Article Text

Abstract
Objectives To assess within-player change in injury risk and between-player subsequent injury risk associated with concussive and common non-concussive injuries in professional rugby union.
Methods This prospective cohort study in Welsh professional male rugby union analysed within-player and between-player injury risk for five common injuries: concussion, thigh haematoma, hamstring muscle strain, lateral ankle sprain and acromioclavicular joint sprain. Survival models quantified within-player injury risk by comparing precommon (before) injury risk to postcommon (after) injury risk, whereas between-player subsequent injury risk was quantified by comparing players who had sustained one of the common injuries against those who had not sustained the common injury. HRs and 95% CIs were calculated. Specific body area and tissue type were also determined for new injuries.
Results Concussion increased the within-player overall injury risk (HR 1.26 (95% CI 1.11 to 1.42)), elevating head/neck (HR 1.47 (95% CI 1.18 to 1.83)), pelvic region (HR 2.32 (95% CI 1.18 to 4.54)) and neurological (HR 1.38 (95% CI 1.08 to 1.76)) injury risk. Lateral ankle sprains decreased within-player injury risk (HR 0.77 (95% CI 0.62 to 0.97)), reducing head/neck (HR 0.60 (95% CI 0.39 to 0.91)), upper leg and knee (HR 0.56 (95% CI 0.39 to 0.81)), joint and ligament (HR 0.72 (95% CI 0.52 to 0.99)) and neurological (HR 0.55 (95% CI 0.34 to 0.91)) injury risk. Concussion (HR 1.24 (95% CI 1.10 to 1.40)), thigh haematomas (HR 1.18 (95% CI 1.04 to 1.34)) and hamstring muscle strains (HR 1.14 (95% CI 1.01 to 1.29)) increased between-player subsequent injury risk.
Conclusion Elevated within-player injury risk was only evident following concussive injuries, while lateral ankle sprains reduced the risk. Both concussion and ankle injuries altered head/neck and neurological injury risk, but in opposing directions. Understanding why management of ankle sprains might be effective, while current concussion management is not at reducing such risks may help inform concussion return to play protocols.
- Hamstring Muscles
- Ankle
- Shoulder
- Sporting injuries
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Using a between-player analysis, subsequent injury risk is higher following concussion than non-concussive injuries in rugby union.
However, to assess whether an injury changes injury risk before and after a predefined injury, assessing within-player changes in injury risk is needed.
The within-player changes in injury risk and subsequent injury risk of other, non-concussive, common injuries in rugby union is unknown.
WHAT THIS STUDY ADDS
Concussion elevated within-player injury risk by 26%, increased the risk of head/neck, pelvic region and neurological injuries, and shortened the time to the next injury.
Lateral ankle sprains reduced within-player injury risk by 30% and decreased the risk of head/neck, upper leg and knee, joint/ligament, and neurological injuries.
Thigh haematoma, hamstring muscle strains and acromioclavicular joint sprains did not change within-player injury risk.
Concussion, thigh haematomas and hamstring muscle strains increased between-player subsequent injury risk by 24%, 18% and 14%, respectively.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
To reduce the elevated change in injury risk following concussion, objective rehabilitation assessments are needed to ensure players have fully recovered.
Ankle ligament injury rehabilitation may be able to inform concussion rehabilitation possibly due to a relationship between ankle ligament rehabilitation and a reduced risk of head/neck and neurological injuries.
Resource-limited research in male rugby union should focus their resources on concussion prevention and rehabilitation rather than other common injuries.
Introduction
Rugby union has one of the highest injury rates of any team sport,1 with match injury incidence as high as 99.1 injuries/1000 match-hours at the professional level and 200 injuries/1000 match-hours at the international level.2 3 The lower limb is the most common location for match injuries in professional rugby union,2 4 with three of the five most common injuries being thigh haematomas, hamstring muscle strains and ankle ligament sprains.2 However, a shift in injury trends has been observed, with the incidence of common upper body injuries, such as concussions and acromioclavicular injuries, increasing and common lower body injuries decreasing.2 While a change in injury location has been shown, injury rates remain high, with players often sustaining multiple injuries throughout a study period.2 3 Quantifying the risk of sustaining more than one injury has been explored through analysing subsequent injuries, which are defined as any injury occurring following an index injury, where the index injury is the first recorded injury, a predefined injury or a randomly chosen injury.5–8
Common injuries within sport, in particular concussion, have previously been investigated in relation to the occurrence of subsequent injuries. Specifically, a 38%–60% greater subsequent injury risk following concussion has been identified in comparison to non-concussive injuries in rugby union, association football and collegiate sports.5 9–11 Comparing concussion and non-concussive injuries in this way quantifies the between-player subsequent injury risk. However, it does not assess whether a player’s injury risk has changed as a result of sustaining a concussion or non-concussive injury.
Within-player changes in injury risk can be determined by quantifying the change in injury risk before and after a predefined injury. This approach is a more rigorous appraisal of whether a specific type of injury increases or decreases injury risk for a player. Using this approach, concussion elevated within-player injury risk by between 23% and 46%.5 9 Other injuries, such as hamstring strains, have high recurrent injury rates, implicating the index injury as a possible mechanism that contributes to a change in injury risk.7 The within-player change in injury risk is therefore an important consideration for rehabilitation programmes to address. Given the high incidence of injury in rugby union and the frequent nature of subsequent injuries, it is possible that other common injuries may lead to an elevated within-player injury risk. Yet, this has not been examined previously. Consequently, common non-concussive injuries warrant further investigation to provide a better understanding of the risks and improve rehabilitation programmes. Therefore, the aim of this study was to assess within-player change in injury risk and between-player subsequent injury risk associated with concussive and non-concussive injuries commonly occurring in professional rugby union.
Methodology
Participants
The first team players from the four professional male rugby union teams (Cardiff Rugby, Dragons, Ospreys, Scarlets) within Wales participated in this study. First team players were considered as the players who were selected to play for the first team squad each season. Informed consent was obtained from players (height: 1.86±0.08 m; mass: 102.0±12.9 kg) each season. Patients and the public were not involved in the design of this study.
Data collection
Injury surveillance data were prospectively collected for seven seasons, from 1 July 2012 to 30 June 2019 (inclusive). All time-loss injuries were recorded by a medical professional and injury surveillance data were submitted monthly to two of the authors (ISM and CLB). The data were cross-checked to reconfirm any discrepancies where necessary.
Injury definitions and data collection procedures used were compliant with the international consensus for injury surveillance in rugby union.12 Time-loss injuries were defined as injuries resulting in non-participation of rugby training or match play for at least 24 hours following midnight of the injury event.12 Injuries recorded were coded using the Orchard Sports Injury Classification System (OSICS) version 1013 and then grouped based on the first three letters of the OSICS code.
Data and statistical analysis
Match injury incidence for each three letter OSICS code was calculated using an estimated match exposure (ie, 15 players exposed for 80 min). Situations such as foul play, head injury assessments or time-lost due to injury, which resulted in less than 15 players on the pitch at any one time, were not accounted for. Corresponding 95% CIs were calculated using the Poisson distribution.14 The five injuries with the highest match incidence will hereafter be referred to as the ‘common injuries’. The common injury OSICS codes were: concussion (HNC), thigh haematoma (THM), hamstring strain (TMH), acromioclavicular joint injuries (SJA) and lateral ankle sprains (AJL). The severities of the common injuries were compared using the Kruskall-Wallis test due to the non-normal distribution of the data, with a post hoc test conducted using the Dunn test with Bonferonni adjustment. Significance was accepted at 0.05.
Injury risk was calculated using the Anderson-Gill extension to the Cox proportional hazard model. Within-player change in injury risk for each common injury was quantified using hazard ratios (HRs), which were calculated by comparing pre-common (before) injury risk to post-common (after) injury risk (figure 1). Between-player subsequent injury risk post each common injury HRs were calculated by comparing players who had sustained one of the common injuries against those who had not sustained the common injury (figure 1). The following processing steps were required to prepare the data for analysis. If a player was not on a team list for one of the regional teams, the injury was excluded. Each common injury was analysed separately by grouping players into those who had sustained the common injury and those who had not, with players who had not suffered the common injury forming the uncommon injury group. Those who had sustained the common injury were split into two datasets; injuries sustained pre-common injury and injuries sustained post-common injury. For the uncommon injury group, their first injury entry in the injury surveillance was chosen as their index injury. This process was then repeated for each common injury. We assumed playing exposure remained approximately constant before and after an injury, as player-specific exposure was not available for each match. A similar approach has been used in previous research.5 11 A p value of less than 0.05 indicates the data were unlikely given the null hypothesis and the HRs were unlikely to be consistent with unity (1.0). If within-player or subsequent between-player injury risk were significant, further analysis was undertaken to identify the specific body areas (head/neck, upper body, trunk, pelvic region, upper leg/knee and lower leg) and tissue types (bone, muscle/tendon, joint/ligament, neurological) that had a different injury risk. The median number of days between injury occurrences were calculated for common and uncommon injuries, in addition to 95% CI. Significance was set by 95% CI for number of days between injury occurrences not overlapping. All data was analysed using R.15 The R programming language (V.3.3.1) and the Survival library (V.2.40–1) were used to perform the survival analysis.16 17

The hazard ratio for within-player change in injury risk compares the dashed line risk pathway for players #1, #2 and #3. The hazard ratio for between-player subsequent injury risk compares the risk pathway following the injury of interest for the common injury (players #1, #2 and #3) and non-common injuries (players #4 and #5).
Results
A total of 2888 injuries were sustained by 382 players. The median (IQR) and mean (SD) injuries per player were 6 (3–11) and 7.5 (6.2), respectively. Concussion had the highest incidence of all common injuries, with the other four showing a similar incidence to one another (table 1). Based on days lost to injury, thigh haematomas had a lower severity than all other common injuries (lateral ankle sprains: z=6.9, p<0.001; concussion: z=−7.8, p<0.001; acromioclavicular joint injuries: z=−11.4, p<0.001; hamstring strains: z=−12.4, p<0.001). Concussion and lateral ankle sprains had a lower severity than acromioclavicular joint injuries (z=−6.4 and −4.1 respectively, p<0.001) and hamstring strains (z=−7.2 and −4.5 respectively, p<0.001), but were similar to each other (z=1.1, p=1.00).
The injury incidence (injuries/1000 match hours) with 95% CIs, mean and median severities (days lost) with SD and IQRs, respectively, for the five common injuries
Within-player change in injury risk
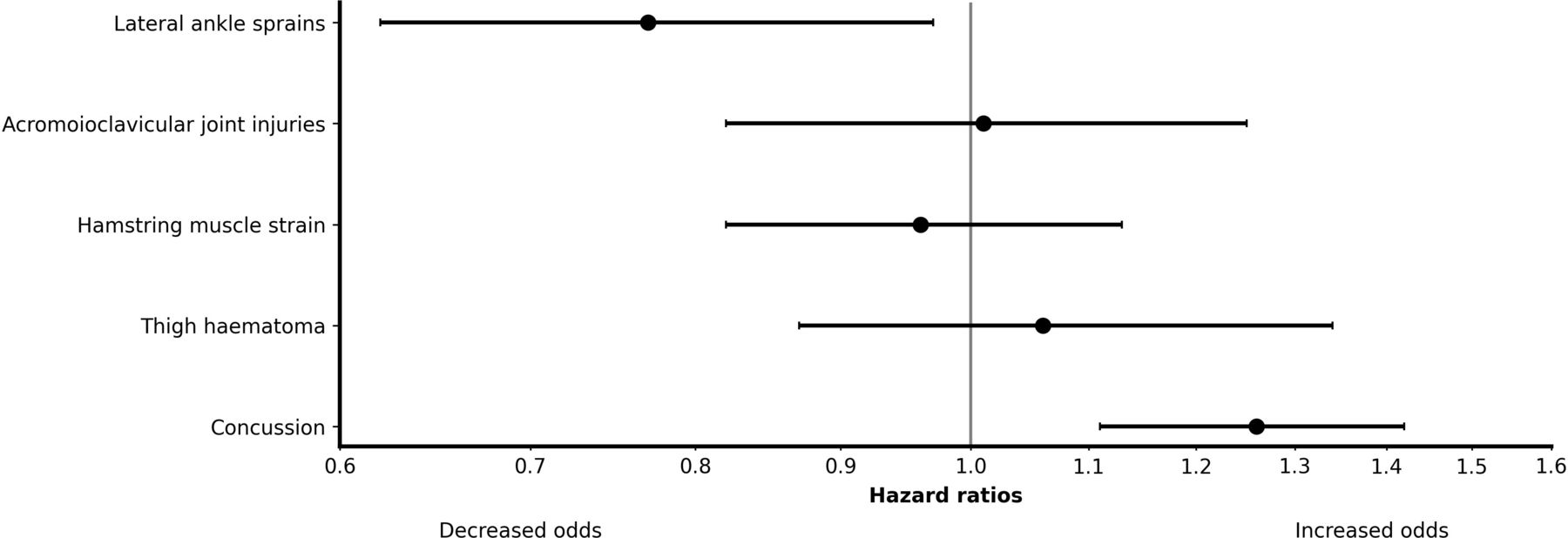
Concussion was the only injury to increase the within-player injury risk, with players at a 26% greater risk of injury post-concussion than preconcussion (HR 1.26 (95% CI 1.11 to 1.42); figure 2). In contrast, lateral ankle sprains decreased within-player injury risk by 30% (HR 0.77 (95% CI 0.62 to 0.97)). The body areas with elevated injury risk post-concussion were head/neck (HR 1.47 (95% CI 1.18 to 1.83)) and pelvic region (HR 2.32 (95% CI 1.18 to 4.54)), while the only tissue type with elevated risk was neurological (HR 1.38 (95% CI 1.08 to 1.76)). Lateral ankle sprains reduced the risk of subsequent head/neck injuries (HR 0.60 (95% CI 0.39 to 0.91)), upper leg and knee injuries (HR 0.56 (95% CI 0.39 to 0.81)), joint and ligament injuries (HR 0.72 (95% CI 0.52 to 0.99)) and neurological injuries (HR 0.55 (95% CI 0.34 to 0.91)).
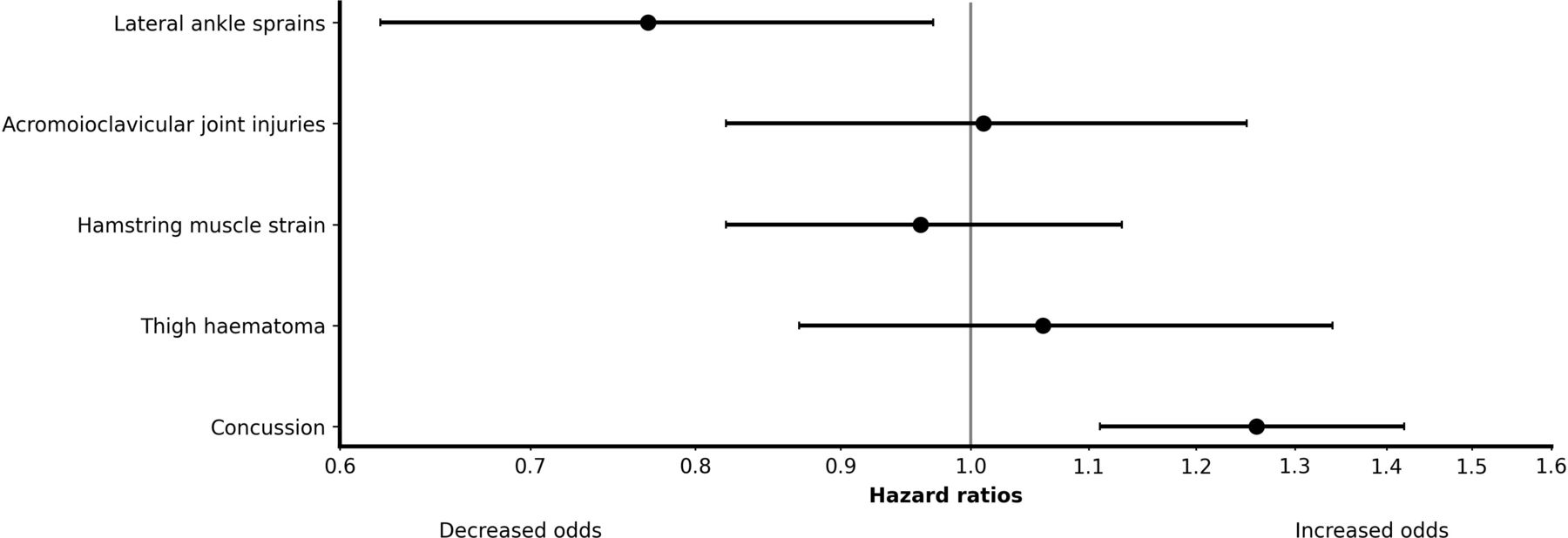
Hazard ratios (95% CI) for within-player change in injury risk for common injuries. Data are presented on a log scale.
Between-player injury risk
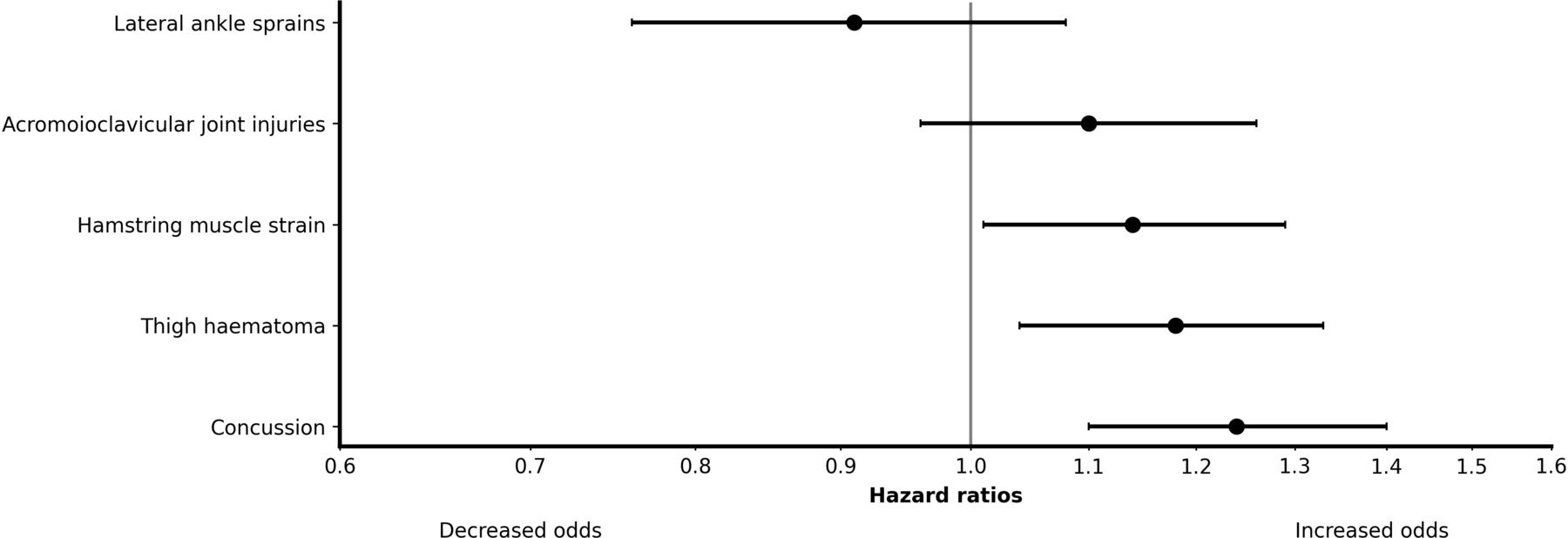
Compared with non-concussive injuries, concussion led to a 24% greater between-player subsequent injury risk (HR 1.24 (95% CI 1.10 to 1.40)). Thigh haematomas led to a 18% greater between-player subsequent injury risk than non-thigh haematoma injuries (HR 1.18 (95% CI 1.04 to 1.34)) and hamstring muscle strains had a 14% greater between-player subsequent injury risk than non-hamstring injuries (HR 1.14 (95% CI 1.01 to 1.29)). Concussion increased the subsequent injury risk of head/neck (HR 1.40 (95% CI 1.08 to 1.83)) and lower limb injuries (HR 1.38 (95% CI 1.12 to 1.69)), as well as joint/ligament injuries (HR 1.33 (95% CI 1.12 to 1.58)). There was a greater risk of muscle/tendon injuries following thigh haematomas (HR 1.25 (95% CI 1.05 to 1.49)) and hamstring muscle strains (HR 1.23 (95% CI 1.02 to 1.48)), but no significant body areas. Between-player subsequent injury risk was similar for other common injuries when compared with uncommon injuries (figure 3). Concussion led to a shorter time to next injury than non-concussive injuries, but no differences were observed in the other common injuries (table 2).
{kind=link}
{kind=link}
{kind=link}
Hazard ratios (95% CI) for between-player injury risk for common injuries. Data are presented on a log scale.
Median time (days; 95% CIs) between injury and subsequent injury of the five common injuries compared to non-common injuries
Discussion
The primary aim of this study was to assess within-player change in and between-player subsequent injury risk associated with concussive and non-concussive injuries commonly occurring in professional male rugby union. Only concussion led to an elevated within-player injury risk following its occurrence, while concussion, thigh haematomas and hamstring muscle strains had greater between-player subsequent injury risks. Concussion also shortened the time to next injury when compared with non-concussive injuries.
Within-player injury risk
This was the first study to identify that concussion was the only common injury to elevate a player’s injury risk. Specifically, it elevated within-player injury risk by 26%, while lateral ankle sprains reduced within-player injury risk by 30%, and other common injuries had no appreciable effect on within-player injury risk. The elevated risk following concussion is in agreement with previous reports5 9 11 and goes a step further in identifying that increases to within-player injury risk is a concussion-specific issue. In particular, concussion increases the risk of head/neck and neurological injuries. We hypothesise that this may be due to several factors, such as the neurological nature of concussion and rehabilitation focused on self-reported symptom resolution. There was also an increased risk of pelvic region injuries. Due to the subsequent injuries being head/neck and neurological in nature, rehabilitation needs to address disturbances to the vestibular-ocular system, postural control and ability to perform dual-tasks,18–24 which may negatively impact decision-making and skill execution during rugby. Additionally, while the physical signs and symptoms of concussion such as dizziness and headaches resolve relatively quickly, the neurological symptoms such as balance and coordination can result in more persistent impairments. This emphasises the importance of adequate rehabilitation with objective assessments10 rather than relying on symptom resolution, which the current rugby union return-to-play protocols do. For example, assessing movement execution during dual tasks (eg, walking and a cognitive task) has shown promise in identifying concussion impairments once symptoms have resolved.23 The subsequent injuries to the pelvic region may indicate that players were not appropriately physically prepared to return to match play and the associated demands involved in multidirectional sport and need to stabilise the body, potentially due to the limited active rehabilitation players are exposed to. Understanding why specific body regions do or do not show a change in within-player injury risk requires further examination.
Within rugby union the return-to-play following concussion must follow World Rugby’s graduated return-to-play protocol.25 However, the current findings suggest this protocol may require updating to adequately address undetected impairments following concussion and mitigate the change in within-player injury risk and shortened time to next injury when compared with non-concussive injuries. This supports a recent call to revise concussion return-to-play protocols, including extending the minimum time requirements to meet the rehabilitation needs.26 In addition, other example changes include greater levels of physical preparation (eg, active rehabilitation), the inclusion of proprioceptive training, objective assessments of postural control used alongside concussive symptom reporting,19 20 followed by rugby-specific assessments relating to decision-making and skill execution, and ongoing management of contact exposure following return to play. Consequently, having a multifaceted approach to concussion rehabilitation to ensure all physical and neurological impairments following concussion have been addressed could help with reducing the elevated change in injury risk.
Lateral ankle sprains led to a reduced within-player change in injury risk, meaning that the injury and subsequent rehabilitation might have had a protective effect for a player. In addition, the median severity of lateral ankle sprains was low (10 days), showing similar severity to male association football27 and concussive injuries in the current study. This suggests that very few severe (>28 days) ankle ligament injuries occurred, such as high ligament injuries or total ligament ruptures.27 28 This low degree of ligament sprain may play a role in the observed reduction in injury risk. Specifically, players may have been removed from play with a minor ankle injury to mitigate the chances of developing a more severe ankle injury. It is also possible that movement execution may be altered following an ankle injury due to reductions in plantarflexion strength. For example, lower ankle plantarflexor forces may be generated during ground contact, which could be a protective strategy limiting high speed running29 and or impact force capabilities in contact events. However, empirical data are required to verify such movement and strength effects. Rehabilitation for ankle ligament sprains can follow evidence-based recommendations, specifically an active recovery28 that includes early mobilisation30 and proprioceptive training, consequently reducing reinjury risk.31 32 It is likely that proprioceptive training may be a crucial component that facilitates the protective association of ankle injury rehabilitation, which concussion rehabilitation in rugby union could benefit from due to the known disruption of balance following concussion19 and lack of clear guidance relating to such training in the graduated return-to-play protocol.25 Further, several objective assessments can be undertaken to determine the level of function and exercise progression during rehabilitation.33 There are also ongoing management strategies (eg, bracing) that can be implemented once a player has returned to play, which can reduce the reinjury risk of ankle ligament sprains.34 The combination of all these factors are likely to have contributed to the protective effect observed.
Although previous research has shown that ankle sprains carry a high risk of reinjury,28 30 we found a lower risk of joint/ligament injuries following lateral ankle sprains. However, the reduced risk was only shown for the upper leg and knee, rather than lower leg, suggesting a direct decrease in reinjury risk was not evident. The management strategies outlined for ankle injuries differ to what is currently advocated or available for sports concussion rehabilitation,25 and the opposing effects of ankle ligament and concussive injuries with similar severities on the risk of head/neck and neurological injuries means such management strategies warrant further investigation.
The other non-concussive common injuries did not alter within-player change in injury risk. These injuries were either muscle or joint related. While we did not assess all non-concussive injuries in rugby union, given the broad range of injury types it is conceivable that other uncommon, non-neurological injuries may show similar findings. There are likely to be several possible explanations for non-concussive injuries not increasing within-player change in injury risk, such as: (1) the unique neurological alterations that occur following concussion predispose players to a greater injury risk; (2) rehabilitation protocols for common non-concussive injuries may mitigate elevated injury risk and in case the of lateral ankle sprains reduce injury risk; (3) clinical and functional screening tests for muscle, ligament and joint-related injuries enable objective criterion based return-to-play progression that does not solely rely on symptom reporting.33 35–37 Although the non-concussive common injuries did not increase within-player change in injury risk, hamstring and shoulder injuries did have higher severities than concussion. Further, hamstring strains and shoulder injuries have been shown to have high reinjury rates.38–41 Therefore, unlike concussion, the prevention strategies for these injuries should focus on the potential reinjury occurrence of the exact same injury rather than a more holistic focus on any type of injury.
Between-player subsequent injury risk
Concussion, thigh haematoma and hamstring muscle strains increased between-player subsequent injury risk by 24%, 18% and 14% respectively. In addition, concussion shortened the time to next injury compared with non-concussive injuries. Concussion between-player subsequent injury risk and shorter time to next injury has been well documented across several sports.5 9 10 When this increase in risk is combined with the change in within-player risk, it suggests that the between-player injury risk findings previously identified may be a result of within-player alterations. Conversely, thigh haematomas and hamstring muscle strains only increased between-player subsequent injury risk and not within-player change in injury risk. Specifically, both injuries increased the risk of muscle/tendon injuries. This may mean that such injuries may suffer from inappropriate injury management rather than altering internal risk factors. For thigh haematomas, this may be due to their low severity and potential to be deemed as a non-significant injury due to the minimal tissue damage incurred.2 42 Whereas, the increased muscle/tendon injury risk for hamstring muscle strains may indicate underlying injury risk factors such as strength deficits43 and sprint biomechanics44 may not have been adequately addressed during rehabilitation. Indeed strength deficits have been shown to persist for 20–50 days posthamstring muscle strain, which surpasses the median severity reported in our study.43 This may lead players to returning to play prematurely and/or dismissing symptoms. It may also mean that players who sustain thigh haematomas and hamstring muscle strains have a predisposition to rugby related injuries due to playing position, style of play or musculoskeletal factors. Further work is warranted to understand the mechanisms.
Limitations
This study focused on injuries during male professional level matches and therefore does not take into account injuries that may have occurred while playing international matches or while training. However, the risk of between-player subsequent injury risk following concussion is similar to our previous research that included both professional and international matches. Further, data show 69% of all rugby injuries occur during matches.45 Collectively, this indicates that the majority of a player’s injuries are captured through professional level match records. Yet, excluding training injuries may have underestimated a player’s injury risk in our study and requires further examination in the future. Additionally, similar research into female rugby players is warranted due to the higher risk of concussion and its severity.46 Our study provides a new approach to considering injury risk in sport. However, because individual-level exposure data were unavailable to us, we assumed that match exposure for each player was approximately constant exposure preinjury and postinjury. As an example, a player who was regularly selected to start prior to injury was assumed to be regularly selected to start following injury. We do not believe this omission increases model bias, but future studies may consider testing this assumption by combining video and or global positioning system data with injury records to quantify player-specific exposure minutes. Such measures were not available in this large longitudinal study. If exposure had been accounted for, two scenarios that differ from our assumption of constant exposure preinjury and postinjury would be possible; greater exposure or reduced exposure post injury compared with preinjury. For concussion, this would mean our model overestimated or underestimated within-player change in injury risk, respectively. Only the top-five common injuries were examined due to the number of injuries within the injury surveillance database. Including other injuries may have identified different injury trends. However, the top-five common injuries included various types of injuries (eg, contusion, muscle strain, ligament sprain) and show only neurological-related injuries (eg, concussion) cause an increase in within-player injury risk. The first three letters of the OSICS codes were used to categorise injuries, meaning only lateral ankle sprains (AJL) and hamstring muscle injuries (TMH) were analysed. Other ankle ligament sprains and hamstring tendon injuries were not examined, as they were not in the top-five common injuries.
Conclusion
In this multiseason prospective study of four male professional rugby union teams, concussion was the only common injury that resulted in elevated within-player injury risk within and shortened the time to next injury. Conversely, lateral ankle sprains led to a reduction in within-player injury risk. Concussion return-to-play protocols should be re-evaluated to mitigate the increase in within-player injury risk, particularly for head/neck and neurological injuries, and the shorter time to next injury. Given that ankle ligament sprains led to a reduced risk of head/neck and neurological injuries, principles used in ankle rehabilitation may be of benefit for concussion management, such as evidence-informed active rehabilitation, objective assessments and proprioceptive enhancement. Thigh muscle haematomas and hamstring muscle strains demonstrated a higher between-player subsequent injury risk. Understanding why players who sustain thigh haematomas and hamstring muscle strains appear to have a higher injury risk than those who do not is warranted.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Cardiff Metropolitan University 12/7/01S 15/5/02S 18-7-02S. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors would like to thank the team physiotherapists and strength and conditioning coaches that diligently recorded all the injury and exposure data.
References
Footnotes
Twitter @IzzyMoorePhD
Contributors ISM and PM conceived the study idea. JR and ISM wrote the code for the analysis. ISM processed and interpreted the data. ISM, CLB and DV prepared the first draft of the manuscript. ISM, CLB, DV, JR, BCR and PM all made substantial contributions to the revision of the manuscript prior to submission. ISM is guarantor for the work.
Funding Welsh Rugby Union. The second author (CLB) was on a financially supported PhD, funded by the Knowledge Economy Skills Scholarships 2 (KESS2; grant number 82196).
Competing interests ISM is an associate editor for the British Journal of Sports Medicine. ISM received a research grant from Welsh Rugby Union. CLB received PhD part-funding by the Welsh Rugby Union. BCR received PhD funding by the Welsh Rugby Union. PM is the Head of Medical Services for the Welsh Rugby Union.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.