
Abstract
Introduction
Immobilization in external rotation after a first-time traumatic anterior shoulder dislocation has been shown to improve the position of the labroligamentous lesion relative to the glenoid rim. The purpose of the present study was to evaluate the effect of the external rotation position of the shoulder on different types of labroligamentous lesions in patients with first-time traumatic anterior shoulder dislocation by using MRI.
Patients and methods
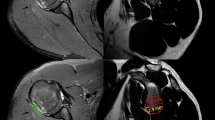
We performed a standardized MRI in internal and external rotation of the shoulder after initial reduction in 34 patients with a first-time traumatic anterior shoulder dislocation. Labroligamentous lesions were classified as Bankart, Perthes, or nonclassifiable. Four distinct grades were used to classify the amount of plastic deformation of the anterior labroligamentous structures. The position of the labrum was defined relative to the tip of the glenoid rim by measuring the dislocation and separation.
Results
In all patients, dislocation and separation of the labrum relative to the rim of the glenoid were significantly improved in shoulders in the external rotation position compared to those in the internal rotation position. We observed 15 Bankart, 15 Perthes, and 4 non-classifiable lesions. No HAGL or GLAD lesions were found. Fourteen patients showed a plastic deformation grade I, 16 showed grade II, 3 showed grade III, and 1 showed grade IV. In regression analysis, the odds ratio was 1.100 for the type of lesion and 1.660 for the grade of plastic deformation. Perthes lesions (with an intact anterior scapular periosteum) and grade I plastic deformations showed the best labral reduction on the external rotation MRI.
Conclusion
Placing the shoulder in external rotation after a first-time traumatic shoulder dislocation, significantly improves the position of the labroligamentous lesion on the glenoid rim. Perthes lesions that showed a low grade of plastic deformation displayed better reduction in external rotation and then compared to Bankart or other lesions that showed a high grade of plastic deformation. In conclusion, immobilization of the shoulder after a first-time traumatic shoulder dislocation is most effective in patients with Perthes lesions that show low grade plastic deformation.



Similar content being viewed by others


References
Arciero RA (2000) Acute arthroscopic Bankart repair? Knee Surg Sports Traumatol Arthrosc 8:127–129
Arciero RA, Taylor DC (1998) Primary anterior dislocation of the shoulder in young patients. A ten-year prospective study. J Bone Joint Surg Am 80:299–300
Bankart ASB (1923) Recurrent or habitual dislocation of the shoulder joint. BMJ 2:1132–1133
Bankart ASB (1938) The pathology and treatment of recurrent dislocation of the shoulder joint. Br J Surg 26:23–29
Bigliani LU, Pollock RG, Soslowsky LJ, Flatow EL, Pawluk RJ, Mow VC (1992) Tensile properties of the inferior glenohumeral ligament. J Orthop Res 10:187–197
Bottoni CR, Wilckens JH, DeBerardino TM, D’Alleyrand JC, Rooney RC, Harpstrite JK (2002) A prospective, randomized evaluation of arthroscopic stabilization versus nonoperative treatment in patients with acute, traumatic, first-time shoulder dislocations. Am J Sports Med 30:576–580
De Baere T, Delloye C (2005) First-time traumatic anterior dislocation of the shoulder in young adults: the position of the arm during immobilisation revisited. Acta Orthop Belg 71:516–520
Habermeyer P, Magosch P, Lichtenberg S (2004) Shoulder instability. Classification and treatment. Orthopade 33:847–872
Hart WJ, Kelly CP (2005) Arthroscopic observation of capsulolabral reduction after shoulder dislocation. J Shoulder Elbow Surg 14:134–137
Hippocrates (1989) Injuries of the shoulder, dislocations. Clin Orthop Relat Res 246:4–7
Hovelius L, Augustini BG, Fredin H, Johansson O, Norlin R, Thorling J (1996) Primary anterior dislocation of the shoulder in young patients. A ten-year prospective study. J Bone Joint Surg Am 78:1677–1684
Itoi E, Hatakeyama Y, Urayama M, Pradhan RL, Kido T, Sato K (1999) Position of immobilization after dislocation of the shoulder. A cadaveric study. J Bone Joint Surg Am 81:385–390
Itoi E, Sashi R, Minagawa H, Shimizu T, Wakabayashi I, Sato K (2001) Position of immobilization after dislocation of the glenohumeral joint. A study with use of magnetic resonance imaging. J Bone Joint Surg Am 83:661–667
Itoi E, Hatakeyama Y, Kido T, Sato T, Minagawa H, Wakabayashi I (2003) A new method of immobilization after traumatic anterior dislocation of the shoulder: a preliminary study. J Shoulder Elbow Surg 12:413–415
Kroner K, Lind T, Jensen J (1989) The epidemiology of shoulder dislocations. Arch Orthop Trauma Surg 108:288–290
Lichtenberg S, Habermeyer P (2002) Operative arthroskopie des glenohumeralgelenkes. In: Habermeyer P (eds) Schulterchirurgie. Urban & Fischer, München, pp 237–271
McLaughlin HL, MacLellan DI (1967) Recurrent anterior dislocation of the shoulder. II. A comparative study. J Trauma 7:191–201
Miller BS, Sonnabend DH, Hatrick C, O’Leary S, Goldberg J, Harper W (2004) Should acute anterior dislocations of the shoulder be immobilized in external rotation? A cadaveric study. J Shoulder Elbow Surg 13:589–592
Mizuno N, Yoneda M, Hayashida K, Nakagawa S, Mae T, Izawa K (2005) Recurrent anterior shoulder dislocation caused by a midsubstance complete capsular tear. J Bone Joint Surg Am 87:2717–2723
Neviaser TJ (1993) The anterior labroligamentous periosteal sleeve avulsion lesion: a cause of anterior instability of the shoulder. Arthroscopy 9:17–21
Norlin R (1993) Intraarticular pathology in acute, first-time anterior shoulder dislocations: an arthroscopic study. Arthroscopy 9:546–549
Perthes G (1906) Über Operationen bei habitueller Schulterluxation. Dtsch Z Chir 85:199–227
Postacchini F, Gumina S, Cinotti G (2000) Anterior shoulder dislocation in adolescents. J Shoulder Elbow Surg 9:470–474
Rowe CR (1963) Anterior Dislocations of the Shoulder: Prognosis and Treatment. Surg Clin North Am 43:1609–1614
Rowe CR, Zarins B, Ciullo J (1984) Recurrent anterior dislocation of the shoulder after surgical repair. Apparent causes of failure and treatment. J Bone Joint Surg 66:159–168
Seybold D, Gekle C, Fehmer T, Pennekamp W, Muhr G, Kalicke T (2006) Immobilization in external rotation after primary shoulder dislocation. Chirurg 77:821–826
Speer KP, Deng X, Borrero S, Torzilli PA, Altchek DA, Warren RF (1994) Biomechanical evaluation of a simulated Bankart lesion. J Bone Joint Surg Am 76:1819–1826
Taylor DC, Arciero RA (1997) Pathologic changes associated with shoulder dislocations. Am J Sports Med 25:306–311
te Slaa RL, Wijffels MP, Brand R, Marti RK (2004) The prognosis following acute primary glenohumeral dislocation. J Bone Joint Surg Br 86:58–64
Waldt S, Burkart A, Imhoff AB, Bruegel M, Rummeny EJ, Woertler K (2005) Anterior shoulder instability: accuracy of MR arthrography in the classification of anteroinferior labroligamentous injuries. Radiology 237:578–583
Wintzell G, Haglund-Akerlind Y, Ekelund A, Sandstrom B, Hovelius L, Larsson S (1999) Arthroscopic lavage reduced the recurrence rate following primary anterior shoulder dislocation. A randomised multicentre study with 1-year follow-up. Knee Surg Sports Traumatol Arthrosc 7:192–196
Wintzell G, Hovelius L, Wikblad L, Saebo M, Larsson S (2000) Arthroscopic lavage speeds reduction in effusion in the glenohumeral joint after primary anterior shoulder dislocation: a controlled randomized ultrasound study. Knee Surg Sports Traumatol Arthrosc 8:56–60
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Seybold, D., Schliemann, B., Heyer, C.M. et al. Which labral lesion can be best reduced with external rotation of the shoulder after a first-time traumatic anterior shoulder dislocation?. Arch Orthop Trauma Surg 129, 299–304 (2009). https://doi.org/10.1007/s00402-008-0618-6
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-008-0618-6