Article Text

Abstract
Objective Certain exercise prescriptions for patients with cancer may improve self-reported quality of life (QoL) and self-reported physical function (PF). We investigated the effects of exercise on QoL and PF in patients with cancer and studied differences in effects between different intervention-related and exercise-related characteristics.
Design We searched four electronic databases to identify randomised controlled trials investigating exercise effects on QoL and PF in patients with cancer. Pooled effects (Hedges’ g) were calculated using Comprehensive Meta-Analysis software. Subgroup analyses were conducted based on intervention dimensions, including timing, duration and delivery mode, and exercise dimensions, including frequency, intensity, type and time (FITT factors).
Results We included 74 exercise arms. Patients who were randomised to exercise interventions had significantly improved QoL (g=0.15, 95% CI (0.10 to 0.20), n=67 exercise arms) and PF (g=0.21, 95% CI (0.15 to 0.27), n=59 exercise arms) compared with patients in control groups. We found a significant between-group difference for exercise delivery mode, with significant beneficial effects for supervised exercise interventions (g=0.20, 95% CI (0.14 to 0.26) for QoL and g=0.27, 95% CI (0.20 to 0.33) for PF), but not for unsupervised interventions (g=0.04, 95% CI (−0.06 to 0.13) for QoL and g=0.09, 95% CI (−0.01 to 0.19) for PF). No statistically significant differences in intervention effects were found for variations in intervention timing, duration or exercise FITT factors. Unsupervised exercise with higher weekly energy expenditure was more effective than unsupervised exercise with lower energy expenditure (z=2.34, p=0.02).
Conclusions Exercise interventions, especially when supervised, have statistically significant and small clinical benefit on self-reported QoL and PF in patients with cancer. Unsupervised exercise intervention effects on PF were larger when prescribed at a higher weekly energy expenditure.
- neoplasm
- quality of life
- physical activity
- exercise
- meta-analysis
Statistics from Altmetric.com
Introduction
Previous randomised controlled trials (RCTs) and meta-analyses have demonstrated beneficial effects of exercise during and following cancer treatment on muscle mass and strength, fatigue, cardiorespiratory fitness, physical function (PF) and self-reported quality of life (QoL).1–5 The effect of exercise on self-reported QoL and self-reported PF may be related to characteristics of the intervention, including the timing, duration and mode of the intervention delivery, as well as exercise characteristics, including frequency, intensity, type and time (often referred to as exercise FITT factors).6
Previous systematic reviews and meta-analyses on the effects of exercise on self-reported QoL and PF during and following cancer treatment have reported small-to-moderate effects.2 7 8 The effects of exercise may vary with the specifics of the exercise intervention.9 10 Insight into differences in effects regarding intervention-related (ie, intervention timing, duration and delivery mode) and exercise-related characteristics (ie, FITT factors) for patients with cancer is required in order to identify which exercise prescriptions are effective to improve QoL and PF.11 Unfortunately, only limited so-called second-generation studies have directly compared different intervention-related and exercise-related characteristics. For example, an RCT comparing aerobic exercise (AE) with resistance exercise (RE) in patients with prostate cancer during androgen deprivation treatment demonstrated a larger effect of RE than AE compared with usual care on QoL,10 while intervention effects did not differ significantly by exercise type in patients with breast cancer.12 Previous RCTs have also found evidence for a dose–response relationship of exercise intensity or volume on QoL4 13 and PF.9
We recently conducted an individual patient data (IPD) meta-analysis of 34 RCTs, as part of the Predicting Optimal cAncer RehabIlitation and Supportive care (POLARIS) study11 and found that exercise significantly improved self-reported QoL and PF.14 These effects were not moderated by demographic (age, sex, marital status and education) or clinical (body mass index, cancer type and treatment and presence of metastasis) characteristics.14 However, larger effects were found for supervised than for unsupervised interventions.14
While an IPD meta-analysis has the advantage of allowing standardised analytic techniques across studies and testing of interactions of the intervention with demographic and clinical characteristics at the patient level,14 it is susceptible to retrieval bias. Because not all principal investigators of the eligible studies were able to share their data, only 49% of eligible RCTs were included. Because intervention-related and exercise-related characteristics are set at study level, an aggregate data meta-analysis is appropriate to investigate optimal intervention and exercise characteristics and allows for the inclusion of a larger number of studies. Therefore, we conducted an aggregate data meta-analysis on RCTs identified in the POLARIS study, supplemented by more recent RCTs to further increase statistical power. We aimed to evaluate the effects of exercise on self-reported QoL and self-reported PF and to identify which specific intervention-related and exercise-related characteristics were effective for patients with cancer.
Methods
Identification and selection of studies
We used the original search from the POLARIS study, which was conducted in 2012, to identify eligible studies11 and updated this search in January 2017. The study protocol of the POLARIS study was registered in PROSPERO in February 2013 (CRD42013003805). Details of the search strategy can be found elsewhere.11 Briefly, electronic databases of PubMed, Embase, PsycINFO and CINAHL were searched using keywords and MeSH terms related to neoplasms, physical fitness, exercise therapy, quality of life, randomized controlled trial and adolescent. Other sources (systematic reviews, meta-analyses, personal communication with experts, collaborators and colleagues) were searched to identify additional studies. After removing duplicates, studies were screened by title and abstract, and full-text articles were assessed for eligibility. Studies were included if the study: (1) was an RCT; (2) included adult (≥18 years) patients with cancer; (3) evaluated the effects of an exercise intervention compared with a wait-list, usual care or attention control group; (4) included QoL and/or PF as a primary or secondary outcome measure; and (5) was written in English, German or Dutch. Because the search update yielded only one study evaluating exercise prior to cancer treatment, we excluded this RCT from the current meta-analysis.
Quality assessment
The quality assessment was performed by two independent reviewers (MGS and LMB) using the Cochrane Collaboration’s tool for assessing risk of bias.15 Each study was rated on: (1) random sequence generation; (2) allocation concealment; (3) incomplete outcome data; (4) incomplete reporting; (5) adherence; and (6) contamination as other potential sources of bias, based on published papers and documentation in trial registries. The quality for each item could be rated as ‘high’ (+), ‘low’ (−) or ‘unclear’ (?), based on the criteria presented in the online supplementary table 1.15 Items related to blinding were not included because blinding of participants and personnel is typically not feasible for exercise interventions. The rating of blinding of outcome assessment was omitted because QoL and PF are subjective constructs, measured using self-report questionnaires. Quality assessments of both reviewers were compared, and disagreements were resolved by discussion.
Supplementary file 1
Data extraction
Two independent reviewers (MGS and LMB or MGS and TMA) extracted information about the country where the RCT was conducted, the sample size, cancer type, mean age, sex, type of control group and the questionnaires used to measure QoL and PF, as well as the timing, mode and duration of intervention delivery and exercise FITT factors.
Outcome measure
Both QoL, including general health, global and overall QoL and PF were self-reported. The general health and PF subscale from the generic Short-Form 36 (SF-36)16 were used as measures of self-reported QoL and self-reported PF, respectively. The total score from the Quality of Life Index17 and the Spitzer QoL uniscale18 were used as measures for QoL. The global QoL and PF scales from the disease-specific European Organisation for Research and Treatment of Cancer QLQ-C30 questionnaire19 and Cancer Rehabilitation Evaluation System short form20 were used as measures of self-reported QoL and self-reported PF. The total score from the Functional Assessment of Cancer Therapy-General (FACT-G)21 was used as a measure for self-reported QoL, and the physical well-being scale was used as a measure of self-reported PF. These questionnaires are reliable and valid measures of QoL and PF.16–21 If both a generic and a disease-specific questionnaire were used to measure QoL and PF, we included results from the disease-specific questionnaire in the analyses. In cases where the total QoL score from the FACT-G questionnaire was not presented separately from the results of the tumour-specific modules (eg, total FACT-Breast or FACT-Prostate score), we used the latter score as a measure of QoL. In cases where the PF subscale of the SF-36 was not reported, the physical component summary score was used in the pooled analyses on PF.16
Statistical analysis
We calculated effect sizes for all individual studies by subtracting the average postintervention score of the control group from the average postintervention score of the intervention group and dividing the result by the pooled SD of the intervention and control group.22 All effect sizes were pooled using Hedges’ g, thereby adjusting for studies with a small sample size.23 Using Cohen’s convention, we interpreted an effect size of 0.2 as small, 0.5 as moderate and 0.8 as large.24 25 When average scores or SD were not reported, we investigated whether other statistics could be used to calculate effect sizes (ie, average scores and 95% CI, between-group differences and p values). When results on self-reported QoL or PF were reported incompletely, the principal investigator of the study was contacted. Because the samples and interventions were expected to be heterogeneous, effect sizes were pooled with a random effects model, taking any systematic difference in the effects between the studies into consideration. The I² statistic was reported as an indicator of heterogeneity, with an I² of 25% representing low, 50% representing moderate and 75% representing high heterogeneity.26 Studies were considered outliers if the 95% CI of the effect did not overlap with the 95% CI of the pooled effect and were excluded from further analyses. All analyses were conducted using Comprehensive Meta-Analysis software (V.2.2.064).
We studied differences in effects between subgroups based on intervention timing (categorised into during, following and combined during and following cancer treatment according to the physical activity and cancer control framework developed by Courneya and Friedenreich27), duration (categorised into ≤12, >12–24 and >24 weeks), delivery mode (ie, supervised when multiple face-to-face supervised exercise sessions over time were included vs unsupervised when there was no instructor or exercise specialist present during exercise) and exercise FITT factors. Exercise frequency of supervised exercise sessions was dichotomised into <3 and ≥3 times/week and unsupervised interventions into <5 and ≥5 times/week. Exercise intensity was categorised into low and low-moderate versus moderate versus moderate-high and high intensity using the American College of Sports Medicine guidelines (online supplementary table 2),28 exercise type was categorised into AE, RE, AE+RE and RE+impact loading exercises (ie, two-footed jumps with weighted vests) and exercise time (ie, session duration) into ≤30, 30–60 and >60 min. In case a statistically significant difference in effects was found between subgroups, we reported the effects stratified per subgroup. Meta-regression analyses were used to study whether the effect was influenced by the weekly exercise volume (ie, frequency×time) and weekly energy expenditure (ie, frequency×intensity× time). To estimate intensity, we used metabolic equivalents (METs) in which a value of 1.5 METs was used to indicate low intensity, 3 METs to indicate low-to-moderate intensity, 4.5 METs for moderate intensity, 6 METs for moderate-to-high intensity and 7.5 METs for high intensity exercise.29 We reported z-values, which express the statistically significance of the slope of the relationship between the variable (ie, exercise volume or exercise intensity) and the effect size. As there is some evidence that the effects of exercise on QoL and PF vary with cancer type,8 10 12 we checked whether there were differences in effects between exercise intervention characteristics across cancer types and performed a sensitivity analysis in studies that only included patients with breast cancer as the majority of included RCTs (44%) focused on this type of cancer.
Supplementary file 2
We investigated publication bias by inspecting the funnel plot and calculated the effect size with a correction for possible publication bias using Duval and Tweedie’s procedure.30 This procedure trims (removes) studies in case of asymmetry in the funnel plot, estimates the true ‘centre’ of the funnel and replaces (fills) the omitted studies around the centre. A statistically significant dispersion between the true effect size and the calculated effect size after correcting for possible missing studies or an asymmetry in the funnel plot, calculated using Egger’s test, could suggest publication bias. An alpha level of p≤0.05 was applied as the criterion for statistical significance.
Results
Description of study inclusion (figure 1)
The original search from the POLARIS study resulted in 69 RCTs investigating the effect of exercise compared with a control group, all of which were included in the current meta-analysis. The search update identified 389 additional studies of which 33 were eligible. We also included two additional studies via personal communication. After removing duplicates (n=18) and unpublished RCTs (n=2), 84 studies were retrieved of which 910 12 31–37 studies investigated 2 exercise arms, leading to a total of 93 exercise arms that were compared with a usual care, wait-list or attention control group.

Flow chart of study inclusion. *Studies were not yet published in 2012; however, within POLARIS, we maintained contact about the study completion date, and these studies were included at a later stage. **Data from two studies were included in POLARIS but full text is not yet available. POLARIS, Predicting Optimal Cancer RehabIlitation and Supportive care; QoL, quality of life; RCTs, randomised controlled trials.
The principal investigators of 26 studies were contacted because of incomplete reporting of both QoL and PF data, and 21 principal investigators were contacted because only self-reported QoL or PF was reported. After personal communication, we obtained additional information for 1712 31 32 35 36 38–49 studies, leading to an exclusion of 1834 50–65 exercise arms. Finally, this meta-analysis included 66 RCTs, investigating 74 exercise arms (n=6509 patients), of which 71 exercise arms examined QoL and 64 exercise arms examined PF.
Quality assessment of studies included in the meta-analysis
A random sequence generator was used in 54 studies (82%) and allocation of randomisation was concealed in 45 studies (68%) (online supplementary table 3). In 49 studies (74%), missing data were limited (<10%) or an appropriate imputation method was used. Eight studies (12%) incompletely reported QoL and PF, and an additional 21 studies (32%) only reported QoL or PF. Twenty-four studies (36%) had high adherence, and 13 studies (20%) had low contamination. Study characteristics and quality assessment of 1934 50–66 exercise arms not included in the meta-analyses are presented in the online supplementary table 4.
Supplementary file 3
Supplementary file 4
Characteristics of exercise arms included in the meta-analysis
As exercise arms are used as separate entities in the current meta-analysis, this paragraph will describe intervention characteristics for each study arm. Characteristics of the exercise arms included in the meta-analysis are presented in online supplementary table 3. Sample size ranged from 14 to 295. Patients were, on average, 55 years old and 68% was female. On average, recruitment rate and dropout rate were 52% and 13%, respectively, and did not differ significantly between studies investigating patients with different types of cancer. Twenty-nine3 12 31 32 36 37 41 43 46 48 67–80 exercise arms evaluated the effects of exercise interventions in patients with breast cancer, 1010 81–88 in patients with prostate cancer, 547 89–92 in patients with lung cancer, 1538 45 49 93–100 in patients with other types of cancer (bladder (n=1), colorectal (n=3), haematological (n=7), head and neck (n=1) and gynaecological (n=1)) and 154 35 39 40 42 101–108 in patients with various types of cancers. Thirty-three10 12 35 37 39 40 44 48 67 72 74 75 78–83 85–88 91 95 96 101 102 107 109 exercise arms investigated the effects of an exercise intervention during cancer treatment, 323 4 31 36 38 41–43 45–47 68–71 73 76 77 84 89 92 94 100 103–106 110 111 following treatment and 932 49 90 93 97–99 108 during and following cancer treatment. Intervention duration was ≤12 weeks in 42,4 31 37 38 41 44 45 47 68 69 71 72 74 77–81 83 85 86 89 91 92 94 96 98–102 104–110 >12–24 weeks in 243 10 12 35 36 39 40 42 49 67 70 75 82 84 88 90 93 95 97 103 and >24 weeks in 832 43 46 48 73 76 87 exercise arms. A supervised exercise intervention was investigated in 523 4 10 12 31 35 37 41 43–46 49 68 70–75 77–88 90–92 95–97 99 100 102 104–106 109–111 and an unsupervised exercise intervention in 2231 32 35 36 38–40 42 47 48 67 69 89 93 94 98 103 107 108 exercise arms. The frequency of supervised exercise sessions was <3 times per week in 294 35 37 41 43 45 46 72–76 78–84 87 95 100 102 104 106 109 110 and ≥3 times per week in 233 10 12 31 44 49 68 70 71 77 85 86 88 90–92 96 99 101 105 111 exercise arms. The frequency of unsupervised exercise sessions was <5 times per week in 931 32 38 42 48 93 94 108 and ≥5 times per week in 1135 36 39 40 67 89 97 98 103 107 exercise arms. Two47 69 studies investigating an unsupervised exercise intervention did not describe the frequency of exercise prescription. Prescribed exercise intensity was low in 172 study arm, low-to-moderate in 9,40 44 82 96 99 100 104 105 111 moderate in 34,10 31 32 35–38 43 47 48 67 70 77 83 86–88 91–93 98 102 103 108 109 moderate-to-high in 163 12 42 49 68 74–76 78 80 81 84 89 95 97 and high in 84 10 35 37 69 79 90 101 exercise arms. Five39 45 46 71 73 exercise arms did not report any information on exercise intensity. Twenty-six3 10 12 31 35 37 39–41 49 67–70 77–79 85 89 93 94 102–105 108 exercise arms investigated the effect of AE, 1210 12 37 46 73 74 80 86 88 99 100 109 investigated RE, 334 31 32 36 38 42 44 45 47 48 71 72 75 81–84 90–92 95–98 101 106 107 110 111 investigated a combined AE and RE programme and 343 76 87 investigated RE+impact exercises. Session duration was reported as ≤30 min in 29,3 10 12 31 35 36 38 40 42 49 67 70 77–79 89 93 94 97 98 103–105 108 110 111 30–60 min in 314 31 32 35 37 39 43–45 48 68 72 74–76 80–85 87 90 95 96 99 101 102 and >60 min in 341 46 106 exercise arms. Eleven47 69 71 73 86 88 91 92 100 107 109 studies did not report information on session duration. The mean volume of exercise per week was 121 min (SD=48) for supervised exercise and 132 min (SD=37) for unsupervised exercise, and the mean weekly energy expenditure was 637 MET-minutes/week (SD=313) for supervised exercise and 615 MET-minutes/week (SD=248) for unsupervised exercise.
Publication bias
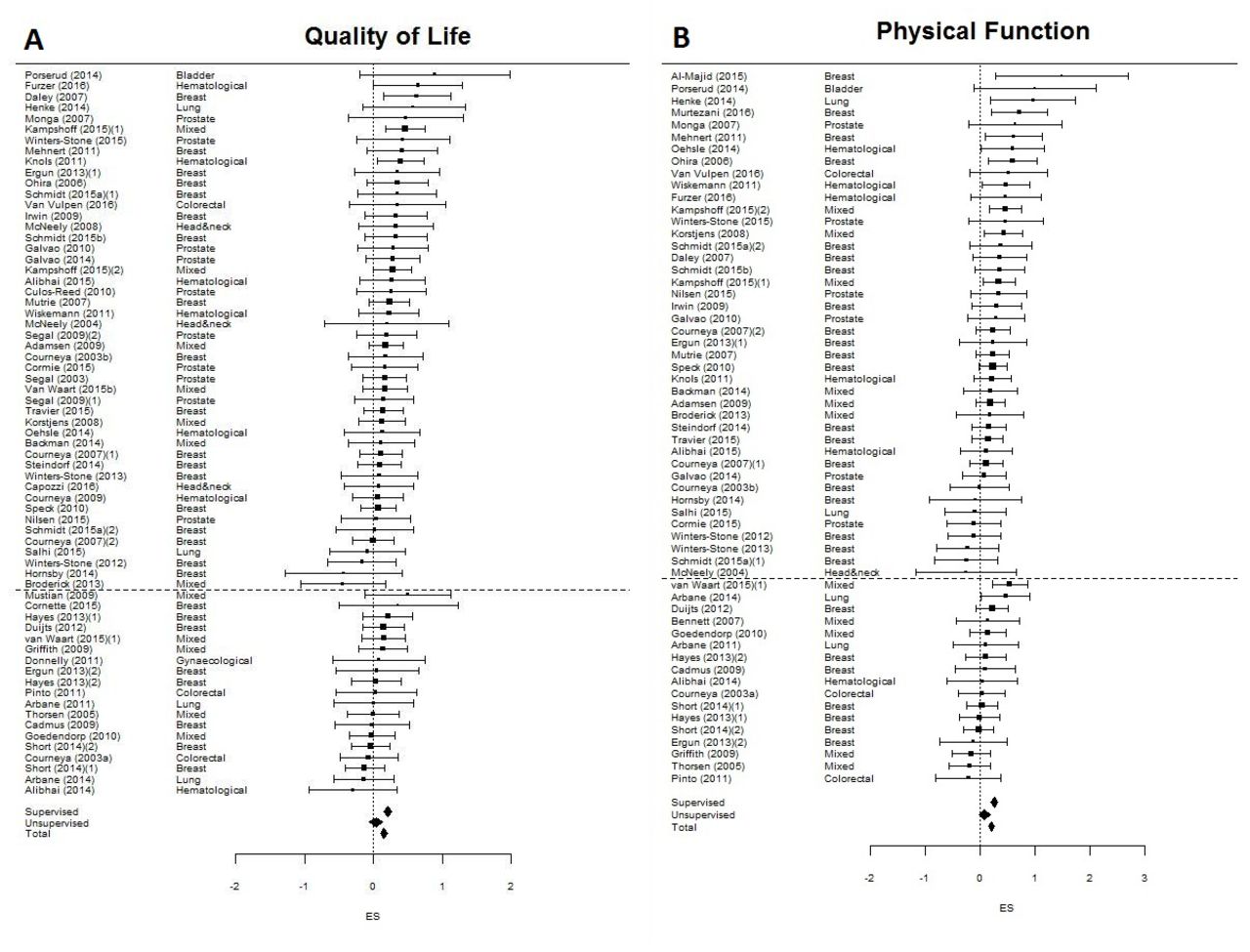
Data on QoL were available for 67 exercise arms after excluding four71 77 78 105 outliers of which the CI did not overlap with the pooled effect, and data on PF were available for 59 exercise arms after excluding five35 49 71 90 108 outliers. We found small, statistically significant beneficial effects on QoL (g=0.15, 95% CI (0.10 to 0.20), figure 2A) and PF (g=0.21, 95% CI (0.15 to 0.27), figure 2B).

Comparison of effect sizes on quality of life (A) and physical function (B) for studies investigating supervised (above dashed line) versus unsupervised (below dashed line) exercise: Hedges’ g and 95% CI.
For exercise arms evaluating QoL, the Duvall and Tweedie’s trim and fill procedure suggested six trials were missing, resulting in an effect size of g=0.13 (95% CI (0.08 to 0.18)) after adjusting for possible publication bias. Egger’s test was not statistically significant (p=0.22), suggesting no evidence of publication bias. Regarding PF, the Duvall and Tweedie’s trim and fill procedure suggested two trials were missing, resulting in an effect size of g=0.21 (95% CI (0.14 to 0.27)) after adjusting for possible publication bias. Egger’s test was not statistically significant (p=0.26), again suggesting no evidence of publication bias.
Effect of exercise on self-reported QoL and PF
Intervention effects on self-reported QoL and PF did not differ significantly between types of cancer, the timing of intervention delivery or intervention duration (table 1). The effects of supervised exercise on self-reported QoL (p<0.01) and PF (p=0.01) were significantly larger than the effects of unsupervised exercise. Supervised exercise significantly improved QoL (g=0.20, 95% CI (0.14 to 0.26)) and PF (g=0.27, 95% CI (0.20 to 0.33)), while the effect of unsupervised exercise was not statistically significant for self-reported QoL (g=0.04, 95% CI (−0.06 to 0.13)) nor PF (g=0.09, 95% CI (−0.01 to 0.19)).
Pooled effects of exercise on quality of life and physical function in patients with cancer during and post-treatment
Stratified analyses showed no statistically significant differences in effects on self-reported QoL and PF between interventions with various exercise FITT factors for both supervised and unsupervised exercise interventions. The effects on PF were larger for exercise interventions with a duration of ≤12 weeks than exercise interventions with a longer duration (p=0.08). However, no statistically significant between group difference for intervention duration was found when it was studied separately for supervised (p=0.49) and unsupervised exercise (p=0.71).
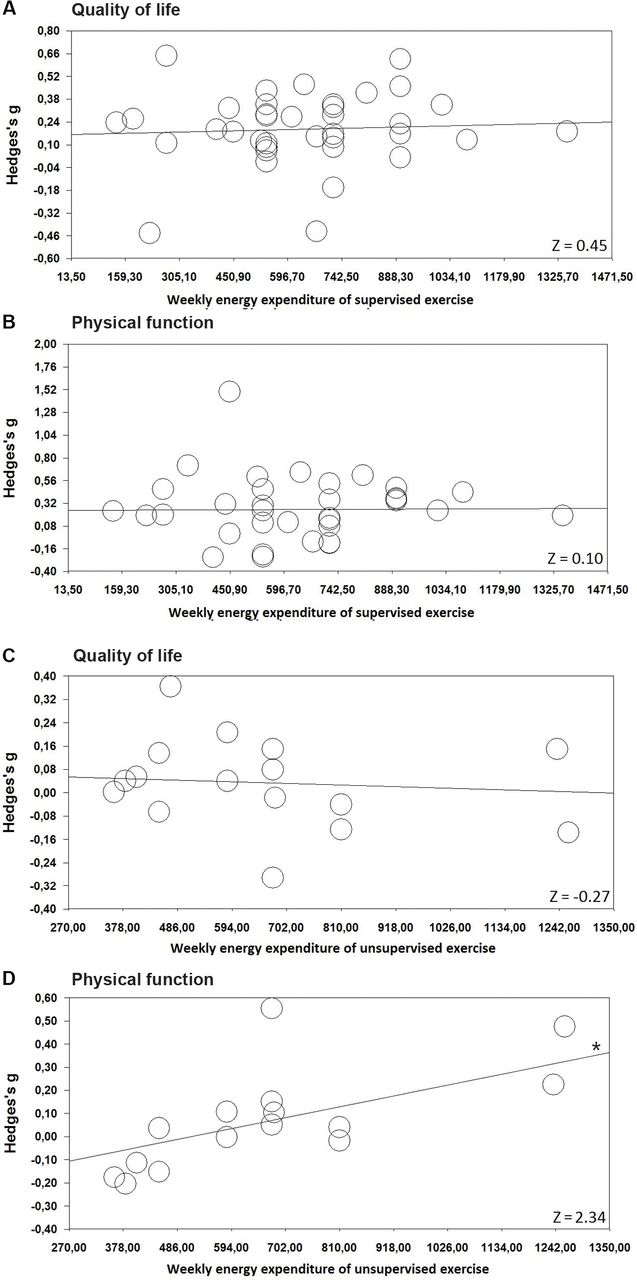
Meta-regression analysis showed that the effects of unsupervised exercise on PF was significantly larger for exercise interventions with a higher weekly energy expenditure (Z=2.34, p=0.02) (figure 3) but not weekly exercise volume. The effect of exercise on self-reported QoL did not differ by weekly exercise volume or energy expenditure.
{kind=link}
{kind=link}
{kind=link}
The association between weekly energy expenditure and the effect of exercise on self-reported quality of life and physical function. (A) Weekly energy expenditure and the effect of supervised exercise on quality of life. (B) Weekly energy expenditure and the effect of supervised exercise on physical function. (C) Weekly energy expenditure and the effect of unsupervised exercise on quality of life. (D) Weekly energy expenditure and the effect of unsupervised exercise on physical function. *statistical significant association between weekly energy expenditure and the effect of exercise.
Sensitivity analyses in a subgroup of studies that included patients with breast cancer only showed comparable effect sizes. However, the difference in effect on self-reported QoL between supervised and unsupervised exercise (p=0.13) as well as the association between weekly energy expenditure and the effects of unsupervised exercise on PF (Z=1.08, p=0.28) were not statistically significant.
Discussion
The current meta-analysis synthesised the data from 66 RCTs, including 74 exercise arms that evaluated the effects of exercise interventions during and following cancer treatment on self-reported QoL and PF. The large number of studies allowed us to study differences in effects across the timing, duration and mode of intervention delivery and exercise FITT factors.
Main finding
We found statistically significant and small clinical benefits of exercise interventions on self-reported QoL and PF. Supervised exercise interventions had statistically significant beneficial effects on QoL and PF, while unsupervised exercise interventions had no statistically significant beneficial effects on QoL and PF. We found no evidence for differences in effects between subgroups formed on the basis of intervention timing, duration or exercise FITT factors. However, within the category of unsupervised exercise interventions, there were larger effects on PF for interventions with a higher prescribed weekly energy expenditure.
The results from the current meta-analysis strengthen the findings from our previous IPD meta-analysis by including 32 additional RCTs, thereby increasing power to identify optimal intervention-related and exercise-related characteristics.14 The small effect sizes (QoL: 0.15, PF: 0.21) found in our meta-analysis are in line with those reported in our previous IPD meta-analysis and in a previous meta-analysis by Speck et al.2 However, Mishra et al reported moderate effect sizes in the meta-analyses of the effects of exercise during8 and following7 cancer treatment, which may be caused by our decision to exclude the outliers and the use of Hedges’ g to adjust for studies with small sample sizes. In addition, RCTs using objective measurement of PF such as gait speed, stair climb or chair-rise tests found larger effect sizes.53 81 83 84 Possibly, patients may not perceive large improvements in PF over time or self-reported PF may be susceptible to a response shift.112
No differences in effect of timing, duration or delivery mode of treatment
In line with a previous RCT49 and other (IPD) meta-analyses,2 7 8 14 we found no evidence for differences in effects on QoL or PF between studies that investigated exercise interventions during, following or both during and following cancer treatment. This finding suggests that exercise may contribute to preventing a decrease in self-reported QoL and PF during treatment as well as to improving QoL and PF following cancer treatment.113 Additionally, it was not possible to distinguish between the different types of treatment (eg, chemotherapy, radiation therapy, immune or hormone therapy) that may have influenced our results.
Mechanisms that underpin our main finding
Larger effects of supervised compared with unsupervised exercise interventions were also reported in our previous IPD meta-analysis14 and may be explained by a more demanding exercise prescription, a higher compliance to the prescribed exercise intervention, access to better equipment with more adjustment and performance feedback, the attention and support of the exercise physiologist delivering the intervention and possibly social interaction with other participants.114 One of the included RCTs found no statistically significant difference on QoL between an exercise placebo (including body conditioning/stretching exercises) and a usual care control group,68 indicating that attention was probably not, in itself, responsible for the beneficial effects of exercise on QoL. Previous RCTs comparing a supervised AE and RE programme with an unsupervised AE programme reported larger effects of supervised compared with unsupervised exercise on QoL following treatment31 and PF during treatment.35 However, this difference could also be due to differences in exercise types. To identify the effects of the supervision, we recommend a head-to-head comparison of supervised and unsupervised exercise with identical exercise-related characteristics in patients with cancer. In addition, objective methods for assessing exercise intensity and duration (eg, accelerometry and heart rate monitoring) could assess the compliance to the prescribed exercise intervention. This could help to compare the exercise undertaken by patients when following a supervised or unsupervised exercise programme and to investigate the effects of the supervision.
Differences in effects of exercise characteristics
We found no evidence for a difference in effect between different exercise types, and both supervised AE and RE resulted in a statistically significant increase in self-reported QoL and PF. This finding is in contrast to the findings of a previous RCT, reporting larger effects of RE compared with usual care than AE on QoL in patients with prostate cancer receiving radiation therapy,10 but in line with results from previous studies comparing AE with RE12 and AE with AE+RE9 in patients with breast cancer receiving chemotherapy. However, the effects of different exercise types on other outcomes such as aerobic fitness, percentage body fat, muscle strength and lean body mass may differ, as has been reported by Courneya et al in patients with breast cancer.12
For unsupervised exercise interventions, we found evidence for larger intervention effects on PF when weekly energy expenditure prescriptions were higher, while there was no evidence for an effect of high-intensity exercise or a high weekly exercise volume alone. This finding suggests that, in the case of unsupervised exercise, patients should be encouraged to increase their weekly energy expenditure when aiming to improve PF. However, the optimal combination of weekly exercise volume and exercise intensity for unsupervised interventions is still unclear. For supervised exercise, no dose–response relationship was found between weekly energy expenditure and the effect on self-reported QoL or PF. A previous RCT reported a higher dose of supervised AE to be related to larger effects on PF,9 while a higher frequency (3 vs 2 days/week) of RE was related to higher effects on the physical component summary (including PF).115 In the current meta-analysis, the dose–response relationship between weekly energy expenditure and the effect of exercise on self-reported QoL and PF was investigated for AE and RE combined. Future research should clarify whether this relationship differs by exercise type.
Exercise seems equally effective in improving self-reported QoL and PF across patients with different cancer types, which extends the conclusion of our previous IPD meta-analysis.14 Sensitivity analyses in patients with breast cancer showed comparable effect sizes. However, most likely due to larger confidence levels, the difference in effect between supervised and unsupervised exercise interventions on QoL, was not statistically significant. Comparably, the dose–response relationship of weekly energy expenditure and the effect on PF were not statistically significant in patients with breast cancer.
It is important to note that some RCTs reported low recruitment rates without describing demographic or clinical differences between participants and non-participants to inform generalisability of the results. Previous RCTs investigating the effects of an exercise intervention during or following cancer treatment in patients with cancer on physical fitness, fatigue and QoL reported that non-participants are more likely to have a low educational level, are less likely to be working, have longer travel time, live alone, have more comorbidities than participants and are often aged ≥70 years.35 116 Additionally, sex and diagnosis did not differ between participants and non-participants in patients with different diagnosis.4 As most previous studies did not report the reasons for dropout, we were unable to provide information on the characteristics of participants who dropped out of the exercise trials. From a previous systematic review investigating the determinants of exercise adherence, it is known that exercise history is a main determinant of adherence, but the results for baseline cardiorespiratory fitness and physical activity were unclear.117 Studies investigating exercise interventions in patients with a poor prognosis (such as pancreatic or lung cancer) are scarce, and some caution is warranted with generalising the results to all cancer populations. Future research should focus on the effects of exercise in patients with understudied cancer types.
The lack of statistically significant differences in exercise intervention effects as a function of exercise timing, duration or exercise FITT factors may be the result of comparing the effects of different combinations of exercise-related characteristics. For example, the exercise effect as a function of intervention duration may be influenced by the difference between supervised exercise interventions, which predominantly have an intervention duration of less than 12 weeks and unsupervised exercise interventions with a longer intervention duration. To further disentangle the effects of different intervention and exercise-related factors, it is necessary to conduct second-generation studies that directly compare different intervention and exercise-related characteristics, focusing on one aspect while keeping others similar.9 49 115 118
Quality assessment
Most studies showed high quality regarding random sequence generation and allocation concealment. A large number of studies had limited missing data or used an appropriate imputation technique. However, more than 40% of exercise arms were rated with high risk of adherence bias. Possibly, this bias could explain the small effect sizes found in the current meta-analysis. Adherence to unsupervised exercise is difficult to monitor, and small effects of unsupervised exercise could be a result of low adherence to the prescribed exercise programme. More than 75% of included exercise arms did not report any information on contamination, while high contamination could result in small pooled effect sizes. Overall, the quality of studies included in the current meta-analysis was higher than studies not included; this finding holds for all of the quality items assessed.
Strengths and limitations
Strengths of the current meta-analysis are the extensive search in multiple databases, the inclusion of RCTs and the large number of exercise arms, allowing subgroup analyses based on intervention and exercise-related characteristics. There are, however, several limitations. First, subgroups were based on exercise prescription that depended on whether the researchers have specifically appointed the intensity (ie, % maximum heart rate or maximum rate of oxygen consumption) and whether they have measured and reported the intensity correctly. In addition, a large number of studies did not report information on exercise adherence. Accordingly, subgroups could be categorised differently if they were based on the exercise actually performed by the patients. Second, in eight studies, two exercise arms were included, which we both compared with the same control group as if they were independent. This decision may have reduced the heterogeneity in effects and could result in a small bias in the pooled effect size.119
Conclusion
In conclusion, the results of our meta-analysis indicate that exercise interventions can improve self-reported QoL and PF compared with usual care. We found a statistically significant difference in effect between supervised exercise and unsupervised exercise. Supervised exercise interventions had statistically significant beneficial effects on QoL and PF, while unsupervised exercise interventions had no statistically significant effect on QoL and PF. For unsupervised exercise, weekly energy expenditure was a determinant of success.
Future studies should identify the most optimal combination of weekly exercise volume and intensity. Exercise intervention effects were comparable across subgroups based on timing and duration of intervention delivery and exercise FITT factors. Nevertheless, only adequately powered, high-quality RCTs can determine the causal effects of manipulating each exercise factor on outcomes in patients with cancer.
What is already known?
Previous randomised controlled trials (RCTs) and meta-analyses have demonstrated beneficial effects of exercise during and following cancer treatment on self-reported quality of life and self-reported physical function.
What are the findings?
We found a significant between-group difference for exercise delivery mode, with significant beneficial effects for supervised exercise interventions on quality of life and physical function, but not for unsupervised interventions.
No significant differences in intervention effects were found for variations in intervention timing and duration, or exercise frequency, intensity, type or time.
Unsupervised exercise intervention effects on self-reported physical function were larger when prescribed at a higher weekly energy expenditure.
References
Footnotes
Contributors MGS, TMA, MJC, LMB and JB contributed to the concept and design of the study. MGS, TMA, LMB and JK gathered and analysed the data. This study was performed alongside the POLARIS study. LMB, JB and IMVdL are members of the steering committee of POLARIS. KSC, RUN, PBJ and NKA are members of the international advisory board of POLARIS. All authors have revised the manuscript and approved the final version.
Funding Via ‘Bas Mulder Award’ granted to LMB by the Alpe d’HuZes Foundation/Dutch Cancer Society (VU 2011-5045).
Competing interests None declared.
Ethics approval Ethics committee from local institutes where randomised controlled trials were conducted, which are included in this review/meta-analysis.
Provenance and peer review Not commissioned; externally peer reviewed.
Correction notice This article has been corrected since it was published Online First. Figure 2B has been corrected.