportive experience) as our efforts included online meetings to share and discuss study resources and topic-specific information and giving patient and public involvement partners leading roles in all aspects of the study (including steering committee membership, active involvement in study design, leading roles in online discussions and coauthorship of study reports, including peer-reviewed papers). Finally, in addition to the steering committee members, the main authors included a biostatistician (AF), two radiologists (EM, VM) and two additional members of the YAHiR Collaborative’s Patient and Public Involvement Group (DPR and RWW). The 18 main authors include 6 women (including the senior author, TG). Richard de Villiers is deceased
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.