Article Text

Abstract
Objectives To summarise evidence of benefits of sport for health among people aged 60+.
Design Systematic review with meta-analysis of randomised controlled trials (RCTs).
Data sources Medline, CINAHL, SPORTDiscus, the Physiotherapy Evidence Database from inception to April 2021.
Study selection RCTs investigating the effect of sport on health-related outcomes in people aged 60+ compared with non-active control.
Data synthesis and analysis Pooled effect sizes were calculated using random-effect models. Standardised mean differences (SMD), and mean difference (MD) were calculated. The Grading of Recommendations Assessment, Development and Evaluation system was used to assess the certainty of the evidence for analyses with ≥3 studies.
Results Nine trials (628 participants) reported in 15 articles were included. Participation in sport improved cardiorespiratory fitness (n=5 trials; SMD=0.43, 95% CI 0.17 to 0.70; low certainty evidence), physical function (n=4; SMD=0.62, 95% CI 0.05 to 1.18; very low certainty evidence), and mental health (n=2; SMD=0.28, 95% CI 0.06 to 0.51) and reduced fat mass (n=6; MD=−0.99 kg, 95% CI −1.75kg to −0.23 kg; low certainty evidence) among older people. We found no significant effects of sport on overall physical activity participation, strength, balance, lean mass and bone mineral density (BMD). One study investigating quality of life reported a positive, but non-significant effect of sport.
Conclusion Sport may have a positive impact on health outcomes in people aged 60+. There was uncertainty on the effect of sport on strength, balance, lean mass and BMD. Further research is needed to investigate the optimal type and dose of sport to maximise the long-term benefits among older people.
- sport
- health
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The demographic profile of the global population is ageing rapidly. People aged 60 years and older are forecast to total 2 billion by 2050, outnumbering adolescents and young people for the first time in history.1 2 As this demographic transition will affect almost all aspects of society, the WHO has recently launched the Decade of Healthy Ageing 2021–2030 to foster long and healthy lives among older people.3 Ageing is strongly associated with the onset of non-communicable diseases (NCDs),4 5 and preventive strategies that address the main risk factors for NCDs, such as physical inactivity, are crucial.
Being physically active throughout life is key to maintaining health, optimising physical function, independent living and enhancing satisfaction with life and the ageing process.6–10 To achieve the health benefits of physical activity, including functional capacity and preventing falls, the WHO 2020 Guidelines on Physical Activity and Sedentary Behaviour recommend that older adults undertake 150–300 min of moderate intensity, or 75–150 min of vigorous-intensity physical activity per week.11 The WHO11 and other international exercise consensus statements10 12 support the prescription of structured exercises for older people, including resistance and aerobic training activities, as well as multicomponent physical activity that emphasises functional balance and strength training, on at least 2 days of the week. The WHO recommendations endorse that some physical activity is better than none, but more physical activity is better for maximising health outcomes.11 Although it is still unclear what type or domain of physical activity impacts specific health outcomes, it is known that physical activity accumulated at leisure, work, home and during transportation counts towards the WHO recommended amounts.11
Sport is a type of leisure-time physical activity2 and it could be an appealing and enjoyable option for older people to be physically active. Many people aged 60+ participate in sport. For example, the AusPlay survey of over 117 000 Australian adults revealed that around 40% of people aged 65+ years participate in organised sport.13 Different sport versions can cater for older people at different physical function levels, and modified versions of sport now exist to accommodate the skills and abilities of older people, including people with lower physical function, such as walking football and walking basketball.
The four domains of physical activity are work, active transport, household and leisure. Sport is a type of leisure-time physical activity, and it is worth being investigated as an option of intervention to promote physical activity. Although the health benefits of other forms of leisure-time physical activity, such as walking, have been extensively studied, sport participation has not been widely explored as a physical activity opportunity for older adults.14 15 Our previous scoping review15 of physical activity interventions for older adults identified a lack of reviews investigating the impact of sports in older people. To fill this knowledge gap, we aim to summarise the evidence on the effect of sports-based interventions on health outcomes among people aged 60 years and older. This systematic review is a component of work on the best available evidence for the effectiveness of physical activity programmes and services for older adults commissioned by the WHO. This commissioned work aimed to inform the development of an upcoming toolkit to assist countries to adopt, tailor and implement physical activity recommendations for older adults.
Methods
Search strategy
Our systematic review with meta-analysis followed the methods described in the Cochrane Handbook for Systematic Reviews of Interventions and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.16 17 We performed this review in accordance with the methods documented in the protocol registered with the PROSPERO database prior to commencement (#CRD42021250901).
We conducted a systematic search of four electronic databases, including Medline (Ovid), Cumulative Index to Nursing and Allied Health Literature (CINAHL) (EBSCO), SPORTDiscus (EBSCO), the Physiotherapy Evidence Database (PEDro) for relevant English-language literature published from inception to April 2021. We used a combination of Medical Subject Heading terms and text words related to ‘sport’, ‘older people’, ‘randomised’ and ‘controlled trial’ to create our search strategy (see online supplemental appendix 1). In addition, included studies and reference lists of relevant reviews were hand searched.
Supplemental material
Selection criteria
Study type
We included randomised controlled trials (RCTs) (see box 1).
Inclusion criteria
Design: Randomised controlled trials
Participants: Adults aged 60 years and over
Intervention: Any type of sport
Control: Non-active control intervention, no intervention, usual care
Outcomes measured related to: Physical activity, social functioning (participation), physical functioning, cognitive and emotional functioning, well-being and quality of life
Setting: Sport conducted in the community or clinical settings
Population
Trials involving adults aged 60+ years were eligible for inclusion. We also included trials where participants had an average or median age of at least 60 years. We included studies where participants were from the general population and studies where participants were recruited on the basis of having clinical conditions.
Intervention
We included any trial that examined the effects of any type of sport in older people. Sport was defined as ‘an activity involving physical exertion, skill and/or hand-eye coordination as the primary focus of the activity, with elements of competition where rules and patterns of behaviour governing the activity exist formally through organisations’.18 We excluded studies involving combined interventions (eg, supplement/nutrition and sports) unless the difference between groups was sport (eg, sport and nutrition vs nutrition). We also excluded video game-based sport interventions, rehabilitation and passive interventions.
We restricted our review to sport conducted in the community or clinical settings. We included trials that involved sport-based activities arranged through recreation clubs, sporting or non-sporting associations, gymnasiums or a wide variety of other sporting and non-sporting arrangements such as social clubs, church groups, retirement villages and seniors’ associations. We excluded studies where the sport was conducted in participants’ homes, residential care facilities, research laboratories or other non-community settings. Clinical settings were only included where there was a specific sports programme completed rather than routine rehabilitation programmes.
Comparator
To be eligible, trials had to compare one group that participated in sport with a non-active comparison group, such as usual care, waitlist or control group. We did not include trials that compared sport with another physical activity intervention.
Outcome measures
We previously developed a framework15 to classify physical activity intervention studies for older adults in terms of study sample, intervention characteristics, comparison group and outcomes investigated. We used this framework to guide inclusion of relevant health-related outcomes. As per our framework, outcome domains included physical activity, social functioning (participation), physical functioning, cognitive and emotional functioning, well-being and quality of life. We excluded any blood, metabolic or cardiovascular biomarkers (eg, inflammatory markers, neurotrophic biomarkers) and measures that are not routinely collected in clinical practice (eg, laboratory measures of cognitive function such as brain volume).
If we identified multiple publications from the same trial, we only included manuscripts that reported different outcomes. We excluded publications that included the same participants and reported the same outcomes as a previously included publication.
Study selection, data collection and extraction
Each title and abstract were independently screened by two out of three reviewers (SG, LM or LBM), and full texts of eligible studies were retrieved. Two out of three reviewers also assessed each retrieved full-text paper independently using the eligibility criteria. A third reviewer (JSO) resolved any conflicts. Titles, abstract and full-text studies were screened using Covidence systematic review software.19 Data extraction was conducted by one reviewer (SG or LBM), and all data were checked for consistency by a second reviewer (LBM) using standardised data extraction forms. We extracted the following data from each included trial: author, published year, country, sample characteristics (sample size, age and sex of participants, health status and recruitment setting), intervention description (type of sport, frequency, session duration, length of intervention, who delivered the intervention, where the intervention was delivered), comparison intervention, measured outcomes, follow-up and quantitative data for the meta-analysis.
Methodological quality assessment and quality of the evidence
We used the PEDro scale scores to assess the internal validity and methodological quality of the included RCTs.20 21 We downloaded PEDro scores from the PEDro database (https://www.pedro.org.au/). The PEDro scale consists of 11 items: inclusion criteria and source, random allocation, concealed allocation, similarity at baseline, subject blinding, therapist blinding, assessor blinding, completeness of follow-up, intention-to-treat analysis, between-group statistical comparisons, and point measures and variability. Scores on the PEDro scale range from 0 (very low methodological quality) to 10 (high methodological quality) although the highest possible score for a trial of a sport intervention is 8/10 as blinding of participants and deliverers is not possible. A score≥6/10 on the PEDro scale was considered moderate to high quality. Methodological quality was not an inclusion criterion for this review.
To assess the overall certainty of the evidence for outcomes with results from≥3 studies, we used the Grading of Recommendations Assessment, Development and Evaluation system.22 We assigned a general rating of the certainty of the body of evidence as ‘high’, ‘moderate’, ‘low’, or ‘very low’ based on the presence or extent of four factors: design limitation, inconsistency, imprecision and publication bias. We downgraded from high quality by one level for the presence of each factor, as follows: (1) study limitation (>25% of participants from studies with low methodological quality: PEDro score<6), (2) inconsistency of results (large heterogeneity between trials: I2>60%), (3) imprecision (<400 participants across all studies) and (4) publication bias (serious small study effects suggested by the funnel plot). As the population, intervention, or outcomes did not differ from those in which we are interested, we do not have concerns about the indirectness criterion and did not downgrade for this criterion.
Data analysis
We used the random-effect model to pool estimates for each analysis obtained using Comprehensive Meta-analysis, V.2.2.064 (Biostat, Englewood, New Jersey, USA). We calculated standardised mean difference (SMD) (Hedges’ g) and 95% CI when the studies measured the same outcome but assessed it using different scales or tools. We standardised the SMD by postscore SD (or its estimate) and calculated it using the pre-mean and post-mean and SD or, when this was unavailable, the mean change score. If multiple follow-up data points were provided, the scores obtained as close to the completion of the intervention as possible were used for the analysis. Effect sizes were categorised as small (0.1 to 0.4), medium (0.5 to 0.7) or larger (0.8 or greater).23 For the outcomes measured on the same scale, we calculated the mean difference (MD) (difference in means) and 95% CI to facilitate interpretation.
Statistical heterogeneity was determined by visual inspection of the forest plots and with consideration of the I2 test. We considered substantial heterogeneity if I2>60%. We also investigated small study effects by using a funnel plot of the effect estimates from included studies. The funnel plot was assessed by visual inspection and by using Egger’s test, with p<0.1 as evidence of publication bias.24
Differences between protocol and review
Minor changes in the planned review protocol occurred. As we had anticipated few trials on sport in older people would be available, we did not initially place any restrictions on the comparator in the protocol. However, we decided to focus this review on investigating the impact of sport on health outcomes, so we limited the comparator to non-active control.
Results
The flow of trials through the review
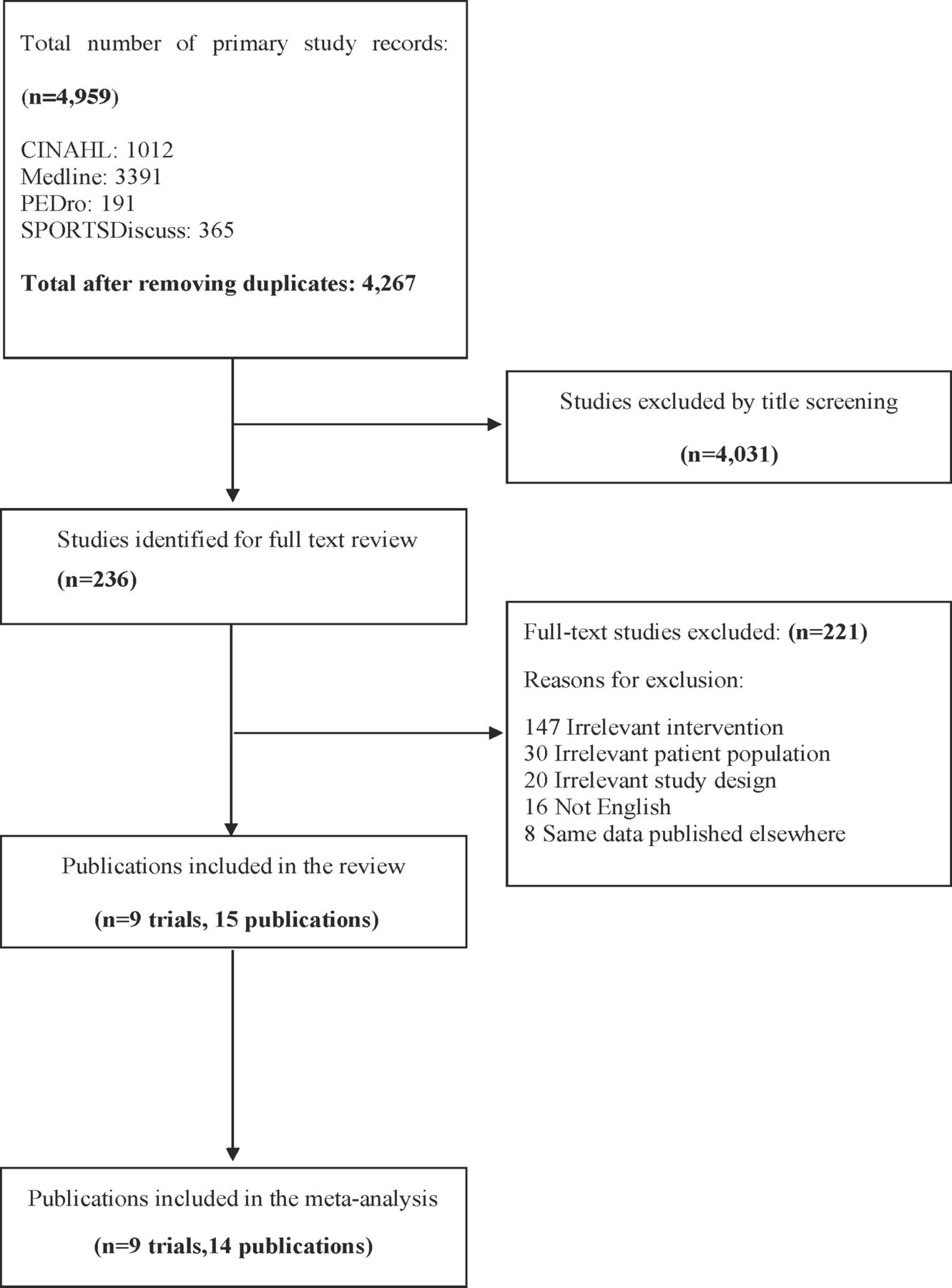
After duplicates were removed, the electronic search retrieved 4267 references, and no additional studies were found by hand search. After abstract and title screening of all references and full-text screening of 236 published papers, 15 publications25–39 reporting results of 9 RCTs met our inclusion criteria. We documented the screening process in a PRISMA study flow diagram (figure 1).
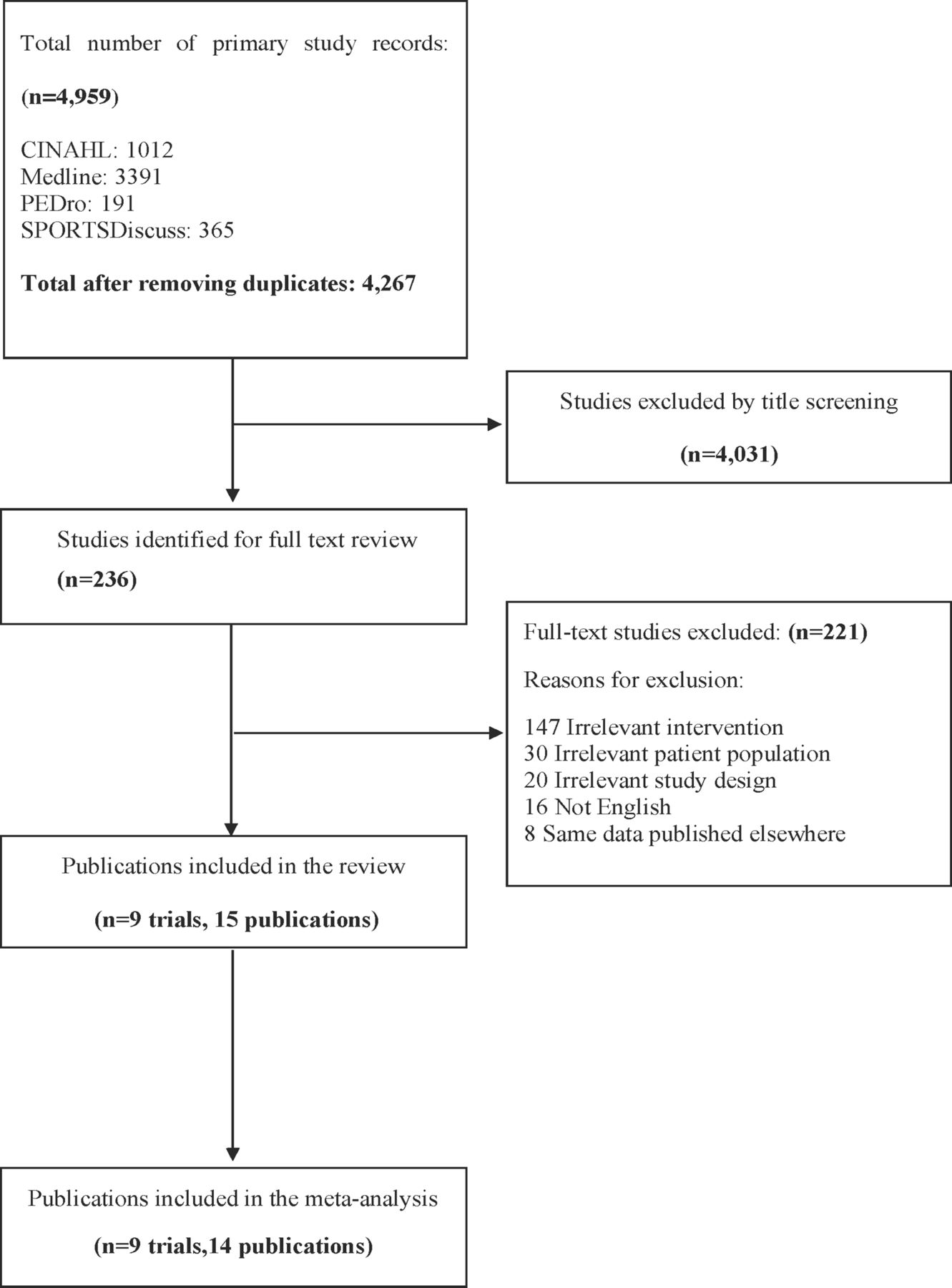
Flow of studies through the review.
Characteristics of included trials
Publication dates ranged from 2014 to 2020 (median, 2017), with 60% of trials published after 2017. Most trials were conducted in high-income countries (8/9, 89% trials): Denmark (n=5/9 trials, 9 publications),25–27 29–31 36 37 39 Japan (n=1/9, 1 publication),32 Portugal (n=1/9, 1 publication),31 Faroe Islands (n=1/9 trials, 2 publications).33 34 One trial (2 publications)28 38 was conducted in an upper middle income country (ie, Brazil), and none of the studies were from low-/middle-income countries (LMIC).
We synthesised the details of the population, intervention, measured outcomes and follow-up in online supplemental table 1. For a single trial,30 details of the intervention were summarised in online supplemental table 1, but the data were not included in any meta-analysis as this study only reported pooled sport intervention and resistance training results.
Supplemental material
Quality
The online supplemental table 2 summarises the methodological quality of eligible studies. The total PEDro score ranged from 4 to 8, with a mean of 5. Four publications were of moderate-to-high methodological quality (PEDro score≥6), and 11 publications were of low methodological quality (PEDro score<6). All participants were randomly allocated, and all studies provided between-group comparisons and the calculation of point estimates and variability. Intention-to-treat analysis was infrequently undertaken (4 studies; 33%). None of the trials included blinded participants or blinded therapists, as expected in sports interventions.
Supplemental material
Participants
The nine trials involved a total sample of 628 participants ranging from 26 to 214 (median, 67 participants). All studies included older people with a mean age between 60 and 80 years (mean, 67 years). Three trials (seven publications)25–27 29 35–37 included men only, a single trial included women only (one publication),31 and all the other trials (five studies, seven publications)28 30 32–34 38 39 involved mixed-sex populations. Most studies selected participants based on participants’ low physical activity level (7 studies, 12 publications),25 26 28–35 39 and none selected participants based on physical or cognitive impairment.
Participants were recruited from varied settings, including community, outpatient clinics, senior centres and a population register. The target population recruited in the trials was mainly the general population (four studies, seven publications).25 26 29 30 32 35 39 Three studies recruited participants with a specific clinical condition: two trials (three publications) recruited people with prostate cancer,27 36 37 and one trial (two publications) included people with type 2 diabetes.28 33 34 38 One trial (two publications) included participants with pre-diabetes30 31 and one trial (one publication) included post-menopause women.31
Intervention
The most commonly investigated sport type was soccer (5 trials, 11 publications),25–29 33–38 followed by floorball, a type of floor hockey played indoors (two trials, two publications),30 39 golf (one trial, one publication),32 and handball (one trial, one publication).31 The length of sport intervention in the included trials ranged from 12 weeks to 52 weeks, and the mean duration was 16 weeks. Intervention frequency ranged from one to three times per week, with each session ranging from 16 to 120 min. In trial reports that specified who delivered the intervention, sport sessions were delivered by local and professional coaches, research staff, and experienced instructors were involved in the intervention delivery. The intervention took place in the community, university and local clubs, but most trials did not specify the delivery location.
Comparator
The comparators of the included studies were the control group (ie, no active group, general health education, nutritional interventions) in 7 trials (12 publications),25 26 28–35 38 39 and usual care in 2 trials investigating clinical populations (3 publications).27 36 37
Outcome measures
The most commonly investigated outcome was body composition (ie, lean body mass and fat mass) using dual-energy X-ray absorptiometry (DXA) (n=6 trials), followed by cardiorespiratory fitness measured by expired gas analysis (n=5), bone mineral density (BMD) measured by DXA (n=4), muscle strength using various measures, including isokinetic and hand-held dynamometer (n=4), physical function measured using sit-stand test or by the physical domain of the 12-Item Short Form Health Survey (SF-12) (n=4), physical activity measured by the International Physical Activity Questionnaire (n=2), balance assessed using force platform (n=2), mental health measured by Geriatric Depression Scale and mental health domain of SF-12 (n=2), and quality of life using the Functional Assessment of Cancer Therapy—Prostate (n=1).
Adverse events
Adverse events (AEs) were reported to some degree in all trials (online supplemental table 3). Six trials reported 90 AEs and three studies reported no AEs.28 32 34 Seventy-two out of 90 AEs were sports-related injuries, and the average incidence was 249 injuries per 1000 hours of exposure. The reported sport injuries included partial or total achilles’ tendon rupture (reported in three trials), muscle sprain or strain (two trials), fibula subluxation (one trial) or fibula fracture (one trial), shoulder and knee injury (one trial). A single study27 reported a serious adverse event (SAE) in both intervention and control groups (ie, hospital admissions), but only one was related to the intervention that occurred due to a scratch sustained from a shin guard that scratched the lower leg. This injury later became infected resulting in a skin transplant. Only one study reported falls in the control (6 falls) and intervention (10 falls) group, but this difference was not significant (p=0.44).27
Supplemental material
Meta-analysis
Meta-analyses for the included outcomes are presented in figures 2–5 and the certainty of the evidence summary is reported in online supplemental table 3. Social functioning (participation) was also not assessed by the trials.

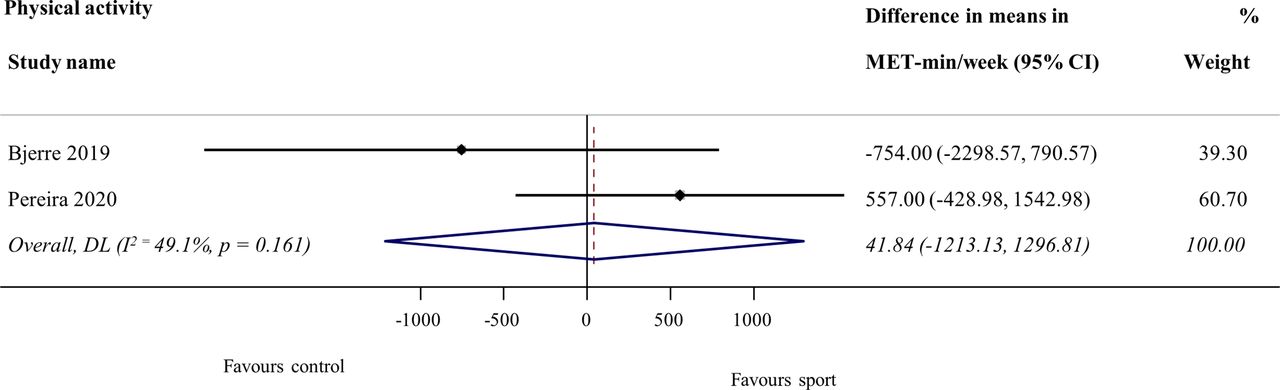
Difference in means (95% CI) of sport versus control on physical activity using random-effects meta-analysis.
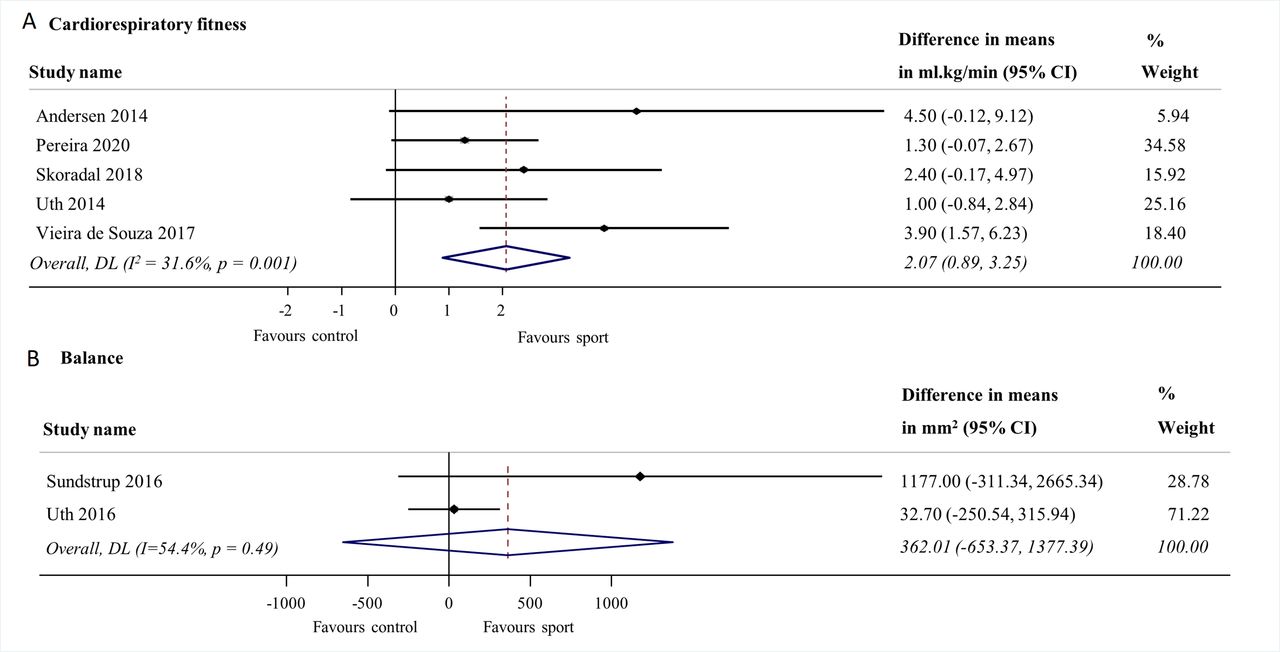
Difference in means (95% CI) of sport versus control on cardiorespiratory fitness and balance using random-effects meta-analysis.

Standardised mean difference (Hedges’ g) (95% CI) of sport versus control on strength and physical function using random-effect meta-analysis.
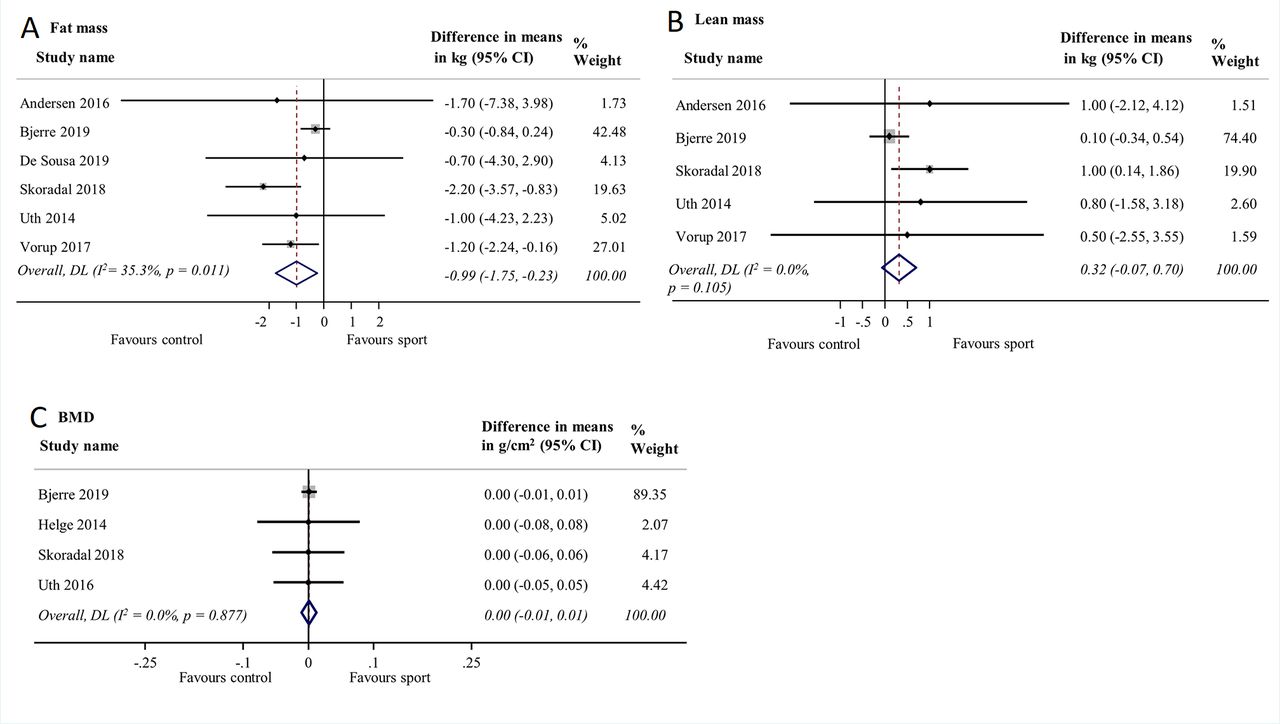
Difference in means (95% CI) of sport versus control body composition and bone mineral density (BMD) using random-effect meta-analysis.
Effect of sport on physical activity
We pooled two trials in the meta-analysis evaluating the effect of soccer and handball on overall physical activity levels (total pooled sample=244 participants). The pooled effect of sport on physical activity showed no effect compared with the control group (MD=41.84 MET-min/week, 95% CI −1213.13 MET-min/week to 1296.81 MET-min/week; I2=49%; figure 2). We were unable to assess the certainty of evidence, as the meta-analysis results included<3 studies.
Effect of sport on physical functioning: cardiorespiratory fitness, balance, strength, physical function, body composition (fat mass and lean muscle mass) and BMD
Cardiorespiratory fitness
The meta-analysis showed a small significant effect of soccer and handball on cardiorespiratory fitness compared with control participants (5 studies, 224 participants; MD=2.07 mL.kg/min, 95% CI 0.89 mL.kg/min to 3.25 mL.kg/min; I2=32%; low certainty evidence; figure 3).
Balance
We found no significant impact of soccer on balance, assessed with force platform, compared with control (2 studies, 64 participants; MD=362.01 mm2, 95% CI −653.37 mm2 to 1377.39 mm2; I2=54%, figure 3). The overall quality of evidence for the effect of sport on balance was not assessed, as the meta-analysis results included<3 trials.
Strength
The meta-analysis showed no significant effect of soccer, golf and floorball in improving strength compared with control (4 studies, 312 participants; SMD=0.05, 95% CI −0.23 to 0.33; I2=3%; low certainty evidence; figure 4).
Physical function
The pooled effect of soccer and floorball showed a medium significant effect on physical function in participants who undertook sport versus control participants (4 studies, 314 participants, SMD=0.62, 95% CI 0.05 to 1.18; I2=74%; very low certainty of evidence; figure 4).
Body composition
We detected a significant effect of soccer and floorball in reducing fat mass (6 studies, 361 participants; MD=−0.99, 95% CI −1.75 to −0.23; I2=35%; low certainty of evidence; figure 3) but not in improving lean mass (5 studies, 359 participants; MD=0.32 kg, 95% CI −0.07 kg to 0.70 kg; I2=0%; low certainty of evidence; figure 5) compared with control.
Bone mineral density
The meta-analysis showed no significant difference in the effect of soccer compared with control on BMD (4 studies, 317 participants; MD=0.00 g/cm2, 95% CI −0.01 g/cm2 to 0.01 g/cm2; I2=0%; very low certainty of evidence; figure 5).
Effect of sport on cognitive and emotional functioning: mental health
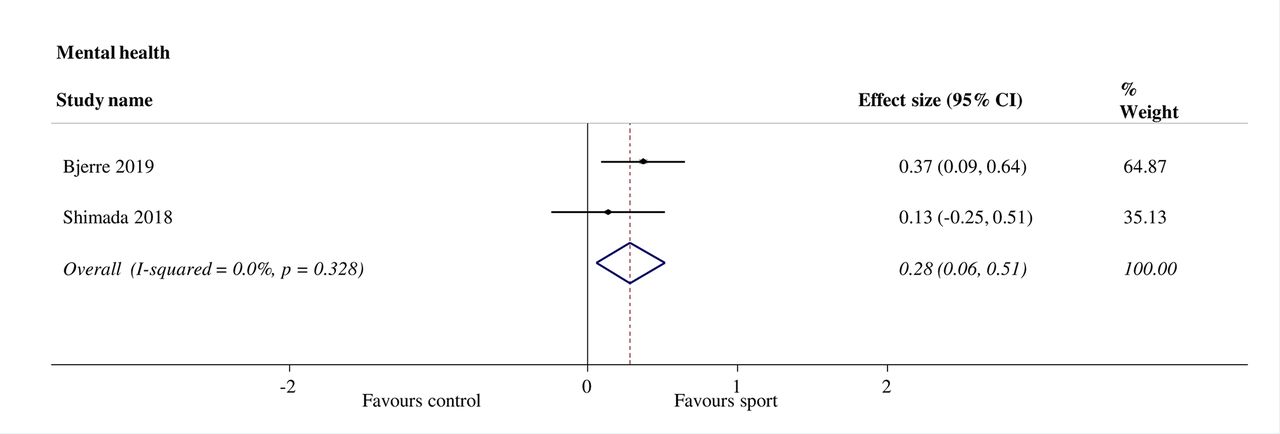
The pooled effect of sport indicates a small significant effect on mental health in participants allocated to soccer or golf versus control participants (2 studies, 306 participants, SMD=0.28; 95% CI 0.06 to 0.51; I2=0%; figure 6). We were unable to assess the overall certainty of the evidence for mental health, as its results are from <3 studies.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Standardised mean difference (Hedges’ g) (95% CI) of sport versus control on mental health using random-effect meta-analysis.
Effect of sport on well-being and quality of life
Only one trial reported the effects of sport on quality of life outcomes.27 Overall, participants allocated to soccer intervention presented no significant differential effect in quality of life compared with control (1 study, 200 participants; MD +0.5 points, 95% CI −2.8 to 3.8; p=0.76).
Publication bias
Funnel plot symmetry was displayed and revealed no significant publication bias for all included outcomes, except BMD (see online supplemental figures 1 and 2).
Supplemental material
Supplemental material
Discussion
Principal findings
This systematic review with meta-analysis demonstrated that sport may improve cardiorespiratory fitness, physical function and mental health, and reduce fat mass among older people. We are uncertain whether sport improves physical activity, strength, balance, lean mass, BMD and quality of life. No studies investigated social functioning as an outcome. Three trials reported no AEs, but most trials reported AEs and sport injuries (67% trials), and the average incidence was 249 injuries per 1000 hours of exposure, which is high but expected for older population. However, the majority of the injuries were minor AEs and only one was SAE.
Interpretation of the findings
Our findings showed that sport participation was associated with significant cardiorespiratory fitness and physical function improvements. Similarly, a previous review40 on small-sided soccer games indicated improvements in cardiorespiratory fitness and aerobic capacities assessed through maximum oxygen consumption (Vo2max) in healthy individuals and clinical populations regardless of age. This review also demonstrated positive effects on physical function across the lifespan.40 Our findings are also consistent with other related scoping reviews in untrained participants and clinical populations.41–43 The significant effects on cardiorespiratory fitness and physical function may reflect the physical requirements of the type of sports included in this review, which involved vigorous-intensity activities (ie, soccer 7 METs; handball: 12 METs and floorball (hockey): 8 METs).44 These types of sport usually involve high-intensity movements in various directions and accelerations, imposing considerable demands on the cardiovascular system and requiring certain levels of mobility.
Our findings also showed a small significant effect of sport on mental health. However, another recent review without meta-analysis on the psychological impacts of sport in older people found inconsistent results for the relationship between depression, anxiety and stress and sport participation.45 As only two studies27 32 reported mental health as an outcome, caution is recommended in interpreting our findings. Studies further exploring the impact of sport on mental health are needed.
The general positive effects of sport on fat mass are also in keeping with other related systematic reviews.40 42 43 The positive changes in body composition might be associated with increases in intensive energy expenditure during sport sessions. Another potential explanation is that the increase in energy expenditure also potentially increased lipid metabolism during training and post-training.25
In contrast to other reviews,40–43 our study did not show a significant effect of sport on strength, balance, lean mass, BMD and quality of life. Improvements in these outcomes may be related to the type of training or dose of the intervention, but we were unable to draw firm conclusions due to the limited evidence and number of studies investigating these outcomes. Given the lack of impact on these outcomes, further studies should investigate the combination of sport and other types of training (ie, resistance, functional and/or balance training). Further studies are warranted to explore the impact of different forms of sport, the combination of sport and different types of exercise and to identify the optimal dose to maximise the benefits for these outcomes in older people.
Surprisingly, we did not find any impact of sport on overall physical activity levels in older participants. However, only two studies investigated physical activity outcomes.27 31 This finding may be explained by the fact that participants might have replaced their usual physical activity with sport. Another potential explanation is that some participants allocated to the sports group experienced AEs during the intervention, which has impacted sport participation and consequently might have decreased overall physical activity levels.
Strengths and limitations
This is the first systematic review with meta-analysis to summarise the impact of sport participation on health-related outcomes specifically in older people. Although some outcomes were not commonly assessed across the studies, we performed a meta-analysis and summarised the pooled effect of sport for most of the included outcomes. We conducted this systematic review in accordance with the PRISMA recommendations and Cochrane Handbook guidelines and followed a protocol registered on PROSPERO. We used a comprehensive search strategy in four medical literature and topic-specific databases. We also included trials where participants were from the general population and with clinical conditions, contributing to a diverse sample.
We acknowledge some limitations of this review. Our results are limited to the short-term or immediate impacts of sport without considering the sustainability of effects, as we only analysed data from the closest post-intervention time-point. Due to the practical challenges in locating and assessing non-English studies, we only included trials published in English. Hence, we may have missed key data from studies in other languages and from LMIC, which may bias our review. We also included studies that involved healthy populations as well as participants with clinical conditions, which could introduce statistical heterogeneity. Due to the inclusion of a few studies in the meta-analysis, we were unable to explore the effect of participants’ characteristics on the pooled effect size. Another limitation is that our review did not identify a wide range of sport types. Only four types of sport were explored in the included trials, and the trials predominantly investigated the impact of soccer (56% trials; 73% publications) on health-related outcomes. As such, conclusions may not be applicable to all forms of sport, such as combat or water sports. Additionally, we identified a limited number of studies investigating outcomes such as quality of life, balance and physical activity, and the interpretation of the impact of sport on these outcomes requires caution and warrants further investigation. Finally, the small number of studies included in our review shows a limited body of evidence in the area. In interpreting the review findings, it is important to note that we provided preliminary evidence, and further research is warranted to investigate the impact of sport on health-related outcomes among older people.
Implications for clinicians and policy-makers
Given the increasing ageing population worldwide and the expected age-associated decline in health, prevention of chronic conditions through an active lifestyle is a priority action area for governments. Therefore, it is crucial to investigate different ways to enable appropriate opportunities for older adults to undertake enjoyable physical activity as they age. One way to promote physical activity at the population level could be sports participation. Our results support promoting sports participation to improve physical and mental health among older people. Sports can be recommended to promote an active lifestyle in leisure time for both healthy older people and those with a wide range of clinical conditions. Sports organisations should prioritise older adults and create appropriate opportunities for those with or without physical limitations and clinical conditions who want to participate in sports. It is also important to draw attention to safe sport participation for older people. Different sports and different ways of commencing sports are likely to impact differently on AEs. Sport organisations should take into consideration appropriate injury prevention strategies when promoting sport participation among older people.
Unanswered questions
Our results identified evidence of the short-term effects of sport in improving health-related outcomes among older people. However, the long-term impact of this type of intervention is not clear. Studies that evaluate the long-term health benefits of sport in older people are needed. Our findings also indicate the need for future research investigating the impact of sport participation in LMIC. Additionally, we only found nine trials investigating the effects of sport in older people, and most of the included trials involved soccer as a form of sport. Further RCTs are warranted to explore the impact of different forms of sport on health-related outcomes in older people. Our review also identified only a few studies of the effect of sport on physical activity, balance, quality of life and mental health, and none on social functioning among older people. More high-quality research targeting these outcomes are needed. The methodological quality of most studies assessed by the PEDro scores was moderate to low (ie, most trials did not include concealed allocation, blinded assessors and intention-to-treat analysis). A better understanding of the role of sport participation on older people’s health outcomes will be enhanced by more methodologically rigorous future research using well-designed interventions. Finally, our results showed a relatively high rate of injuries related to sport, so further studies investigating ways to prevent sport-related injuries and improve safe sport participation for peoeple aged 60+ are also warranted.
Conclusion
This systematic review with meta-analysis provides evidence that sport may offer a promise for improving cardiorespiratory fitness, physical function and mental health, and reducing fat mass among people aged 60 years and older. However, there was uncertain evidence regarding the impact of sport on strength, balance, lean mass, BMD and quality of life, so different types of training or dose may be required to impact these outcomes. Future research is needed to explore the benefits of sports in LMIC, over the long-term and sport-related AEs. More high-quality and well-designed studies targeting the impact of sport on physical activity, balance, quality of life, mental health, social functioning are needed. Further research should also investigate different forms of sports, the combination of sport and other types of exercise, and the optimal dose to maximise the impact of sport participation among older people. A high rate of injuries related to sport participation was identified, and ways to increase safe participation for older people should be further investigated. Due to the limited number of studies in the area, future studies examining the impact on health-related outcomes in older people are also needed.
What are the findings?
Being physically active across the life course is key to maintaining physical function, health and well-being in older age.
Sport could be an enjoyable physical activity option for older people. Many people aged 60+ now participate in traditional and newer modified versions of sport, such as walking football and walking basketball.
There is a clear need for studies investigating the impact of sport participation in older age.
How might it impact on clinical practice in the future?
Sport may offer significant promise for improving cardiorespiratory fitness, physical function, mental health and reducing fat mass among older people.
The impact of sport on other outcomes, including strength, balance, lean mass, bone mineral density and quality of life requires further investigation.
Supplemental material
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @JulianaSOlive11, @mabpinheiro, @AnneTiedemann1, @Leanne_Hassett, @CathieSherr
Contributors JSO, SG, MBP, LH, AT, WK and CS contributed to the study design. JSO coordinated the literature search and data collection with assistance from SG, LBM and LBM. JSO contributed to data analysis and interpretation of the data. JSO drafted the manuscript, and all authors contributed to revisions and approved the final manuscript.
Funding This review used searches undertaken as part of work funded by the World Health Organization.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.