Article Text

Abstract
Background The use of text messaging or short message service (SMS) for injury reporting is a recent innovation in sport and has not yet been trialled at the community level. Considering the lack of personnel and resources in community sport, SMS may represent a viable option for ongoing injury surveillance. The aim of this study was to evaluate the feasibility of injury self-reporting via SMS in community Australian football.
Methods A total of 4 clubs were randomly selected from a possible 22 men's community Australian football clubs. Consenting players received an SMS after each football round game asking whether they had been injured in the preceding week. Outcome variables included the number of SMS-reported injuries, players’ response rates and response time. Poisson regression was used to evaluate any change in response rate over the season and the association between response rate and the number of reported injuries.
Results The sample of 139 football players reported 167 injuries via SMS over the course of the season. The total response rate ranged from 90% to 98%. Of those participants who replied on the same day, 47% replied within 5 min. The number of reported injuries decreased as the season progressed but this was not significantly associated with a change in the response rate.
Conclusions The number of injuries reported via SMS was consistent with previous studies in community Australian football. Injury reporting via SMS yielded a high response rate and fast response time and should be considered a viable injury reporting method for community sports settings.
Statistics from Altmetric.com
Introduction
Participation in organised sport is an important part of the overall strategy for physical activity promotion.1 However, injury associated with sport has the potential to outweigh the health benefits of participation and the perceived risk of injury could also act as a deterrent to future participants.2 ,3 Sports injuries are largely preventable,4 ,5 but the development of relevant and effective preventive strategies for certain populations has been hampered by a lack of available injury data.6
Researchers in community sport settings have previously incorporated a range of injury surveillance methods, including employing data collectors and enlisting medical personnel at clubs to record injuries.7–10 These methods are labour intensive and lack sustainability as an ongoing surveillance method in the under-resourced environment of community sport. Moreover, community sports participants often seek treatment from a range of health professionals outside of their clubs,11 which could make it difficult for club-based personnel to capture all injuries.
As an alternative to traditional injury registration methods, researchers have recently trialled text messaging or short message service (SMS) for self-reporting of injuries with considerable success.12–14 Potential benefits of using SMS include the fact that messages can be sent and received on a highly frequent basis which limits the risk of recall bias by respondents, previously an issue in studies using injury self-reporting.15 ,16 Another major strength of SMS is the speed with which data can be obtained. When field-based personnel are used for injury surveillance, researchers often have to wait until the end of the season to receive compiled injury data. Using SMS, injuries can be reported shortly after they occur, enabling injury trends to be monitored from 1 week to the next. This could be particularly useful in sport for evaluating players’ responses to changes in training loads or match conditions over the course of a season, providing the opportunity for timely intervention by coaches, trainers and medical personnel.
Considering the lack of personnel and resources for injury surveillance in community sport17 ,18 and the widespread mobile phone usage among Australian adults,19 this method has the potential to be convenient for participants and researchers and may represent a feasible option for ongoing surveillance. Previous studies using SMS in sports settings have been conducted with elite Danish handballers,12 elite Norwegian soccer players13 and for leisure-time sports injuries in Danish schoolchildren.14 Text messaging for injury reporting has not yet been trialled within any community club sports. Nor have any other studies reported on the feasibility of the method for sports settings in terms of SMS response times or the sustainability of response rates. We aimed to evaluate the feasibility of injury self-reporting via SMS in terms of the number of injuries captured, the response rates and the response time.
The study was carried out within community Australian football, a setting associated with a high rate of injuries, particularly to the lower limb.8 ,20 This fast-moving team sport is characterised by physical contests between players, kicking, handballing and running.21 It is a football code unique to Australia but has similar elements to rugby (such as tackling), to soccer (such as running and kicking) and to Gaelic football (such as handballing). At the community level, the sport is played from March to September with 16–18 weeks of competition (rounds).
Methods
Participants
Australian football players were recruited from four men's community football clubs (nine teams in total) in Victoria, Australia. Each club was randomly selected from a pool of 22 community Australian football clubs concurrently involved in a larger injury prevention project.22 At a club training session prior to the start of the football season, the research team provided players with information about the study and gave players the opportunity to ask questions before obtaining written informed consent. Participants were eligible for inclusion if they were aged 18+ years and planned to play football for their club throughout the entire 2012 football season (16–18 rounds or weeks of competition). No incentives were offered for participation. A total of 139 players from the 4 clubs agreed to participate, which represented 44% of all registered players (n=316). We did not record the exact number of players in attendance the night each club was visited but it was less than the total number of registered players. The mean (SD) age of participants was 25 (4) years and ranged from 18 to 38 years. In all, 17 participants were lost to follow-up over the course of the season; 2 due to season-ending injuries, 10 due to quitting football and 5 for unknown reasons. We included results from these participants up until their dropout date in all analyses. Ethics approval was obtained from the Monash University Human Research Ethics Committee.
Procedures
After providing consent, we asked participants whether they wished to be contacted by email or SMS but all preferred to be contacted by SMS. Participants then gave their mobile phone numbers and preferred days and times for receiving messages. Throughout the playing season, participants received a message on their personal mobile phone 1–2 days after each weekly match. The message read: ‘Please reply ‘yes’ or ‘no’ indicating whether you have experienced a new football injury in the last 7 days’. If a participant answered ‘no’ they were thanked with a return SMS and there was no further contact from the research team that week. If a participant replied ‘yes’, he received a follow-up phone call at a time of his choosing from the primary author (CE), a physiotherapist, to provide the details of his injury (see online supplementary file for questionnaire used). If a participant did not respond to the initial SMS, he received another SMS 2 days and again 4 days after the initial attempt.
The primary outcome was any football-related injury. We recorded only those injuries that had been sustained during official football training sessions or matches, as confirmed during follow-up interview. The definition of injury was kept deliberately broad to allow players to report on all injuries rather than a subset.
Data analysis
We downloaded all weekly SMS responses (‘yes’/‘no’) from our mobile phone to an Excel (Microsoft Office Excel 2010) spread sheet and then exported all data to Stata 12 (StataCorp) for analysis. To determine whether the number of SMS-reported injuries changed over the course of the season, we calculated the correlation between number of injuries and football round number using the Spearman correlation coefficient. For each round of the season, we recorded the percentage of players who responded to the initial SMS sent, the percentage who responded after all three reminder messages and the percentage requiring one or two SMS reminders. For a random sample of eight rounds, we calculated the time to reply to the initial SMS rounded to the closest minute.
To establish whether the response rate changed over the course of the season we fitted a mixed-effects Poisson regression model with the number of responses as the outcome, the football round as the covariate of interest and the number of people messaged each round as the exposure. We observed a non-linear relationship between response rate and the round number. Therefore, ‘round number’ was entered into the model as a categorical rather than continuous variable. The reference category was the round with the highest response rate (round 1). Response rates differed between clubs. Therefore, club was included in the model as a random effect to account for clustering.
To determine whether the response rate influenced the number of injuries reported, we fitted a second mixed-effects Poisson regression model with the number of responses as the outcome, the number of injuries reported by each club each round as the covariate of interest and the number of people messaged each round as the exposure. ‘Number of injuries’ was entered into the model as a categorical variable. The reference category was the lowest number of injuries reported in any round (n=0 injuries) and again, club was included as a random effect to account for clustering. We set the significance level for all analyses at p<0.05 and reported rate ratios and 95% CIs for the Poisson regression models.
Results
In total, we sent 2516 text messages to players across the whole season. The percentage of players requiring one SMS reminder ranged from 5% to 16% across rounds. The percentage requiring two SMS reminders ranged from 2% to 10% across rounds.
Number of injuries
A total of 171 injuries were reported via SMS by 66% of participants (n=92). One of these injuries did not fit the injury definition as it occurred outside of official football training sessions or matches. A further three injuries were not included as participants could not be contacted for their follow-up injury interviews. Therefore, a total of 167 recordable injuries remained (table 1). This equated to an incidence of 1.20 (95% CI 1.14 to 1.28, range 0–6) injuries per participant over the season. The number of injuries reported per round ranged from 2 to 16. For 1 club (n=18 players) the season ran from rounds 1 to 16, and for another club (n=54 players) data were collected for rounds 3–18 only.
Number of injuries reported by SMS and response rates for each round
Figure 1 shows the number of injuries reported each round. Only rounds 3–16, where a full sample was available, were included. There was a significant negative association between the number of injuries and the football round (rs=−0.76, p=0.002), with the number of reported injuries decreasing as the season progressed.
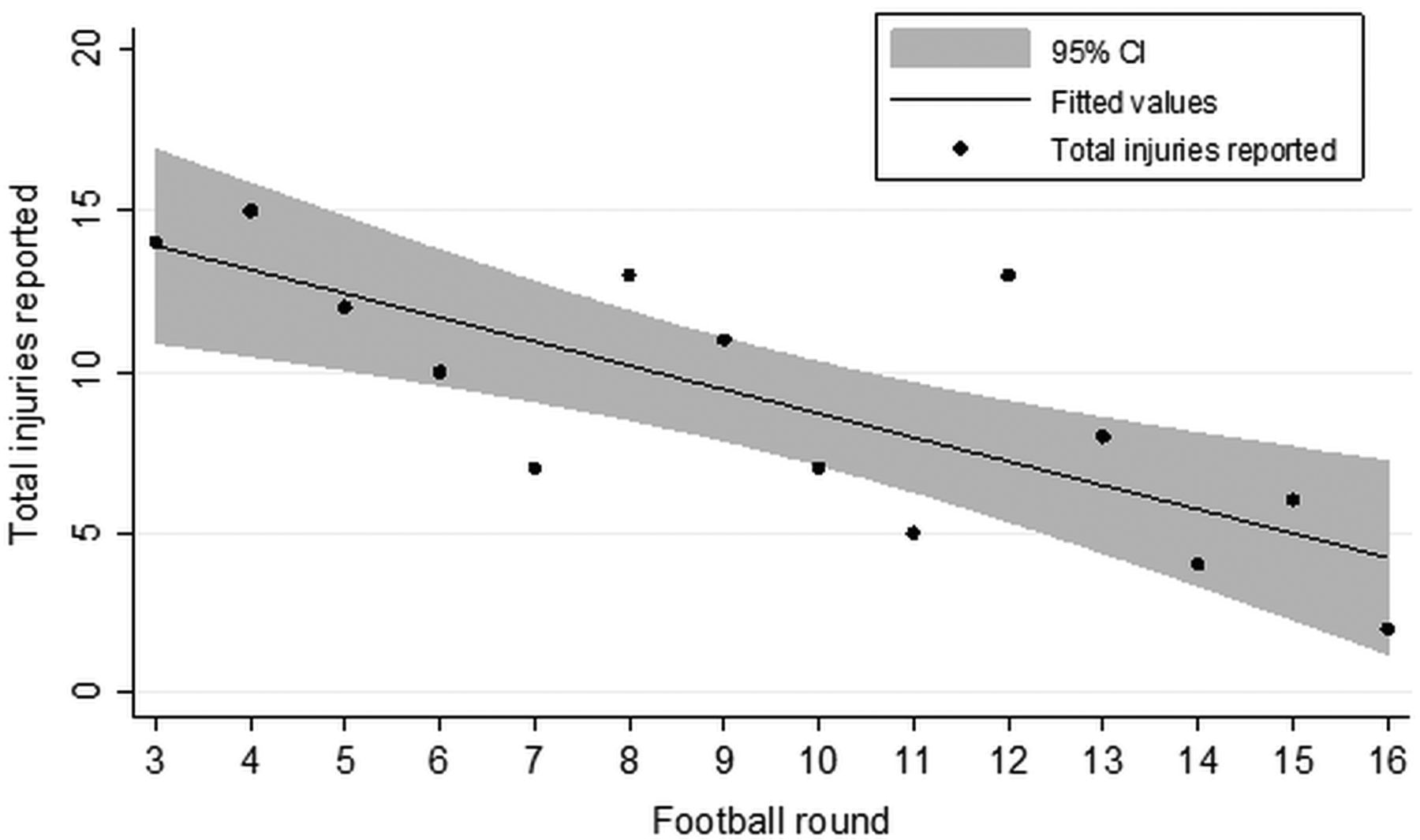
Number of injuries reported by players via short message service (SMS) each round (rounds 3–16).
Response rate
The response rates to the first weekly SMS sent by researchers ranged from 84% to 94% across rounds (table 1). After all three reminder messages for each round were sent (if necessary), total response rates increased and ranged from 90% to 98% (table 1). The highest total response rate was achieved in the first round (98%) and the scatter plot in figure 2 shows an apparent decline in the total response rate over the season, followed by a slight recovery in rounds 17 and 18.
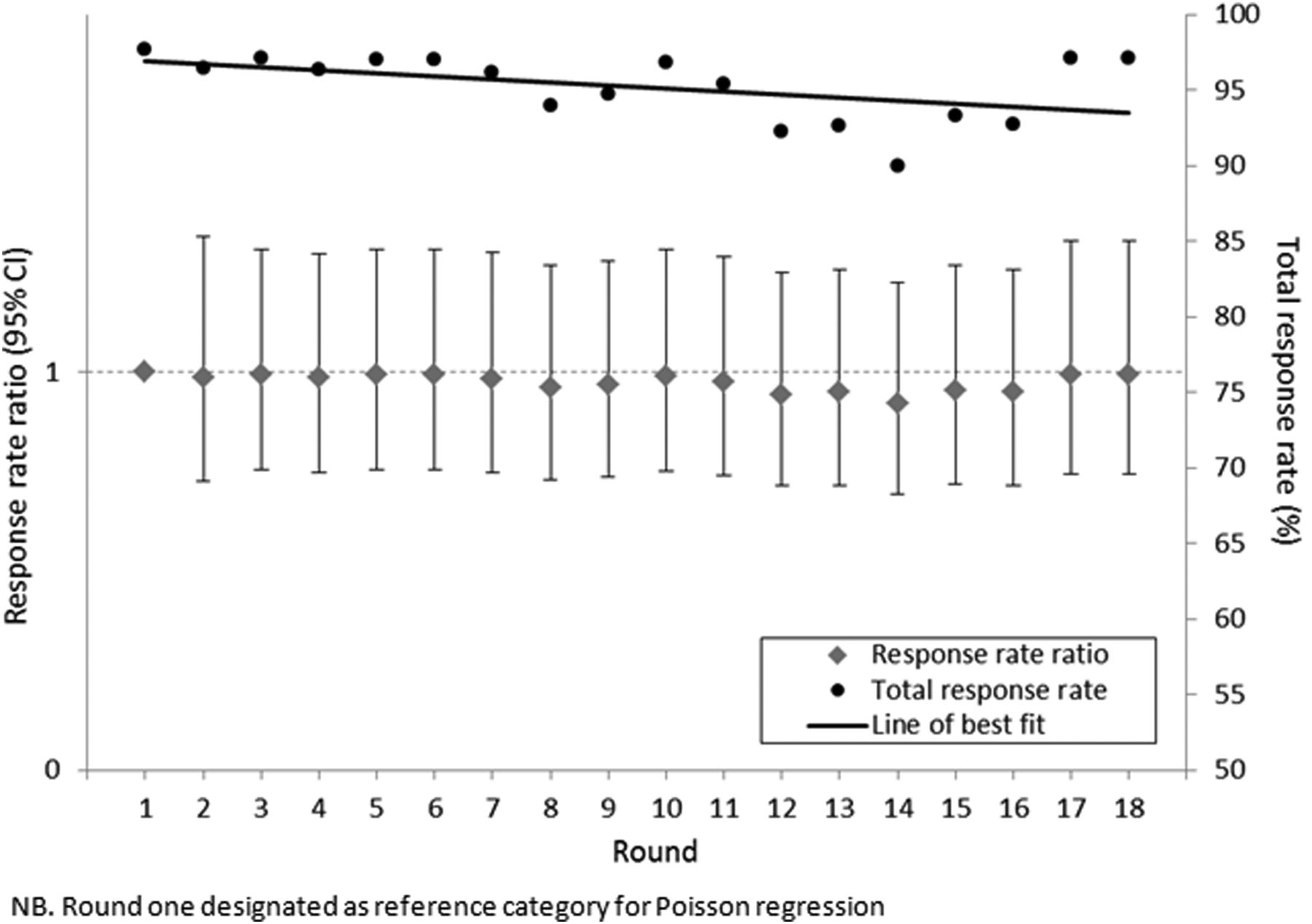
Total response rates and response rate ratios derived through Poisson regression for rounds 1–18.
Results of the first Poisson regression analysis are shown in figure 2. Relative to round 1, response rate ratios for rounds 2–18 ranged from 0.92 to 0.99 and all 95% CIs contained the null value. Thus, there were no significant differences in response rates across the season relative to round 1.
Table 2 shows response rate ratios based on the number of injuries reported per club per round. The number of injuries reported by each club each round ranged from 0–9. Relative to the rounds in which no injuries were reported, response rate ratios ranged from 0.98 to 1.08 and all 95% CIs contained the null value. Thus, the number of injuries reported was not significantly associated with the response rate.
Response rate ratios derived through Poisson regression for number of injuries reported per club per round
Time to respond
We totalled the number of messages sent by researchers and received from players across eight randomly-selected rounds. A total of 89% (95% CI 87% to 91%) of players replied to the first weekly SMS sent by researchers (figure 3). Of those that replied to the first SMS, 97% (95% CI 96% to 98%) responded on the same day and of those that responded on same day, 47% (95% CI 43% to 50%) responded within 5 min.

{kind=link}
{kind=link}
{kind=link}
Day and time of response to first short message service (SMS) sent (totals across 8 randomly sampled rounds).
Discussion
We aimed to investigate the use of injury self-reporting via SMS in community sport. There have been a diverse range of injury reporting methods used in community sport and, as such, an optimal technique for capturing the full extent of the injury problem in this setting is yet to emerge.6 This study is the first to investigate the use of SMS for the collection of injury data in community sport and also the first in Australian football. This is also the first injury study to report on the sustainability of response rates and response times achieved with SMS.
From the high total response rate of 90% to 98% and the fact that almost half of the participants responded within 5 min, it is evident that most participants found SMS a convenient method for reporting their injuries. Other studies using SMS for injury reporting have reported similarly high response rates.12–14 In their study of injuries in elite handballers, Moller et al12 reported a response rate of 85% to 90%, Nilstad et al13 achieved a response rate of 90% with their cohort of elite female soccer players and Jespersen et al's14 study of schoolchildren achieved an average weekly response rate of 96%.
As with any surveillance system a balance must be achieved between obtaining high quality injury data and ensuring that participants are not deterred by excessive data requests.23 Although there was a decline in the total response rate over the course of this season, this was non-significant, indicating that most participants were consistent in their willingness to respond over the 6-month football season. There was also a slight increase in response rates towards the end of the season possibly suggesting a recovery in participants’ enthusiasm as the study drew to a close. No other injury studies have reported whether their SMS response rates changed over time. However, in a study by Hanauer et al,24 which used SMS reminders regarding blood glucose monitoring in adolescent diabetics, the response rates declined markedly over the course of the 3-month study. The authors alleged that the novelty of the system wore off and became repetitive and exhausting for participants over time. Conversely, in Anhoj and Moldrup's25 study using SMS for data collection of asthma symptoms, response rates were sustained over the 2-month study period. However, their overall response rates of 69% were comparatively low and thus possibly easier to maintain. Future injury research may need to consider the optimal frequency for SMS requests and an optimal length of follow-up for studies of this kind.
The number of injuries reported by SMS (1.2 per player) was within the range reported by previous studies of adult community Australian footballers.26 ,27 In their study of footballers within the Victorian Amateur Football Association (VAFA), Gabbe et al26 reported an incidence of 1.3 injuries per player over a season of 18 rounds. In that study, data was recorded by club-based medical personnel and their definition of injury encompassed injuries leading to time loss from training or matches and those requiring treatment. A later study, with a similar methodology, reported an incidence of only 0.7 injuries per player per season in community Australian football.27 The authors used non-medical club personnel to collect data which may explain the lower injury incidence. While we used a broader definition of injury than either of these previous studies, it is worth noting that we recorded a comparable number of injuries using SMS. Another study using SMS for injury self-reporting in elite female soccer players achieved even greater success, with 90% of injuries reported by players via SMS and only 38% by club-based personnel.13
A notable finding from this study was that the number of injuries reported by players decreased over the course of the season, but this was not associated with a change in the response rate. There are two possible alternate explanations for the decline in injury numbers. Firstly, previous studies using other data collection methods have also reported a decline in the occurrence of new injuries as the season progresses.27 ,28 This is because players are thought to become fitter and better adapted to the training and match loads over the course of the season.27 ,28 Another explanation for the decline in injury incidence is that participants may have become reluctant to report their injuries as the season progressed and, while they were still responding to the messages, they were not always responding reliably. It has been suggested previously that athletes may underreport their injuries in order to avoid missing matches.13 Although players were informed during the consenting process that their injury reports would not be shared between researchers and coaches, players may have still had some concerns about this. Further to this, players may also have deliberately answered ‘no’ to avoid future reminder messages and the follow-up phone call, which they may have found too time consuming or disruptive. As a possible solution, future research may wish to investigate linking SMS reminders to web-based questionnaires or mobile phone applications (‘apps’), allowing players to record the details of their own injuries. The ubiquitousness of ‘smartphones’ greatly enhances the capacity for these kinds of technologies to be used for research.19 However, the validity of such data would need to be carefully evaluated.
There are some disadvantages to consider in relation to the use of SMS technology for injury reporting. In this study, more than 2500 text messages were sent during the course of the football season. We were able to minimise the associated costs of sending this volume of messages by using an unlimited text messaging plan, charged at $A35 per month. However, although there were no issues raised by our participants, it cannot be assumed that all participants would be willing to bear the costs of replying to messages. Also, as with any electronic records, participants may be concerned about the privacy of their data and they may be reluctant to provide their personal mobile phone numbers. It is therefore vital that processes are implemented to ensure all privacy requirements are met. Finally, it should be acknowledged that, while SMS provided a fast and simple way of identifying which participants were injured, this study still involved a substantial amount of work for researchers in collecting and recording injury details via follow-up phone calls. Future research should investigate whether more detailed information on injury nature and mechanism can be obtained via SMS.
There may be limitations affecting the generalisability of our findings. Firstly, owing primarily to the absence of players from training on the night they were recruited, we only recruited 44% of all registered players. It is possible that we may not have achieved such high SMS response rates had a more complete sample been represented. Secondly, it is unknown whether or not the high response rates could be achieved with another age group. The mean age of participants was 25 years in this study and therefore, there was a clear advantage to using SMS with this population where there is almost universal mobile phone usage.19 Also, for pragmatic reasons, we did not ask participants any additional questions about training or match exposure. While this information would have been valuable for calculating exposure-adjusted injury rates, its inclusion may have led to a reduction in response rates. It would also have been useful to analyse whether the SMS response time increased over the season as an indicator of participant fatigue but because we only had access to 8 of the 18 rounds of response time data this analysis was not possible. Finally, while SMS injury reporting has been shown to be feasible, with a high response rate and fast response times, future research should evaluate the validity of data captured by SMS compared to traditional forms of injury reporting.
The shortage of resources and personnel in community sport has inhibited the development and implementation of any ongoing injury surveillance systems in this setting. Thus, novel solutions are required if we are to achieve sustainable access to data useful for prevention purposes. The use of SMS for injury self-reporting is still in its infancy but holds promise, being convenient for respondents and providing fast access to simple injury statistics. While there have been a handful of studies outside of sport that have used SMS to monitor injury recovery and for health reminders,24 ,29–31 there have been no other studies outside of sport that have used SMS for injury surveillance. Hence, there is still great scope to expand the use of SMS surveillance outside of the field of sports injury.
What is already known on this topic
-
A diverse range of injury reporting methods has been used in community sport, and there is currently no clear consensus on optimal injury surveillance methods for this setting.
-
Injury self-report via short message service (SMS) has been shown to be effective in elite sports and with schoolchildren.
What this study adds
-
We achieved a high response rate and fast response times using SMS for injury self-reporting in a sample of community Australian footballers.
-
Injury numbers declined throughout the football season, but this was unrelated to a decline in the response rate.
-
Injury self-report via SMS represents a feasible surveillance method for community sport and potentially elsewhere.
Acknowledgments
The authors are grateful to all of the players and club personnel who participated in this study, and thank Dr Alex Donaldson (Australian Centre for Research into Injury in Sport and its Prevention (ACRISP), Federation University, Ballarat, Victoria, Australia.) for his contributions to the design and execution of the study. Thanks also to Professor Jill Cook (Department of Physiotherapy, School of Primary Health Care, Monash University) and Professor David Lloyd (Centre for Musculoskeletal Research, Griffith Health Institute, Griffith University) for their contributions as chief investigators on the NoGAPS research project.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors CLE conceived and designed the study, analysed and interpreted the data and had major responsibility for the paper writing. BJG and CFF contributed to the design of the study, assisted with data analysis and contributed to the writing of the paper.
-
Competing interests None.
-
Ethics approval Monash University Human Research Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.