
Abstract
Objective
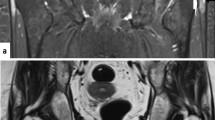
Greater trochanter pain syndrome due to tendinopathy or bursitis is a common cause of hip pain. The previously reported magnetic resonance (MR) findings of trochanteric tendinopathy and bursitis are peritrochanteric fluid and abductor tendon abnormality. We have often noted peritrochanteric high T2 signal in patients without trochanteric symptoms. The purpose of this study was to determine whether the MR findings of peritrochanteric fluid or hip abductor tendon pathology correlate with trochanteric pain.
Materials and methods
We retrospectively reviewed 131 consecutive MR examinations of the pelvis (256 hips) for T2 peritrochanteric signal and abductor tendon abnormalities without knowledge of the clinical symptoms. Any T2 peritrochanteric abnormality was characterized by size as tiny, small, medium, or large; by morphology as feathery, crescentic, or round; and by location as bursal or intratendinous. The clinical symptoms of hip pain and trochanteric pain were compared to the MR findings on coronal, sagittal, and axial T2 sequences using chi-square or Fisher’s exact test with significance assigned as p < 0.05.
Results
Clinical symptoms of trochanteric pain syndrome were present in only 16 of the 256 hips. All 16 hips with trochanteric pain and 212 (88%) of 240 without trochanteric pain had peritrochanteric abnormalities (p = 0.15). Eighty-eight percent of hips with trochanteric symptoms had gluteus tendinopathy while 50% of those without symptoms had such findings (p = 0.004). Other than tendinopathy, there was no statistically significant difference between hips with or without trochanteric symptoms and the presence of peritrochanteric T2 abnormality, its size or shape, and the presence of gluteus medius or minimus partial thickness tears.
Conclusions
Patients with trochanteric pain syndrome always have peritrochanteric T2 abnormalities and are significantly more likely to have abductor tendinopathy on magnetic resonance imaging (MRI). However, although the absence of peritrochanteric T2 MR abnormalities makes trochanteric pain syndrome unlikely, detection of these abnormalities on MRI is a poor predictor of trochanteric pain syndrome as these findings are present in a high percentage of patients without trochanteric pain.



Similar content being viewed by others


References
Bird PA, Oakley SP, Shnier R, Kirkham BW. Prospective evaluation of magnetic resonance imaging and physical examination findings in patients with greater trochanteric pain syndrome. Arthritis Rheum 2001; 44(9): 2138–2145.
Kingzett-Taylor A, Tirman P, Feller J, et al. Tendinosis and tears of gluteus medius and minimus muscles as a cause of hip pain: MR imaging findings. AJR 1999; 173: 1123–1126.
Walsh G, Archibald CG. MRI in greater trochanter pain syndrome. Australas Radiol 2003; 14: 85–87.
Little H. Trochanteric bursitis: a common cause of pelvic girdle pain. Can Med Assoc J 1979; 120: 456–458.
Shbeeb MI, O’Duffy JD, Michet CJ Jr, O’Fallon WM, Matteson EL. Evaluation of glucocorticosteroid injection for the treatment of trochanteric bursitis. J Rheumatol 1996; 23(12): 2104–2106.
Brown RR, Rosenberg ZS, Schweitzer ME, et al. MRI of medial malleolar bursa. AJR 2005; 184: 979–983.
Chung CB, Robertson JE, Cho GJ, et al. Gluteus medius tendon tears and avulsive injuries in elderly women: imaging findings in six patients. AJR 1999; 173: 351–353.
Traycoff RB. “Pseudotrochanteric bursitis”: the differential diagnosis of lateral hip pain. J Rheumatol 1991; 18: 1810–1812.
Bunker TD, Esler CNA, Leach WJ. Rotator-cuff tear of the hip. J Bone Jt Surg Br 1997; 79-B: 618–620.
Raman D, Haslock I. Trochanteric bursitis—a frequent cause of ‘hip’ pain in rheumatoid arthritis. Ann Rheum Dis 1982; 41: 602–603.
Farr D, Selesnick H, Janecki C, Cordas D. Arthroscopic bursectomy with concomitant iliotibial band release for the treatment of recalcitrant trochanteric bursitis. Arthroscopy 2007; 23(8): 905.e1–905.e5.
Pfirrmann CWA, Chung CB, Theumann NH, Trudell DJ, Resnick D. Greater trochanter of the hip: attachment of the abductor mechanism and a complex of three bursae—MR imaging and MR bursography in cadavers and MR imaging in asymptomatic volunteers. Radiology 2001; 221: 469–477.
Cvitanic O, Henzie G, Skezas N, Lyons J, Minter J. MRI diagnosis of tears of the hip abductor tendons (gluteus medius and gluteus minimus). AJR 2004; 182: 137–143.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Blankenbaker, D.G., Ullrick, S.R., Davis, K.W. et al. Correlation of MRI findings with clinical findings of trochanteric pain syndrome. Skeletal Radiol 37, 903–909 (2008). https://doi.org/10.1007/s00256-008-0514-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-008-0514-8