
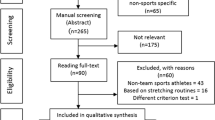
Abstract
Purpose of Review
We reviewed the occurrence of outbreaks at past Olympics and discuss the threat of the COVID-19 pandemic at the Tokyo Games.
Recent Findings
Evidence for large respiratory tract infection outbreaks at past Olympics is scant. Nevertheless, in order to control the spread of the COVID-19 outbreak, the Tokyo 2020 Olympics were postponed for 2021. Given the high contagiousness of the disease and the epidemiology of COVID-19 in Japan, this decision was appropriate and important in order to safeguard athletes and the public. However, it is a major problem for Japan, involving massive financial losses and a lost opportunity for athletes, coaches, and instructors.
Summary
Up-to-date epidemiological data is needed on which to base an appropriate decision regarding the Tokyo 2021 Olympics. The actual effect of cancellations of such events in reducing the spread of COVID-19 needs to be determined.
Similar content being viewed by others


Introduction
Mass gatherings (MGs) are defined as a “concentration of people at a specific location for a specific purpose over a set period of time which has the potential to strain the planning and response resources of the country or community” [1]. MGs can be spontaneous or programmed and irregular or recurrent [1]. Sporting, religious, and cultural events such as the Olympic Games, the Hajj, and music festivals are programmed MGs [1]. MGs pose considerable public health challenges to health authorities and host governments, not only in regard to transmissible disease but also noncommunicable disease, such as trauma or injuries. In addition, illness related to the use of drugs and alcohol and environmental effects are well described as public health problems during certain types of MGs [1]. Infectious disease is one of the major challenges at MGs, as it affects the attendees during the event and can increase the load on the health system in the host country. In addition, infected participants may spread the disease on a large scale upon return to their home countries. In fact, several MGs have been identified as the source of infectious diseases that have spread globally [2•]. Among the infectious diseases, respiratory tract infections (RTIs) are particularly frequent at MGs, due to the inevitable overcrowding and nature of its mode of transmission [2•, 3, 4].
Recently, a novel coronavirus named SARS-CoV-2 emerged in Wuhan city, Hubei province, China, causing an outbreak of a respiratory infectious disease (COVID-19). The outbreak has spread rapidly and widely throughout the world. The World Health Organization (WHO) declared the event a Public Health Emergency of International Concern (PHEIC) on January 30, 2020, and a pandemic on March 12, 2020 [5]. At the time of writing, the COVID-19 pandemic has accounted for 20,812,367 confirmed cases and 747,327 deaths in 213 countries and territories around the world [6].
As part of efforts to control the spread of the COVID-19 pandemic, several important MGs events have been cancelled worldwide since early March 2020, including international and national sporting, religious, cultural, and other MGs. Many prominent sporting events with millions of participants have been cancelled or postponed, such as the Formula 1 Grand Prix in China, the Euro 2020 football championship, the Six Nations rugby championship in Italy and Ireland, the Mobile World Congress in Barcelona, and Olympic boxing qualifying events [7]. The 2020 Summer Olympics and Paralympics in Japan were originally scheduled to take place from July 24 to August 9, 2020, and from August 25 to September 6, 2020, respectively. Finally, it was halted in March 2020 because of the COVID-19 pandemic [8]. This international multisport event is now planned for July 23 to August 8, 2021 (Olympics), and August 24 to September 5, 2021 (Paralympics) in Tokyo, Japan. As with many other MGs events, the Tokyo 2020 Olympics would have been a significant opportunity for dispersing pathogens, especially SARS-CoV-2. We review the occurrence of infectious diseases at past Olympic Games, with a special focus on the threat of the COVID-19 pandemic at the Tokyo games.
An Overview of Infectious Diseases at the Olympic Games
Infectious diseases have been frequently reported in religious events like the Hajj, one of the largest religious MGs worldwide, and music festivals. But no strong evidence for a significant increase of infectious disease outbreak during sporting events has been identified [9]. Only a few RTI and gastrointestinal infection outbreaks were found in a review of Gautret et al., which included the Summer and Winter Olympics from 1984 through 2015 [9]. In the 2002 Winter Olympics in Salt Lake City, 36 cases of influenza among participants were recorded [10]. During the Vancouver 2010 Winter Olympics in Canada, an epidemic with 82 cases of measles occurred [11]. No major public health incidents occurred during the London 2012 Olympic Games. Only a few cases of RTIs and gastrointestinal illness were reported during this event, but no food-borne illness was directly linked to a Games venue [12]. During the London 2012 Olympics, a total of 47 sexually transmitted infections were diagnosed in 289 visitors, including 8 chlamydia and 15 nonspecific genital infections. There were no new cases of HIV or syphilis diagnosed [13]. During the Sochi 2014 Winter Olympics in Russia, 249 illnesses were reported among the 2788 athletes (the incidence was 8.9 illnesses per 100 athletes). Of those, 58% were caused by infectious diseases. RTIs were the most frequent (63.9%), followed by gastrointestinal symptoms (11%) [14].
The Rio de Janeiro 2016 Olympic Summer Games in Brazil included 11,274 athletes from 207 countries. During this event, 613 illnesses were reported. Infectious diseases affected 56% of ill individuals. RTIs and gastrointestinal symptoms were the most common and occurred in 202 (47%) and 131 individuals (21%), respectively [15]. Although the Rio de Janeiro 2016 Olympics took place during the time of a Zika outbreak, no cases of Zika virus were detected among the athletes and attendees [16, 17].
In 2018, the Pyeong Ghang Winter Olympics in South Korea had the highest number of athletes (2920) and participating countries (92) in the history of the Winter Olympics [18•]. During this event, the most common cause of illness was RTIs [18•, 19•]. A total of 1639 athletes consulted polyclinics, including 1402 (85.5%) visits for illness, with 107 cases of upper RTIs. Common cold was also observed in 42 of 112 members of the Finland team [20]. The etiology of the RTIs was detected in 30 of 42 patients by multiplex-PCR, with 9 different respiratory viruses identified. Human coronavirus (HCoV) 229E (11 cases) was the most frequent, followed by HCoV NL63, influenza B, human rhinovirus, respiratory syncytial virus type A, and metapneumovirus (5 cases). The survey showed that the viral infections spread easily within the same sport discipline or the team. In addition, co-infections were also common [20]. Also, during the Pyeong Ghang 2018 Winter Olympics, a norovirus outbreak emerged a few days before the event began. This outbreak affected 172 volunteers staying at hostels but only 4 athletes [18•].
Large RTI outbreaks were rarely reported at previous Olympic Games. This can be explained by the fact that the participants move to other locations at the end of an event and do not live on site, contrary to large religious MGs. Furthermore, the duration of each sport event is short (less than 1 day) [9,10,11,12,13,14,15,16,17, 18•].
Olympic Game Massive Gatherings and Risk Assessment for Dissemination of COVID-19
Unlike the case of Zika virus during the 2016 Summer Olympics in Rio de Janeiro, the SARS-CoV-2 virus is transmitted by the respiratory route and can be easily transmitted between humans. The reproduction number R (R0) of SARS-CoV-2 is estimated up to 4.1 [21,22,23]. In comparison with the SARS-CoV and influenza virus, SARS-CoV-2 is more transmissible [24•]. In addition, the strong infectivity of SARS-CoV-2 and rapid transmission even from asymptomatic carriers during the long incubation period have been previously described [25]. Because the incubation period of the virus is long (up to 14 days) [26], controlling viral dispersion seems to be difficult. The Tokyo Olympic Games were supposed to receive 20 million non-residents visitors from 204 countries and regions [27••, 28], and the stadiums would have been overcrowded. The relatively close contact between participants, including athletes and staff, spectators, and journalists, could increase the spread of COVID-19. Moreover, there was a high risk of globalization of virus transmission by travellers. Screening at airports is feeble, and nearly 46% of infected travellers cannot be identified [29]. Body temperature is ineffective for screening SARS-CoV-2 among young adult travellers; only 18% of COVID-19 cases present a fever of 38 °C [30].
Currently, the risk of a rebound of COVID-19 in the near future is worrisome in several countries [21], including Japan. Figure 1 shows the two waves of COVID-19 in Japan. The number of new daily cases in the second wave tends to be higher than the first wave. COVID-19 new daily cases varied from 853 to 1998 during the planned periods of the Tokyo 2020 Olympics (from July 24 to August 9, 2020) (Fig. 1) [6].

COVID-19 pandemic in Japan [6]
Regarding athletes, they are viewed as being fit and healthy, but this might not be accurate [31]. The overtraining syndrome and high glycemic diet are often associated with chronic diseases. Those with chronic diseases are more susceptible to SARS-CoV-2 infection and aggravation or complications of COVID-19 [5]. Athletes are exposed to a higher risk of infection because of their compromised immune system [31,32,33]. Pedersen et al. conducted a study on the relationship between immune depression and infection among athletes [34]. After exercise, athletes have a transitory “open window” effect of immune depression lasting 3 to 72 h. This period makes the host more susceptible to infection from several microorganisms and potentially increases the risk for SARS-CoV-2 infection [35••].
Paralympics athletes are exposed to more risks for infectious disease, including RTIs [35••]. During the Rio 2016 Paralympics season, athlete delegations were approximately 60% physical-motor deficient, 25% visually impaired, and 5% intellectually disabled [35••]. They presented twice the amount of total illness in comparison to the Olympic athletes, and RTIs were the most frequent. Controlling disease in Paralympic athletes is relatively more complex. It is estimated that between 10 and 20% of these athletes are at risk of aggravating symptoms if they are infected by COVID-19 [35••].
Impact of the Cancellation of the Tokyo 2020 Olympic Games
In order to take measures to contain the spread of the COVID-19 pandemic, several national and international MGs, including sporting events, have been cancelled or postponed worldwide since early March 2020 [7]. The question of stopping the Tokyo 2020 Olympic was raised early [8]. On April 28, 2020, the President of the International Olympic Committee confirmed that the 2020 Olympic Games should be cancelled and postponed until 2021 [36]. The name of the event will remain unchanged: “Tokyo 2020 Olympic and Paralympic Games.” In the past, several Olympic Games have been cancelled by world wars, including the 1940 Tokyo Summer Olympics due to the onset of World War II [36]. Some Olympic Games have been held successfully despite global health crises, such as the Vancouver 2010 Winter Olympics during the H1N1 influenza pandemic and the Rio 2016 Olympics during the outbreak of Zika virus. This is the first time in the 124-year history of the modern Olympic Games that they have been postponed due to a medical issue.
The decision to postpone the Tokyo 2020 Olympic and Paralympic Games to 2021 was appropriate and important in order to safeguard the athletes as well as the public [37]. However, it is a major problem not only for the host country in terms of massive financial losses but also for the 11,000 Olympic and 4400 Paralympic athletes who were due to take part in this important sporting event mostly because of loss of opportunity [38••].
The cancelling of this event cost Japan 4.52 trillion yen (41.5 billion USD), based on operating expenses, considering maintenance expenditures for the unused facilities and loss of tourism activity.
Athletes have been directly affected by the decision to postpone the Tokyo 2020 Olympics due to the COVID-19 pandemic. The postponement of the 2020 Olympics automatically meant retirement and the permanent loss of opportunity for some [38••, 39]. Athletes have lost daily, weekly, monthly, and yearly workout routines, which affects their mental and physical state [38••]. The spread of COVID-19 forced nearly every training site to close and forced players to stay home. Social distancing measures have affected not only the Tokyo Olympic and Paralympic games but all other sporting events, including the cancellation of qualifying tournaments. These changes have increased feelings of uncertainty, confusion, and frustration and made it difficult to establish a specific set of goals [38••, 39, 40]. In addition, because of the limited opportunity to leave the house for systematic and intensive training, when players are allowed to train for shorter periods of time, they tend to overwork to maximize impact and that may increase the likelihood of injury. Limiting interactions with teammates, coaches, and others can also make athletes more anxious [38••, 40].
Coaches and instructors were another group affected by the COVID-19 outbreak. They had particular difficulty in coaching athletes. Also, they may not have been able to allocate enough energy and time to focus on the athlete’s conditions, because they needed to care for themselves and their families [38••].
Mandatory doping tests were severely limited by the COVID-19 outbreak in early 2020. European anti-doping organizations raised concerns that urine and blood tests could not be performed. Mobilizing the staff necessary to do so before the end of the pandemic may increase health risks. The World Anti-Doping Agency stated that public health and safety was their topmost priority despite the need for extensive testing [36]. Due to the COVID-19 outbreak, the Chinese anti-doping agency temporarily ceased testing in early February 2020. Also, the USA, Great Britain, France, and Germany anti-doping organizations had reduced their testing activities by the end of March 2020 [36]. That can significantly increase doubts about fair play in the Olympic Games.
Tokyo 2021 Summer Olympics, What Needs to Be Prepared in the Current State?
The President of the Japan Medical Association has been quoted as saying that the Tokyo Olympic Games can only be organized next year if an effective vaccine against COVID-19 is developed for public use and the pandemic is fully controlled, not only in Japan but worldwide. Regarding the current COVID-19 pandemic, it is certainly too early to predict whether the Tokyo Olympic Games will occur in 2021 or will once again be cancelled. SARS-CoV-2 surveillance should be maintained for a long time after the elimination of the initial pandemic [41]. However, this is an important sporting event in the world that only happens once every 4 years, so everyone hopes that it will take place as planned.
During this event, the movement of participants across frontiers and within the host country would most certainly intensify the spread of COVID-19 from one country to another, since travel is clearly one of the key contributors to disease globalization.
To date, there is no specific evidence available for planning and implementing a MG during the COVID-19 pandemic nor is there evidence for the effectiveness of individual mitigation actions for COVID-19 [42]. In collaboration with global partners involved in MGs health, the WHO made recommendations for sports event organizers regarding planning for MGs in the context of COVID-19 (Table 1) [43]. By complying with the existing WHO guidelines, governments can impose limits and minimize the spread of SARS-CoV-2 [44].
Detection and monitoring of MG-related COVID-19 cases should be carefully considered in the context of surveillance schemes, and enhanced surveillance is necessary. In collaboration with local health authorities, organizers should agree in advance about the circumstances in which risk mitigation measures would need to be reinforced. The host country must be prepared to provide adequate prevention measures and diagnostic capabilities. However, during the Games, there are about 14 million food dishes expected to be delivered to participants [37]. This represents a huge challenge for organizers, particularly as regards health security. And the control of COVID-19 will add to this burden.
Conclusion
Up-to-date epidemiological data is needed on which to base an appropriate decision regarding the Tokyo 2021 Olympic and Paralympic Games. If the pandemic continues and is uncontrolled, not only in Japan, but worldwide, or if there is no effective vaccine developed for public use, these events may remain cancelled. The cancellations have social and economic impacts on individual livelihoods, public morale, and on national economies. The effect of cancellations of these events on reducing the spread of COVID-19 needs to be determined. If a decision is made to proceed with the Olympic Games, risk mitigation measures must be put in place, consistent with WHO guidelines on social distancing for COVID-19. The rationale for the decision should be also clearly explained and communicated to the public.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
WHO. Public Health for Mass Gatherings: Key Considerations. World Health Organization. Available from: http://www.who.int/ihr/publications/WHO_HSE_GCR_2015.5/en/ (Accessed August 12, 2020).
• Memish ZA, Steffen R, White P, Dar O, Azhar EI, Sharma A, et al. Mass gatherings medicine: public health issues arising from mass gathering religious and sporting events. Lancet. 2019;393:2073–84. This recent review gives an overview on health issues in mass gatherings, including sporting events.
Gautret P, Mockenhaupt F, Grobusch MP, Rothe C, von Sonnenburg F, van Genderen PJ, et al. Arboviral and other illnesses in travellers returning from Brazil, June 2013 to May 2016: implications for the 2016 Olympic and Paralympic Games. Euro Surveill. 2016;21.
Hoang V-T, Gautret P. Infectious diseases and mass gatherings. Curr Infect Dis Rep. 2018;20:44.
WHO. Coronavirus (COVID-19) events as they happen. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/events-as-they-happen (Accessed August 12, 2020).
Worldometer. Coronavirus Update. Available from: https://www.worldometers.info/coronavirus/ (Accessed August 12, 2020).
Ebrahim SH, Memish ZA. COVID-19 - the role of mass gatherings. Travel Med Infect Dis. 2020;34:101617.
Gautret P, Al-Tawfiq JA, Hoang VT. COVID 19: will the 2020 Hajj pilgrimage and Tokyo Olympic Games be cancelled? Travel Med Infect Dis. 2020;34:101622.
Gautret P, Steffen R. Communicable diseases as health risks at mass gatherings other than Hajj: what is the evidence? Int J Infect Dis. 2016;47:46–52.
Gundlapalli AV, Rubin MA, Samore MH, Lopansri B, Lahey T, McGuire HL, et al. Influenza, winter Olympiad, 2002. Emerg Infect Dis. 2006;12:144–6.
Gardy JL, Naus M, Amlani A, Chung W, Kim H, Tan M, et al. Whole-genome sequencing of measles virus genotypes H1 and D8 during outbreaks of infection following the 2010 Olympic winter games reveals viral transmission routes. J Infect Dis. 2015;212:1574–8.
McCloskey B, Endericks T, Catchpole M, Zambon M, McLauchlin J, Shetty N, et al. London 2012 Olympic and Paralympic Games: public health surveillance and epidemiology. Lancet. 2014;383:2083–9.
Sile B, Mohammed H, Crook P, Hughes G, Mercer C, Cassel J, et al. Epidemiology of sexually transmitted infections in visitors for the London 2012 Olympic Games: a review of attendees at sexual health services. Sex Transm Dis. 2015;42:710–6.
Soligard T, Steffen K, Palmer-Green D, Aubry M, Grant M-E, Meeuwisse W, et al. Sports injuries and illnesses in the Sochi 2014 Olympic Winter Games. Br J Sports Med. 2015;49:441–7.
Soligard T, Steffen K, Palmer D, Alonso JM, Bahr R, Lopes AD, et al. Sports injury and illness incidence in the Rio de Janeiro 2016 Olympic summer games: a prospective study of 11274 athletes from 207 countries. Br J Sports Med. 2017;51:1265–71.
Hamilton B, Exeter D, Beable S, Coleman L, Milne C. Zika virus and the Rio Olympic Games. Clin J Sport Med. 2019;29:523–6.
No Zika Cases Reported During Rio Olympics, W.H.O. Says - The New York Times. Available from: https://www.nytimes.com/2016/09/03/health/zika-rio-olympics.html (Accessed August 12, 2020).
• Kim D-S, Lee Y-H, Bae KS, Baek GH, Lee SY, Shim H, et al. PyeongChang 2018 Winter Olympic Games and athletes’ usage of “polyclinic” medical services. BMJ Open Sport Exerc Med. 2019;5:e000548. This study shows a high proportion of athletes consulted polyclinics with the most common cause of illness being infectious diseases during the 2018 Winter Olympic Games.
• Kim K, Jang JY, Moon G, Shim H, Jung PY, Kim S, et al. Experiences of the emergency department at the Pyeongchang polyclinic during the 2018 PyeongChang winter Olympic Games. Yonsei Med J. 2019;60:474–80. This study describes the experience of Emergency Department during the 2018 Winter Olympics which served staff and athletes from many countries. That may provide useful information for planning medical care at similar events.
Valtonen M, Waris M, Vuorinen T, Eerola E, Hakanen AJ, Mjosund K, et al. Common cold in team Finland during 2018 winter Olympic Games (PyeongChang): epidemiology, diagnosis including molecular point-of-care testing (POCT) and treatment. Br J Sports Med. 2019;53:1093–8.
Ribas RM, de Campos PA, de Brito CS, Cavalcanti Dantas RC. 2021 Olympic Games Tokyo: safety issues and protection against COVID-19 transmission. J Glob Insect Dis. 2020;12:114–5.
Musa SS, Zhao S, Wang MH, Habib AG, Mustapha UT, He D. Estimation of exponential growth rate and basic reproduction number of the coronavirus disease 2019 (COVID-19) in Africa. Infect Dis Poverty. 2020;9:96.
Nabil B, Sabrina B, Abdelhakim B. Transmission route and introduction of pandemic SARS-CoV-2 between China, Italy, and Spain. J Med Virol. 2020. https://doi.org/10.1002/jmv.26333.
• Petersen E, Koopmans M, Go U, Hamer DH, Petrosillo N, Castelli F, et al. Comparing SARS-CoV-2 with SARS-CoV and influenza pandemics. Lancet Infect Dis. 2020;S1473–3099(20):30484–9. This study shows that SARS-CoV-2 is more transmissible than influenza virus that was frequently circulating during mass gatherings.
Huang L, Zhang X, Zhang X, Wei Z, Zhang L, Xu J, et al. Rapid asymptomatic transmission of COVID-19 during the incubation period demonstrating strong infectivity in a cluster of youngsters aged 16-23 years outside Wuhan and characteristics of young patients with COVID-19: a prospective contact-tracing study. J Inf Secur. 2020;80:e1–13.
Hoang VT, Dao TL, Gautret P. Recurrence of positive SARS-CoV-2 in patients recovered from COVID-19. J Med Virol. 2020;92:2366–7. https://doi.org/10.1002/jmv.26056.
•• Nakamura S, Wada K, Yanagisawa N, Smith DR. Health risks and precautions for visitors to the Tokyo 2020 Olympic and Paralympic Games. Travel Med Infect Dis. 2018;22:3–7. This study summarizes the potential health risks for visitors to Tokyo 2020, related to communicable disease risks and other health threats.
Yanagisawa N, Wada K, Spengler JD, Sanchez-Pina R. Health preparedness plan for dengue detection during the 2020 summer Olympic and Paralympic Games in Tokyo. PLoS Negl Trop Dis. 2018;12:e0006755.
Quilty BJ, Clifford S, Flasche S, Eggo RM. Effectiveness of airport screening at detecting travellers infected with novel coronavirus (2019-nCoV). Euro Surveill. 2020;25:2000080.
Bielecki M, Gerardo Crameri GA, Schlagenhauf P, Buehrer TW, Deuel JW. Body temperature screening to identify SARS-CoV-2 infected young adult travellers is ineffective. Travel Med Infect Dis. 2020;101832.
Maffetone PB, Laursen PB. Athletes: fit but unhealthy? Sports Med Open. 2015;2:24.
O’Keefe JH, Franklin B, Lavie CJ. Exercising for health and longevity vs peak performance: different regimens for different goals. Mayo Clin Proc. 2014;89(9):1171–5.
Nieman DC. Risk of upper respiratory tract infection in athletes: an epidemiologic and immunologic perspective. J Athl Train. 1997;32:344–9.
Pedersen BK, Ullum H. NK cell response to physical activity: possible mechanisms of action. Med Sci Sports Exerc. 1994;26:140–6.
•• de Carvalho Guerreiro R, Silva A, de Araújo Andrade H, Biasibetti IG, Vital R, Vital da Silva HG, et al. Was postponing the Tokyo 2020 Olympic and Paralympic Games a correct decision? Rev Bras Med Esporte. 2020;26:191–5 Sao Paulo Sp: Soc Brasileira Med Esporte. This study describes the impact of the decision to postpone the Tokyo 2020 Olympic due to the COVID-19 outbreak on several important issues, including impacts on the health of athletes.
Wikipedia. 2020 Summer Olympics. Available at: https://en.wikipedia.org/wiki/2020_Summer_Olympics (Accessed August 12, 2020).
Gallego V, Nishiura H, Sah R, Rodriguez-Morales AJ. The COVID-19 outbreak and implications for the Tokyo 2020 Summer Olympic Games. Travel Med Infect Dis. 2020;34:101604.
•• Taku K, Arai H. Impact of COVID-19 on athletes and coaches, and their values in Japan: repercussions of postponing the Tokyo 2020 Olympic and Paralympic Games. J Loss Trauma. 2020. https://doi.org/10.1080/15325024.2020.1777762. This article summarizes the reactions of athletes and coaches related to the repercussions triggered by the postponement of the Tokyo 2020 Olympic.
Mann RH, Clift BC, Boykoff J, Bekker S. Athletes as community; athletes in community: covid-19, sporting mega-events and athlete health protection. Br J Sports Med. 2020;54:1071–2. https://doi.org/10.1136/bjsports-2020-102433.
Sarto F, Impellizzeri FM, Spörri J, Porcelli S, Olmo J, Requena B, et al. Impact of potential physiological changes due to COVID-19 home confinement on athlete health protection in elite sports: a call for awareness in sports programming. Sports Med. 2020;50:1417–9.
Kissler SM, Tedijanto C, Goldstein E, Grad YH, Lipsitch M. Projecting the transmission dynamics of SARS-CoV-2 through the postpandemic period. Science. 2020;368:860–8.
McCloskey B, Zumla A, Ippolito G, Blumberg L, Arbon P, Cicero A, et al. Mass gathering events and reducing further global spread of COVID-19: a political and public health dilemma. Lancet. 2020;395:1096–9.
WHO. Considerations for sports federations/sports event organizers when planning mass gatherings in the context of COVID-19: interim guidance. Available from: https://www.who.int/publications-detail-redirect/considerations-for-sports-federations-sports-event-organizers-when-planning-mass-gatherings-in-the-context-of-covid-19-interim-guidance (Accessed August 12, 2020).
Escher AR. An ounce of prevention: coronavirus (COVID-19) and mass gatherings. Cureus. 2020;12:e7345.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Van Thuan Hoang, Jaffar A. Al-Tawfiq, and Philippe Gautret declare that they have no conflict of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Massive Gathering Events and COVID-19
Rights and permissions
About this article

Cite this article
Hoang, V.T., Al-Tawfiq, J.A. & Gautret, P. The Tokyo Olympic Games and the Risk of COVID-19. Curr Trop Med Rep 7, 126–132 (2020). https://doi.org/10.1007/s40475-020-00217-y
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40475-020-00217-y