Article Text

Abstract
Objectives: To compare estimates of the prevalence of injury among adolescents in 35 countries, and to examine the consistency of associations cross nationally between socioeconomic status then drunkenness and the occurrence of adolescent injury.
Design: Cross sectional surveys were obtained from national samples of students in 35 countries. Eight countries asked supplemental questions about injury.
Setting: Surveys administered in classrooms.
Subjects: Consenting students (n = 146 440; average ages 11–15 years) in sampled classrooms. 37 878 students (eight countries) provided supplemental injury data.
Exposure measures: Socioeconomic status (material wealth, poverty) and social risk taking (drunkenness).
Outcome measures: Specific types and locations of medically treated injury.
Results: By country, reports of medically treated injuries ranged from 33% (1060/3173) to 64% (1811/2833) of boys and 23% (740/3172) to 51% (1485/2929) of girls, annually. Sports and recreation were the most common activities associated with injury. High material wealth was positively (OR>1.0; p<0.05) and consistently (6/8 countries) associated with medically treated and sports related injuries. Poverty was positively associated with fighting injuries (6/8 countries). Drunkenness (social risk taking) was positively (p<0.01) and consistently (8/8 countries) associated with medically treated, street, and fighting injuries, but not school and sports related injuries.
Conclusion: The high prevalence of adolescent injury confirms its importance as a health problem. Social gradients in risk for adolescent injury were illustrated cross nationally for some but not all types of adolescent injury. These gradients were most evident when the etiologies of specific types of adolescent injury were examined. Prevention initiatives should focus upon the etiologies of specific injury types, as well as risk oriented social contexts.
- HBSC, Health Behaviour in School-Aged Children survey
- adolescent
- aetiology
- risk factors
- social determinants
Statistics from Altmetric.com
Over the past two decades, injury has been recognized as an important cause of morbidity in pediatric populations and is a leading cause of death among children internationally.1–3 In many countries1,4 pediatric injuries account for more childhood deaths than all other causes combined. Burdens associated with pediatric injury in terms of lost potential, disability, treatment costs, and rehabilitation are substantial.4,5 Peaks in the occurrence of injury related traumas are observed in adolescents1 and their etiologies are obvious health research priorities.6 Social risk factors are of interest as potential injury determinants, yet studies of social factors and adolescent injury are uncommon, especially cross nationally.
Increasing attention has been given to the effects of socioeconomic status on health, although research in the injury field has mainly concentrated on adults7,8 and young children.9,10 Socioeconomic status has been shown to be negatively associated with injury risk but the level of association varies from modest7,11,12 to strong7,8,13,14 according to the type of injury, the population under study, and the indicators of socioeconomic status that were applied. Few studies of adolescents have examined socioeconomic status relations with specific types of injury, and existing studies report inconsistent findings.15,16 This aspect of the social aetiology of injury is of continued interest as the economic gap between the rich and poor is widening17 and adolescents who are financially deprived may be embedded in a hazardous social context.
Risk taking behaviour represents a second potential focus for etiological studies.18 Adolescent lifestyles that include engagement in substance use, truancy, and the taking of physical and sexual risks are the social norm in many adolescent societies.19–21 Most of these risk behaviours (for example, drunkenness22–24) occur in a social context. A recent systematic review25 that examined the link between social risk taking and injury identified few (n = 7)26–32 high quality studies that focused upon these topics, and none among adolescents. Risk taking behaviour was associated with the occurrence of unintentional injury except in the case of injuries in highly skilled sports.
In this study, we present contemporary estimates of the prevalence of injury among adolescents in 35 countries. We also examine relations between illustrative social determinants (two measures of socioeconomic status; drunkenness, a risk behaviour that occurs in social contexts22–24) and the occurrence of specific types of adolescent injury (school, street, sports related, and fighting). The etiologic analysis was used to model the occurrence of different types of injury (dependent variables) as a function of socioeconomic status and drunkenness (independent variables), in multiple logistic regression analyses that adjusted for other known risk factors. Through this analysis we hoped to: (1) describe contemporary rates of adolescent injury on a cross national basis; (2) use illustrative examples of social factors and specific types of injury to confirm the existence of gradients in risk for injury when the social etiologies of specific (for example, sports, fighting) as opposed to general (for example, injured/not injured) injury outcomes were examined, and (3) determine whether these gradients could be observed consistently across countries. Increased understanding of the distribution of the injury problem as well as potential social determinants could guide future preventive interventions.
METHODS
Description of survey and study population
The study was based on international records from the 2001/2002 Health Behaviour in School-Aged Children survey (HBSC); a World Health Organization collaborative cross national study. The HBSC involves a cross sectional survey of elementary and high school students.33 The survey consists of a questionnaire completed in the classroom (completion time 45 minutes). Institutional ethics approval is obtained at the country level.
The goal of the HBSC is to identify youth health indicators and the factors that influence them.33 One of its primary functions is to further understanding about the social factors that put adolescents at risk or are notably protective. The survey includes a set of indicators that provide a valid representation of the health and lifestyle of adolescents in industrialized countries.
Sampling
A full description of the sampling method appears in the HBSC protocol (see http://www.hbsc.org). Because differences exist between countries in “school systems, age of admission to school and levels of advancement of students across countries”, the HBSC cannot have a uniform approach to sampling.33 The sampling protocol always involves a cluster design with the school class being the basic cluster. Countries are initially asked to randomly sample schools that teach 11–15 year old children. School classes are then selected using a weighted probability technique to ensure that students from schools of different sizes are equally likely to be included. In some countries, regional geography and other salient demographic factors (for example, religion, language of instruction) are taken into consideration via stratification.33
Measures
The 2001/2002 HBSC survey contained both mandatory items and optional groups of questions. This analysis focused upon injury items (one mandatory question; an optional package of items used in eight countries), as well as available measures of social risk factors: socioeconomic status items (two mandatory questions), and a drunkenness item (one mandatory question). All measures were taken from previous studies,34,35 previous HBSC surveys,34 or were adapted from existing surveillance initiatives.36,37 All measures were pretested for face and content validity in classrooms within each participating country.
Outcome measures: injury
The occurrence of injury was measured using a single mandatory question that is consistent with the widely accepted definition of an injury as an “event that requires medical attention”.33,35 Questions about injury were preceded with the following statement: “Many young people get hurt or injured from activities such as playing sports or fighting with others at different places such as the street or home. Injuries can include being poisoned or burned. Injury does not include illnesses such as Measles or the Flu. The following questions are about injuries you may have had during the past 12 months.” Participants were asked to report injury events that required medical attention from a doctor or a nurse. Response options were: “I was not injured in the past 12 months”; “one time”; “two times”; “three times”; “four or more times”.
Eight countries employed the optional package of injury questions: Belgium-French, Canada, Czech Republic, Estonia, Israel, Latvia, Poland, and the United States (high school students only). Participants reporting one or more medically treated injuries were asked to identify their most serious injury event. Supplemental items included close-ended questions that addressed external causes of injury. This was done because “virtually all injury classification systems36,37 attempt to describe and classify the external factors and circumstances that precipitate injury events”.34,38 Descriptors of external cause included: location of injury (response options included: “home or yard”; “school including school grounds”; “sports facilities or fields”; “street, road or parking lot”) and the mechanism of injury (response options included but not limited to: “playing or training for organized sport or recreational activity”; “physical fight”). The wording of these questions and the response categories was based upon existing surveillance systems36,37 but limited to common responses observed in previous surveys.34,39
Primary risk factor variables
A composite Family Affluence Scale score was calculated based on responses to questions about family, as follows: “car ownership”; “owning a bedroom for oneself”; “holiday travel during past 12 months”; “computer ownership”. This scale infers absolute levels of material wealth expressed in terms of consumption, has a possible range of values from 0–7, is conceptually related to common indices of material deprivation,39,40 and is similar to an existing index of home affluence.41 The motivation for inclusion of this variable was to consider the relative effects of deprivation and wealth on injury risk.
A more direct measure of poverty was also derived from a question reporting the frequency that a young person went to school or bed hungry because there is not enough food at home (response options: “always”; “often”; “sometimes”; “never”).
As a measure of social risk taking, participants reported the number of times that they had ever consumed so much alcohol that they were really drunk (response options: “never”; “once”; “4–10 times”; “more than 10 times”). This drunkenness measure has been used in the HBSC survey since its inception, and represents a commonly used, validated approach to the assessment of heavy alcohol intake on single occasions.42 It has proven to be a “very good predictor” of other risk behaviours, as well as poor adjustment to school.33
Confounding variables
Three variables were selected a priori for inclusion as confounders: age (in years), sex, and physical activity participation. These variables are risk factors for injury, and preliminary analyses demonstrated variations in these variables by the social risk factors under study.
Physical activity was measured as follows: after being provided with a definition and examples of common activities, subjects were asked how many days in the past week and in a typical week they were physically active (cumulative activity) for 60 minutes or more. These questions were based on the Moderate-to-Vigorous Physical Activity measure developed by Prochaska and colleagues.43 The mean number of days from the past week and a typical week were used as an index of participation.43
Statistical analysis
Descriptive analyses were conducted within each country to obtain the prevalence of medically treated injury by sex, and these were ranked across the 35 countries. Frequency distributions of injury occurrence were plotted within the eight countries by location then mechanism of injury. Multiple logistic regression analyses were used to estimate odds ratios (OR) for injury associated with the available social risk factors (material wealth, poverty, drunkenness). Separate models for eight countries were run for injury locations (for example, school injuries, home injuries, street injuries), and mechanisms (for example, playing or training for sports/recreational activities, fighting injuries). All odds ratio estimates were adjusted simultaneously for age, sex, physical activity, and the other primary social risk factors. All descriptive and regression analyses were performed within countries and were conducted using SPSS (version 12, SPSS Inc, Chicago, IL, USA). Design effects of 1.20 were applied to standard errors and hence confidence intervals surrounding risk estimates using Excel (version 2000, Microsoft Inc, Redmond, WA, USA).
RESULTS
Samples
146 440 children in 35 countries provided reports of injury experiences and of these, 38 878 children in eight countries answered supplemental questions about their one most serious injury (if any). At the participant level, responses rates varied from 64.5% (3481/5400) in Latvia to 91.2% (4560/5000) in Estonia.
Descriptive findings
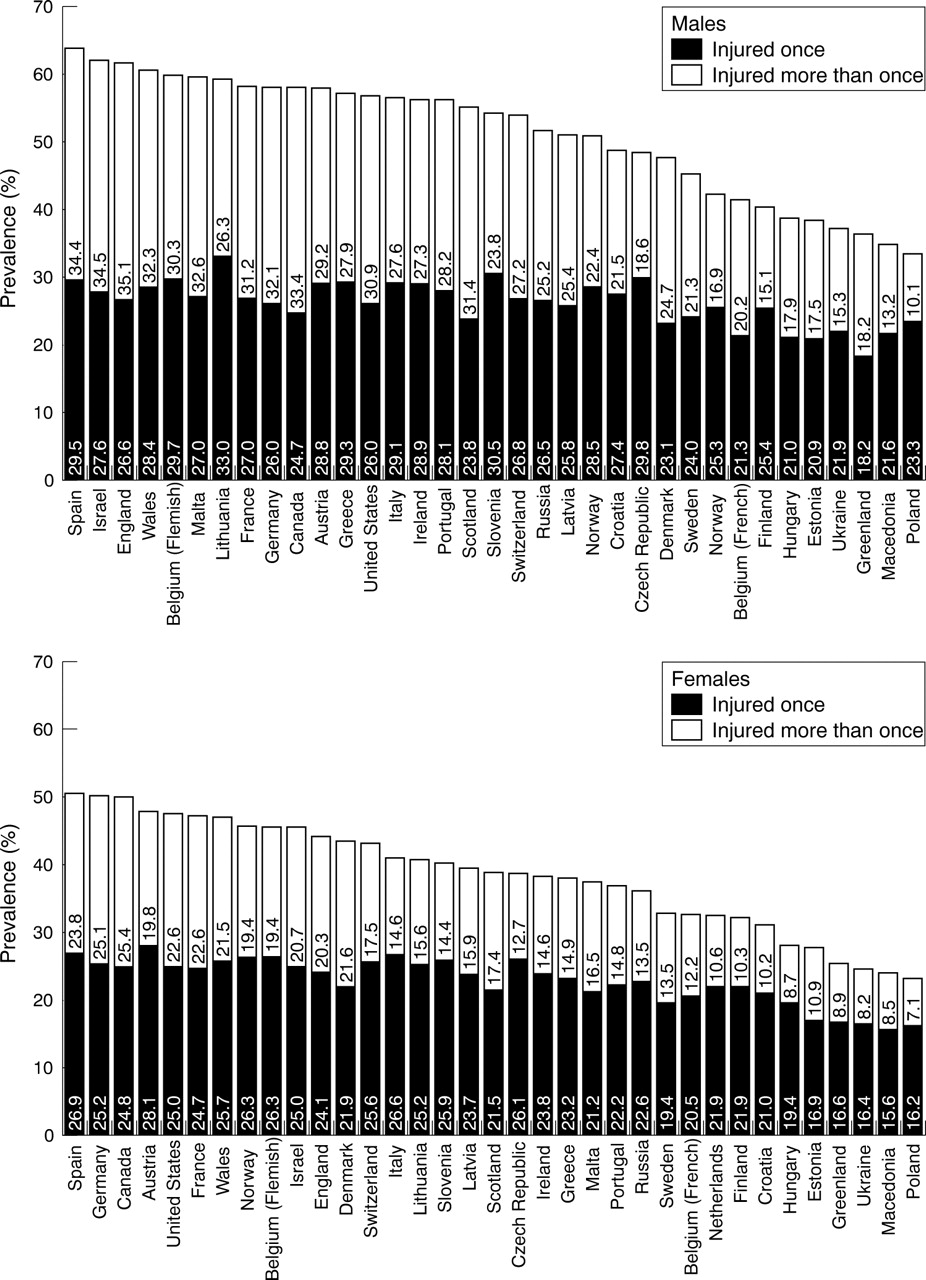
The percentage of youth reporting one or more medically treated injuries within the past 12 months was more common in boys than in girls in all 35 countries, with cross national prevalence estimates ranging from 33% (1060/3173) to 64% (1811/2833) of boys and 23% (740/3172) to 51% (1485/2929) of girls (fig 1). Estimates of youth reporting a single injury were much less variable. Major differences in prevalence estimates by country were attributable to variations in the number of youth reporting multiple injuries. There was no evidence of strong regional (for example, North America v Europe) differences.
{kind=link}
Annual prevalence of medically treated injuries among 146 440 adolescents in 35 countries, by sex.
Among the eight countries that used optional injury questions, the median proportions of youth reporting one or more injuries were very high (table 1). There was considerable variation between countries in the rank order of injury locations. By activity, playing or training for a sport/recreational activity was the leading external cause of injury. Fighting injury was the only form of intentional injury reported. Summary values provided in table 1 indicate the variability between countries in the prevalence of social risk factors, by sex, as well as median ages and levels of physical activity of the samples of adolescents under study.
Prevalence of injury outcomes and social risk factors among 37 878 adolescents in eight countries
Etiologic findings
Medically treated injuries
Low material wealth was protective for the occurrence of medically treated injuries (6/8 countries), with the suggestion of a protective effect in the other two countries (see http://www.injuryprevention.com/supplemental for table 2). Always/often going to bed or school hungry (an indicator of poverty) was an uncommon social exposure, but as inferred from point estimates it was consistently (6/8 countries) associated with trends towards increased risk for medically treated injuries. Frequent drunkenness during a youth’s lifetime was a strong and consistent risk factor for medically treated injuries (8/8 countries).
School injuries
The occurrence of school injuries was not consistently associated with low levels of material wealth, going to bed or school hungry, or drunkenness (see http://www.injuryprevention.com/supplemental for table 3).
Sports-related injuries
Low material wealth was strongly and consistently associated with protection from sports related injuries, even after controlling for physical activity (8/8 countries; see http://www.injuryprevention.com/supplemental for table 4). There was no evidence of associations between poverty and sports related injury, and inconsistency in the risk estimates observed for frequent drunkenness and sports related injury.
Street injuries
There was no evidence of significant associations between material wealth and street injuries (0/8 countries; see http://www.injuryprevention.com/supplemental for table 5). The direction of risk estimates for poverty/hunger and street injury were positive but not always statistically significant. Frequent drunkenness was a strong and consistent risk factor for street injuries (8/8 countries), and the risk estimates generally followed a dose related pattern.
Fighting injuries
Fighting injuries were uncommon and this is reflected in the variability of the confidence intervals surrounding risk estimates (see http://www.injuryprevention.com/supplemental for table 6). There was no consistent association between low material wealth and fighting injuries. Although not statistically significant, based upon the consistency of point estimates (6/8 countries) there was the suggestion of an association between poverty/hunger and fighting injuries. Drunkenness was a strong and significant risk factor for fighting injuries (8/8 countries).
DISCUSSION
With a prevalence between 33% and 62% across countries among males (19% to 39% among females), our findings indicate that adolescent injuries are very common cross nationally. Our analysis represents one of the first cross national examinations of adolescent injury patterns, and our focus on the social etiology of specific types of injury cross nationally is also novel. Variations in the strength and direction of associations were observed for different combinations of social risk factors and types of injury. Increased material wealth was positively associated with sports related but none of the other forms of injury. Drunkenness (as a measure of socially oriented risk taking) and hunger (as a measure of poverty) were positively and consistently associated with street injuries and injuries involving physical fights, but not school and sports related injuries. These examples do illustrate that specific types of adolescent injury appear to have different social etiologies.
The cross national variations in injury prevalence observed are intriguing, but it is unclear whether these variations are attributable to underlying differences in risk. Our analysis involved study of medically treated injuries, and there are known international variations in access to medical treatment.44 The 35 countries under study operate under a variety of healthcare delivery models from fully public systems to systems that mix public and private healthcare models.45 This may in part account for the apparent protective effect of low material wealth on rates of medically treated injury and sports injury. Some but not all countries have resident nurses in school systems. This too could contribute to overreporting of injury events in more affluent schools, which would introduce a differential bias by socioeconomic class.
Depending upon the country, the 2001/2002 HBSC was administered temporally during fall or winter school terms. Risks for adolescent injury vary by season, and injuries are most reliably reported within three months.46 Variations in the timing of the survey across countries may have impacted injury rates and hence the cross national comparisons.
With respect to etiologic findings, past studies of socioeconomic status and injury have demonstrated consistent gradients in risk for injury in association with low socioeconomic status among general populations,7,8 populations of young children,9,10 and for specific types of injury.47 Most existing studies have focused upon fatal or other forms of traumatic injury, and ecological (group level) analyses predominate this literature. Social gradients in risk for injury have not, however, been demonstrated consistently within adolescent populations.15,16,48 Past explanations for this issue centre around the assessment of socioeconomic status in adolescents, and the unique mixing that occurs in adolescent cultures.15,16,48 Our study confirms that gradients in adolescent injury risks by socioeconomic class do exist, but are only clearly demonstrated when specific combinations of socioeconomic status measures and injury types are examined in a focused manner.
Our measure of poverty was consistently associated with injuries caused by violence (fighting) and injuries in less organized (street/road) locations. Mechanistically, this poverty indicator appears to be operating as a measure of social deprivation and these associations demonstrate the existence of classic, inverse health gradients among adolescent populations that are exposed to contextual risks. Poorer children may not be afforded protection from physical risks in their social environment. Similar risk gradients were not identified in school locations which suggests that social context does impact upon health risk gradients.
We failed to identify associations between the Family Affluence Scale and most external causes of injury. Exceptions were associations between family affluence and sports/recreational injuries, which were in a positive direction (higher affluence, more injuries). The family affluence measure may correlate strongly with increased opportunities for participation in organized sports that are expensive. We also recognize the potential for a differential misclassification of sports injury outcomes by level of material wealth due to variations in access to medical care.
Strong associations were observed between increased amounts of drunkenness and fighting injuries and injuries that occurred on the street. Drunkenness is clearly a direct cause of injury, and its association with some but not all injury outcomes is expected given variations in social context that surround adolescent drinking patterns. Drunkenness is also a marker for a problem behaviour lifestyle18 that includes engagement in multiple risk behaviour.48,49 This social behaviour is normative in many youth cultures, and is associated with a variety of injury consequences. It is also notable that similar etiologic patterns exist for fighting and street injuries in that poverty and drunkenness were associated with these injury types. This pattern might suggest that aggression is also a mediating factor for certain types of injury that occur in unstructured social contexts.
Major strengths of this analysis are its international scope and the large numbers of young people involved from a diversity of cultures. The HBSC questionnaire items were developed iteratively over several years and are supported by validation efforts.33,34 The ability to examine relations between different social measures and a variety of injury types is a second strength. Gradients in risk for injury may be masked in other studies that examine more general injury outcomes. Weaknesses include the fact that data were based upon self reports with associated reporting errors, and inferences made about etiology are further limited by the cross sectional nature of data collection. In addition, we studied only a limited range of social risk factors and injury types. In the future it would be better to study a broader range of risk factors in a prospective manner using validated measures that were not reliant on self-reports. This task would be very difficult to accomplish on a cross national basis.
Our findings inform the planning of future social research. There is an inherent need for etiologic models to be theoretically based, and there is also a need for injury studies to focus upon underlying physical mechanisms (for example, impairment, hazards) and behavioral mechanisms (for example, bullying, aggression) that directly link social risk factors to injury occurrence. These mechanisms are likely to be responsible for the fact that individual risk factor measures are associated with some but not all injury outcomes. Some existing studies of socioeconomic status and injury, for example, use only a single measure of socioeconomic status and do not consider the possibility that etiologic relations may vary by injury type. In addition, characteristics of social contexts (home, school, peer group) that could protect adolescents from injury, or conversely put them at increased risk, also require consideration. Conceptual models such as the population health framework50 could be useful in that regard. This framework states that determinants of health operate at two levels—contextual and individual. With respect to the etiology of adolescent injury, contextual and individual determinants may have direct and additive effects that would interact to produce varying levels of risk.50
The results also have implications for adolescent health policy. Adolescent injuries should be recognized as a major public health issue. Social gradients in risk for adolescent injury can be demonstrated cross nationally for some but not all types of adolescent injury. These gradients are most evident when the etiologies of specific types of adolescent injury are examined. Health policy surrounding the prevention of adolescent injuries requires a solid evidence base, and our findings identify vulnerable subgroups and social contexts that lead consistently to the occurrence of adolescent injury. Preventive interventions should also focus upon the etiologies of specific as opposed to general injury types, as well as these risk oriented social contexts.
Key points
-
The social etiology of adolescent injury remains poorly understood.
-
This cross national study demonstrates that injury is an important, contemporary adolescent health problem cross nationally.
-
Gradients in risk for adolescent injury can be demonstrated for some combinations of social risk factors and injury. These are evident when the etiologies of specific as opposed to general forms of adolescent injury are examined.
-
Some social contexts appear to protect adolescents from socially oriented injury events.
Acknowledgments
Please visit http://www.injuryprevention.com/supplemental for the full list of acknowledgements.
REFERENCES
Supplementary materials
The tables are available as a downloadable PDF (printer friendly file).
If you do not have Adobe Reader installed on your computer,
you can download this free-of-charge, please Click hereFiles in this Data Supplement:
- [view PDF] - Tables 2-6.