
Abstract
Background
Physical activity appears to be inversely related to cancer risk, although the evidence is convincing for colon cancer only. As physical activity levels are difficult to measure in the general population, we aimed to investigate how physical activity influences cancer risk using a cohort of Norwegian world class athletes.
Methods
The cohort includes 3,428 athletes. Individual questionnaires gave information about physical activity and lifestyle variables until attained age. To elucidate the level of cancer risk, groups of athletes were compared to the general population (external comparisons) and to each other (internal comparisons).
Results
A slightly reduced risk of total cancer was observed in the cohort of athletes, but stronger effects were observed for subgroups. The risk reduction was most pronounced for lung cancer and for leukemia/lymphoma. In women, a threefold increased risk of thyroid cancer was observed.
Conclusion
This cohort of athletes seems to have a reduced risk of cancer. The beneficial association, however, is weak and may be attributed to healthy lifestyle as well as to physical activity. Prolonged strenuous exercise may also increase the risk of thyroid cancer in women.
Similar content being viewed by others


Introduction
During the last 2 decades, there has been a large focus on beneficial effects of physical activity on cancer development. The evidence of such an effect is convincing, however, for colon cancer only [1]. A probable inverse relationship has been established for postmenopausal breast cancer and endometrial cancer, whereas limited evidence exists for lung, pancreatic, and premenopausal breast cancer [1]. The consensus report from World Cancer Research Fund and American Institute of Cancer Research, which is based on the existing literature related to physical activity and cancer, suggests a continuous inverse relationship between physical activity and cancer, within the range of physical activity examined. The hypothesis of an inverse relationship has biological plausibility as physical activity is observed to influence several processes and mechanisms related to cancer development [2]. On the other hand, intense exercise maintained for prolonged periods is related to immune suppression and susceptibility to infections [3, 4], which has been associated with lymphoid cancer [5–7]. Several sport activities [8, 9] and strenuous exercise [10] have also been associated with an increased risk of testicular cancer in men. In women, excessive exercise can cause thyroid dysfunction [11, 12], which also might impact the risk of thyroid cancer [13].
As a high quality measurement of physical activity is difficult to determine over a long time period, the possible effects of physical activity on cancer might have been diluted. Elite athletes, however, is a group that in a structured way have performed exercise during adolescence and adulthood to reach the high performance level required within elite sports. Furthermore, they often also keep an active lifestyle at older ages. Hence, elite athletes should be well suited for investigations on the relationship between physical activity and cancer.
The present study aims to investigate whether physical activity influences cancer risk, using a cohort of Norwegian world class athletes. Previously observed inverse relationships between physical activity and cancer were explored, and the cancer forms of particular interest were thus colon, breast, endometrial, lung, pancreatic, and prostate cancer. Whether prolonged strenuous exercise can elevate the risk of malignant diseases was investigated focusing on lymphoma, leukemia, testicular cancer, and female thyroid cancer. Cancer rates in the athletes were compared with the general Norwegian population (external comparisons) as well as between subgroups of athletes (internal comparisons).
Materials and methods
Study cohort
The study cohort includes male and female Norwegian world class athletes. All have represented Norway in international championships (team or individual disciplines) or have been placed top 3 in national championships (individual disciplines only), during the period 1936–2006. All participants were active as senior athletes (age ≥ 17). The Olympians were identified from 2 publications of Olympic history [14, 15], including complete lists of all Norwegian participants. Other athletes were identified through discipline-specific annuals and ranking lists from the Norwegian Olympic and Paralympic Committee and Confederation of Sports (NIF), which were systematically and thoroughly examined to ensure a complete and valid recruitment of athletes. No athletes from the Paralympic side were included in this study. All Norwegian residents alive after 1 January 1960 have been assigned a unique personal identification number (PIN), which is in use in all national registers. Hence, only athletes alive in 1960 were included. The athletes’ identities were verified by the National Population Register, using the PIN. Altogether, 6,169 elite athletes were identified. Information about place of residence, vital status, and date of emigration were obtained through a linkage to the National Population Registry. In August 2007, all athletes with a Norwegian address were sent an inquiry to participate in the study and they were asked to fill in a questionnaire (n = 5,894). Non-respondents received a reminder after 6 weeks, in line with the permission given by the Regional Committee for Medical and Health research Ethics. For athletes who were deceased, the questionnaire was addressed to their next of kin (n = 416). The Directorate of Health and Social Affairs gave permission to include all deceased athletes in the study cohort, regardless of the relatives’ response.
According to Norwegian law, the athletes had to give their consent to participate before they were included into the study cohort. Of the invited, 2,466 persons were excluded from the study because: their registered addresses were incorrect (n = 321), they abstained from participation (n = 82), or they did not gave their consent (n = 2,063). In total, the study cohort included 3,428 athletes, of whom 3,012 were alive and 416 were deceased (Fig. 1).

The Norwegian elite athletes eligible for the cohort and the selections into the final study cohort. *NQ no questionnaire from relatives, **Q questionnaire from relatives
A questionnaireFootnote 1 was used to collect information about physical activity during childhood (ages 8–12), adolescence (ages 13–17), and during and after the sports career. For each period, they were asked to assign the number of hours (per week) spent on physical activity at clearly defined intensity levels, which were categorized as “low,” “medium,” and “high.” For later purposes, the athletes also were asked to report alcohol habits, tobacco use, educational level, anthropometric measures (during life), age at onset of puberty, parity, selected health problems of particular interest, menstrual status, and hormone use (women).
Physical activity assessment
This group of athletes is quite diverse with regard to discipline and, thus, exercise habits. To make more homogenous groups, all the athletes were included in 1 of 3 mutually exclusive categories according to their sports discipline: endurance, power/technique, or ball games, before any cancer information was retrieved. The endurance category consists of disciplines that require frequent activity at high intensity levels (i.e., cross country skiing, alpine skiing, biking, skating, swimming, long distance running, and rowing). The ball game category, which includes all kinds of ball sports, is associated with frequent activity at more moderate intensity levels. The power/technique category consists of disciplines that widely vary regarding type of activity and intensity level: track and field (throw, jump, sprint, and hurdle), golf, sailing, diving, snowboard, freestyle, combat sports, and weight lifting.
During the last decades, the exercise levels among athletes have increased to meet the elevated requirements within elite sports. The athletes were thus categorized in 2 subgroups: career period <1975 and ≥1975.
According to their questionnaire answers about physical activity (frequency and intensity level) from childhood until attained age, the athletes were categorized into 1 of 3 mutually exclusive levels of lifetime physical activity: low, medium, or high. The low level included athletes who reported an exercise practice of less than 4 h per week and mainly at low intensity level. Athletes who reported a more frequent exercise practice (4–8 h per week) at higher intensity levels were included in the moderate level. Athletes who reported to exercise more than 8 h per week and mainly at high intensity levels were included in the highest level of lifetime activity. Athletes with incomplete (n = 125) or without (n = 265) questionnaire response were included in a category named “unknown.”
Cancer information
Cancer information was obtained by a linkage to the Cancer Registry of Norway. All incident cancer cases in Norway have been registered in this national registry since 1952, and the reporting is compulsory. Start of follow-up for cancer was set to 1 January 1953, provided that the person was at least 18 years of age. Follow-up ended at date of diagnosis, emigration, death, or 31 December 2007, whichever occurred first.
Statistical analyses
Two types of analyses were conducted. First, the cancer risk in the group of athletes was compared with the risk in the general population, when sex, age, and birth cohort were taken into account. This is an external comparison based on the standardized incidence ratio (SIR). The person-years at risk and the observed number of cancer cases were counted within 10-year age groups (20–29, 30–39,…, 70–79, 80+), separately for 6 calendar periods (1953–1961, 1962–1971, …, 2002–2007). The expected number of cancer cases was calculated by multiplying the number of person-years in each age group and calendar period in the study cohort by the corresponding cancer incidence rates in the general Norwegian population during the period of observation. The 95% confidence interval (CI) for the SIR was based on the assumptions that the observed number of cases was Poisson-distributed, and the expected number was non-stochastic. Secondly, the risk of total cancer was internally compared between subgroups of athletes within the study cohort. Poisson regression analysis was used to estimate incidence rate ratios (IRRs), where sex, attained age, and calendar period were taken into account. All statistical analyses were conducted in STATA [16]. A 5% level of statistical significance was used.
Results
Table 1 presents the distribution of Norwegian world class athletes according to sex, discipline category, and time period of sports career. No obvious selection into the study cohort is seen as the athletes were distributed similarly in the invited and the identified cohorts. The proportion of participants from the most recent career period was slightly reduced in the study cohort, compared to the cohorts of invited and identified athletes.
Table 2 gives the distribution of athletes in the study cohort according to characteristics based on information from the questionnaire. The educational levels in the athletes were distributed in a similar way as the general population [17]. The majority of the athletes reported to be never users of tobacco (smoke/snuff), who constituted a larger proportion than never users in the general population [18]. The intake of alcohol in the athletes was similar as in the general population [19]. The age at onset of voice change/beard growth or menarche was used to indicate the age of puberty in men and women, respectively. Compared to the general female population [20], the athletes had a higher median age at onset of menarche (0.6 years). As far as we know, there exists no descriptive documentation on onset of male puberty in Norway.
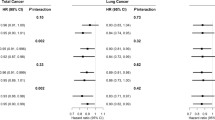
Table 3 shows the observed number of cancer cases and the SIRs for the selected cancer forms studied. Altogether, 266 cancer cases occurred during follow-up. Relative to the general Norwegian population, the cohort of athletes was shown to have a slightly reduced risk of total cancer. A stronger risk reduction was seen for lung cancer, and also the risk of leukemia/lymphoma tends to be reduced. Sex specific SIRs revealed a threefold risk of thyroid cancer in women. In men, a significant risk reduction was seen for total cancer and lung cancer. Table 3 also presents results from SIR analyses stratified by the discipline categories. In female endurance athletes, no significant differences in cancer risk were observed, compared to the general women. In men, significant risk reductions were seen for total cancer and lung cancer, but the risks of testicular and pancreatic cancer tend to be elevated. In the technique/power category, no influence of being an athlete was observed, except for the strongly elevated risk of thyroid cancer in women. Compared to the general population, the ball game practitioners were shown to have a reduced risk of total cancer, however, not significant for women. Analyses including both sexes show a reduced risk for colon cancer and for leukemia/lymphoma, although few cancer cases were present.
External analyses stratified by levels of lifetime activity were also performed (not shown). The results revealed no influence of being an athlete in the low level of lifetime activity, when compared to the general population. For the medium activity level, a significant reduced risk of total cancer was observed, in men (40%) and women (35%). Also the risk of lung cancer (80%) and leukemia/lymphoma (65%) was significantly reduced. In women, a fourfold risk increase was seen for thyroid cancer. No significant differences in cancer risk were observed between the general population and athletes in the highest level of lifetime activity, except for a reduced risk of total cancer in men (40%).
Table 4 presents results from internal analyses, comparing risk of total cancer between the subgroups of athletes. The results support the observation from the external analyses, indicating a lower cancer risk in the subgroup of ball game athletes. The Poisson regression analyses, however, did not confirm any differences between athletes in the 2 career periods, <1975 and ≥1975. A reduced risk of total cancer was seen for athletes in the medium or high level of lifetime activity, compared to athletes in the low level category, although, not significant for women. The results for the “unknown” category, mainly consisting of deceased athletes, showed a significantly elevated risk of total cancer, for both sexes. However, when excluding athletes with an unknown lifetime activity level from the analyses, the estimates remained almost unchanged (not shown).
Discussion
Lifetime physical activity is difficult to measure. Although occupations, interviews, and questionnaires have been the available tools to measure activity levels in epidemiological studies, the misclassification problem is considerable. In this cohort study, only athletes at a world class level were included, which ensures a study population that has performed prolonged systematic exercise. The levels of physical activity were assessed by using individual information about sports discipline and career period, received from NIF, and the risk of misclassification should thus be low.
Through the questionnaire, information about lifetime activity was collected. This subjective reporting, over a long time span, represents a risk of misclassification when the lifetime activity levels were to be assessed. Furthermore, the major part of the deceased athletes was categorized as “unknown” in this regard, as the relatives had poor information about their lifetime activity. Possible misclassifications make it difficult to interpret the results from this variable. Hence, less impact has been put on these results, although they seem to support the associations observed between the discipline categories and cancer risk.
According to Norwegian law, the athletes (alive) had to give their consent to be included into the study and, hence, the cohort only includes 58.2% of the invited athletes. This did, however, not appear to introduce major selection bias according to sex, sports discipline, or career period, as the distribution of participants was similar to that of the invited and identified cohorts (Table 1). Other selections, however, might be present, as different groups could have different motivation for participation and a higher participation of previous patients with cancer, for instance, would aggregate the number of cancer cases. As we were allowed to include all deceased athletes, the incidence rates between deceased athletes, with and without responding relatives, were compared, as a help to understand the possible selection. No difference was, however, observed between the 2 groups (not shown). As athletes live healthier than the average population and often keep up healthy habits into older ages [21], our inclusion criterion might have selected a particularly healthy population into the study. This selection might be strengthened by the fact that a serious illness early in life decreases a person’s possibility to become an elite athlete. Due to possible selection, it might be difficult to separate between potential effects of physical activity and effects from other variables related to a healthy lifestyle.
Colon cancer is inversely related to physical activity, with a dose–response relationship, and several mechanisms by which physical activity may be protective are suggested [1]. In the present study, comparing world class athletes with the general population, no significant risk reduction was seen, except for the subgroup of ball game athletes (Table 3). In 2000, Pukkala and colleagues presented results from a cohort study of Finnish male athletes [22]. Neither did they observe any reduced risk of colon cancer among elite athletes. In a large cohort study from the European Prospective Investigation into Cancer and Nutrition, daily activity at vigorous intensity levels were suggested to be the activity pattern that prevent colon cancer [23]. The activity levels categorized as vigorous in general populations may fit well with the activity pattern in ball game sports, and the apparent beneficial result seen for this subgroup may support the conclusion by Friedenreich et al. [23].
A large number of studies have investigated the role of physical activity in the etiology of breast cancer, and the results vary according to different subgroups of women [24]. In the present study, no significant risk differences were seen between the female athletes and the general population. Physical activity is mainly suggested to protect against postmenopausal breast cancer [1]. In the present study, however, separate analyses according to menopausal status were not performed, as the women mainly reported to be in a premenopausal stage (73.2%). The mechanisms by which physical activity protect against breast cancer are related to endogenous steroid hormone metabolism, and a factor in this regard is a delayed age at onset of menarche [25]. Although the women seem to be delayed regarding menarcheal age (Table 2), no reduced risk of breast cancer was seen. The female athletes also seem to differ from the general population with regard to parity pattern. As close to 40% of the female athletes were nulliparous and the age at first childbirth apparently seem to be delayed, this might eliminate the potential beneficial effect of physical activity.
Physical activity is also suggested to protect against endometrial cancer, through mechanisms that regulate body fat and sex hormone metabolism [1]. However, only 3 cases were observed in the present study and, hence, no conclusion can be drawn.
Lung cancer is principally attributed to smoking [26]. However, physical activity is suggested to influence the risk of this malignancy [27, 28]. Physical activity improves ventilation and perfusion of the lungs and, thus, reduces the concentration of carcinogens in the airways and the duration of potential adverse exposure [27]. In the present study, a low risk of lung cancer was seen, in particular in men, in line with the low percentage of ever smokers reported (Table 2). Similar results were observed in the study by Pukkala and colleagues, who also observed a reduced risk of other smoking related cancer forms [22]. The low proportion of ever smokers might be a reasonable explanation of the reduced risk seen in the present study.
Extensive physical activity has been linked to immunosuppressive mechanisms and increased susceptibility to infections [3, 29]. Mononucleosis from Epstein–Barr virus infections has been related to the risk of lymphoma [6, 7]. In the present cohort, 8.2% of the athletes reported an episode of mononucleosis, which may indicate a high susceptibility to infections. Nevertheless, the risk of leukemia/lymphoma tended to be reduced in all subgroups of athletes, but significant for the ball game category only. Prolonged strenuous physical activity may influence the risk of these malignancies in a beneficial way rather than adverse. Similar associations have previously been observed [30, 31], although no biological explanation has been suggested. However, this observation should be further investigated before any conclusion can be drawn.
A threefold increased risk of thyroid cancer was observed in the female athletes, although the number of cancer cases was small. The highest risk was seen in the technique/power category, but the increased risk pattern was consistent for all the female subgroups. Few strong risk factors have been identified for this disease, except for irradiation and benign thyroid diseases [12], and physical activity has inversely been related to this malignancy [32]. Endurance exercise is, however, also observed to cause hypothyroidism [11, 12], which has been suggested to influence the cancer risk [13]. In the present study, a relatively high frequency of thyroidal dysfunction symptoms was reported (n = 48), which supports a potential association between physical activity and thyroidal stress. Thyroid dysfunction caused by strenuous physical activity may thus be a possible explanation of the elevated cancer risk observed. Further investigations are, however, required before any conclusions can be drawn.
Testicular cancer has been associated with strenuous exercise during adolescence [10] and sports disciplines related to trauma or injuries [8, 9]. In the present study, the male endurance athletes tend to have an elevated risk of this malignancy. Although none of these cancer cases belong to sports disciplines associated with trauma or injuries, they certainly have performed strenuous exercise during adolescence. As cryptorchidism and inguinal hernias [33] are factors strongly associated with testicular cancer, information on these conditions was analyzed. However, no differences were observed that could explain the probable increased risk in the endurance athletes. We are aware of the low number of cases present, and the result might thus be spurious.
For prostate cancer, the relation to physical activity is rather unclear [1], and the present study did not reveal further clarification as no differences in risk of prostate cancer were seen between the athletes and the general population. Physical activity is suggested to reduce the risk of pancreatic cancer [34], but no further clarification was revealed here. Although a twofold risk of pancreatic cancer was observed in male endurance athletes, further investigation is required to clarify whether strenuous activity influences the risk of this malignancy.
To conclude, the risk of total cancer was only slightly reduced in this cohort of world class athletes compared to the general population. Stronger effects were observed for total cancer and specific cancer forms when analyzing subgroups of athletes separately. The ball game category seems to have the lowest cancer rates. The observed decrease in cancer risk may be attributed to a healthy lifestyle as well as to physical activity. Female athletes, however, seem to have an elevated risk of thyroid cancer. As the results may be valid for this study cohort only, the associations should be investigated in similar and larger cohorts.
Notes
The questionnaire is available upon request.
References
World Cancer Research Fund/American Institute of Cancer Research (2007) Physical activity. In: Nutrition, physical activity and the prevention of cancer, a global perspective. Washington DC: AICR, pp. 198–209
Friedenreich CM (2001) Physical activity and cancer prevention: from observational to intervention research. Cancer Epidemiol Biomarkers Prev 10:287–301
MacKinnon LT (2000) Chronic exercise training effects on immune function. Med Sci Sport Exerc 32(Suppl):S369–S376
Pedersen BK, Hoffman-Goetz L (2000) Exercise and the immune system: regulation, and adaption. Physiol Rev 80:1055–1081
Zahm S, Hoffman-Goetz L, Docemeci M, Kantor KP, Blair A (1999) Occupational physical activity and Non-Hodgkin’s lymphoma. Med Sci Sports Exerc 31:566–571
Kvale G, Hoiby EA, Pedersen E (1979) Hodgkin’s disease in patients with previous infectious mononucleosis. Int J Cancer 23:593–597
Chang ET, Zheng T, Weir EG et al (2004) Childhood social environment and Hodgkin’s lymphoma: new findings from a population-based case–control study. Cancer Epidemiol Biomarkers Prev 13:1361–1370
Coldman AJ, Elwood JM, Gallagher RP (1982) Sports activities and risk of testicular cancer. Br J Cancer 46:749–756
Gallagher RP, Huchcroft S, Phillips N et al (1995) Physical activity, medical history, and risk of testicular cancer. Cancer Causes Control 6:398–406
Srivastava A, Kreiger N (2000) Relation of physical activity to risk of testicular cancer. Am J Epidemiol 151:78–87
Boyden TW, Pamenter RW, Rotkis TC, Stanforth P, Wilmore JH (1984) Thyroidal changes associated with endurance training in women. Med Sci Sports Exerc 16:243–246
Boyden TW, Pamenter RW, Stanforth P, Rotkis T, Wilmore JH (1982) Evidence for mild thyroidal impairment in women undergoing endurance training. J Clin Endocr Metab 54:53–56
Franceschi S, Preston-Martin S, Dal Maso L et al (1999) A pooled analysis of case–control studies of thyroid cancer. IV. Benign thyroid diseases. Cancer Causes Control 10:583–595
Dalby Å, Greve J, Jorsett P (2004) Norwegian participants in Olympic Games. In: Olympic Summer Games 1896–2004 (Norwegian). Oslo: Akilles, NIF, pp. 281–323
Dalby Å, Greve J, Jorsett P (2006) Norwegian participants in Olympic games. In: Olympic Winter Games 1924–2006 (Norwegian). Oslo: Akilles, NIF, pp. 505–548
StataCorp (2007) Stata Statistical Software: Release 10. StataCorp LP, College Station
Statistics Norway (2008) Official statistics of Norway. Statistics Norway, Oslo, p 183
Statistics Norway (2009) Smoking habits in Norway (in Norwegian). Statistics Norway, Oslo
Horverak Ø, Bye E (2007) Alcohol habits in Norway 1973–2004 (In Norwegian). SIRUS report nr 2/2007
Liestøl K, Rosenberg M (1995) Height, weight and menarcheal age of schoolgirls in Oslo—an update. Ann Hum Biol 22:199–205
Sarna S, Kaprio J, Kujala UM, Koskenvuo M (1997) Health status of former elite athletes. The Finnish experience. Aging 9:35–41
Pukkala E, Kaprio J, Koskenvuo M, Kujala U, Sarna S (2000) Cancer incidence among Finnish world class male athletes. Int J Sports Med 21:216–220
Friedenreich CM, Norat T, Steindoef K et al (2006) Physical activity and risk of colon and rectal cancers: the European prospective investigation into cancer and nutrition. Cancer Epidemiol Biomarkers Prev 15:2398–2407
Friedenreich CM, Cust AE (2009) Physical activity and breast cancer risk: impact of timing, type and dose of activity and population subgroup effect. Br J Sports Med 42:636–647
Bernstein L (2002) Epidemiology of endocrine-related risk factors for breast cancer (review). J Mammary Gland Biol Neoplasia 7:3–15
Parkin DM, Pisani P, Lopez AD, Masuyer E (1994) At least one in seven cases of cancer is caused by smoking. Global estimates for 1985. Int J Cancer 59:494–504
Thune I, Lund E (1997) The influence of physical activity on lung-cancer risk. A prospective study of 81, 516 men and women. Int J Cancer 70:57–62
Mao Y, Pan S, Wen SW, Johnson KC (2003) Physical activity and the risk of lung cancer in Canada. Am J Epidemiol 158:564–575
Reid VL, Gleeson M, Williams N, Clancy RL (2009) Clinical investigation of athletes with persistent fatigue and/or recurrent infections. Br J Sports Med 38:42–45
Paffenberger RS, Lee I-M, Wing AL (1992) The influence of physical activity on the incidence of site-specific cancers in college alumni. In: Jacobs MM (ed) Exercise, calories, fat, and cancer. Plenum Press, New York
Keegan TH, Glaser SL, Clarke CA et al (2006) Body size, physical activity, and risk of Hodgkin’s lymphoma in women. Cancer Epidemiol Biomarkers Prev 15:1095–1101
Rossing MA, Remler R, Voigt LF, Wicklund KG, Daling JR (2001) Recreational physical activity and risk of papillary thyroid cancer (United States). Cancer Causes Control 12:881–885
Garner MJ, Turner MC, Ghadirian P, Krewski D (2005) Epidemiology of testicular cancer: an overview. Int J Cancer 116:331–339
Bao Y, Michaud DS (2008) Physical activity and pancreatic cancer risk: a systematic review. Cancer Epidemiol Biomarkers Prev 17:2671–2682
Acknowledgments
We address sincere thanks to all the Norwegian athletes who participated in this study. The Norwegian Olympic and Paralympic Committee and Confederation of Sports and Akilles Publisher are gratefully acknowledged for cooperation and contributions that made the data collection possible. In particular, we acknowledge the authors of the Norwegian Olympic history books with identification of all the Norwegian Olympians: Aage Dalby, Jan Greve, and Per Jorsett. Furthermore, we owe gratitude to several sports veterans and local sports clubs for invaluable contributions in the athlete identification process.
Financial support
This study was funded by The Norwegian Cancer Society.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Robsahm, T.E., Hestvik, U.E., Veierød, M.B. et al. Cancer risk in Norwegian world class athletes. Cancer Causes Control 21, 1711–1719 (2010). https://doi.org/10.1007/s10552-010-9600-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10552-010-9600-z