Article Text

Abstract
Background Optimal strategies for massage and its use in athletes have not been conclusively demonstrated.
Purpose/study design Effects of varying duration, frequency and magnitude of massage-like compressive loading (MLL) on recovery of skeletal muscle active properties (torque angle (T-Θ) relationship) following exercise-induced muscle injury were studied.
Methods Twenty-four New Zealand White rabbits were surgically instrumented with bilateral peroneal nerve cuffs for stimulation of hindlimb tibialis anterior muscles. Following a bout of eccentric exercise (EEX), rabbits were randomly assigned to a MLL protocol of 0.25 or 0.5 Hz at 5 or 10 N for 15 or 30 min. T-Θ was obtained for 21 tibiotarsal joint angles pre- and post-EEX and post 4 consecutive days of MLL. Muscle wet weight and H&E sections were obtained following final treatments.
Results EEX produced an average 61.8%±2.1 decrease in peak isometric torque output. Differences in torque recovery were found between magnitudes (5 and 10 N; p=0.004, n=12) and frequencies (0.25 and 0.5 Hz; p=0.012, n=12), but no difference for durations (15 and 30 min) with the 0.5 Hz, 10 N, 15 min protocol showing greatest recovery 4 days post-EEX. MLL muscle (n=12) wet weight was 3.22±0.18 g, while no MLL tissue (n=9) weighed 3.74±0.22 g (p=0.029). Histological analysis showed a difference in torn fibres between low-parameter and high-parameter MLL (6.5±1.04 vs 0.5±0.29 per 0.59 mm2, p=0.005).
Conclusions Results showed a dose-response effect for magnitude and frequency of MLL on recovery of active muscle properties following EEX. Future studies will investigate underlying biological mechanisms for this enhanced recovery of muscle function.
Statistics from Altmetric.com
Introduction
Muscle soreness and weakness accompany intense or prolonged physical activity, particularly eccentric exercise (EEX) with symptoms typically peaking 48 h postexercise and lasting for up to 1 week resulting in reduction of physical activity and time away from sport.1,–,4 Although there is interest in adaptive properties of skeletal muscle following EEX in humans, studies have focused on attenuation of muscle soreness and symptoms of delayed onset muscle soreness.5,–,8
Massage is a popular complementary and alternative medicine that is being increasingly used by general public and athletes. Up to 45% of time in physiotherapy for sport-related injury and performance consists of massage treatments.9 Despite the frequency of massage use by athletes and self-reported positive effects, there is a paucity of sound evidence for efficacy of this therapy to mitigate muscle pain and weakness associated with exercise.10 A systematic review concluded that the effects of massage-based therapies on recovery from intense EEX are inconsistent across studies.11 The authors were unable to synthesise the data into definitive conclusions from case series and randomised controlled trials given the variability in type of massage as well as differences in timing of massage and rate, magnitude and duration of loading.11 Previous work in our laboratory highlights the role of inflammation in postexercise muscle damage, suggesting that modulating certain aspects of inflammation may effect the repair processes.12 A recent clinical trial in humans supports the idea that massage downregulates pro-inflammatory cytokine expression following EEX.13 Taken together, these studies suggest that further work is needed to clarify the role of inflammation following muscle injury and intense exercise. Moreover, the effects of mechanical tissue loading, such as that which occurs with massage, may have important mechanistic and clinical implications that should be considered when prescribing this modality.
Questions regarding the use of manual therapies have recently been highlighted in mathematical modelling studies quantifying the effects of applied loads to the human biceps brachii.14 Findings showed that the biceps is surrounded by a fascia much stiffer than the muscle illustrating that while relatively small loads can deform the muscle, larger forces, often outside the normal physiological range, are required to produce even small deformations of the overlying fascia.14 The different stiffness of the various soft tissues is difficult to account for in the clinical setting and may help to explain the conflicting observations on the benefit of manual therapies for treatment and prevention of soft tissue injuries associated with sport and exercise.9 ,15 ,16
Based upon previous studies in our lab showing that 4 days of massage-like compressive loading (MLL) for 30 min daily resulted in accelerated recovery of tibialis anterior (TA) isometric torque production, we hypothesised that (1) there exists an optimal MLL protocol (combination of magnitude, frequency and duration) that enhances recovery of muscle function (isometric joint torque) after a bout of intense EEX and (2) the optimal protocol of MLL of the exercised muscle results in decreased muscle wet weight, myofibre damage and cell infiltration.1 The primary goals of this study were to (1) use an experimental approach that approximates massage to evaluate the effect of varying parameters of MLL on recovery of muscle function from EEX-induced muscle damage and (2) evaluate the effect of MLL on muscle fibre damage and muscle wet weight.
Methods
Animal surgery for nerve cuff implantation and experimental design
Following Institutional Laboratory Animal Care and Use protocol approval (Ohio State University), 24 skeletally mature female New Zealand White rabbits (3.42±0.32 kg) were anaesthetised using Isoflurane (IsoSol, Vedco St. Joseph, Missouri, USA) and surgically instrumented with bilateral peroneal nerve cuffs for stimulation of hindlimb TA muscles of as previously described.1 ,17 ,18
In order to compare the effects of varying MLL duration, magnitude and frequency on recovery of active muscle properties, a 2×2×2 design was used to create eight different MLL protocols (table 1).
Massage-like compressive loading protocols
Seven days post nerve cuff implantation, each rabbit was randomly assigned to an MLL protocol defined as a frequency of 0.25 or 0.5 Hz, compressive force of 5 or 10 N and duration of 15 or 30 min. Three rabbits were assigned to each protocol, providing 12 rabbits to compare each pair of conditions, for example n=12 for 5 N and n=12 for 10 N. Loading parameters were chosen after careful scaling calculations that allowed forces used to be estimated from human massage studies.1
EEX bout and evaluation of torque-joint angle properties
Rabbits were anaesthetised and secured supine in a sling with one foot attached to a foot pedal.1 The hindlimb underwent an isometric T-Θ analysis and a bout of EEX.1 The T-Θ relationship was obtained in 5° increments from 55° to 155° (21 measurements). At each 5° increment, the foot pedal was locked in a fixed position and an isometric contraction was elicited by supramaximal stimulation (three times the α-motoneuron threshold voltage, pulse duration=0.1 ms, frequency=150 Hz, train duration=1000 msec) of the peroneal nerve. Two minutes of rest with the foot at 55° tibiotarsal angle were allowed between each measurement to minimise fatigue. The EEX bout consisted of seven sets of 10 cyclic lengthening contractions with a 2 min rest between sets. For each contraction, the ankle moved within a tibiotarsal angle of 95° to 145° of plantarflexion at 150°s−1. Muscle activation preceded stretch of the TA muscle-tendon unit by 100 ms (total stimulus train duration=433 ms). Immediately following exercise bout a repeat T-Θ analysis was performed to assess for EEX effect.
Massage (MLL) protocol
All MLL protocols began immediately after exercise and occurred daily for 4 consecutive days. The MLL bouts were approximately 24 h apart using a customised device for application of lengthwise strokes of MLL protocol.19 Following daily MLL, the animals were recovered from anaesthesia, returned to cages, given food and water ad libitum, and weighed every other day to monitor for any signs of nutritional deficiency. A final T-Θ relationship was obtained 1 day post last MLL bout to assess the effects of the 4-day MLL protocol. After completion of final T-Θ measurements, the animals were euthanised with intravenous KCL administered during deep anaesthesia (5% Isoflurane).
Statistical analysis
Using this 2×2×2 design, three rabbits were tested under each of the eight MLL protocols, which provided n=12 for comparison of the high and low condition of each parameter (magnitude, duration and frequency). A saturated linear model (analysis of variance) was used to estimate residual variance and focused on the overall effects of the three parameters. The two-way interactions and three-way interaction of parameters were explored in a sensitivity analysis. The main measure of interest was the recovery index that a MLL condition produced, defined as a contrast of peak torque at three fixed time points (pre-exercise, immediate postexercise and post 4 days of MLL).
 rmEq1
rmEq1
The denominator measured loss of torque postexercise relative to pre-exercise and the numerator measured torque post 4-day MLL protocol relative to pre-exercise. When the pre-exercise and post-MLL torques were the same, the recovery was 100% and the RI=1.0, however an RI=0 indicated no recovery from postexercise torque value.
Peak torque was also measured in the contralateral hindlimb, which received no MLL serving as a measurement control for RI. Each rabbit was used as its own control by comparing the RI for the two hindlimbs; one exercised and MLL (RI_MLL) and the other exercised, but no MLL (RI_noMLL). For the no MLL hindlimb, the same 4-day protocol (including anaesthesia) was used as for the MLL protocol, except no MLL was applied. A washout period of 7 days occurred between the completion of testing for the initial hindlimb and the exercise of the contralateral hindlimb. Twelve animals received exercise and MLL first, followed by exercise and no MLL for the contralateral hindlimb and in the other 12 animals the order was reversed. Measuring the contralateral hindlimb at the same point in time postexercise allowed for correction for natural recovery over the 4-day protocol. This adjustment was not needed to make relative comparisons of RIs across conditions, but necessary to provide an absolute estimator of recovery for each condition. A RI_adjusted value was determined by subtracting the RI of the no MLL hindlimb from the RI of the MLL hindlimb.
 rmEq2
rmEq2
In order to investigate the MLL effect over the whole tested angle range, the area under the curve (AUC) for the corresponding torques was calculated using the trapezoidal method. The same recovery index was used by substituting AUC for peak torque. In addition, the angle corresponding to the peak torque output for each condition was also compared to investigate to what extent MLL shifted the peak torque angle back to that of pre-exercise.
Histological analysis
Although both hindlimbs of each rabbit were tested, only the muscle tissue that was tested after the washout period was used for analysis to allow comparisons to be made at the same time point. There were 12 MLL tissues and nine no MLL, control tissues due to three animals without testing of the contralateral control hindlimb. Immediately after killing, the tissue was harvested, weighed, flash frozen in liquid nitrogen and carefully mounted on cork and oriented perpendicular to the long axis of the muscle. Samples were later sectioned at 8 μm thickness and stained with H&E to assess myofibre damage and cellular infiltration. Sections were viewed at 200x magnification (Nikon light microscope; Fryer Company, Huntley, Illinois, USA) in order to quantitatively measure torn fibre and leucocyte infiltration. In both longitudinal and cross-sectional images, fibres were counted as damaged if there was any evidence of membrane discontinuity. In the longitudinal sections, all cells were counted, while in the cross sections, infiltrating leucocytes were counted as those cells that completely infiltrated the fibre.1 Quantitative analysis was performed by two blinded individuals in order to test for repeatability. Two randomly selected equal 0.59 mm2 (0.89 mm×0.67 mm) areas of the specimen (midbelly of MLL muscle area) in both the longitudinal and cross sections were assessed for leucocyte infiltration of myofibres.
Results
All animals survived the entire study (approximately 1 month for each animal) without greater than 10% loss of body weight. In three animals, there were no data for the contralateral control (no MLL condition) hindlimb due to nerve cuff disruption at various stages of testing.
The EEX protocol produced an average peak isometric torque deficit of 61.8% (±2.1). There was a significant difference for the RI of the MLL hindlimb between the two magnitudes in favour of 10 N (5 N vs 10 N: RI=0.28 vs 0.76, p=0.004, n=12). The two frequencies also showed a significant difference in favour of 0.5 Hz (0.25 Hz vs 0.5 Hz: RI=0.32 vs 0.73, p=0.012, n=12). No significant difference for the two durations was found (15 min vs 30 min: RI=0.47 vs 0.58, p=0.48, n=12) (table 2).
Comparison of recovery index for massage between each of the three parameters
There were no significant interactions between or among the frequency, magnitude and duration conditions eliminating concerns about combining results across conditions to test the effects of magnitude, frequency and duration (figure 1). Comparison of RI across the conditions showed that the 0.5 Hz, 10 N, 15 min combination of MLL parameters showed highest RI (1.08).

Recovery index for massage (RI_MLL) showed a dose-dependent effect of magnitude (A) frequency (p value=0.012) and (B) magnitude (p value=0.004), but no dependence on (C) duration.
The above relative comparisons across conditions required no adjustment of RI with the no MLL hindlimb in order to identify an ideal condition for recovery of peak torque (figure 2). Analysis of RI_adjusted confirmed that the most effective MLL condition was at the 0.5 Hz, 10 N, 15 min combination. Table 3 provides the RI_MLL (MLL only) and RI_adjusted (RI_MLL relative to RI_no MLL) means and SEs. Using this adjustment, the combination of the same three conditions as seen with the RI_MLL showed 97% recovery. Two of the remaining seven conditions resulted in at least 50% adjusted recovery (0.25 Hz, 10 N, 15 min and 0.5 Hz, 10 N, 30 min).

Representative T-Θ plots demonstrating that the combinations of low conditions produces approximately the same degree of recovery as the non-massaged control, while the combination of high conditions of magnitude and frequency facilitated recovery back to and beyond the baseline (pre-exercise). These plots represent the smallest effect and greatest effect range for the massage conditions.
Recovery index for RI_MLL and RI_adjusted (n=3 for each of the eight conditions)
Area under curve
Area under the T-Θ curve (AUC) for pre-exercise, postexercise, post-MLL and no MLL measurements was examined as a secondary indicator of recovery. Similar to peak torque analysis, the combination of 0.5 Hz, 10 N, 15 min gave the highest AUC recovery index at 1.05. The correlation between peak torque and AUC was 0.91 showing high redundancy between the two measures.
Joint angle shift
The effect of the EEX bout on the torque angle curve was calculated by subtracting the mean peak isometric torque angle pre-exercise bout from the corresponding postexercise angle and an RI for joint angle shift was calculated.
Exercise produced a 4.4°±0.6 rightward shift from pre-exercise peak isometric torque angle. Four days of MLL produced an average −2.9°±0.5 leftward angular shift from the postexercise peak isometric torque angle while control, no MLL hindlimbs produced a 1.8°±0.5 rightward angular shift from postexercise peak isometric torque angle (figure 3).

The angle where peak torque is produced moves rightward due to exercise and even further rightward for the non-massaged, control condition. Conversely, massage produced a leftward shift of peak torque angle back towards pre-exercise angle.
Muscle wet weight and histology
Average hindlimb muscle wet weight for no MLL (n=9) was 3.7±0.22 g and MLL (n=12) was 3.22±0.18 g (p=0.029). The difference of peak torque output between the two magnitudes in favour of 10 N and two frequencies in favour of 0.5 Hz was further explored via histological analysis. The MLL protocols that included the combination of low and high-parameter values for both magnitude and frequency were analysed and compared for torn muscle fibres and cell infiltration (0.25 Hz, 5 N, 15 min vs 0.5 Hz, 10 N, 15 min).
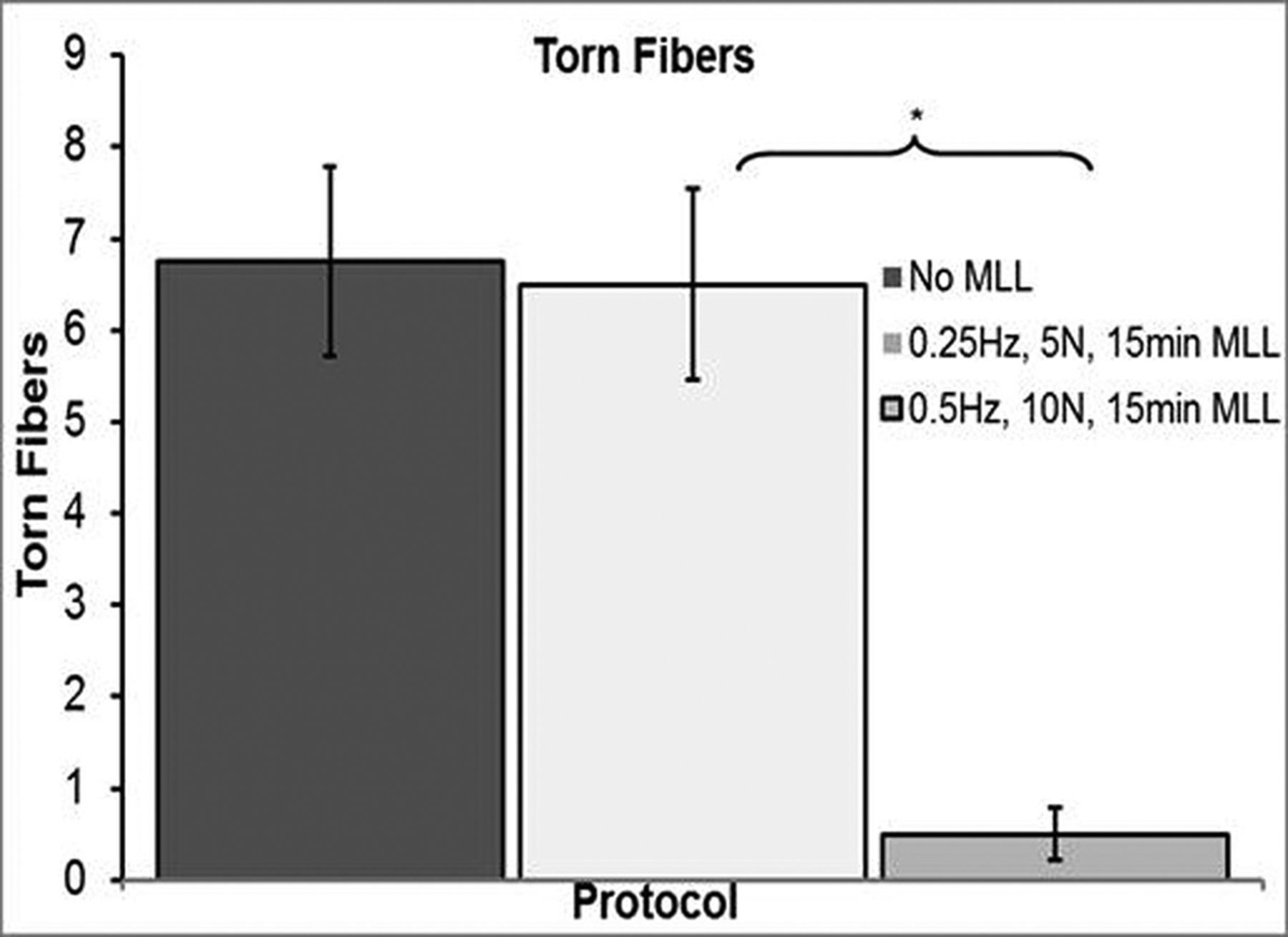
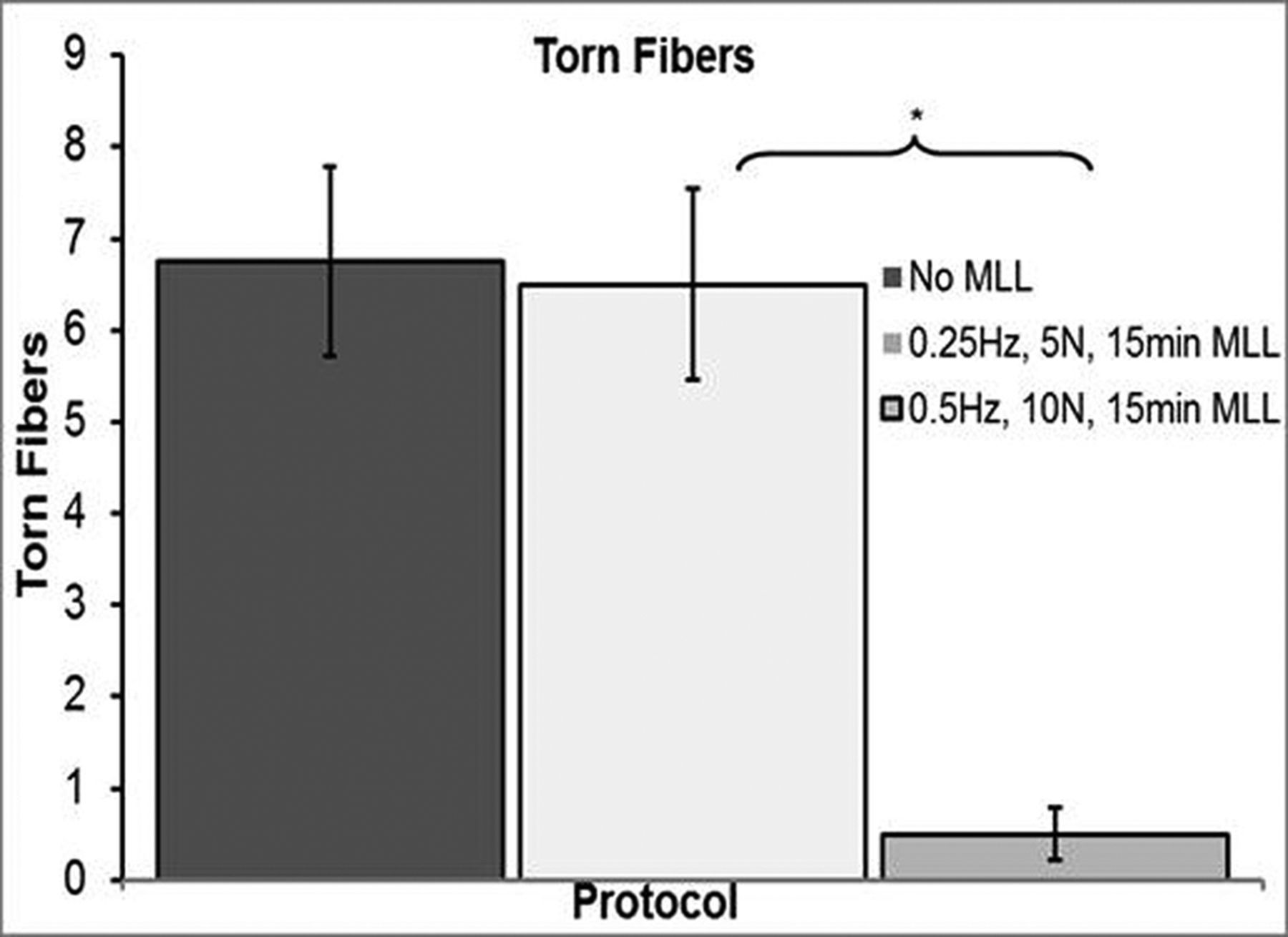
Longitudinal sections showed that the combination of low-parameter MLL resulted in minimal effect on muscle fibre damage and extent of cellular infiltration, while the combination of high magnitude and frequency MLL resulted in decreased myofibre damage and cellular infiltration (figure 4). Longitudinal sections showed a difference of average leucocytes between no MLL tissue and both low-parameter and high-parameter MLL (447.5±36.28 vs 121±12.13, p=0.001 and 81.3±20.64, p=0.0005, respectively). Cross-sectional images showed no difference (p=0.18) for leucocytes within the interstitial space between the low-parameter and the high-parameter MLL (52.5±10.36 vs 77±6.28 per area, respectively), however, a difference in infiltrating leucocytes was found (p=0.002) (36±3.18 vs 10.3±1.44 per area, respectively). Analysis of both cross sectional and longitudinal sections showed a significant difference in torn fibres between the low and the high parameter conditions MLL (5±0.41 vs 0, p=0.001 and 6.5±1.04 vs 0.5±0.29, p=0.005, respectively). Longitudinal sections showed no significant difference in torn fibres between the no MLL and the low-parameter MLL (6.75±1.03 vs 6.5±1.04, p=0.9) (figure 5).
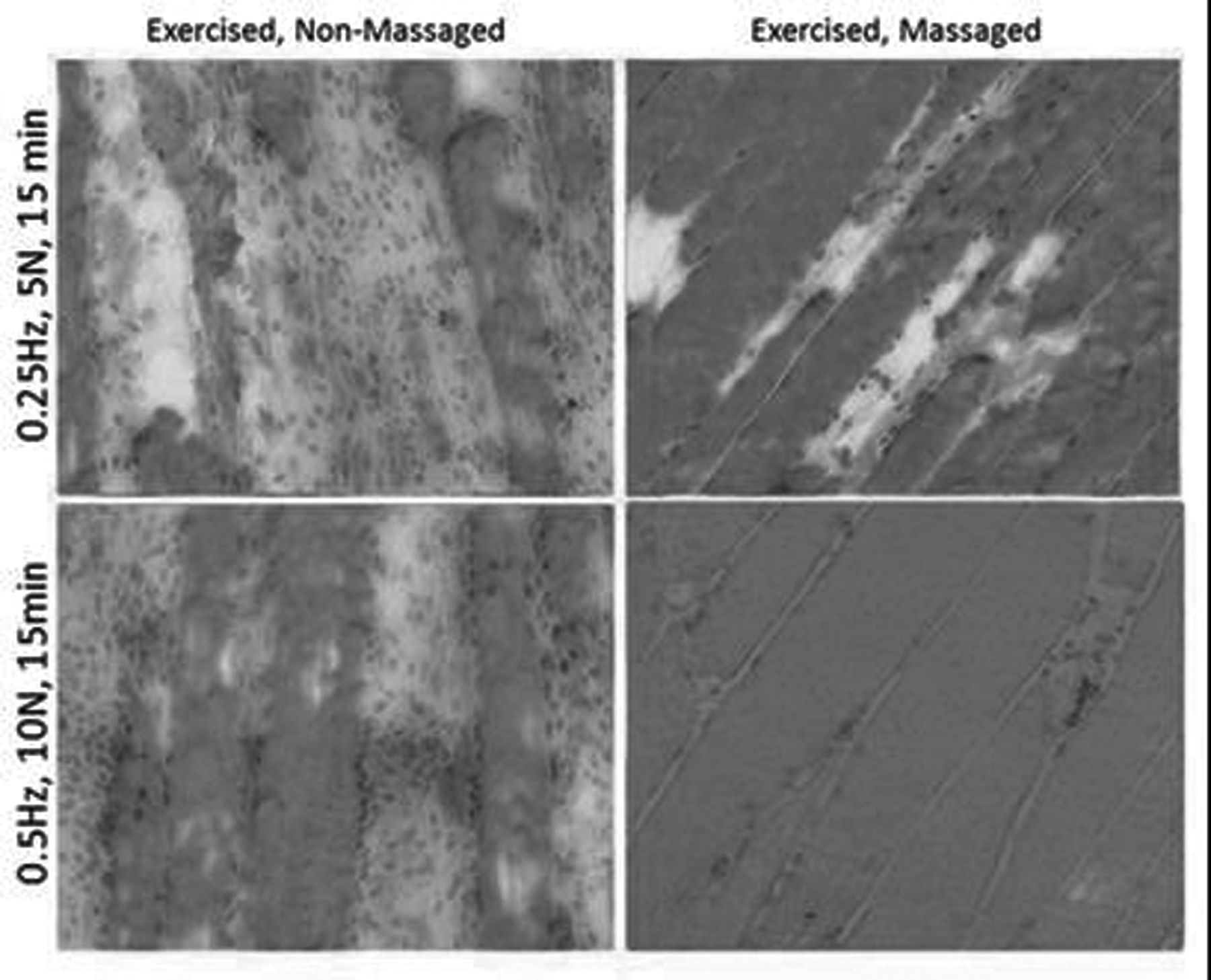
For the 0.25 Hz, 5 N, 15 min condition there was little difference between the massage and non-massed muscles. In contrast, massage lead to decreased myofibre damage and cellular infiltration for the 0.5 Hz, 10 N and 15 min condition.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Longitudinal sections showed no significant difference in torn fibres for the no massage-like compressive loading (MLL) and the 0.25 Hz, 5 N, 15 min MLL protocol. In contrast, the 0.5 Hz, 10 N, 15 min MLL protocol resulted in a significantly decreased number of torn fibres.
Discussion
This study shows the ability of MLL to accelerate recovery of muscle and joint function following EEX. Moreover, it is shown for the first time that there is a dose-dependent effect of MLL on the recovery of mechanical properties as well as histological evidence for MLL to decrease muscle fibre damage. Our in vivo animal model and self-designed device permitted loading frequency, magnitude and duration to be varied in order to examine dose-response effects of MLL on recovery of muscle function. Similar controlled experiments in humans will be important when designing interventions and determining an optimal magnitude, duration and frequency of massage in order to optimise its clinical indications for athletes.
The ability to quantify the effect of MLL parameters allowed for a detailed investigation of the effect of each parameter individually. Frequency and magnitude were shown to be important loading variables for promoting recovery of joint torque, while loading duration, at the parameters chosen (15 or 30 min), provided no significant effect. These findings suggest that greatest recovery of peak isometric torque is produced by the high condition for both magnitude and frequency (10 N and 0.5 Hz), with the low conditions (5 N and 0.25 Hz) producing significantly less recovery.
Histological analysis confirmed that the optimal MLL protocol (0.5 Hz, 10 N, 15 min) resulted in a significant reduction in torn muscle fibres and cellular infiltration as compared to both the low-parameter MLL and the no MLL protocols. Torn muscle fibres could result in lower torque production due to less cross bridge attachment and therefore force production. Moreover, the same number of torn muscle fibres for both the control and the low-parameter MLL conditions correlated with the equal effects of these two conditions on recovery of torque production. The significant increase in number of infiltrating cells in the low-parameter MLL as compared to the high-parameter MLL may be an indicator of further inflammation and perhaps the increase in number of torn muscle fibres. However, the decrease in cell infiltration and muscle fibre damage correlated with the greater recovery of peak toque observed with the high-parameter MLL condition.
The current findings support our previous work where we observed a beneficial effect of 4 days of MLL following EEX. The optimal MLL protocol (0.5 Hz, 10 N, and15 min) showed not only the largest RI_adjusted, but also greatest RI_AUC. Area under the T-Θ curve was shown to be a secondary indicator of enhanced recovery and took into account all 21 joint angles measures, as opposed to only the joint angle at which the highest peak isometric torque was produced.
The rightward shift in peak torque angle produced by the bout of EEX is consistent with previous studies that showed an increased series compliance in muscle due to EEX.1 ,6 ,20 Over the 4-day no MLL protocol, the exercised, control limb produced a further rightward shift from the postexercise peak torque angle suggesting further tissue damage. Conversely, MLL produced a leftward shift from the postexercise torque angle suggesting recovery from muscle damage associated with the bout of EEX. This recovery is further emphasised by the return of peak isometric torque values to pre-exercise level.1 ,21 ,22
We acknowledge that the injury created in our animal model may not be completely analogous to that produced in humans with EEX, with higher torque deficits than could necessarily be tolerated in humans produced by our protocol. However, limited objective data exist that quantify torque deficits experienced by humans following a single bout of EEX. Moreover, the deficits produced by our protocol allowed for differentiation between natural recovery and recovery due to the applied MLL protocol. The potential therapeutic effects of touch with massage cannot be directly addressed in our animal model, particularly given that the actual MLL and evaluation of torque production were carried out under general anaesthesia. Nevertheless, the highly reproducible conditions allowed testing of MLL effects using a minimum number of animals and systematic investigation of various loading parameters. Our results demonstrate the effects of loading on recovery of muscle function, irrespective of motor unit recruitment and potential confounding variables such as pain and motivation. There is a significant difference in recovery of function at the basic level of muscle force production, which most likely could not be achieved in a human study.
It has been postulated that the inflammatory process is responsible not only for successful repair but may also contribute to extending the initial damage process.23 ,24 This progression of injury could occur through a variety of mechanisms, including neutrophil infiltration and activation of the respiratory burst.24 In fact, studies from our lab suggest that infiltrating neutrophils may play a key role in both injury and repair.25 Collectively, these studies suggest that inflammation may play an integral role in the pathogenesis of both acute and chronic muscle dysfunction and pain and loss of muscle strength.
Despite the popular use of massage by athletes for a variety of reasons, its optimal use and indications are still not well known. The current study provides the first evidence of the effect of varying MLL parameters (magnitude, duration and frequency) on the recovery of muscle active properties following EEX-induced damage. Massage has been hypothesised to moderate inflammation, improve blood flow and reduce tissue stiffness, among other possible mechanisms. Indeed, a recent study in humans showed that a single bout of massage downregulated the expression of pro-inflammatory cytokines following EEX.13 Our data showed MLL reduced muscle wet weight and fibre damage and therefore support the findings of Crane et al.13 Future investigations will explore the effects of delayed versus immediate massage on functional recovery and inflammation as well as local blood flow to help further define the mechanism for this therapy. Our eventual goal is translating findings from our animal model to human trials in order to develop cost-effective optimal indications and strategies for the use of massage-based therapies.
What this study adds
-
Controlled laboratory setting for indepth analysis of massage-like loading parameters (magnitude, duration and frequency) and their independent and collective effects on recovery of muscle and joint function
-
Massage-like loading immediately following a bout of eccentric exercise (EEX) improves recovery of muscle and joint function
-
Massage-like loading following a bout of EEX decreases muscle fibre damage and muscle wet weight
Acknowledgments
The project described was supported by Award Number R01AT004922 (TMB) from the National Center for Complementary & Alternative Medicine. The content is solely the responsibility of the authors and does not necessarily represent the views of the National Center for Complementary & Alternative Medicine or the National Institutes of Health.
References
Footnotes
-
Funding Research reported in this publication was supported by the National Center for Complementary and Alternative Medicine of the National Institutes of Health under Award Number R01AT004922. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
▸ References to this paper are available online at http://bjsm.bmjgroup.com