
Abstract
Background
Vegetables and fruit provide a significant part of human nutrition, as they are important sources of nutrients, dietary fibre, and phytochemicals. However, it is uncertain whether the risk of certain chronic diseases can be reduced by increased consumption of vegetables or fruit by the general public, and what strength of evidence has to be allocated to such an association.
Methods
Therefore, a comprehensive analysis of the studies available in the literature and the respective study results has been performed and evaluated regarding obesity, type 2 diabetes mellitus, hypertension, coronary heart disease (CHD), stroke, cancer, chronic inflammatory bowel disease (IBD), rheumatoid arthritis (RA), chronic obstructive pulmonary disease (COPD), asthma, osteoporosis, eye diseases, and dementia. For judgement, the strength of evidence for a risk association, the level of evidence, and the number of studies were considered, the quality of the studies and their estimated relevance based on study design and size.
Results
For hypertension, CHD, and stroke, there is convincing evidence that increasing the consumption of vegetables and fruit reduces the risk of disease. There is probable evidence that the risk of cancer in general is inversely associated with the consumption of vegetables and fruit. In addition, there is possible evidence that an increased consumption of vegetables and fruit may prevent body weight gain. As overweight is the most important risk factor for type 2 diabetes mellitus, an increased consumption of vegetables and fruit therefore might indirectly reduces the incidence of type 2 diabetes mellitus. Independent of overweight, there is probable evidence that there is no influence of increased consumption on the risk of type 2 diabetes mellitus. There is possible evidence that increasing the consumption of vegetables and fruit lowers the risk of certain eye diseases, dementia and the risk of osteoporosis. Likewise, current data on asthma, COPD, and RA indicate that an increase in vegetable and fruit consumption may contribute to the prevention of these diseases. For IBD, glaucoma, and diabetic retinopathy, there was insufficient evidence regarding an association with the consumption of vegetables and fruit.
Conclusions
This critical review on the associations between the intake of vegetables and fruit and the risk of several chronic diseases shows that a high daily intake of these foods promotes health. Therefore, from a scientific point of view, national campaigns to increase vegetable and fruit consumption are justified. The promotion of vegetable and fruit consumption by nutrition and health policies is a preferable strategy to decrease the burden of several chronic diseases in Western societies.
Similar content being viewed by others


Introduction
Vegetables and fruit are extremely important in human nutrition as sources of nutrients and non-nutritive food constituents as well as for the reduction in disease risks. While their importance as sources of nutrients and non-nutritive food constituents is generally accepted, there are still uncertainties regarding their relevance for the prevention of diseases. For this reason, it has to be determined first, for which diseases studies have detected an association between the consumption of vegetables and fruit and the risk of disease, and subsequently, how this association has to be judged. This information provides an important basis to judge the preventive potential of a diet rich in vegetables and fruit. For example, this would allow to estimate the changes regarding the incidence of certain diseases that have to be expected if, for example, the “5 a day” recommendation on the consumption of about 650 g vegetables and fruit per day would be implemented by the majority of subjects in Germany.
Therefore, a working group within the German Nutrition Society (DGE) was established in 2006 with the aim to evaluate the evidence on the role of vegetables and fruit regarding the prevention of certain chronic diseases. The available data were recorded by comprehensive literature search, and the respective strength of the evidence was determined by criteria defined in advance. This evaluation of the evidence was published in 2007 in German as a DGE-statement [1].
As further studies on the association between the consumption of vegetables and fruit and the risk of disease have been published since 2007, it was necessary to update the statement. Therefore, the available data on the diseases selected in 2007 once again were comprehensively recorded with focus on prospective epidemiologic observational and intervention studies, and based upon these study data, the evidence regarding a preventive effect was judged.
Methods
The review is based upon the comprehensive analysis of the epidemiological studies available in the literature on vegetables and fruit. The authors agreed at the beginning of the study to cover the same list of diseases that were included into the DGE-statement from 2007 [1] since no other disease group than the previously selected appeared to be newly associated with consumption of vegetables and fruit. For each disease under consideration, a literature search in the NCBI PubMed database was done that included the literature until December 2010. The search strategy comprised the keywords “fruit” and “vegetables” and the various disease outcomes (Table 1). The type of studies that are searched for differed according to endpoint. Based on the experience from the DGE-statement from 2007 [1], for some endpoints such as type 2 diabetes, hypertension, coronary heart disease, stroke, and cancer, the search had been restricted to intervention and cohort studies. For other endpoints, all types of epidemiological studies had been looked at in the database. In addition to the studies identified in the newly conducted literature search, the references in relevant publications were reviewed in order to have identified all of the studies. Also, the literature research in conjunction with the DGE-statement from 2007 [1] was taken into account. Furthermore, studies that have been published until April 2011 were included in the review if they contain new information relevant for the judgement of the evidence.
The scheme of generating the level of evidence associated with each study according to its study design followed the considerations of the WHO [2] and the evidence-based guidelines for the prevention of nutrition-related diseases of the DGE [3]. Intervention studies were given the highest level of evidence, followed by methodologically well-conducted cohort studies (Table 2). Meta-analyses are rated higher than individual studies among its level. In theory, for deriving the relative risk, case–control studies have similar strength than cohort studies. In practice, however, compared with cohort studies, they have the disadvantage of recall and selection bias. This especially applies to case–control studies in the field of nutrition. Therefore, they are rated with a lower level of evidence than cohort studies. Likewise, cross-sectional studies are allocated with a low level of evidence because their study design does not show a clear temporal connection between the investigated nutritional factor and the disease.
Based on the number of available studies and their classifications of level of evidence, the judgement of the strength of the evidence was performed (Table 2). In total, four categories of the strength of the evidence were used [3], termed as convincing, probable, possible, and insufficient. Table 2 shows the connection between the levels of evidence of the studies and the overall strength of the evidence. In addition to the relation between the level of evidence of the studies and the strength of the evidence, there were also further specifications that determined the strength of the evidence:
Convincing evidence regarding a preventive effect or a lack of an association
The strength of evidence was judged as “convincing” if at least 2 studies of highest quality (level of evidence I) showed consistent results. If the studies showed methodological weakness or were only cohort studies, the minimum number of intervention studies was raised to 5. However, for this strength of the evidence, it was required that the question has been extensively investigated and that there were a lot of results from different study populations including comprehensive data on consumption. Results from cohort studies should have been confirmed by intervention studies with intermediary markers regarding causality. Ideally, a meta-analysis of the present studies is available that did neither indicate heterogeneous study results nor include a high percentage of study results with opposite effects.
Probable evidence regarding a preventive effect or a lack of an association
The strength of the evidence was judged as “probable” if epidemiological studies showed consistent relations between factor and disease, but also showed weaknesses regarding the causal argumentation. This may be the case, for example, (1) if compared with the “positive” studies, there are a considerable number of studies without risk relation, (2) if there is a lack of study results or inconsistent results from intervention studies with intermediary markers, or (3) if meta-analyses gave heterogeneous results. The number of studies required to classify the strength of the evidence as “probable” remains at not <5 very good studies with level of evidence I and/or level of evidence II.
Possible evidence regarding a preventive effect or a lack of an association
The strength of the evidence was judged as “possible”, if most epidemiological studies, but at least 3, showed consistent results. There may exist a few other studies without any risk relation or with opposite risk relation, respectively.
Insufficient evidence regarding a preventive effect or a lack of an association
The strength of evidence was judged as “insufficient” if data were lacking because the relation between nutritional factor and disease has not yet or only rarely been investigated in the present studies. Further criteria were inconsistent results with a majority of studies without risk relation and nearly equally as strong opposite results.
However, despite the assignment of the level of evidence to each study and the strict specification of the strength of evidence, the database has not been shown to be always clear. Thus, in addition to the level of evidence and the number of studies, both the assessment of the study quality and the current estimation of the studies’ importance based on its design and size were considered as well.
The evaluation of the strength of evidence does not include the estimate of the quantity of intake of vegetables and fruit. In view of the ranking ability of the food frequency questionnaire as prime measurement feature that is the most often used dietary assessment instrument in cohort studies, and the difficulty in estimating adherence to dietary behaviour in intervention studies, we also abstained from considering the published intake values of vegetables and fruit. In addition, we would like to note that in nearly all of the studies, a linear model of trend across the ordered categories of intake was fitted meaning that a change in intake has been related to risk and not an absolute intake.
Consumption of vegetables and fruit
For the European Nutrition and Health Report [4], food consumption in Europe was analysed with data from representative nutrition surveys in 19 countries, which were documented in a database of the European Food Safety Authority (as of 2008). Data were directly comparable only to a limited extent due to different survey methodology and periods. However, the following results on the average consumption of vegetables and fruit per person can be derived: along with Poland, Italy, Austria, Germany is among the 4 countries in which an average of more than 400 g vegetables and fruit was consumed daily. The consumption of vegetables in Southern Europe (Greece, Italy, Portugal, Spain, Cyprus) as well as in Central and Eastern Europe (Germany, Austria, Poland, Romania, Slovenia, Czech Republik, Hungary) with about 250 g/day was higher than in Northern Europe (Denmark, Estonia, Finland, Latvia, Lithuania, Norway, Sweden) with 140 g/day. The highest fruit consumption was found in Central and Eastern Europe (209 g/day) as well as in Southern Europe (203 g/day). In Northern Europe, the fruit consumption was 129 g/day and in Western Europe (Belgium and Luxembourg, France, Ireland, The Netherlands, Great Britain) 113 g/day.
This south–north gradient was also observed in a cross-sectional analysis of the consumption data (24-h recall) in 35,955 men and women from the EPIC cohorts in 10 European countries. In men, the highest mean vegetable intake adjusted for age, season, and day of the week was observed in Greece (270 g/day), the lowest (103 g/day) in Umeå (Sweden). In men from Germany, the vegetable intake was 170 g/day (Heidelberg) or 151 g/day (Potsdam). In women, vegetable intake was highest in southern France (261 g/day) and lowest in Asturias, Northern Spain (103 g/day). In the German survey centres, the intake in women was about 165 g/day. The mean fruit intake adjusted for age, season, and day of the week in men was between 454 g/day in Murcia (Spain) and 122 g/day in Malmö (Sweden), and in women between 400 g/day in Ragusa (Italy) and 151 g/day in Malmö (Heidelberg: men 175 g/day and women 213 g/day; Potsdam: men 239 g/day and women 260 g/day) [5].
Data from 196,373 adults from 52 countries with mainly small and middle income who were interviewed in the World Health Survey (2002–2003) (24-h recall) showed that about 78 % of the men and women consumed <5 portions of vegetables and fruit daily as recommended by the World Health Organisation (WHO, according to the WHO: 400 g/day) [6].
Judgement of the evidence regarding individual diseases
In the following, at first, the symptoms of the individual diseases and the most important influencing factors are described. Then, the available data and the most important studies are summarised, and in conclusion, the strength of the evidence is judged.
Obesity
The prevalence of pre-obesity and obesityFootnote 1 has been rising in recent decades in European countries. For example, in the EPIC–DIOGENES cohort, the prevalence of obesity in 60- to 65-year-olds increased within 8.6 years of follow-up from 21.5 to 27.8 %. In this cohort study, it was also observed that in the current generation of elderly people, overweight persisted into old age once it has been developed [7]. Overweight or obesity occurs disproportionately often in individuals that have unfavourable socioeconomic indicators regarding education, income, and professional position [8]. Particularly, alarming is the sharp increase in obesity in children and adolescents. According to the data of the PreVENT Study, which includes the results of the German representative national KiGGS Study and also of other large surveys in Germany (KOPS, IDEFICS, CHILT), 12 % of the 3- to 6-year-old, 17.9 % of the 7- to 10-year-old, 18.9 % of the 11- to 13-year-old, and 15.0 % of the 14- to 17-year-old children and adolescents are overweight.Footnote 2 Averaged over all age groups, nowadays, 6 % of the children and adolescents are obeseFootnote 3 (Müller M, own results).
Overweight occurs if energy intake is higher than energy expenditure. Compared with many other foods, the volume of vegetables and fruit in relation to the energy content is larger. Due to the favourable volume to energy ratio of vegetables, and fruit, satiety signals can emerge without consuming a large amount of energy [9]. The extent is not known to which individual constituents of vegetables and fruit such as dietary fibre are involved in the regulation of hunger and saturation and hence body weight.
The association between vegetable and fruit consumption and weight development was summarised in the ISAFRUIT Project of the EU from 2008 [12]. Eleven out of the 16 identified studies observed an inverse association, including 3 intervention studies and 8 prospective observational studies. In addition to the 8 prospective studies of the ISAFRUIT summary, including 5 studies that showed an inverse relation, there are other prospective studies on the association between the consumption of vegetables and fruit and weight change, which either have been published later than the ISAFRUIT summary or have not been included in the summary. They either showed an inverse relation [13–16] or no relation or relations that were only evident in subgroups differentiated by gender or food groups [17–19]. In one of the studies, a positive relation was observed [20]. Some of the studies investigated the consumption of vegetables and fruit in relation to a dietary pattern. In these studies, the role of vegetable and fruit consumption per se is difficult to assess. In longitudinal investigations in infants and children (observation periods were between 1 and 8 years), the consumption of vegetables and fruit did not have a significant influence on the maintenance of normal weightFootnote 4 or the incidence of overweight [21, 22]. Children with persistent overweight throughout the observation period had a higher fat and a lower vegetable and fruit consumption than overweight children, who could reduce weight during the observation period [23]. However, it is not possible to detect differences in the effects of fat and vegetables and fruit in this study. The same weak or not evident influence was seen in results from cross-sectional studies ([24, 25], PreVENT unpublished data). Contradictory, a prospective study showed that a high consumption of fruit juice had a minor positive influence on weight gain [26].
Intervention studies with vegetables and fruit without focus on weight reduction were systematically analysed in a review [27]. The few studies that only had vegetables and fruit as an intervention either showed no changes in weight development or observed weight changes were comparable to the control group. A slightly more favourable effect regarding weight development was observed in studies with simultaneous fat reduction, as in some of these interventions, spontaneous weight loss occurred. Intervention studies on weight reduction are investigations that only indirectly provide information on the role of vegetables and fruit for weight development. Instructions to eat more vegetables and fruit to stabilise weight resulted in variable extents of weight reduction including substantial weight loss. This weight loss had been linked to reduced energy density [28]. It was shown in an intervention study that at fat reduction, an increase in vegetable intake enhances weight loss [29]. However, another intervention study with 1,510 women with breast cancer did not observe weight loss with such an intervention over 4 years [30].
In summary, these studies showed that an increase in vegetable and fruit consumption might be a suitable measure to facilitate initial weight loss and subsequent weight stability [27]. In this context, it seems also to be important to address energy reduction as well. We could not identify studies investigating in children and adolescents, whether an increase in vegetable and fruit consumption influences body weight.
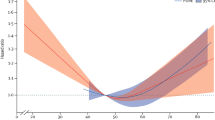
For the range of normal weight and slight overweight, the Women’s Health Initiative (WHI) Dietary Modification Trial reported about the role of vegetables and fruit for long-term weight stability. In this randomised intervention study including 48,385 women (aged 50–79 years), the intervention group was given specific advice regarding an increase in the consumption of both vegetables and fruit (target ≥5 portions/day) and cereal products (target ≥6 portions/day) as well as a reduced intake of fat (target <20 energy %). A first analysis showed a lower weight increase in normal-weight women in the intervention group (+1.1 portions of vegetables and fruit per day at fat reduction of 8 energy %) than in the control group, while in obese women, weight reduction was observed in both, the intervention and the control group. Thus, using all study data and a multivariate regression model, the change in consumption of vegetables and fruit was just not significantly (p = 0.06) associated with weight increase, with one portion being associated with 60 g body weight increase over 9 years. Another analysis across all BMI classes showed that this relation is nonlinear and that an increase in consumption of vegetables and fruit of more than 2.2 portions per day (ca. 200 g) was associated with weight reduction [31]. As the primary objective of this multiple intervention was a reduction in fat intake, the significance of this study regarding the benefit of vegetable and fruit consumption is limited.
It can be concluded from both the prospective and the intervention studies that there is possible evidence that an increase in the consumption of vegetables and fruit contributes to weight stability (i.e. no weight increase occurs). There is also probable evidence that an increase in vegetable and fruit consumption alone does not result in weight loss. There is probable evidence that an increase in the consumption of vegetables and fruit leads to weight reduction, if this replaces foods rich in fat or energy. In children and adolescents, there is only insufficient evidence regarding an association between the consumption of vegetables and fruit and weight development due to a lack of intervention studies and the existence of only a few cohort studies with no risk relation.
Type 2 diabetes mellitus
Type 2 diabetes mellitus is one of the most common and most expensive chronic diseases. According to the International Diabetes Federation, the diabetes prevalence in the 20- to 79-year-olds was 6.4 % for women [32] with large regional differences (e.g. 3.8 % in Africa, 6.9 % in Europe, and 10.2 % in North America). Due to ageing of populations, this prevalence is expected to increase to 7.7 % by the year 2030 with an expected 237 million affected individuals. These estimates include millions of undetected cases, because at the beginning, the disease often is free of symptoms and is only diagnosed years later [33], but does not include the rise of prevalence due to changes in other major risk factors beyond age, like the rise of obesity prevalence rates and adoption of Westernised diet and lifestyle habits in many parts of the world. The prognosis of affected individuals is crucially determined by the presence of accompanying risk factors and by the development of micro- and macroangiopathic complications. Cardiovascular events like myocardial infarction, stroke, and peripheral arterial circulation disorders are predominant [34].
Type 2 diabetes mellitus develops due to a complex interaction between genetic predisposition and lifestyle. The actual manifestation of the disease is preceded by a phase of impaired glucose regulation, in which the cardiovascular risk is already increased. Particularly important among the lifestyle factors that promote or accelerate the manifestation of type 2 diabetes mellitus are bad nutritional habits and a lack of physical activity [35]. However, the most important risk factor for the development of type 2 diabetes mellitus is truncal obesity, which also is the result of an unfavourable lifestyle including overeating and a lack of physical activity.
The results of several prospective cohort studies that investigated whether the consumption of vegetables and fruit is associated with the risk of type 2 diabetes mellitus were summarised in 2 meta-analyses. The meta-analysis by Hamer and Chida [36] including 5 cohort studies in total did not show a relation between the consumption of fruit and/or vegetables and the risk of diabetes. Individuals who consumed at least 5 portions of vegetables and fruit per day had a relative risk (RR) of 0.96 (95 % CI 0.79–1.17) compared with persons with low consumption (lowest quintile or non-consumers; 3 cohort studies). For vegetables and fruit analysed separately (4 cohort studies each), there also was no association (RR regarding ≥3 vs. <3 portions/day: fruit consumption: 1.01; 95 % CI 0.88–1.15; vegetable consumption: 0.97; 95 % CI 0.86–1.10). In another meta-analysis [37], 2 more recent cohort studies were included, but one study that was included into the meta-analysis by Hamer and Chida was not considered. Here again, there was no risk relation regarding the total intake of vegetables and fruit: the RR for the comparison of the highest with the lowest category of consumption was 1.00 (95 % CI 0.92–1.09). Also, the consumption of either fruit (RR 0.93; 95 % CI 0.83–1.01) or vegetables alone (RR 0.91; 95 % CI 0.76–1.09) was not associated with the risk. However, the risk of diabetes was significantly reduced in persons that consumed relatively large amounts of green leafy vegetables. Other subgroups of vegetables and fruit have not been investigated.
In addition to the studies considered in the meta-analyses, some other prospective cohort studies exist, but in general, they also did not observe a significant relation between the overall consumption of vegetables and fruit and the risk of diabetes [38–40]. However, in the EPIC-Norfolk Study [40], a significant risk reduction was observed with increased fruit consumption (RR for the comparison of highest and lowest quintile: 0.70; 95 % CI 0.54–0.90). In a meta-analysis of cohort studies, no significant associations were observed between the intake of dietary fibre from fruit (9 individual cohort studies; RR comparing extreme quintiles/quartiles 0.96; 95 % CI 0.88–1.04) or vegetables (7 individual cohort studies; RR comparing extreme quintiles/quartiles 1.04; 95 % CI 0.94–1.15) and the risk of diabetes [41].
The present cohort studies were usually adjusted for BMI, as the possible effect of a higher vegetable and fruit consumption on body weight could not be separated from the potential confounding effect of body weight. Therefore, the results of the cohort studies describe the relation between vegetable and fruit consumption and the risk of diabetes excluding this important factor, through which the consumption can ultimately influence the risk of diabetes. In randomised controlled intervention studies, it was shown that a change in lifestyle with a focus on weight reduction through dietary changes can reduce the conversion from impaired glucose tolerance to type 2 diabetes [42–44]. However, the role of vegetable and fruit consumption remained unclear in these studies, as the interventions were designed multifactorially and included increased physical activity in addition to dietary changes [43, 44]. It may still be expected that higher consumption of vegetables and fruit can lower the risk of diabetes, as such a dietary change might prevent the development of obesity ([27], see “Obesity”). In the intervention arm of the WHI Dietary Modification Trial (see “Obesity”), an increase in vegetable and fruit consumption by 1 portion combined with a reduction in the fat proportion by 8 % of energy intake did not result in a changed risk of type 2 diabetes mellitus over 7 years [45].
In summary, it can be concluded that most of the studies and their meta-analysis indicate a lack of an association between the consumption of vegetables and fruit and the risk of diabetes. Because of this, there is probable evidence that the risk of developing type 2 diabetes mellitus is not influenced by the consumption of vegetables and fruit. However, vegetables and fruit indirectly influence the prevention of type 2 diabetes mellitus, as consumption thereof might lower the risk of weight gain in adults.
Hypertension
Hypertension is one of the most relevant clinical findings for public health policy, with a global prevalence of 26 % in the adult population in 2000. Twenty-nine percent were projected to have this condition by 2025 [46]. About 90 % of subjects with hypertension suffer from essential hypertension, that is, hypertension is not the consequence of another disease. Due to the increased risks of stroke and CHD [47], and also of renal cancer [48] associated with hypertension, lifelong medication is usually required. It could be shown that even a slight reduction in the mean blood pressure in the population strongly reduces the incidence of cardiovascular diseases [49, 50]. The American Heart, Lung and Blood Institute has stated in 2003 that the measures for the prevention of hypertension include a health-promoting lifestyle which in addition to weight reduction (at existing overweight) comprise the adherence to the DASH diet,Footnote 5 the limitation of sodium and alcohol intake as well as increased physical activity [51]. The ESH–ESC Task Force on the Management of Arterial Hypertension [52] of the European Society of Hypertension regards the increase in the consumption of vegetables and fruit as one of the lifestyle measures that can lower blood pressure in individuals with only a few risk factors for cardiovascular diseases and slightly increased blood pressure.
The INTERSALT Study with data of more than 10,000 subjects from 52 centres in 32 countries has shown an inverse relation between the intake of potassium (a mineral associated with a plant-based diet high in vegetables and fruit) and blood pressure, independent of the quantity of sodium intake [53]. However, in a small tightly controlled intervention study over 6 weeks including 48 participants with slightly increased blood pressure, such an effect could not be shown [54].
In vegetarians, there is often a lower blood pressure observed than in the total population, and a reduction in the blood pressure has been seen after changing from a normal to a vegetarian diet [55]. In cohort studies, there were either inverse relations between the consumption of vegetables and fruit and new cases of hypertension [56, 57] or inverse relations with one of the two food groups considered here or with a dietary pattern including vegetables and fruit [58, 59]. In the cross-sectional and in the longitudinal analysis of the SU.VI.MAX Study, an inverse relation was observed between vegetable and fruit consumption and blood pressure [60]. There was no relation seen regarding other components of the DASH diet. The intervention with antioxidant vitamins did also not influence the development of blood pressure. In the SUN cohort study in turn, it was observed that a high consumption of vegetables and fruit was only associated with a reduced risk of hypertension, if the consumption of olive oil was low (<15 g/day) [61]. Another analysis of the Nurses’ Health Study (NHS) I and II and the Health Professionals Follow-up Study (HPFS) after 14 years of follow-up with flavonoid intake calculated by an updated nutrient database from 2010 showed a risk reduction in hypertension with increasing intake of anthocyanins [62].
The DASH diet is based upon the DASH Study, which is a randomised 8-week intervention study including 459 hypertensive patients. One intervention group was instructed to eat a diet rich in vegetables and fruit, and the other group got the same instructions with additional information on a diet low in fat and high in dietary fibre. In both intervention groups, a lowering of blood pressure was reported [63]. In the latter group, the blood-pressure-lowering effect was more pronounced than in the group that was only instructed to eat a diet rich in vegetables and fruit. Other intervention studies have confirmed the effectiveness of the DASH diet as measure for reducing blood pressure levels. For example, the DASH intervention in the Premier Trial Study including 810 adults with hypertension achieved a greater decrease in blood pressure levels by an increased consumption of vegetables and fruit as well as of low-fat dairy products than the intervention with weight reduction, enhanced physical activity, and limitation of sodium intake [64]. In children and adolescents, too, this diet is suitable to lower blood pressure levels [65]. A 6-month intervention study including 690 subjects at the age of 25–64 years in England confirmed the results of the DASH study [66]. In this study, an increase in the consumption of vegetables and fruit to at least 5 portions/day was accompanied by a lowered blood pressure. Furthermore, the study showed that an increase in vegetable and fruit consumption does neither lower the blood cholesterol concentration nor leads to weight loss, but keeps weight stable. An intervention study conducted in the 1990s including 78 participants with low consumption of vegetables and fruit (<3 portions/day) revealed that lipid and lipoprotein metabolism are not influenced by an increase in vegetable and fruit consumption [67].
Based on the present data, the evidence regarding a blood-pressure-lowering effect of an increase in the consumption of vegetables and fruit is judged as convincing. Both cohort and intervention studies show consistent results.
Coronary heart disease
Coronary heart disease (CHD) is the most important manifestation of arteriosclerosis in humans and belongs to the large group of cardiovascular diseases. CHD is still the single largest cause of premature death in the world. Ischaemic heart disease has been estimated to account for 12 % of all deaths worldwide in 2004 [68]. In 2008, 17 million deaths worldwide were due to cardiovascular diseases, accounting for 48 % of non-communicable disease deaths [69]. While CHD death rates have declined in many parts of the industrialised world, death rates are increasing in most developing countries [70]. CHD is also a major cause of disease burden in terms of disability-adjusted life years lost (DALY), accounting for 63 million DALYs worldwide in 2004 [68].
In addition to age and gender, modifiable risk factors are important, especially lifestyle factors like smoking and a lack of physical activity and the medical diagnoses hypertension, diabetes mellitus, obesity, and dyslipoproteinaemia [71]. Among these factors, the 4 medical diagnoses are clearly nutrition-related and can be influenced by a change in nutrition. Other biological mechanisms that are probably important in atherogenesis are influenced by nutrition, including inflammatory processes, oxidative stress, and increased homocysteine concentrations [72].
Several prospective cohort studies that investigated whether the consumption of vegetables and fruit is associated with the risk of CHD were summarised in 2 meta-analyses. In the meta-analysis by Dauchet et al. [73], which included 9 cohort studies, the risk of CHD was reduced by 4 % (RR 0.96; 95 % CI 0.93–0.99) per portion of vegetables and fruit and by 7 % (RR 0,93; 95 % CI 0.89–0.96) per portion of fruit daily. For vegetables, the inverse relation regarding the risk of CHD was stronger for the overall cardiovascular mortality (RR per portion 0.74; 95 % CI 0.75–0.84) than for fatal or non-fatal myocardial infarction (RR 0.95; 95 % CI 0.92–0.99). Between mortality and consumption of fruit as well as total intake of vegetables and fruit, a linear dose–response relation was observed. In contrast, the relation between mortality and consumption of vegetables was nonlinear. The meta-analysis of He et al. [74] included 13 cohort studies. Compared with individuals who consumed <3 portions of vegetables and fruit per day, persons with a consumption of 3–5 portions per day (RR 0.93; 95 % CI 0.86–1.00) and of >5 portions per day (RR 0.83; 95 % CI 0.77–0.89) had a lower risk of CHD. Subanalyses revealed a significant inverse relation with the risk of CHD both for fruit and for vegetables. In the following years, after the publication of these meta-analyses, the result of other cohort studies was published. A higher vegetable and fruit intake was inversely associated with the risk of CHD in the EPIC-Heart Study [75], the Morgen Study [76], a Swedish [77], and a Japanese cohort [78], while in the Italian arm of the EPIC Study, no association was found for vegetables and fruit in total, but for leafy vegetables [79]. These data are also reflected in the judgement of the WHO [80] and current nutritional recommendations of the European Society of Cardiology [71] and the American Heart Association [81] that both recommend the consumption of vegetables and fruit to reduce the risk of CHD.
However, the results of the WHI Dietary Modification Trial (see “Obesity”) suggest that an additional portion of vegetables and fruit daily does not influence the risk of CHD [82]. As the primary objective of this multiple intervention is a reduction in fat intake, the significance of this study regarding the assessment of the benefit of vegetable and fruit consumption is limited.
The data on the outcome “CHD” are supplemented by intervention studies that have investigated intermediary clinical markers of the cardiovascular system when offering specific kinds of vegetables and fruit. These studies showed that the consumption of vegetables and fruit can improve the regulation of blood vessel enlargement [83], prevent platelet aggregation [84–86], and reduce inflammation markers [87, 88].
In summary, it can be concluded that many cohort studies on this question have been performed, and most of the cohort studies have shown a protective association between the consumption of vegetables and fruit and the risk of CHD. In addition, there are intervention studies that prove a beneficial influence of vegetables and fruit on metabolic pathways that are associated with the risk of CHD. Therefore, the evidence regarding the prevention of CHD by high consumption of vegetables and fruit is judged as convincing.
Stroke
Stroke is one of the major causes of death in the world. In 2004, 9.7 % of all deaths were caused by stroke [68]. Stroke causes also a considerably proportion of disability adjusted life years (DALYs), ranking sixth among the leading causes worldwide [68].
In addition to age and gender, modifiable risk factors are important, especially lifestyle factors like smoking and a lack of physical activity as well as postmenopausal hormone replacement therapy, and the diagnoses hypertension, diabetes mellitus, obesity, dyslipoproteinaemia, CHD, arterial occlusive disease, extracranial stenoses, or occlusion of the arteries supplying the brain [89]. The clinical findings of these factors are clearly nutrition-related and can be influenced by a change in nutrition.
The results of several prospective cohort studies that investigated whether the consumption of vegetables and fruit is associated with the risk of stroke were summarised in 2 meta-analyses [90, 91]. In the first meta-analysis, including 7 cohort studies, the risk of stroke was reduced by 11 % (RR 0.89; 95 % CI 0.85–0.93) per portion of fruit per day, by 5 % (RR 0.95; 95 % CI 0.92–0.97) for vegetables and fruit, and by 3 % (RR 0.97; 95 % CI 0.92–1.02) for vegetables [90]. In this meta-analysis, a linear dose–response relation was observed. The second meta-analysis included 9 individual cohort studies [91]. Compared with individuals with an intake of vegetables and fruit of <3 portions per day, subjects with 3–5 portions per day (RR 0.89; 95 % CI 0.83–0.97) and with >5 portions per day (RR 0.74; 95 % CI 0.69–0.79) had a significantly lower risk of stroke. These results were confirmed by a study that was published after the meta-analyses. In this cohort study with Japanese participants, a higher fruit consumption was associated with a significantly lower risk of stroke (RR for the comparison of the highest with the lowest quintile of consumption: 0.67; 95 % CI 0.55–0.81) [78]. However, there was no significant relation between the intake of vegetables and the risk of stroke. Overall, the available data indicate a risk-reducing effect of vegetable and fruit consumption. This is also reflected in the judgement of the WHO [80] and current dietary recommendations of the European Society of Cardiology [71] and the American Heart Association [89].
In the WHI Dietary Modification Trial (see “Obesity”), with an additional portion of vegetables and fruit per day, there was no difference regarding the occurrence of stroke [82]. However, the significance of this study is limited, because the primary objective of this multiple intervention was a reduction in fat intake.
The data on the outcome “stroke” are supplemented by intervention studies that have investigated intermediary clinical markers of the cardiovascular system when offering specific kinds of vegetables and fruit (see “Coronary heart disease”; [83–88]).
The meta-analyses of cohort studies clearly indicate that there is an inverse association between the consumption of vegetables and fruit and the risk of stroke. Additional intervention studies show a favourable influence of the consumption of vegetables and fruit on important metabolic pathways, which also have an impact on the risk of stroke. From these results it can be concluded that a high intake of vegetables and fruit reduces the risk of stroke with convincing evidence.
Cancer
In 2008, about 2,457,610 new cases of cancer were observed in the European Union [92]. For the same year, cancer was recorded as cause in 1,231,220 deaths. Therefore, both in numerical and in socioeconomic terms, cancer is one of the most important chronic diseases in the European Union.
The occurrence of cancer as a whole is increasing with age and the pathogenesis often takes several decades. The disease is characterised by chromosomal changes that can be induced due to different reasons. In addition to age, the most important risk factors include tobacco smoking, consumption of alcohol, overweight, hormonal factors, physical activity, and food intake [2].
A summary published in 1992 of the results of epidemiological studies, mostly case–control studies, on the association between consumption of vegetables and fruit and the occurrence of cancer showed high consistency regarding an inverse risk relation (128 out of 156 studies; [93]). This resulted in the “5 a day” campaign in the USA with the aim to reduce the incidence of cancer. In the report of WCRF experts published in 1997, which was based upon data until the beginning of the 1990s, vegetables and fruit were rated among the most important cancer preventive factors with a calculated prevention potential of 23 % and the strength of evidence was rated as convincing for many cancer sites [94]. Similar, but also lower prevention figures were revealed for some European countries when using a different methodological approach and similar relative risk estimates [95, 96].
In 2003, a new revaluation of the cancer preventive potential of vegetables and fruits was performed by an expert panel of the International Agency for the Research on Cancer [97]. As data from prospective cohort studies had become available increasingly, they were included in this evaluation for the first time. This new evaluation resulted in strength of the evidence that was one grade lower than in the WCRF report. According to the data in 2003, there was probable evidence for a protective effect of vegetables regarding cancer of the oesophagus and colon and rectum, and possible evidence regarding cancer of the oral cavity, pharynx, stomach, larynx, lung, ovary and kidney. There was probable evidence for a protective effect of fruit regarding cancer of the oesophagus, stomach, and lung and possible evidence for a protective effect regarding cancer of the oral cavity, pharynx, colon, rectum, larynx, kidney, and bladder. A meta-analysis published at the same time period resulted in the same conclusions [98]. The data available until 2007 and a detailed systematic evaluation of the evidence regarding the different sites of cancer are included in the German Nutrition Report 2008 [99]. This evaluation will be continued in the German Nutrition Report 2012.
Currently, data are dominated by the results of the large prospective cohort studies such as EPIC [100] and NIH–AARP Study [101], each including more than 500,000 participants, and the Pooling Project, which is a pooled analysis of up to 17 cohort studies. Key [102] summarised the results of these studies until 2009, both for cancer in general and regarding the most important cancer sites. The data regarding the different cancer sites are characterised by reduced risks in connection with high consumption of vegetables and fruit; however, the risk relations are often not statistically significant or only just significant, and the risks differ depending on the smoking behaviour. Therefore, the data situation regarding a specific cancer site appears to have a high degree of complexity, and conclusions for a specific cancer site cannot be drawn within the context of this review. Regarding a judgement on the association between the consumption of vegetables and fruit and different types of cancer, we therefore refer to future work.
Several studies have investigated the relation between the consumption of vegetables and fruit and cancer in general [103–106]. Such investigations do not provide information on specific mechanisms, but are important for public health, as they give an overall evaluation. The analyses of the Harvard studies (NHS I, NHS II, HPFS) and of a Japanese study did not indicate a relation between this nutritional factor and the risk of cancer [103, 104]. The analysis of the NIH–AARP showed a significantly reduced risk at high vegetable intake in men, but not in women [105]. In the EPIC study, a lowered risk of cancer was observed both with higher intake of vegetables and with higher intake of fruit [106]. In all of the studies, the reduction in risk was small in view of the investigated range of consumption. In addition, it has to be considered that the risk reduction was mainly seen in those types of cancer that are associated with smoking [106]. Therefore, it remains unclear, whether this risk reduction goes along with a lifestyle of high exposure to carcinogens, or whether the risk reduction is due to a lack of statistical control of the smoking factor.
In addition to cardiovascular diseases, the aim of the WHI Dietary Modification Trial (see “Obesity”) was the investigation into colon and breast cancer. Compared with the control group, the achievements in the intervention arm of an increase in vegetable and fruit consumption by 1 portion per day and a reduction in the percentage of fat on energy intake by 8 % did not result in a changed risk of colon cancer over 7 years and resulted in only a slight, non-significant reduction in risk of breast cancer [107, 108]. Although the significance of this study regarding vegetables and fruit is limited due to the multiple interventions, the results are in accordance with the results obtained from the observational studies by confirming that there will be no detectable effects on risk of cancer if there are only small differences in the consumption of vegetables and fruit.
The risk reductions that have been observed in some large cohort studies with increasing consumption of vegetables and fruit still suggest that the consumption of vegetables and fruit influences the risk of cancer. However, this influence is only detectable if there are large differences in the consumption of vegetables and fruit between the groups and could appear only in case of high exposure to carcinogens, like, for example, in smokers. However, these restrictive statements do not directly influence the evidence regarding an inverse relation between the consumption of vegetables and fruit and the risk of cancer, which is judged as probable.
Chronic inflammatory bowel diseases
Chronic inflammatory bowel diseases (IBD) like Crohn’s disease and ulcerative colitis are examples of chronically recurrent diseases of the gastrointestinal tract. Incidence and prevalence of these diseases are increasing in Western industrial countries [109, 110]. Both disorders affect people in approximately equal female/male proportion with a combined mean frequency of 5–200 cases per 100,000 European and North American inhabitants [110]. The incidence of Crohn’s disease is still increasing in Western societies, demonstrating the importance to add mechanistic insights into the yet unknown aetiology of the disease pathogenesis. The low concordance rate in identical twins for Crohn’s disease (~50 %) and ulcerative colitis (~10 %) confirms epidemiologic observations that environmental factors strongly contribute to the disease progression [111].
The aetiology of Crohn’s disease and ulcerative colitis is still not known, but evidence is growing that environmental factors (nutrition, smoking, infections) combined with genetic predisposition strongly enhance the risk of this disease [112]. The clinically manifest inflammation of the disease might be caused by a primary intestinal barrier malfunction that leads to a secondary inflammatory response and is maintained by chronically activated immune cells in the bowel [113]. The results of many clinical and experimental investigations into gnotobiotic animal models in recent years show that an imbalance between intestinal microorganisms (microbiome) and the immune system contributes significantly to the development of chronic inflammatory processes in the bowel [114]. These uncontrolled activation reactions in the bowel cause tissue damage that affects all layers of the intestinal wall in Crohn’s disease (transmural), whereas in ulcerative colitis, it mainly involves the superficial epithelial layer of the colon. Recent animal studies show the influence of iron on the composition of the intestinal microbiome and that a high intake might be involved in the pathogenesis of chronic inflammatory processes in the bowel [115]. In addition, the role of vitamin D deficiency in the pathogenesis of chronic intestinal inflammatory processes and the IBD-associated colorectal carcinoma is also discussed [116]. The close interaction of the composition and function of the microbial ecosystem with nutritional factors suggests that the intake of vegetables and fruit might be involved in the occurrence of inflammatory processes in the bowel [117].
A first systematic review (5 case–control studies on Crohn’s disease and 8 case–control studies on ulcerative colitis) concluded that a high intake of fruit is associated with reduced risk of Crohn’s disease; there was no statistically significant association regarding vegetables. No association was found between ulcerative colitis and fruit, while a trend was observed towards a risk reduction regarding vegetables [118]. There are no prospective cohort and intervention studies that investigated the role of vegetables and fruit for the aetiology of IBDs.
There is insufficient evidence regarding the association between the consumption of vegetables and fruit and the risk of developing IBDs.
Rheumatoid arthritis
Rheumatoid arthritis (RA) is the most common rheumatic disease. In industrialised countries, 0.3–1.5 % of the population suffers from RA [119]. Women are affected three times more often than men [120]. RA is a chronic inflammatory disease that primarily affects the joints. The cause of the disease is unknown to a large extent. In addition to genetic factors, smoking, overweight, and nutrition contribute to the risk of disease [121]. As to nutrition, the risk seems to be increased by the consumption of red meat, protein, and coffee, while it is lowered by oily fish and olive oil.
To estimate the importance of the consumption of vegetables and fruit for the development of RA, 4 prospective cohort studies [121–124], 1 cross-sectional study [125], 1 case–control study [126], and 1 intervention study [127] in total were identified. Most of the cohort studies show a reduced risk at high consumption of vegetables and fruit [121–123]. The study that did not find an inverse association did not report the absolute amount of vegetable and fruit consumption [24]. Therefore, it is difficult to compare this study with the other cohort studies. In the only available case–control study, higher consumption of cooked vegetables (2.9 servings/day) was significantly associated with lower risk, while raw vegetables were not effective [126]. In a cross-sectional study by Wang et al. [125], less bone marrow lesions were observed in healthy individuals with high intake of fruit. Vegetable intake was not significantly associated with bone measures. In a pilot study in women suffering from RA, a long-lasting improvement of symptoms was achieved through the intervention resulting in a small increase in intake of fruit, vegetables, and legumes (increase from 3.4 to 3.7 total servings/day) [127].
The evidence regarding the prevention of RA with a high intake of vegetables and fruit is judged as possible due to the low number of studies.
Chronic obstructive pulmonary disease
The pooled prevalence for chronic obstructive pulmonary disease (COPD) for 28 countries has been reported to be 7.6 %, and for adults aged ≥40 years, the prevalence is 9 %-10 % [128]. The disease is associated with narrowing (obstruction) of the airways, which causes typical breathing sounds such as whistling or wheezing. According to estimates of the WHO, by the year 2020, COPD will be the third most common cause of death worldwide. The diagnosis of COPD is confirmed by a test that measures the forced expiratory volume in 1 s (FEV1), which is the greatest volume of air that can be breathed out in the first second of a large breath. A high FEV1 value indicates normal pulmonary function. Smoking is the most important risk factor of COPD.
A total of 22 studies were analysed. Four of the studies were prospective cohort studies [129–132] and 2 were case–control studies [133, 134], while the majority were cross-sectional studies [135–150]. In the prospective cohort studies by Miedema et al. [129], the consumption of fruit was inversely associated with the risk of COPD (RR 0.68; <14 g/day vs. >70 g/day). In the prospective study by Walda et al. [130], an increase in fruit consumption by 100 g/day was associated with a reduction in the COPD risk by 24 %. In both studies, no association was found between the risk of COPD and vegetable intake. In the HPFS and the NHS, Varraso et al. [131, 132] investigated dietary patterns and observed a risk of COPD lowered by up to 50 % with a diet high in fruit, vegetables, and fish. The case–control study by Hirayama et al. [134] determined a significantly lower intake of vegetables and fruit in COPD patients than in control persons. There was a primary inverse correlation between the prevalence of COPD and the quantity of vegetable intake. In the second case–control study in smokers, high consumption of vegetables (≥93 g/day) and fruit (≥121 g/day) was associated with a COPD risk reduction by 54 % each. High intake of apples (≥3 apples/week) resulted in a reduction in the COPD risk by 53 % [133].
Most of the cross-sectional studies also show a significant positive association between the quantity of fruit intake and the FEV1 or reduced occurrence of obstruction, respectively [135–138, 140–144, 146, 147, 149, 150]. Only 3 studies indicate a risk reduction due to high consumption of vegetables [144, 145, 148]. In one study, for both the intake of flavonoids and the consumption of apples and pears, a significant positive association with the FEV1 value was found [141, 143]. The intake of dietary fibre from fruit was also associated with a reduced risk of COPD [151, 152]. As only a few cohort studies exist and there are mainly cross-sectional studies, the evidence regarding the association between high intake of vegetables and fruit and reduced risk of COPD is currently judged as possible.
Asthma
Asthma is one of the most common chronic diseases and occurs in 5–10 % of the population in Western countries [153]. In addition to genetic factors, environmental factors including nutrition are primarily responsible for the increase in the prevalence of asthma in recent decades [154]. Asthma is often accompanied by increased sensitivity to allergies. Various nutritional factors (like oily fish, unsaturated fatty acids, vitamins, and micronutrients) probably influence the risk of asthma [155, 156].
For judging the evidence regarding the association between risk of asthma and consumption of vegetables and fruit, a total of 20 studies were identified (adults and children at the age of ≥4 years), 10 of which were cross-sectional studies [157–166], 4 were case–control studies [167–170], 4 were cohort studies [138, 171–173], and 1 was an intervention study [174]. All studies except of those by Huang et al. [158], Garcia et al. [168], and Lewis et al. [162] showed an inverse association between the incidence of asthma and the intake of fruit or of vegetables and fruit, respectively. This association is particularly obvious for apples [160, 161, 167, 171]. In the cohort study by Willers et al. [172], apples also were identified as food that is associated with a reduced risk of asthma. A high consumption of apples in pregnant women was accompanied by a lower risk of asthma in the children within the first 5 years after birth. In another cross-sectional study, the consumption of apple juice, but not of fresh apples was inversely associated with the risk of asthma [175].
In an intervention study with asthma patients, a control diet restricted in the intake of vegetables and fruit enhanced the asthma symptoms, while the supplementation of tomato juice improved the symptoms [174].
Only in one cohort study [171] and one cross-sectional study [161], the consumption of vegetables alone was inversely associated with the risk of asthma. Preliminary results suggest that genetic polymorphisms (mutations in the catalase gene) exert an additional influence on the association between the risk of asthma and protective effects of high vegetable and fruit intake [176].
The available data are mainly based on cross-sectional studies and show consistently that a high fruit and vegetable intake lowers the risk of asthma. Therefore, there is possible evidence regarding a protective effect of the consumption of this food group. In this respect, the consumption of fruit seems to be more important than the consumption of vegetables.
Osteoporosis
Osteoporosis is defined as a skeletal disorder characterised by compromised bone strength predisposing to an increased risk of fracture [177]. Worldwide, an osteoporotic fracture is estimated to occur every 3 s, a vertebral fracture every 22 s [178]. In Europe, estimated 179,000 men and 611,000 women will suffer a hip fracture each year [179], and the lifetime risk of an osteoporotic fracture is up to 53 % in women and up to 22 % in men [180]. Overall, 61 % of osteoporotic fractures occur in women, with a female-to-male ratio of 1.6. Sex-specific fracture rates vary with fracture site: 58, 70, 75, 80 % of spine, hip, humerus, and forearm fractures, respectively, occur in women [178]. Although more women then men are affected, the disease burden in men is considerable: approximately one-third of hip fractures occur in men [181], and their mortality is higher than in women, with about 37.5 % dying within the first 12 months as compared to 28.2 % of the affected women [182, 183].
The after-effects of osteoporotic fractures are severe and include reduced mobility, chronic pain, loss of independence, need for permanent care, and death. In Europe, disability due to osteoporosis is greater than that caused by cancers [178].
Cost estimates for all osteoporotic fractures in Europe amount to €25 billion [179]. Due to the expected demographic changes in Europe, direct health care costs associated with osteoporotic fractures are expected to rise up to €76.8 billion in the year 2050 [184].
In addition to age and sex, established lifestyle-related risk factors of osteoporosis comprise reduced physical activity [185, 186] and the amount of calcium and vitamin D intake [187]. Body mass or body composition parameters, respectively, are putative risk factors [188, 189]. Other nutrition-related risk factors currently under scientific evaluation include the intake of animal and plant proteins, table salt, phytoestrogens, foods like soya or prunes, other vitamins, minerals and phytochemicals as well as the acid–base-balance and the consumption of vegetables and fruit [190–195]. As a potential biological explanation for the effect of vegetables and fruit on bone health, their influence on the acid–base-balance is considered. The latter exhibits putative interactions with bone metabolism [196–199].
Studies assessing the influence of vegetable and fruit consumption on bone health and osteoporosis cover a broad spectrum of topics, since different endpoints are considered. In addition to the clinical diagnosis of osteoporosis or an osteoporotic fracture (direct evidence regarding the effect of vegetable and fruit intake on osteoporosis), changes in bone density and various parameters of bone metabolism (indirect evidence regarding the effect of vegetable and fruit intake on osteoporosis) are investigated.
Firstly, for this review, the available direct evidence was searched for. One systematic review and 4 additional prospective studies were identified that investigated the association between vegetable and fruit consumption and the occurrence of osteoporosis or an osteoporotic fracture. The systematic review included studies that have investigated the influence of vegetables and fruit consumption on bone health in women ≥45 years of age [200]. Observational and experimental studies on the incidence of osteoporotic fractures, on bone density, and on parameters of bone metabolism were taken into account. Four of the 8 studies that were analysed in detail revealed a high risk of bias. The other 4 studies provided no consistently significant indications on a protective effect of vegetables and fruit. The cross-sectional studies showed positive associations between the consumption of vegetables and fruit and bone density in various locations. However, no significant effects were shown by either cohort or intervention studies. Due to the low number of available studies on fracture risk, no separate conclusions regarding this topic were drawn by this review.
In the WHI Dietary Modification Trial (see “Obesity”), a slightly reduced risk of falling and a slight decrease in bone density, but no influence on the risk of osteoporotic fractures, were seen in the intervention group after 8 years of follow-up [201]. However, due to the complex intervention in that study, the observed effect is not solely attributable to the consumption of vegetables and fruit.
Based on data from 5 European countries of the EPIC study, the incidence of femoral neck fractures was determined over the period of 8 years and examined with respect to associations with the consumption of certain food groups [202]. Among the 18,545 women and 10,538 men aged 60 years and older, 275 femoral neck fractures occurred during follow-up. In multivariate adjusted regression models, no significant association was observed for any of the investigated food groups, including vegetables and fruit. Marginally significant protective effects were shown regarding the consumption of vegetables (HR 0.93; 95 % CI 0.85–1.01).
A Japanese cohort study investigated the association between dietary patterns and fall-related fractures in a group of 877 persons at the age of >70 years. Three dietary patterns were determined. Of these, the “meat pattern” was associated with a lowered risk of fracture and the “vegetable pattern” with an increased risk of fracture [203].
In addition to these studies on direct evidence, selected results of studies on indirect evidence are presented in the following.
In a systematic review, Papaioannou et al. [204] searched for risk factors of low bone mineral density (BMD) in men aged ≥50 years. Neither vegetable nor fruit consumption were found to be risk factors. In a randomised clinical trial regarding the effect of citrate supplementation on parameters of bone metabolism (bone turnover markers) and BMD, the effect of an increase in the consumption of vegetables and fruit by 300 g/day was investigated as additional treatment group. No significant influence on the investigated bone parameters was shown. However, the degree of compliance in that study could not be determined [205]. Using retrospective analyses of data of the Canadian Multicenter Osteoporosis Study, the associations between dietary patterns and the occurrence of fractures were investigated [206]. 3,539 women and 1,649 men aged ≥50 years were followed for 10 years with respect to incident fractures. The analysis revealed 2 dietary patterns that were associated with the occurrence of fractures: the pattern “nutrient dense”, characterised by a high consumption of vegetables and fruit, was associated with a reduced fracture risk in women. In men, a similar effect was observed that did not reach statistical significance. Other indirect evidence is derived from a randomised study that investigated the effect of the DASH diet, which includes a high vegetable and fruit intake ([63]; see “Hypertension”), on various markers of bone and calcium metabolism. Compared to the control diet, the DASH diet achieved a significant reduction in bone remodelling [207] in the 186 study participants (age 23–76 years). However, due to the complex dietary intervention, it is not possible to determine which of the changed nutritional factors are responsible for the observed effects. Kaptoge et al. [208] did not find a significant association between the consumption of vegetables and/or fruit and the rate of bone density decreases over a period of 3 years. The study, conducted in England, included 470 men and women between the age of 69 and 79 years. Analyses of the Framingham Osteoporosis Study showed that in men (aged 69–97 years), but not in women, a significantly lower decrease in bone density was observed with high consumption of vegetables and fruit over a period of 4 years [209]. Similar results were found using prospective analyses of the Framingham Heart Study. Again, a protective effect of high vegetable and fruit consumption was only found in men (aged 69–97 years) [210].
Another aspect investigated is the potential effect of vegetables and fruit consumption during childhood. A prospective study showed that the consumption of vegetables and fruit in compliance with recommendations was an independent predictor of the bone mineral content in boys, but not in girls [211]. A further prospective study found a significantly higher bone mass in children with a high consumption of dark-green and deep-yellow vegetables [212]. DeBar et al. [213] conducted a randomised study over 2 years, in which 228 adolescent girls (in the age between 14 and 16 years) were asked to increase their physical activity and to improve their diet, including an increased consumption of vegetables and fruit. Compared with the control group, the girls in the intervention group had a significantly higher bone density at the spine and the femoral neck. However, due to the complex intervention, the observed effect cannot be attributed to the consumption of vegetables and fruit only.
Another interesting aspect considered in various studies is the maternal dietary influence before and during pregnancy on parameters of bone health in children. For example, dietary patterns during pregnancy were associated with the bone density and bone mineral content of the children at the age of 9 years. This long-term study showed that a maternal diet with a high proportion of vegetables, fruit, and whole-grain products was associated with significantly higher levels of bone density and bone mineral content in the offspring [214]. Another study from India showed that a maternal diet with foods rich in calcium, including green leafy vegetables and fruit, was associated with higher bone density and higher bone mineral content in children [215].
In summary, many studies showed a positive association between the quantity of vegetable and/or fruit consumption and markers of bone health, or such an association was derived from the results of these studies. When solely those studies on direct evidence and studies with higher levels of evidence are taken into account, that is only prospective studies with the endpoints “osteoporosis” or “osteoporotic fracture”, there are currently only few studies available. Furthermore, these studies show inconsistent results. Therefore, the evidence regarding the prevention of osteoporosis due to a higher consumption of vegetables and fruit is judged as possible.
A similar judgement was reached by British experts based on a comprehensive literature review. It was concluded that a protective effect of a high intake of vegetables and fruit on bone health is to be regarded as possible, but the cause of this effect could not be determined [216].
Eye diseases
Based on WHO data [217], it is assumed that more than 28 million subjects in Europe are visually impaired, with a prevalence for blindness of 0.3 %. The main causes for loss of sight in Europe and the United States are age-related macular degeneration (AMD; 50 %), glaucoma (18 %), diabetic retinopathy (17 %), and cataract (5 %) [218]. Despite worldwide trends for reduced prevalence of visual impairment and blindness since the 1990s [219], the prevalence of eye diseases in the ageing population is expected to increase in Western countries, for example, Germany, within the next 20 years [220]. The prevalence is reported to be 3.5–40 % depending on age for AMD, 3.3–14 % for glaucoma, and 4.4–20.9 % for diabetic retinopathy [221]. The prevalence for cataract increases with age and is over 40 % in subjects older than 75 years [222–224].
Macular degeneration is an age-related degenerative retinal disease that leads to the loss of central vision [225]. Risk factors for the development of AMD include age, smoking, and nutrition [226–228]. Important protective factors are dietary fibre [229], mono-unsaturated fatty acids [230], certain vitamins [231–233], and especially carotenoids like lutein and zeaxanthin. These carotenoids selectively accumulate in the macula lutea (point of high-resolution vision) and protect the pigment epithelial cells from blue light and damage by short-wave rays [234].
The dietary intake of carotenoids, the serum levels, and the supplementation of these carotenoids are associated with a risk reduction for AMD in most of the studies [235–244]. While protective effects of a high lutein/zeaxanthin intake were observed, one study showed an increased risk of AMD at high β-carotene intake [244].
In an analysis of the NHS [245, 246] and in the prospective Rotterdam Study [247], the intake of lutein/zeaxanthin and other carotenoids was not associated with the risk of AMD. The results of the CHARM Study (Cardiovascular Health and Age-Related Maculopathy) indicate that at already existing AMD, high lutein/zeaxanthin intake can promote AMD progression [248].
Although lutein/zeaxanthin intake was calculated directly from food intake in the mentioned studies, hardly any studies have been published that have investigated the association between vegetable and fruit consumption and risk of AMD. In a prospective cohort study, the consumption of fruit, but not of vegetables, was associated with a risk reduction by 36 % [249]. In women younger than 75 years, the risk of AMD was reduced by 52 % at higher intake of vegetables (4 vs. 0.9 portions per day) [250]. High intake (>5 times/week) of foods rich in lutein, like spinach and collard greens, was associated with a reduction in the AMD risk by 86 % in a case–control study [251]. According to Goldberg et al. [252], the intake (>7 times/week) of vegetables and fruit rich in provitamin A was associated with a reduction in the AMD risk by 33 % in a cross-sectional study.
Cataract is a clouding of the lens in adults, which results in impaired vision or visual acuity [253]. The risk is influenced by age, ethnic origin, gender, smoking, sunlight, consumption of alcohol, diabetes mellitus, corticosteroid medication, and nutritional factors [254]. The data on the influence of vitamin C and carotenoids on risk of cataract are inconsistent [255–259]. The more recent results of the prospective Blue Mountains Eye Study [260] suggest that high intake of vitamin C, especially from fruit juices, is associated with a significantly reduced risk of cataract. The combined intake of vitamin C and other antioxidants (β-carotene, vitamin E, zinc) from foods and/or supplements was also associated with a reduction in the cataract risk by 38–49 %.
In 4 prospective cohort studies, the influence of vegetable and fruit consumption on risk of cataract was investigated. A diet according to the Dietary Guidelines for Americans 2000 is associated with a cataract risk reduction by more than 50 % [261]. In this subpopulation of the NHS, eating habits and cataract were investigated in 479 women between the age of 52 and 73 years. In the group with the highest fruit consumption (3.9 portions/day), the prevalence of cataract was 42 % lower than in the control group (1.3 portions/day). In the HPFS, high consumption of broccoli and spinach in men was associated with a reduction in the cataract risk by 23 and 27 % [262]. In participants of the Women’s Health Study, a high intake of vegetables and fruit was associated with a significant reduction in the cataract risk by 10–15 % [263]. In the updated analysis of the same study [264], the risk reduction (10 %) at high intake of vegetables and fruit was not significant any more (changed database and analysis). In contrast, in the highest quintile of both lutein/zeaxanthin and vitamin E intake, the risk of cataract was 18 % and 14 % lower than in the lowest quintile of intake. In the Carotenoids in the Age-Related Eye Disease Study (CAREDS), the risk was reduced by 26 % at high vegetable intake [265]. Comparing highest with lowest quintiles, the risk of cataract was reduced by 32 % regarding both the calculated daily intake of lutein and zeaxanthin and the measured plasma concentrations of lutein and zeaxanthin. These findings are confirmed by results of the prospective POLA Study (Pathologies Oculaires Liées à l’Age) [242]. In the group with the highest plasma concentration of zeaxanthin (≥0.09 μM), the risk of cataract was reduced by 43 % compared with the control group (<0.04 μM).
Glaucoma is caused by changes in the intraocular pressure that can damage the optic nerve and may progress to complete blindness [266]. There are hardly any data on the influence of lifestyle factors on the risk of glaucoma. Regarding nutritional factors, so far mainly the role of vitamins has been investigated [267, 268]. Only one study described the association between vegetable and fruit intake and the risk of glaucoma [269]. In this cross-sectional investigation, a lowered risk was observed at high intake of certain kinds of vegetables and fruit, for example fresh carrots (−64 %).
Diabetic retinopathy is a microvascular complication of diabetes mellitus that is characterised by damage of the retina. Since it is a secondary disease of diabetes mellitus, there is a direct causal relation with the underlying primary disease [270, 271]. Currently, there are no studies available regarding the influence of the consumption of vegetables and fruit on the risk of diabetic retinopathy. Only in a small cross-sectional study from the Melbourne Collaborative Cohort Study, the association between the plasma concentration of carotenoids and the prevalence of diabetic retinopathy was investigated in 111 participants [272]. Type 2 diabetes patients with a diagnosis of diabetic retinopathy showed lower plasma concentrations of non-provitamin A carotenoids (lutein, zeaxanthin and lycopene) than patients without retinopathy.
Due to the low number of published studies, the evidence regarding the prevention of macular degeneration and cataract through higher consumption of vegetables and fruit is judged as possible. The evidence regarding the risk of glaucoma and diabetic retinopathy is insufficient due to the lack of data.
Dementia
Dementia is a clinical syndrome that is characterised by a decrease in intelligence, memory, and perception and may be caused by various diseases. Logical and critical thinking, judgement, retentive memory, and short-term memory are impaired, while remote memory (long-term memory) can remain for a long time. In addition, personality may deteriorate [273].
According to the latest Report of the European College of Neuropsychopharmacology and the European Brain Council, 6.34 million people in Europe aged at least 60 years were estimated to suffer from dementia in 2011, corresponding to a mean prevalence of 5.4 % in this population. The prevalence is age-dependent (1–30 %) and increases with advanced age [274]. Due to increasing life expectancy in industrialised countries and the exponential increase in dementia in old age, the prevalence of dementia in these countries will be rising steadily. At global level, with an incidence of 4.6 million per year, an increasing prevalence of dementia with 42 million cases in 2020 has also to be expected [275]. Thus, dementia has become one of the major challenges to public health [276].
Worldwide, Alzheimer’s disease and vascular dementia are the two most common subtypes of dementia, which account for 50–70 and 15–25 % of all dementia cases, respectively [276]. Old age and genetic susceptibility are well established risk factors for dementia and Alzheimers’s disease. Vascular risk factors (e.g. diabetes mellitus, hypertension, and smoking) as well as cardio- and cerebrovascular diseases may contribute to the development and progression of dementia, whereas social, physical, and mental activities may delay their onset [276]. Overweight increases the risk of dementia independent of comorbidities [277].
So far, only a few studies have investigated whether the consumption of vegetables and fruit is associated with the risk of dementia. In addition to dementia, the cognitive performance has also been used as target parameter by using certain tests that are sensitive enough to diagnose dementia (both vascular and Alzheimer‘s dementia) at an early stage [278].
Cross-sectional studies in Spain [279] and Korea [280] have shown that elderly people with good cognitive performance consumed more fruit and vegetables than elderly people with impaired or poor cognitive performance. For the Korean participants, these differences regarding vegetable and fruit consumption were only detected in women; in men, they were only found regarding fruit intake, but not regarding vegetable consumption [280]. Vegetable consumption, however, was comparable in both study populations (Korea: 248 g/day vs. Spain: 239 g/day). In an Indonesian cross-sectional study, the consumption of fruit (including fruit juices), but not of orange/red and green vegetables, was significantly associated with improved short- and long-term memory in elderly people [281].
A cohort study including 3,718 participants of the Chicago Health and Aging Project (mean age at baseline 74 years) investigated the relation between the consumption of vegetables and fruit and the decrease in the cognitive performance (6 years follow-up) [282]. Cognitive performance was quantified using various screening methods. If vegetable and fruit intake was analysed in total, there was not any association between the number of consumed portions and cognitive deficits, while an inverse association was found for the consumption of vegetables alone, but not for the consumption of fruit. Two further cohort studies showed similar results. The cohort study by Kang et al. [283] investigated the decline in cognitive performance in a subgroup of the NHS (age at baseline: 30–55 years, follow-up: 19–25 years). Vegetable and fruit consumption including fruit juices were recorded. The decline in cognitive performance was inversely associated with vegetable consumption, but not with the intake of fruit or fruit juices. In a Dutch cohort (n = 2,613, age at baseline: 43–70 years, follow-up: 10 years), an inverse association was also found only between vegetable consumption and cognitive performance, but not regarding fruit and juices [284]. In contrast to the study by Nooyens et al. [284], the studies by Morris et al. and Kang et al. [282, 283] showed an association between the consumption of green leafy vegetables and a reduced risk, but not for other types of vegetables (yellow vegetables and cruciferous vegetables). Nooyens et al. [284] detected an inverse association between the consumption of root vegetables (carrots, beetroot) and the decrease in cognitive performance. While the results of cross-sectional studies show a protective effect of both fruit and vegetables for maintaining the cognitive performance [279–281], the results of cohort studies suggest only a protective effect regarding vegetables.
To date, 3 cohort studies with dementia or Alzheimer’s dementia as target parameter have been performed [285–287]; a fourth cohort study [288] also included cognitive impairment in addition to dementia. Dai et al. [285] determined the intake of vegetable and fruit juices in 1,836 Japanese immigrants (mean age, 71 years) between 1992 and 1994 in relation to the incidence of Alzheimer’ dementia in 2001. The risk of disease decreased with increasing consumption, independent of the intake of vitamin C, E, and β-carotene [285]. Barberger-Gateau et al. [286] investigated the frequency of vegetables and fruit consumption in 8,085 subjects (aged ≥65 years) in Bordeaux, Dijon, and Montpellier (France). After 3.6 years follow-up, the frequency of vegetable and fruit consumption reduced the risk of dementia, including the risk of Alzheimer’s dementia. Daily consumption compared with rare consumption was associated with a risk reduction by about 30 %. Similar results were found in the study of Hughes et al. [287], which investigated only 3,779 individuals within the Swedish Twins (HARMONY) Study (mean age at baseline: 48 years), but had a follow-up of 30 years. In this study, the medium or high intake of fruit and vegetables was associated with a decreased risk of dementia and Alzheimer’s dementia compared with low or no consumption of fruit and vegetables. However, this difference was only significant in fully adjusted models. Compared with the consumption of more than 2 portions of vegetables and fruit per day, the consumption of <2 portions was associated with a significantly higher risk of dementia including cognitive impairment in the cohort of the Esprit Study (age at baseline: ≥65 years, median follow-up: 7 years) [288], taking into account age and gender.
In summary, the studies on cognitive performance and risk of dementia suggest an inverse relation to the consumption of vegetables and fruit. Due to the limited number of studies, possible evidence exists for a reduced risk of dementia with increasing consumption of vegetables and fruit. In this respect, the consumption of vegetables seems to be more important than the consumption of fruit.
Summary of the evidence judgement
The current evaluation of the association between the consumption of vegetables and fruit and the risk of certain diseases resulted in all grades of the strength of evidence.
For hypertension, CHD, and stroke, there is convincing evidence that increasing consumption of vegetables and fruit reduces the risk of disease. The setting of the strength of evidence for hypertension as convincing is particularly important, because hypertension is widespread and is considered as a risk factor of CHD and stroke. There is probable evidence that the overall risk of cancer is inversely associated with the consumption of vegetables and fruit. The evidence was not individually judged for the different sites of cancer, as this would go beyond the scope of this review due to the various aetiologies. Data on dementia indicate possible evidence for a risk-reducing influence of increased vegetable and fruit consumption. In addition, there is possible evidence that a diet with increased consumption of vegetables and fruit may prevent body weight gain. As overweight is the most important risk factor for type 2 diabetes mellitus, an increased consumption of vegetables and fruit might indirectly reduce the incidence of type 2 diabetes mellitus. However, there is probable evidence that there is no influence of increased consumption of vegetables and fruit on the risk of type 2 diabetes mellitus that is independent of overweight.
Furthermore, the present data indicate that an increased consumption of vegetables and fruit also reduces the risk of certain eye diseases, RA, and osteoporosis. Likewise, the present data indicate that an increase in vegetable and fruit consumption may contribute to the prevention of the lung diseases asthma and COPD. Because of the chosen evidence criteria and the lack of studies with level of evidence I and II, the evidence regarding the association between increased vegetable and fruit consumption and reduced risk of these diseases is only judged as possible. For chronic IBDs, glaucoma, and diabetic retinopathy, evidence is insufficient. Table 3 summarises the evidence judgement regarding the influence of vegetable and fruit consumption on the risk of certain chronic diseases.
Discussion
The present review shows a considerable preventive potential of an increase in consumption of vegetables and fruit by the general public in respect to a number of diseases. The chain of evidence according to the criteria of a risk-reducing effect with convincing evidence is well reflected in the available data on hypertension, CHD, and stroke. In contrast to these diseases, the risk-reducing effect of consumption of vegetables and fruit for cancer is assessed to be much smaller than in earlier evaluations (e.g. [94, 97]) taking the present review and the current literature [102, 289]. It should be noted that the strength of evidence neither indicates the degree of risk reduction nor the intake quantity that is necessary to achieve the risk-reducing effect. Such information cannot be derived from the presented data and is not subject of this review.
The scientific basis of the “5 a day” campaign, which has been greatly promoted in recent years in Europe and nationwide, is strongly supported by the prevention potential demonstrated here. There seems to be a broader basis for disease prevention than assumed at the beginning of the campaign. At the establishment of the Private Public Partnership at the beginning of the 1990s between science—with the National Cancer Institute of the USA as leading institution—and the food industry, the focus was primarily on cancer. Nowadays, the recommendation to increase the consumption of vegetables and fruit is mainly based upon the convincing data regarding hypertension, CHD, and stroke and the potential for many other diseases.
However, not only the “5 a day” campaign profited from the progress in the available data, but also the scientific societies focusing on other diseases besides cancer. For example, the European Society of Cardiology promotes the intake of vegetables and fruit in its guidelines about prevention [290].
The changed data situation on the association between the intake of vegetables and fruit and the risk of cancer is of great scientific interest. In the systematic review by Block et al. [93], case–control studies were predominant, and 128 of the 156 studies available at that time showed an inverse risk relation. Unlike case–control studies, prospective cohort studies do not record the consumption of vegetables and fruit retrospectively after the disease has occurred, but at the time of study entry without already existing disease; studies like these were predominantly published after the year 2000 and showed inconsistent results. They also showed a much lower risk association than the case–control studies [97]. This led to the assumption that there was a considerable systematic bias regarding the retrospective documentation of food intake in the case–control studies. But perhaps, the methodological problems of the study design are not the only possible explanation for the change in the data situation in the recent decade. The change in the data situation might also be due to alterations in lifestyle in recent decades, which, on the one hand, resulted in an improved supply with essential nutrients and, on the other hand, led to a decrease in carcinogenic or tumour growth-promoting factors. It has to be considered that the difference in age in the case–control studies compared with the cohort studies may be much larger than the 10 years mentioned above in which the change in the strength of evidence occurred, as most of the participants in case–control studies are older diseased subjects, while there are mainly younger healthy individuals in cohort studies. The current analysis of the EPIC Study on the impact of consumption of vegetables and fruit on the prevention of cancer indicates that the largest reduction in risk was observed in cancer sites that are promoted by smoking [106]. Obviously, a lifestyle that is associated with higher exposure to carcinogens may allow a stronger cancer preventive effect of vegetables and fruit than a lifestyle with lower exposure to carcinogens. This might be an additional explanation for the observed small risk reduction in the more recent prospective studies.
Changes in lifestyle have resulted in a massive increase in the prevalence of obesity in Western countries. Obesity-related cancer-promoting mechanisms include chronic inflammation, insulin resistance, impaired glucose tolerance, and altered hormone metabolism [291, 292]. Vegetable and fruit intake has proven to influence these processes. For example, an increased consumption of vegetables and fruit can counteract chronic subclinical inflammatory processes involved in cancer and obesity [293]. Greater botanical variety in vegetable and fruit intake is associated with less inflammation [294].
It has been shown that the consumption of vegetables and fruit from certain botanical families exerts special protective effects against various cancers (like lung cancer), which do not become obvious if all kinds of vegetable and fruit are analysed together [295]. Similar observations were made for specific subtypes of cancer. Vegetable and fruit consumption showed a protective effect only against certain types of lung cancer (squamous cell carcinoma), but not against other histological types of lung cancer [296, 297]. Therefore, the overall analysis of all vegetable and fruit kinds and all cancers can result in a serious loss of information.
As vegetables and fruit and the phytochemicals therein particularly influence not only inflammatory processes, but also cellular redox processes as well as endothelial and metabolic processes [83–88], which are involved in the pathogenesis of various diseases, we assume that these mechanisms are primarily responsible for the risk-reducing effect of vegetable and fruit consumption regarding the single diseases. This also applies to diseases with limited data so far, for which the strength of evidence grade “possible” was assigned.
Therefore, it seems to be reasonable to perform intervention studies that specifically contribute to the elucidation of these mechanisms. As it is often not possible to implement well-controlled long-term dietary changes in a randomised study design, at first, intervention studies should be designed as short-term studies with the investigation into appropriate surrogate markers of hard endpoints. These intervention studies should use the full range of available vegetables and fruit as much as possible. Furthermore, it is necessary to systematically continue the data analyses in the present cohort studies regarding the associations between vegetable and fruit consumption and the risk of various diseases. There also seems to be the need to critically review the data on the assessment of the consumption of vegetables and fruit and to improve the methods if possible [298]. The results from prospective cohort studies together with those from intervention studies on the mechanisms of action will provide a sound basis for future evaluations of the preventive potential of vegetable and fruit consumption regarding various chronic diseases using an evidence-based approach.
Notes
Overweight: BMI ≥ 25.0; pre-obesity: BMI 25–29.9; obesity: BMI ≥ 30.0 (according to [10]).
Overweight: >90th percentile of the BMI (according to [11]).
Obesity: >97th percentile of the BMI (according to [11]).
Normal weight: BMI between the 10th and 90th BMI-percentile (according to [11]).
The DASH (Dietary Approaches to Stop Hypertension) diet consists of a high proportion of vegetables and fruit, low-fat dairy products and cereal products high in dietary fibre, combined with a low-fat proportion (<30 energy %).
References
DGE (Deutsche Gesellschaft für Ernährung e. V.; ed.) (2007) Obst und Gemüse in der Prävention chronischer Krankheiten. Bonn. www.dge.de/pdf/ws/Stellungnahme-OuG-Praevention-chronischer-Krankheiten-2007-09-29.pdf
WHO (World Health Organization) (2003) Diet, nutrition and the prevention of chronic diseases. WHO technical report series 916:55
DGE (Deutsche Gesellschaft für Ernährung e. V.; ed.) (2011) Evidenzbasierte Leitlinie: Kohlenhydratzufuhr und Prävention ausgewählter ernährungsmitbedingter Krankheiten. Bonn. www.dge.de/leitlinie
Elmadfa I (ed) (2009) European nutrition and health report 2009. Karger, Basel, p 5
Agudo A, Slimani N, Ocké MC et al (2002) Consumption of vegetables, fruit and other plant foods in the European prospective investigation into cancer and nutrition (EPIC) cohorts from 10 European countries. Public Health Nutr 5:1179–1196
Hall JN, Moore S, Harper SB, Lynch JW (2009) Global variability in fruit and vegetable consumption. Am J Prev Med 36:402–409
von Ruesten A, Steffen A, Floegel A et al (2011) Trend in obesity in European adult cohort populations during follow-up since 1996 and their predictions to 2015. PLoS One 6:e27455
Helmert U, Strube H (2004) Trends in the development and prevalence of obesity in Germany between 1985 and 2002. Gesundheitswesen 66:409–415
Prentice AM, Jebb SA (2003) Fast foods, energy density and obesity: a possible mechanistic link. Obes Rev 4:187–194
WHO (World Health Organization) (2000) Obesity: preventing and managing the global epidemic. WHO technical report series 894
Kromeyer-Hauschild K, Wabitsch M, Kunze D et al (2001) Perzentile für den body-mass-index für das Kindes—und Jugendalter unter Heranziehen verschiedener deutscher Stichproben. Monatsschr Kinderheilkd 249:807–818
Alinia S, Hels O, Tetens I (2009) The potential association between fruit intake and body weight—a review. Obes Rev 10:639–647
Kahn HS, Tatham LM, Rodriguez C et al (1997) Stable behaviors associated with adults’ 10-year change in body mass index and likelihood of gain at the waist. Am J Public Health 87:747–754
Newby PK, Muller D, Hallfrisch J et al (2003) Dietary patterns and changes in body mass index and waist circumference in adults. Am J Clin Nutr 77:1417–1425
Savage JS, Marini M, Birch LL (2008) Dietary energy density predicts women’s weight change over 6 y. Am J Clin Nutr 88:677–684
Buijsse B, Feskens EJ, Schulze MB et al (2009) Fruit and vegetable intakes and subsequent changes in body weight in European populations: results from the project on diet, obesity, and genes (DiOGenes). Am J Clin Nutr 90:202–209
Parker DR, Gonzalez S, Derby CA et al (1997) Dietary factors in relation to weight change among men and women from two south-eastern New England communities. Int J Obes Relat Metab Disord 21:103–109
Quatromoni PA, Copenhafer DL, D’ Agostino RB, Millen BE (2002) Dietary patterns predict the development of overweight in women. The Framingham Nutrition Study. J Am Diet Assoc 102:1239–1246
Togo P, Osler M, Sorensen TI, Heitmann BL (2004) A longitudinal study of food intake patterns and obesity in adult Danish men and women. Int J Obes Relat Metab Disord 28:583–593
Fogelholm M, Kujala U, Kaprio J, Sarna S (2000) Predictors of weight change in middle-aged and old men. Obes Res 8:367–373
Newby PK, Peterson KE, Berkey CS et al (2003) Dietary composition and weight change among low-income preschool children. Arch Pediatr Adolesc Med 157:759–764
Plachta-Danielzik S, Landsberg B, Johannsen M et al (2010) Determinants of the prevalence and incidence of overweight in children and adolescents. Public Health Nutr 13:1870–1881
Wang Y, Ge K, Popkin BM (2003) Why do some overweight children remain overweight, whereas others do not? Public Health Nutr 6:549–558
Field AE, Gillman MW, Rockett HR, Colditz GA (2003) Association between fruit and vegetable intake and change in body mass index among a large sample of children and adolescents in the United States. Int J Obes 27:821–826
Danielzik S, Czerwinski-Mast M, Langnäse K et al (2004) Parental overweight, socioeconomic status and high birth weight are the major determinants of overweight and obesity in 5–7 y-old children: baseline data of the Kiel Obesity Prevention Study (KOPS). Int J Obes Relat Metab Disord 28:1494–1502
Faith MS, Dennison BA, Edmunds LS, Stratton HH (2006) Fruit juice intake predicts increased adiposity gain in children from low-income families: weight status-by-environment interaction. Pediatrics 118:2066–2075
Rolls BJ, Ello-Martin JA, Tohill BC (2004) What can intervention studies tell us about the relationship between fruit and vegetable consumption and weight management? Nutr Rev 62:1–17
Ledikwe JH, Blanck HM, Kettel Khan L et al (2006) Dietary energy density is associated with energy intake and weight status in US adults. Am J Clin Nutr 84:1362–1368
Ello-Martin JA, Roe LS, Ledikwe JH et al (2007) Dietary energy density in the treatment of obesity: a year-long trial comparing 2 weight-loss diets. Am J Clin Nutr 85:1464–1477
Saquib N, Rock CL, Natarajan L et al (2009) Does a healthy diet help weight management among overweight and obese people? Health Educ Behav 36:518–531
Howard BV, Manson JE, Stefanick ML et al (2006) Low-fat dietary pattern and weight change over 7 years: the women’s health initiative dietary modification trial. JAMA 295:39–49
Thefeld W (1999) Prävalenz des diabetes mellitus in der erwachsenen Bevölkerung Deutschlands. Gesundheitswesen 61:S85–S89
Rathmann W, Haastert B, Icks A et al (2003) High prevalence of undiagnosed diabetes mellitus in Southern Germany: target populations for efficient screening. The KORA survey 2000. Diabetologia 46:182–189
Giani G, Janka HU, Hauner H et al (2004) Epidemiologie und Verlauf des diabetes mellitus in Deutschland. In: Scherbaum WA, Kiess W (eds) Evidenzbasierte Leitlinie der Deutschen Diabetes-Gesellschaft (DDG). www.deutsche-diabetes-gesellschaft.de/leitlinien/EBL_Epidemiologie_Update_2004.pdf
Schulze MB, Hu FB (2005) Primary prevention of diabetes: what can be done and how much can be prevented? Annu Rev Public Health 26:445–467
Hamer M, Chida Y (2007) Intake of fruit, vegetables, and antioxidants and risk of type 2 diabetes: systematic review and meta-analysis. J Hypertens 25:2361–2369
Carter P, Gray LJ, Troughton J et al (2010) Fruit and vegetable intake and incidence of type 2 diabetes mellitus: systematic review and meta-analysis. BMJ 341:c4229
Lundgren H, Bengtsson C, Blohme G et al (1989) Dietary habits and incidence of noninsulin-dependent diabetes mellitus in a population study of women in Gothenburg, Sweden. Am J Clin Nutr 49:708–712
Feskens EJ, Bowles CH, Kromhout D (1991) Carbohydrate intake and body mass index in relation to the risk of glucose intolerance in an elderly population. Am J Clin Nutr 54:136–140
Harding AH, Wareham NJ, Bingham SA et al (2008) Plasma vitamin C level, fruit and vegetable consumption, and the risk of new-onset type 2 diabetes mellitus: the European prospective investigation of cancer—Norfolk prospective study. Arch Intern Med 168:1493–1499
Schulze MB, Schulz M, Heidemann C et al (2007) Fiber and magnesium intake and incidence of type 2 diabetes: a prospective study and meta-analysis. Arch Intern Med 167:956–965
Pan XR, Li GW, Hu YH et al (1997) Effects of diet and exercise in preventing NIDDM in people with impaired glucose tolerance. The Da Qing IGT and diabetes study. Diabetes Care 20:537–544
Tuomilehto J, Lindstrom J, Eriksson JG et al (2001) Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N Engl J Med 344:1343–1350
Knowler WC, Barrett-Connor E, Fowler SE et al (2002) Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med 346:393–403
Tinker LF, Bonds DE, Margolis KL et al (2008) Low-fat dietary pattern and risk of treated diabetes mellitus in postmenopausal women: the women’s health initiative randomized controlled dietary modification trial. Arch Intern Med 168:1500–1511
Kearney PM, Whelton M, Reynolds K et al (2005) Global burden of hypertension: analysis of worldwide data. Lancet 365:217–223
Lewington S, Clarke R, Qizilbash N et al (2002) Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet 360:1903–1913
Weikert S, Boeing H, Pischon T et al (2008) Blood pressure and risk of renal cell carcinoma in the European prospective investigation into cancer and nutrition. Am J Epidemiol 167:438–446
Cook NR, Cohen J, Heber PR et al (1995) Implications of small reductions in diastolic blood pressure for primary prevention. Arch Intern Med 155:701–709
Staessen JA, Li Y, Thijs L, Wang JG (2005) Blood pressure reduction and cardiovascular prevention: an update including the 2003–2004 secondary prevention trials. Hypertens Res 28:385–407
Chobanian AV, Bakris GL, Black HR et al (2003) The seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure: the JNC 7 report. JAMA 289:2560–2572
Mancia G, De Backer G, Dominiczak A et al (2007) 2007 ESH–ESC practice guidelines for the management of arterial hypertension: ESH–ESC task force on the management of arterial hypertension. J Hypertens 25:1751–1762
Stamler J (1997) The INTERSALT study: background, methods, findings, and implications. Am J Clin Nutr 65:626S–642S
Berry SE, Mulla UZ, Chowienczyk PJ, Sanders TA (2010) Increased potassium intake from fruit and vegetables or supplements does not lower blood pressure or improve vascular function in UK men and women with early hypertension: a randomised controlled trial. Br J Nutr 104:1839–1847
Berkow SE, Barnard ND (2005) Blood pressure regulation and vegetarian diets. Nutr Rev 63:1–8
Ascherio A, Hennekens C, Willett WC et al (1996) Prospective study of nutritional factors, blood pressure, and hypertension among US women. Hypertension 27:1065–1072
Miura K, Greenland P, Stamler J et al (2004) Relation of vegetable, fruit, and meat intake to 7-year blood pressure change in middle-aged men: the Chicago Western Electric Study. Am J Epidemiol 159:572–580
Steffen LM, Kroenke CH, Yu X et al (2005) Associations of plant food, dairy product, and meat intakes with 15-y incidence of elevated blood pressure in young black and white adults: the Coronary Artery Risk Development in Young Adults (CARDIA) Study. Am J Clin Nutr 82:1169–1177
Schulze MB, Hoffmann K, Kroke A, Boeing H (2003) Risk of hypertension among women in the EPIC-Potsdam Study: comparison of relative risk estimates for exploratory and hypothesis-oriented dietary patterns. Am J Epidemiol 158:365–373
Dauchet L, Kesse-Guyot E, Czernichow S et al (2007) Dietary patterns and blood pressure change over 5-y follow-up in the SU.VI.MAX cohort. Am J Clin Nutr 85:1650–1656
Nuñez-Cordoba JM, Alonso A, Beunza JJ et al (2009) Role of vegetables and fruits in Mediterranean diets to prevent hypertension. Eur J Clin Nutr 63:605–612
Cassidy A, O’Reilly ÉJ, Kay C et al (2011) Habitual intake of flavonoid subclasses and incident hypertension in adults. Am J Clin Nutr 93:338–347
Appel LJ, Moore TJ, Obarzanek E et al (1997) A clinical trial of the effects of dietary patterns on blood pressure. DASH Collaborative Research Group. N Engl J Med 336:1117–1124
Appel LJ, Champagne CM, Harsha DW et al (2003) Effects of comprehensive lifestyle modification on blood pressure control: main results of the PREMIER clinical trial. JAMA 289:2083–2093
Moore LL, Singer MR, Bradlee ML et al (2005) Intake of fruits, vegetables, and dairy products in early childhood and subsequent blood pressure change. Epidemiology 16:4–11
John JH, Ziebland S, Yudkin P et al (2002) Effects of fruit and vegetable consumption on plasma antioxidant concentrations and blood pressure: a randomised controlled trial. Lancet 359:1969–1974
Zino S, Skeaff M, Williams S, Mann J (1997) Randomised controlled trial of effect of fruit and vegetable consumption on plasma concentrations of lipids and antioxidants. BMJ 314:1787–1791
WHO (World Health Organization) (2008) The global burden of disease: 2004 update. WHO, Geneva
WHO (World Health Organization) (2011) Global status report on noncommunicable diseases 2010. WHO, Geneva
Gaziano TA, Bitton A, Anand S et al (2010) Growing epidemic of coronary heart disease in low- and middle-income countries. Curr Probl Cardiol 35:72–115
Graham I, Atar D, Borch-Johnsen K et al (2007) European guidelines on cardiovascular disease prevention in clinical practice: executive summary. Fourth joint task force of the European society of cardiology and other societies on cardiovascular disease prevention in clinical practice (constituted by representatives of nine societies and by invited experts). Eur J Cardiovasc Prev Rehabil 14(Suppl 2):E1–E40
Hu FB, Willett WC (2002) Optimal diets for prevention of coronary heart disease. JAMA 288:2569–2578
Dauchet L, Amouyel P, Hercberg S, Dallongeville J (2006) Fruit and vegetable consumption and risk of coronary heart disease: a meta-analysis of cohort studies. J Nutr 136:2588–2593
He FJ, Nowson CA, Lucas M, Macgregor GA (2007) Increased consumption of fruit and vegetables is related to a reduced risk of coronary heart disease: meta-analysis of cohort studies. J Hum Hypertens 21:717–728
Crowe FL, Roddam AW, Key TJ et al (2011) European prospective investigation into cancer and nutrition (EPIC)-heart study collaborators. Fruit and vegetable intake and mortality from ischaemic heart disease: results from the European Prospective Investigation into Cancer and Nutrition (EPIC)-Heart Study. Eur Heart J 32:1235–1243
Oude Griep LM, Geleijnse JM, Kromhout D et al (2010) Raw and processed fruit and vegetable consumption and 10-year coronary heart disease incidence in a population-based cohort study in The Netherlands. PLoS One 5:e13609
Holmberg S, Thelin A, Stiernström EL (2009) Food choices and coronary heart disease: a population based cohort study of rural Swedish men with 12 years of follow-up. Int J Environ Res Public Health 6:2626–2638
Nagura J, Iso H, Watanabe Y et al (2009) Fruit, vegetable and bean intake and mortality from cardiovascular disease among Japanese men and women: the JACC Study. Br J Nutr 102:285–292
Bendinelli B, Masala G, Saieva C et al (2011) Fruit, vegetables, and olive oil and risk of coronary heart disease in Italian women: the EPICOR Study. Am J Clin Nutr 93:275–283
Bazzano LA (2005) Dietary intake of fruits and vegetables and risk of diabetes mellitus and cardiovascular disease. World Health Organization, Geneva
American Heart Association (2011) Primary prevention of cardiovascular disease in adults. www.americanheart.org/presenter.jhtml?identifier=4704. Accessed 09 Mar 2011
Howard BV, Van Horn L, Hsia J et al (2006) Low-fat dietary pattern and risk of cardiovascular disease: the women’s health initiative randomized controlled dietary modification trial. JAMA 295:655–656
McCall DO, McGartland CP, McKinley MC et al (2009) Dietary intake of fruits and vegetables improves microvascular function in hypertensive subjects in a dose-dependent manner. Circulation 119:2153–2160
Hubbard GP, Wolffram S, de Vos R et al (2006) Ingestion of onion soup high in quercetin inhibits platelet aggregation and essential components of the collagen-stimulated platelet activation pathway in man: a pilot study. Br J Nutr 96:482–488
O’Kennedy N, Crosbie L, Whelan S et al (2006) Effects of tomato extract on platelet function: a double-blinded crossover study in healthy humans. Am J Clin Nutr 84:561–569
Erlund I, Koli R, Alfthan G et al (2007) Favourable effects of berry consumption on platelet function, blood pressure, and HDL cholesterol. Am J Clin Nutr 87:323–331
Watzl B, Kulling SE, Möseneder J et al (2005) A 4-week intervention with high intake of carotenoid-rich vegetables and fruit reduces plasma C-reactive protein in healthy, non-smoking men. Am J Clin Nutr 82:1052–1058
Kelley DS, Rasooly R, Jacob RA et al (2006) Consumption of Bing sweet cherries lowers circulating concentrations of inflammation markers in healthy men and women. J Nutr 136:981–986
Goldstein LB, Bushnell CD, Adams RJ et al (2011) Guidelines for the primary prevention of stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 42:517–584
Dauchet L, Amouyel P, Dallongeville J (2005) Fruit and vegetable consumption and risk of stroke: a metaanalysis of cohort studies. Neurology 65:1193–1197
He FJ, Nowson CA, MacGregor GA (2006) Fruit and vegetable consumption and stroke: meta-analysis of cohort studies. Lancet 367:320–326
Ferlay J, Parkin DM, Steliarova-Foucher E (2010) Estimates of cancer incidence and mortality in Europe in 2008. Eur J Cancer 46:765–781
Block G, Patterson B, Subar A (1992) Fruit, vegetables, and cancer prevention: a review of the epidemiological evidence. Nutr Cancer 18:1–29
WCRF (World Cancer Research Fund) (1997) Food, nutrition, and the prevention of cancer: a global perspective. World Cancer Research Fund/American Institute for Cancer Research, Washington, DC
Hoffmann K, Boeing H, Volatier JL, Becker W (2003) Evaluating the potential health gain of the World Health Organization’s recommendation concerning vegetable and fruit consumption. Public Health Nutr 6:765–772
Boeing H, Barth C, Kluge S (2004) Tumorentstehung—hemmende und fördernde Ernährungsfaktoren. In: Ernährungsbericht 2004. Deutsche Gesellschaft für Ernährung, Bonn
IARC (2003) Fruit and vegetables. IARC handbook of cancer prevention, vol 8. IARC Press, Lyon
Riboli E, Norat T (2003) Epidemiologic evidence of the protective effect of fruit and vegetables on cancer risk. Am J Clin Nutr 78:559S–569S
Boeing H, Barth C, Steffen A (2008) Zusammenhang zwischen Ernährung und Krebsentstehung. In: Ernährungsbericht 2008. Deutsche Gesellschaft für Ernährung, Bonn
Riboli E, Hunt KJ, Slimani N et al (2002) European Prospective Investigation into Cancer and Nutrition (EPIC): study populations and data collection. Public Health Nutr 5:1113–1124
Schatzkin A, Subar AF, Thompson FE et al (2001) Design and serendipity in establishing a large cohort with wide dietary intake distributions: the National Institutes of Health-American association of retired persons diet and health study. Am J Epidemiol 154:1119–1125
Key TJ (2011) Fruit and vegetables and cancer risk. Br J Cancer 104:6–11
Hung HC, Joshipura KJ, Jiang R et al (2004) Fruit and vegetable intake and risk of major chronic disease. J Natl Cancer Inst 96:1577–1584
Takachi R, Inoue M, Ishihara J, JPHC Study Group et al (2008) Fruit and vegetable intake and risk of total cancer and cardiovascular disease: Japan Public Health Center-based prospective study. Am J Epidemiol 167:59–70
George SM, Park Y, Leitzmann MF et al (2009) Fruit and vegetable intake and risk of cancer: a prospective cohort study. Am J Clin Nutr 89:347–353
Boffetta P, Couto E, Wichmann J et al (2010) Fruit and vegetable intake and overall cancer risk in the European Prospective Investigation into Cancer and Nutrition (EPIC). J Natl Cancer Inst 102:529–537
Beresford SA, Johnson KC, Ritenbaugh C et al (2006) Low-fat dietary pattern and risk of colorectal cancer: the women’s health initiative randomized controlled dietary modification trial. JAMA 295:643–654
Prentice RL, Caan B, Chlebowski RT et al (2006) Low-fat dietary pattern and risk of invasive breast cancer: the women’s health initiative randomized controlled dietary modification trial. JAMA 295:629–642
Kaser A, Zeissig S, Blumberg RS (2010) Inflammatory bowel disease. Annu Rev Immunol 28:573–621
Lakatos PL (2006) Recent trends in the epidemiology of inflammatory bowel diseases: up or down? World J Gastroenterol 12:6102–6108
Halfvarson J, Bodin L, Tysk C et al (2003) Inflammatory bowel disease in a Swedish twin cohort: a long-term follow-up of concordance and clinical characteristics. Gastroenterology 124:1767–1773
Shanahan F, Bernstein CN (2009) The evolving epidemiology of inflammatory bowel disease. Curr Opin Gastroenterol 25:301–305
Sartor RB (2006) Mechanisms of disease: pathogenesis of Crohn’s disease and ulcerative colitis. Nat Clin Pract Gastroenterol Hepatol 3:390–407
Clavel T, Haller D (2007) Bacteria- and host-derived mechanisms to control intestinal epithelial cell homeostasis: implications for chronic inflammation. Inflamm Bowel Dis 13:1153–1164
Werner T, Wagner SJ, Martinez I et al (2011) Depletion of luminal iron alters the gut microbiota and prevents Crohn’s disease-like ileitis. Gut 60:325–333
Raman M, Milestone AN, Walters JR et al (2011) Vitamin D and gastrointestinal diseases: inflammatory bowel disease and colorectal cancer. Therap Adv Gastroenterol 4:49–62
Renz H, von Mutius E, Brandtzaeg P et al (2011) Gene-environment interaction in chronic inflammatory disease. Nat Immunol 12:273–277
Hou JK, Abraham B, El-Serag H (2011) Dietary intake and risk of developing inflammatory bowel disease: a systematic review of the literature. Am J Gastroenterol 106:563–573
Symmons D, Turner G, Webb R et al (2002) The prevalence of rheumatoid arthritis in the United Kingdom: new estimates for a new century. Rheumatology 41:793–800
Theis KA, Helmick CG, Hootman JM (2007) Arthritis burden and impact are greater among U.S. women than men: intervention opportunities. J Womens Health 16:441–453
Pattison DJ, Silman AJ, Goodson NJ et al (2004) Vitamin C and the risk of developing inflammatory polyarthritis: prospective nested case-control study. Ann Rheum Dis 63:843–847
Cerhan JR, Saag KG, Merlino LA et al (2003) Antioxidant micronutrients and risk of rheumatoid arthritis in a cohort of older women. Am J Epidemiol 157:345–354
Pattison DJ, Symmons DPM, Lunt M et al (2004) Dietary risk factors for the development of inflammatory polyarthritis. Arthritis Rheum 50:3804–3812
Pedersen M, Stripp C, Klarlund M et al (2005) Diet and risk of rheumatoid arthritis in a prospective study. J Rheumatol 32:1249–1252
Wang Y, Hodge AM, Wluka AE et al (2007) Effect of antioxidants on knee cartilage and bone in healthy, middle-aged subjects: a cross-sectional study. Arthritis Res Ther 9:R66
Linos A, Kaklamani VG, Kaklamani E et al (1999) Dietary factors in relation to rheumatoid arthritis: a role for olive oil and cooked vegetables? Am J Clin Nutr 70:1077–1082
McKellar G, Morrison E, McEntegart A et al (2007) A pilot study of Mediterranean-type diet intervention in female patients with rheumatoid arthritis (RA) living in areas of social deprivation in Glasgow. Ann Rheum Dis 66:1239–1243
Halbert RJ, Natoli JL, Gano A et al (2006) Global burden of COPD: systematic review and meta-analysis. Eur Respir J 28:523–532
Miedema I, Feskens EJM, Heederik D, Kromhout D (1993) Dietary determinants of long-term incidence of chronic nonspecific lung disease. The Zutphen study. Am J Epidemiol 138:37–45
Walda IC, Tabak C, Smit HA et al (2002) Diet and 20-year chronic obstructive pulmonary disease mortality in middle-aged men from three European countries. Eur J Clin Nutr 56:638–643
Varraso R, Fung TT, Hu FB et al (2007) Prospective study of dietary patterns and chronic obstructive pulmonary disease among US men. Thorax 62:786–791
Varraso R, Fung TT, Barr RG et al (2007) Prospective study of dietary patterns and chronic obstructive pulmonary disease among US women. Am J Clin Nutr 86:488–495
Watson L, Margetts B, Howarth P et al (2002) The association between diet and chronic obstructive pulmonary disease in subjects selected from general practice. Eur Respir J 20:313–318
Hirayama F, Lee AH, Binns CW et al (2009) Do vegetables and fruits reduce the risk of chronic obstructive pulmonary disease? A case-control study in Japan. Prev Med 49:184–189
Strachan DP, Cox BD, Erzinclioglu SW et al (1991) Ventilatory function and winter fresh fruit consumption in a random sample of British adults. Thorax 46:624–629
Cook DG, Carey IM, Whincup PH et al (1997) Effect of fresh fruit consumption on lung function and wheeze in children. Thorax 52:628–633
Carey IM, Strachan DP, Cook DG (1998) Effects of change in fresh fruit consumption on ventilatory function in healthy British adults. Am J Respir Crit Care Med 158:728–733
Butland BK, Strachan DP, Anderson HR (1999) Fresh fruit intake and asthma symptoms in young British adults: confounding or effect modification by smoking? Eur Resp J 13:744–750
Tabak C, Smit HA, Räsänen L et al (1999) Dietary factors and pulmonary function: a cross sectional study in middle aged men from three European countries. Thorax 54:1021–1026
Forastiere F, Pistelli R, Sestini P et al (2000) Consumption of fresh fruit rich in vitamin C and wheezing symptoms in children. Thorax 55:283–288
Butland BK, Fehily AM, Elwood PC (2000) Diet, lung function decline in a cohort of 2,512 middle aged men. Thorax 55:102–108
Tabak C, Smit HA, Heederik D et al (2001) Diet and chronic obstructive pulmonary disease: independent beneficial effects of fruits, whole grains, and alcohol (the MORGEN study). Clin Exp Allergy 31:747–755
Tabak C, Arts ICW, Smit HA et al (2001) Chronic obstructive pulmonary disease and intake of catechins, flavonols, and flavones. The MORGEN study. Am J Respir Crit Care Med 164:61–64
Kelly Y, Sacker A, Marmot M (2003) Nutrition and respiratory health in adults: findings from the health survey for Scotland. Eur Respir J 21:664–671
Farchi S, Forastiere F, Agabiti N et al (2003) Dietary factors associated with wheezing and allergic rhinitis in children. Eur Respir J 22:772–780
Antova T, Pattenden S, Nikiforov B et al (2003) Nutrition and respiratory health in children in six central and eastern European countries. Thorax 58:231–236
Gilliland FD, Berhane KT, Li YF et al (2003) Children’s lung function and antioxidant vitamin, fruit, juice, and vegetable intake. Am J Epidemiol 158:576–584
Celik F, Topcu F (2006) Nutritional risk factors for the development of chronic obstructive pulmonary disease (COPD) in male smokers. Clin Nutr 25:955–961
Burns JS, Dockery DW, Neas LM et al (2007) Low dietary nutrient intakes and respiratory health in adolescents. Chest 132:238–245
Chatzi L, Torrent M, Romieu I et al (2007) Diet, wheeze, and atopy in school children in Menorca, Spain. Pediatr Allergy Immunol 18:480–485
Kan H, Stevens J, Heiss G et al (2008) Dietary fiber, lung function, and chronic obstructive pulmonary disease in the atherosclerosis risk in communities (ARIC) study. Am J Epidemiol 167:570–578
Varroso R, Willett WC, Camargo CA (2010) Prospective study of dietary fiber and risk of chronic obstructive pulmonary disease among US women and men. Am J Epidemiol 171:776–784
Braman SS (2006) The global burden of asthma. Chest 130:4S–12S
McKeever TM, Britton J (2004) Diet and asthma. Am J Respir Crit Care Med 170:725–729
Allan K, Devereux G (2011) Diet and asthma: nutrition implications from prevention to treatment. J Am Diet Assoc 111:258–268
Nurmatov U, Devereux G, Sheikh A (2011) Nutrients and foods for the primary prevention of asthma and allergy: systematic review and meta-analysis. J Allergy Clin Immunol 127:724–733
Heinrich J, Hölscher B, Bolte G, Winkler G (2001) Allergic sensitization and diet: ecological analysis in selected European cities. Eur Respir J 17:395–402
Huang SL, Lin KC, Pan WH (2001) Dietary factors associated with physician-diagnosed asthma and allergic rhinitis in teenagers: analyses of the first nutrition and health survey in Taiwan. Clin Exp Allergy 31:259–264
Priftanji AV, Qirko E, Burr ML et al (2002) Factors associated with asthma in Albania. Allergy 57:123–128
Woods RK, Walters EH, Raven JM et al (2003) Food and nutrient intakes and asthma risk in young adults. Am J Clin Nutr 78:414–421
Wong GWK, Ko FWS, Hui DSC et al (2004) Factors associated with differences in prevalence of asthma in children from three cities in China: multicentre epidemiological survey. BMJ 329:486–489
Lewis SA, Antoniak M, Venn AJ et al (2005) Second hand smoke, dietary fruit intake, road traffic exposures, and the prevalence of asthma: a cross-sectional study in young children. Am J Epidemiol 161:406–411
Nja F, Nystad W, Lodrup Carlsen KC et al (2005) Effects of early intake of fruit or vegetables in relation to later asthma and allergic sensitization in school-age children. Acta Paediatr 94:147–154
Chatzi L, Apostolaki G, Bibakis I et al (2007) Protective effect of fruits, vegetables and the Mediterranean diet on asthma and allergies among children in Crete. Thorax 62:677–683
Tsai HJ, Tsai AC (2007) The association of the diet with respiratory symptoms and asthma in schoolchildren in Taipei, Taiwan. J Asthma 44:599–603
Barros R, Moreira A, Fonseca J et al (2008) Adherence to the Mediterranean diet and fresh fruit intake are associated with improved asthma control. Allergy 63:917–923
Shaheen SO, Sterne JA, Thompson RL et al (2001) Dietary antioxidants and asthma in adults: population-based case-control study. Am J Respir Crit Care Med 164:1823–1828
Garcia V, Arts ICW, Sterne JAC et al (2005) Dietary intake of flavonoids and asthma in adults. Eur Respir J 26:449–452
Tabak C, Wijga AH, de Meer G et al (2006) Diet and asthma in Dutch school children (ISAAC-2). Thorax 61:1048–1053
Romieu I, Barraza-Villarreal A, Escamilla-Núnez C et al (2009) Dietary intake, lung function and airway inflammation in Mexico City school children exposed to air pollutants. Respir Res 10:122
Romieu I, Varraso R, Avenel V et al (2006) Fruit and vegetable intakes and asthma in the E3N study. Thorax 61:209–215
Willers S, Devereux G, Craig LC et al (2007) Maternal food consumption during pregnancy and asthma, respiratory and atopic symptoms in 5-year-old children. Thorax 62:773–779
Bacopoulou F, Veltsista A, Vassi I et al (2009) Can we be optimistic about asthma in childhood? A Greek cohort study. J Asthma 46:171–174
Wood LG, Garg ML, Powell H, Gibson PG (2008) Lycopene-rich treatments modify noneosinophilic airway inflammation in asthma: proof of concept. Free Rad Res 42:94–102
Okoko BJ, Burney PG, Newson RB et al (2007) Childhood asthma and fruit consumption. Eur Respir J 29:1161–1168
Polonikov AV, Ivanov VP, Solodilova MA et al (2009) Tobacco smoking, fruit and vegetable intake modify association between −21 > T polymorphism of catalase gene and risk of bronchial asthma. J Asthma 46:217–224
NIH Consens Statement (2000) Osteoporosis prevention, diagnosis, and therapy, vol 17. NIH Consens Statement, Bethesda, Maryland, pp 1–45
Johnell O, Kanis JA (2006) An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos Int 17:1726–1733
Melton LJ III, Gabriel SE, Crowson CS et al (2003) Cost-equivalence of different osteoporotic fractures. Osteoporos Int 14:383–388
Johnell O, Kanis J (2005) Epidemiology of osteoporotic fractures. Osteoporos Int 16:S3–S7
Seeman E, Bianchi G, Khosla S et al (2006) Bone fragility in men—where are we? Osteoporos Int 17:1577–1583
Center JR, Nguyen TV, Schneider D et al (1999) Mortality after all major types of osteoporotic fracture in men and women: an observational study. Lancet 353:878–882
Jiang HX, Majumdar SR, Dick DA et al (2005) Development and initial validation of a risk score for predicting in-hospital and 1-year mortality in patients with hip fractures. J Bone Miner Res 20:494–500
Kanis JA, Johnell O (2005) Requirements for DXA for the management of osteoporosis in Europe. Osteoporos Int 16:229−238
Kohrt WM, Bloomfield SA, Little KD, For the American College of Sports Medicine et al (2004) hysical activity and bone health. Med Sci Sports Exerc 36:1985–1996
Marks R (2011) Physical activity and hip fracture disability: a review. J Aging Res 2011:741918
Tucker KL (2009) Osteoporosis prevention and nutrition. Curr Osteoporos Rep 7:111–117
De Laet C, Kanis JA, Odén A et al (2005) Body mass index as a predictor of fracture risk: a meta-analysis. Osteoporos Int 16:1330–1338
Beck TJ, Petit MA, Wu G et al (2009) Does obesity really make the femur stronger? BMD, geometry, and fracture incidence in the women’s health initiative-observational study. J Bone Miner Res 24:1369–1379
Prentice A (2004) Diet, nutrition and the prevention of osteoporosis. Public Health Nutr 7:227–243
Heaney RP, Layman DK (2008) Amount and type of protein influences on bone health. Am J Clin Nutr 87:156S–170S
Shea MK, Booth SL (2008) Update on the role of vitamin K in skeletal health. Nutr Rev 66:549–557
Michelfelder AJ (2009) Soy: a complete source of protein. Am Fam Physician 79:43–47
Hooshmand S, Arjimani BH (2009) Viewpoint: dried plum, an emerging food that may effectively improve bone health. Aging Res Rev 8:122–127
Peters BS, Martini LA (2010) Nutritional aspects of the prevention and treatment of osteoporosis. Arq Bras Endocrinol Metab 54:179–185
New SA (2002) Nutrition society medal lecture. The role of the skeleton in acid-base homeostasis. Proc Nutr Soc 61:151–164
New SA (2003) Intake of fruits and vegetables: implications for bone health. Proc Nutr Soc 62:889–899
Jajoo R, Song L, Rasmussen H et al (2006) Dietary acid–base balance, bone resorption, and calcium excretion. J Am Coll Nutr 25:224–230
Putnam SE, Scutt AM, Bicknell K et al (2007) Natural products as alternative treatments for metabolic disorders and for maintenance of bone health. Phytother Rev 21:99–112
Hamidi M, Boucher BA, Cheung AM et al (2011) Fruit and vegetable intake and bone health in women aged 45 years and over: a systematic review. Osteoporos Int 22:1681–1693
McTiernan A, Wactawski-Wende J, Wu L et al (2009) Women’s health initiative investigators. Low-fat, increased fruit, vegetable, and grain dietary pattern, fractures, and bone mineral density: the women’s health initiative dietary modification trial. Am J Clin Nutr 89:1864–1876
Benetou V, Orfanos P, Zylis D et al (2011) Diet and hip fractures among elderly Europeans in the EPIC cohort. Eur J Clin Nutr 65:132–139
Monma Y, Niu K, Iwasaki K et al (2010) Dietary patterns associated with fall-related fracture in elderly Japanese: a population based prospective study. BMC Geriatr 10:31
Papaioannou A, Kennedy CC, Cranney A et al (2009) Risk factors for low BMD in healthy men age 50 years or older: a systematic review. Osteoporos Int 20:507–518
Macdonald HM, Black AJ, Aucott L et al (2008) Effect of potassium citrate supplementation or increased fruit and vegetable intake on bone metabolism in healthy postmenopausal women: a randomized controlled trial. Am J Clin Nutr 88:465–474
Langsetmo L, Hanley DA, Prior JC et al (2011) CaMos research group. Dietary patterns and incident low-trauma fractures in postmenopausal women and men aged ≥50 y: a population-based cohort study. Am J Clin Nutr 93:192–199
Lin P-H, Ginty F, Appel LJ et al (2003) The DASH diet and sodium reduction improve markers of bone turnover and calcium metabolism in adults. J Nutr 133:3130–3136
Kaptoge S, Welch A, McTaggart A et al (2003) Effects of dietary nutrients and food groups on bone loss from the proximal femur in men and women in the 7th and 8th decades of age. Osteoporos Int 14:418–428
Tucker KL, Hannan MT, Kiel DP (2001) The acid–base hypothesis: diet and bone in the Framingham Osteoporosis Study. Eur J Nutr 40:231–237
Tucker KL, Hannan MT, Chen H et al (1999) Potassium, magnesium, and fruit and vegetable intakes are associated with greater bone mineral density in elderly men and women. Am J Clin Nutr 69:727–736
Vatanparast H, Baxter-Jones A, Faulkner RA et al (2005) Positive effects of vegetable and fruit consumption and calcium intake on bone mineral accrual in boys during growth from childhood to adolescence: the University of Saskatchewan pediatric bone mineral accrual study. Am J Clin Nutr 82:700–706
Wosje KS, Khoury PR, Claytor RP et al (2010) Dietary patterns associated with fat and bone mass in young children. Am J Clin Nutr 92:294–303
DeBar LL, Ritenbaugh C, Aickin M et al (2006) Youth: a health plan-based lifestyle intervention increases bone mineral density in adolescent girls. Arch Pediatr Adolesc Med 160:1269–1276
Cole ZA, Gale CR, Javaid MK et al (2009) Maternal dietary patterns during pregnancy and childhood bone mass: a longitudinal study. J Bone Miner Res 24:663–668
Ganpule A, Yajnik CS, Fall CH et al (2006) Bone mass in Indian children—relationships to maternal nutritional status and diet during pregnancy: the Pune Maternal Nutrition Study. J Clin Endocrinol Metab 91:2994–3001
Ashwell M, Stone E, Mathers J et al (2008) Nutrition and bone health projects funded by the UK food standards agency: have they helped to inform public health policy? Br J Nutr 99:198–205
Pascolini D, Mariotti SP (2012) Global estimates of visual impairment: 2010. Br J Ophthalmol 96:614–618
Resnikoff S, Pascolini D, Etya’ale D et al (2004) Global data on visual impairment in the year 2002. Bull World Health Organ 82:844–851
WHO (World Health Organization) (2011) Visual impairment and blindness. WHO fact sheet N° 282
Knauer C, Pfeiffer N (2006) Erblindung in Deutschland—heute und 2030. Ophthalmologe 103:735–741
Prokofyeva E, Zrenner E (2012) Epidemiology of major eye diseases leading to blindness in Europe: a literature review. Ophthalmic Res 47:171–188
Laitinen A, Laatikainen L, Härkänen T et al (2010) Prevalence of major eye diseases and causes of visual impairment in the adult Finnish population: a nationwide population-based survey. Acta Ophthalmol 88:463–471
Congdon N, Vingerlin JR, Klein BEK et al (2004) Prevalence of cataract and pseudophakia/aphakia among adults in the United States. Arch Ophthalmol 122:487–494
Sasaki K, Sasaki H, Jonasson F et al (2004) Racial differences of lens transparency properties with aging and prevalence of age-related cataract applying a WHO classification system. Ophthlamic Res 36:332–340
Fine SL, Berger J, Maguire MG, Ho AC (2000) Age-related macular degeneration. N Engl J Med 342:483–492
Evans JR (2001) Risk factors for age-related macular degeneration. Prog Retin Eye Res 20:227–253
Clemons TE, Milton RC, Klein R et al (2005) And age-related eye disease study research group. Risk factors for the incidence of advanced age-related macular degeneration in the age-related eye disease study (AREDS) AREDS report no. 19. Ophthalmology 112:533–539
Guymer RH, Chong EWT (2006) Modifiable risk factors for age-related macular degeneration. Med J Aust 184:455–458
Kaushik S, Wang JJ, Flood V et al (2008) Dietary glycemic index and the risk of age-related macular degeneration. Am J Clin Nutr 88:1104–1110
Parekh N, Voland RP, Moeller SM et al (2009) Association between dietary fat intake and age-related macular degeneration in the Carotenoids in Age-Related Eye Disease Study (CAREDS): an ancillary study of the women’s health initiative. Arch Ophthalmol 127:1483–1493
Evans JR (2006) Antioxidant vitamin and mineral supplements for slowing the progression of age-related macular degeneration. Cochrane Database Syst Rev (2), Article No. CD000254
Evans JR, Heanshaw KS (2008) Antioxidant vitamin and mineral supplements to prevent the development of age-related macular degeneration. Cochrane Database Syst Rev (1), Article No. CD000253
Johnson EJ (2010) Age-related macular degeneration and antioxidant vitamins: recent findings. Cur Opin Clin Nutr Metabol Care 13:28–33
Krinsky NI, Landrum JT, Bone RA (2003) Biologic mechanisms of the protective role of lutein and zeaxanthin in the eye. Annu Rev Nutr 23:171–201
Beatty S, Boulton M, Henson D et al (1999) Macular pigment and age related macular degeneration. Brit J Ophthalmol 83:867–877
Landrum JT, Bone RA (2001) Lutein, zeaxanthin, and the macular pigment. Arch Biochem Biophys 385:28–40
Mares-Perlman JA, Fisher AI, Klein R et al (2001) Lutein and zeaxanthin in the diet and serum and their relation to age-related maculopathy in the third national health and nutrition examination survey. Am J Epidemiol 153:424–432
Gale CR, Hall NF, Phillips DIW, Martyn CH (2003) Lutein and zeaxanthin status and risk of age-related macular degeneration. Invest Ophthalmol Vis Sci 44:2461–2465
Beatty S, Nolan J, Kavanagh H, O’Donovan O (2004) Macular pigment optical density and its relationship with serum and dietary levels of lutein and zeaxanthin. Arch Biochem Biophys 430:70–76
Hogg R, Chakravarthy U (2004) AMD and micronutrient antioxidants. Curr Eye Res 29:387–401
Ribaya-Mercado JD, Blumberg JB (2004) Lutein and zeaxanthin and their potential roles in disease prevention. J Am Coll Nutr 23:567S–587S
Delcourt C, Carrière I, Delage M et al (2006) Plasma lutein and zeaxanthin and other carotenoids as modifiable risk factors for age-related maculopathy and cataract: the POLA Study. Invest Ophthalmol Vis Sci 47:2329–2335
SanGiovanni JP, Chew EY, Clemons TE et al (2007) The relationship of dietary carotenoid and vitamin A, E, and C intake with age-related macular degeneration in a case-control study—AREDS report no. 22. Arch Ophthal 125:1225–1232
Tan JSL, Wang JJ, Flood V et al (2008) Dietary antioxidants and the long-term incidence of age-related macular degeneration—the Blue Mountains Eye Study. Ophthalmology 115:334–341
Cho EY, Hankinson SE, Rosner B et al (2008) Prospective study of lutein/zeaxanthin intake and risk of age-related macular degeneration. Am J Clin Nutr 87:1837–1843
Morris MS, Jacques PF, Chylack LT et al (2007) Intake of zinc and antioxidant micronutrients and early age-related maculopathy lesions. Ophthalmic Epidemiol 14:288–298
Van Leeuwen R, Boekhoorn S, Vingerling JR et al (2005) Dietary intake of antioxidants and risk of age-related macular degeneration. JAMA 294:3101–3107
Robman L, Vu H, Hodge A et al (2007) Dietary lutein, zeaxanthin, and fats and the progression of age-related macular degeneration. Can J Ophthalmol 42:720–726
Cho EY, Seddon JM, Rosner B et al (2004) Prospective study of intake of fruits, vegetables, vitamins, and carotenoids and risk of age-related maculopathy. Arch Ophthalmol 122:883–892
Moeller SM, Parekh N, Tinker L et al (2006) Associations between intermediate age-related macular degeneration and lutein and zeaxanthin in the Carotenoids in Age-Related Eye Disease Study (CAREDS). Arch Ophthalmol 124:1151–1162
Seddon JM, Ajani UA, Sperduto RD et al (1994) Dietary carotenoids, vitamins A, C, and E, and advanced age-related macular degeneration. Eye disease case-control study group. JAMA 272:1413–1420
Goldberg J, Flowerdew G, Smith E et al (1988) Factors associated with age-related macular-degeneration. Am J Epidemiol 128:700–710
BVA (Berufsverband der Augenärzte Deutschlands e. V.) und DOG (Deutsche Ophthalmologische Gesellschaft e. V. Katarakt (Grauer Star) im Erwachsenalter (1998) Leitlinie Nr. 19
Asbell PA, Dualan L, Mindel J et al (2005) Age-related cataract. Lancet 365:599–609
Jacques PF (1999) The potential preventive effects of vitamins for cataract and age-related macular degeneration. Int J Vitam Nutr Res 69:198–205
Lyle BJ, Maresperlman JA, Klein BEK et al (1999) Serum carotenoids and tocopherols and incidence of age-related nuclear cataract. Am J Clin Nutr 69:272–277
Taylor A, Hobbs M (2001) The 2001 assessment of nutritional influences on risk for cataract. Nutrition 17:845–847
Christen WG, Manson JE, Glynn RJ et al (2003) A randomized trial of beta carotene and age-related cataract in US physicians. Arch Ophthalmol 121:372–378
Mares JA (2004) High-dose antioxidant supplementation and cataract risk. Nutr Rev 62:28–32
Tan JSL, Mitchell P, Flood V et al (2008) Antioxidant nutrient intake and the long-term incidence of age-related cataract—the Blue Mountains Eye Study. Am J Clin Nutr 87:1899–1905
Moeller SM, Taylor A, Tucker KL et al (2004) Overall adherence to the dietary guidelines for Americans is associated with reduced prevalence of early age-related nuclear lens opacities in women. J Nutr 134:1812–1819
Brown L, Rimm EB, Seddon JM et al (1999) A prospective study of carotenoid intake and risk of cataract extraction in US men. Am J Clin Nutr 70:517–524
Christen WG, Liu SM, Schaumberg DA, Buring JE (2005) Fruit and vegetable intake and the risk of cataract in women. Am J Clin Nutr 81:1417–1422
Christen WG, Liu S, Glynn RJ et al (2008) Dietary carotenoids, vitamins C and E, and risk of cataract in women. Arch Ophthalmol 126:102–109
Moeller SM, Voland R, Tinker L et al (2008) Associations between age-related nuclear cataract and lutein and zeaxanthin in the diet and serum in the Carotenoids in the Age-Related Eye Disease Study (CAREDS), an ancillary study of the women’s health initiative. Arch Ophthalmol 126:354–364
BVA (Berufsverband der Augenärzte Deutschlands e. V.) und DOG (Deutsche Ophthalmologische Gesellschaft e. V. (2006) Detektion des primären Offenwinkelglaukoms (POWG). Leitlinie Nr. 15c
Kang JH, Pasquale LR, Willet W et al (2003) Antioxidant intake and primary open-angle glaucoma: a prospective study. Am J Epidemiol 158:337–346
Veach J (2004) Functional dichotomy: glutathione and vitamin E in homeostasis relevant to primary open-angle glaucoma. Br J Nutr 91:809–900
Coleman AL, Stone KL, Kodjebacheva G et al (2008) Glaucoma risk and the consumption of fruits and vegetables among older women in the study of osteoporotic fractures. Am J Ophthalmol 145:1081–1089
Frank RN (2004) Diabetic retinopathy. N Engl J Med 350:48–58
Hammes HP, Bertram B, Bornfeld N et al (2004) Diagnostik, Therapie und Verlaufskontrolle der diabetischen Retinopathie und Makulopathie. In: Scherbaum WA, Kiess W (eds) Evidenzbasierte Leitlinie der Deutschen Diabetes-Gesellschaft (DDG). www.deutsche-diabetes-gesellschaft.de/leitlinien/EBL_Retinopathie_Update_2004.pdf
Brazionis L, Rowley K, Itsiopoulos C, O’Dea K (2009) Plasma carotenoids and diabetic retinopathy. Br J Nutr 101:270–277
Delank H-W, Gehlen W (2004) Neurologie. Georg Thieme Verlag, Stuttgart
Wittchen HU, Jacobi F, Rehm J et al (2011) The size and burden of mental disorders and other disorders of the brain in Europe 2010. Eur Neuropsychopharamcol 21:655–679
Ferri CP, Prince M, Brayne C, For Alzheimer‘s Disease International et al (2005) Global prevalence of dementia: a Delphi consensus study. Lancet 366:2112–2117
Qiu C, De Ronchi D, Fratiglioni L (2007) The epidemiology of the dementias: an update. Curr Opin Psychiatry 20:380–385
Whitmer RA, Gunderson EP, Barrett-Connor E et al (2005) Obesity in middle age and future risk of dementia: a 27 year longitudinal population based study. BMJ 330:1360–1362
Kuslansky G, Katz M, Verghese J et al (2004) Detecting dementia with the Hopkins verbal learning test and the mini-mental state examination. Arch Clin Neurol 19:89–104
Ortega RM, Requejo AM, Andres P et al (1997) Dietary intake and cognitive function in a group of elderly people. Am J Clin Nutr 66:803–809
Lee L, Kang SA, Lee HO et al (2001) Relationships between dietary intake and cognitive function level in Korean elderly people. Public Health 115:133–138
Hogervorst E, Sadjimim T, Yesufu A et al (2008) High tofu intake is associated with worse memory in elderly Indonesian men and women. Dement Geriatr Cogn Disord 26:50–57
Morris MC, Evans DA, Tangney CC et al (2006) Associations of vegetable and fruit consumption with age-related cognitive change. Neurology 67:1370–1376
Kang JH, Ascherio A, Grodstein F (2005) Fruit and vegetable consumption and cognitive decline in aging women. Ann Neurol 57:713–720
Nooyens AC, Bueno-de-Mesquita HB, van Boxtel MP et al (2011) Fruit and vegetable intake and cognitive decline in middle-aged men and women: the Doetinchem cohort study. Br J Nutr 106:752–761
Dai Q, Borenstein AR, Wu Y et al (2006) Fruit and vegetable juices and Alzheimer’s disease: the Kame project. Am J Med 119:751–759
Barberger-Gateau P, Raffaitin C, Letenneur L et al (2007) Dietary patterns and risk of dementia: the three-city cohort study. Neurology 89:1921–1939
Hughes TF, Andel R, Small BJ et al (2010) Midlife fruit and vegetable consumption and risk of dementia in later life in Swedish twins. Am J Geriatr Psychiatry 18:413–420
Ritchie K, Carrière I, Ritchie CW et al (2010) Designing prevention programmes to reduce incidence of dementia: prospective cohort study of modifiable risk factors. BMJ 341:c3885
WCRF (World Cancer Research Fund) (2007) Food, nutrition, physical activity, and the prevention of cancer: a global perspective. World Cancer Research Fund/American Institute for Cancer Research, Washington, DC
Graham I, Atar D, Borch-Johnsen K et al (2007) European guidelines on cardiovascular disease prevention in clinical practice: executive summary: fourth joint task force of the European Society of Cardiology and Other Societies on cardiovascular disease prevention in clinical practice (constituted by representatives of nine societies and by invited experts). Eur Heart J 28:2375–2414
Dossus L, Kaaks R (2008) Nutrition, metabolic factors and cancer risk. Best Pract Res Clin Endocrinol Metabol 22:551–571
Hursting SD, Lashinger LM, Wheatley KW et al (2008) Reducing the weight of cancer: mechanistic targets for breaking the obesity–carcinogenesis link. Best Practe Res Clin Endocrinol Metabol 22:659–669
Calder PC, Ahluwalia N, Brouns F et al (2011) Dietary factors and low grade inflammation in relation to overweight and obesity dietary factors and low grade inflammation in relation to the metabolic syndrome. Brit J Nutr 106(S3):S1–S78
Bhupathiraju SN, Tucker KL (2011) Greater variety in fruit and vegetable intake is associated with lower inflammation in Puerto Rican adults. Am J Clin Nutr 93:37–46
Wright ME, Park Y, Subar AF et al (2008) Intakes of fruit, vegetables, and specific botanical groups in relation to lung cancer risk in the NIH–AARP diet and health study. Am J Epidemiol 168:1024–1034
Büchner FL, Bueno-de-Mesquita HB, Linseisen J et al (2010) Fruits and vegetables consumption and the risk of histological subtypes of lung cancer in the European prospective investigation into cancer and nutrition (EPIC). Cancer Causes Control 21:357–371
Büchner FL, Bueno-de-Mesquita HB, Ros MM et al (2010) Variety of fruit and vegetable consumption and the risk of lung cancer in the European prospective investigation into cancer and nutrition. Cancer Epidemiol Biomarkers Prev 19:2278–2286
Bingham S, Luben R, Welch A et al (2008) Associations between dietary methods and biomarkers, and between fruits and vegetables and risk of ischaemic heart disease, in the EPIC Norfolk cohort study. Int J Epidemiol 37:978–987
Open Access
This article is distributed under the terms of the Creative Commons Attribution License which permits any use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
Author information
Authors and Affiliations
Corresponding author
Additional information
The German Nutrition Society initiated this review and convened the working group.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 2.0 International License (https://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Boeing, H., Bechthold, A., Bub, A. et al. Critical review: vegetables and fruit in the prevention of chronic diseases. Eur J Nutr 51, 637–663 (2012). https://doi.org/10.1007/s00394-012-0380-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00394-012-0380-y