Article Text

Abstract
Objective To evaluate the effectiveness of oral glucosamine in subgroups of people with hip or knee osteoarthritis (OA) based on baseline pain severity, body mass index (BMI), sex, structural abnormalities and presence of inflammation using individual patient data.
Methods After a systematic search of the literature and clinical trial registries, all randomised controlled trials (RCTs) evaluating the effect of any oral glucosamine substance in patients with clinically or radiographically defined hip or knee OA were contacted. As a minimum, pain, age, sex and BMI at baseline and pain as an outcome measure needed to be assessed.
Results Of 21 eligible studies, six (n=1663) shared their trial data with the OA Trial Bank. Five trials (all independent of industry, n=1625) compared glucosamine with placebo, representing 55% of the total number of participants in all published placebo-controlled RCTs. Glucosamine was no better than placebo for pain or function at short (3 months) and long-term (24 months) follow-up. Glucosamine was also no better than placebo among the predefined subgroups. Stratification for knee OA and type of glucosamine did not alter these results.
Conclusions Although proposed and debated for several years, open trial data are not widely made available for studies of glucosamine for OA, especially those sponsored by industry. Currently, there is no good evidence to support the use of glucosamine for hip or knee OA and an absence of evidence to support specific consideration of glucosamine for any clinically relevant OA subgroup according to baseline pain severity, BMI, sex, structural abnormalities or presence of inflammation.
- osteoarthritis
- glucosamine
- individual patient data
- meta-analysis
- subgroups
Statistics from Altmetric.com
Introduction
Oral glucosamine has long been recommended for the treatment of knee and hip osteoarthritis (OA). However, recent guidelines by Osteoarthritis Research Society International (OARSI)1 and The National Institute for Health and Care Excellence (NICE)2 highlight the lack of support for the efficacy of oral glucosamine for the management of symptoms or disease modification in OA.3 With increasing study quality over the past decades, reported effect sizes for glucosamine have decreased.4 Furthermore, methodological issues in trials studying the effect of glucosamine for OA symptoms, such as inadequate allocation concealment and absence of intention-to-treat analyses, has resulted in overestimation of its effectiveness.5 A network meta-analysis from seven high-quality, large (>200 participants per trial) randomised controlled trials (RCTs) concluded that oral glucosamine was not superior to placebo in reducing OA pain or reduction in joint space narrowing.3
Notwithstanding the overall lack of efficacy of glucosamine, it is possible that certain subgroups of OA might respond differently (either better or worse) to any specific treatment.6 These subgroups might be based on different pathologies underlying the clinical presentation of OA, different disease stages or on the presence of different comorbidities.6 Accordingly, clinical guidelines increasingly call for the identification of any predictors of response to different treatment modalities.7 Since the effectiveness of glucosamine varies among different populations,4 5 8 it is possible that glucosamine might show higher efficacy when targeted at specific subgroups.
Recently, van Middelkoop et al9 reported on the methodology and legal structure to perform individual patient data (IPD) meta-analyses to identify clinically relevant subgroups that may show differential response to different OA treatments (the OA Trial Bank). The proposed methodologically robust method tests subgroup–treatment interaction effects using IPD from multiple published trials and allows for adjustment for confounding at both study and individual patient levels.9 Using this method, increased short-term efficacy for glucocorticoid treatment among knee OA patients with more severe pain has been demonstrated.10
The present study aimed to collect IPD of all RCTs performed for oral glucosamine in people with knee and hip OA to evaluate the efficacy within predefined subgroups of OA based on pain severity, body mass index (BMI), sex, structural abnormalities and presence of inflammation.
Methods
Systematic search
To identify all available RCTs, a systematic search of the literature was performed in PubMed, the Cochrane Central Register of Controlled Trials, Embase, Web of Science, Cinahl and Scopus. The search strategy was based on the search protocol of the Cochrane publication on the effectiveness of glucosamine.8 It was adjusted for the different databases and limited to publications from 1994 because of the likelihood of communicating with corresponding authors and data being available (searched up to March 2014 and available on request). Reference lists were hand searched for further identification of published work. Additional potential ongoing studies were searched for in clinical trial registries.
Two authors (JR and RR) independently selected citations based on titles and abstracts. Subsequently, full articles were obtained for those citations thought to fulfil the inclusion criteria and were independently assessed by the two review authors. A third review author was consulted if consensus was not reached (MvM). No protocol was registered for the current project, but full protocol details for the systematic review and the IPD meta-analysis were prespecified in the data delivery licence agreement that was approved by all members of the OA Trial Bank Steering Committee before the systematic search of the literature was initiated (available on request).
Inclusion/exclusion criteria
All RCTs evaluating the effect of any oral glucosamine substance in participants with knee or hip OA were included. This included studies testing the effects of glucosamine within a subgroup of participants with OA. Studies solely testing a combination of glucosamine with another substance (eg, chondroitin) were not included. There was no language restriction.
Participants
Participants were men and/or women with a diagnosis of OA of the knee or hip:
according to ACR classification criteria11 or
on the basis of detailed clinical and/or radiographic information.
Studies including a subgroup of knee or hip OA patients were also included, because IPD were collected.
Interventions
All comparisons between different oral glucosamine doses or between different frequencies of intake were included. Cointerventions were allowed as long as they were identically applied to the glucosamine and control group.
Comparator
All comparisons between oral glucosamine and any placebo/medication/dietary supplement/other non-surgical treatment were included.
Outcomes
The minimum criterion for inclusion of RCTs was adequate reporting of pain as an outcome measure.
Baseline predictors
1. Important data
As a minimum, severity of pain, age, sex and BMI should have been assessed at baseline in order to define subgroups.
2. If available
Signs of inflammation, either by physical examination (warmth and effusion) or by additional testing (ultrasound, MRI, biopsy and serum c-reactive protein (CRP)/erythrocyte sedimentation rate (ESR)), and structural abnormalities by radiography or magnetic resonance imaging (MRI)at baseline.
Data collection, transfer and checks
All corresponding authors of eligible trials were approached and asked to share trial data (first by email, subsequently by telephone). When corresponding authors could not be reached, the other listed authors and the institutes in which the trials had been performed were contacted. All data-deliverers willing to participate (ie, the research institutes who own the data) were asked to sign the data delivery licence agreement, including items on input data, obligations, ownership of data, terms, authorship, all subgroup analyses and publications. All anonymous data were transferred to a secured database at the Erasmus University Medical Center Rotterdam. On receiving the data, a thorough check of the data took place by reproducing the main baseline characteristics and the reported changes over time for the available outcome measures. Uncertainties were resolved in collaboration with the trialists.
Risk of bias assessment
The methodological quality of all included trials in the OA Trial Bank were assessed using the 12 criteria recommended by Cochrane (see online supplementary file 1) and were evaluated independently by two researchers (JR and RR). The criteria were scored as ‘yes’ (low risk of bias), ‘no’ (high risk of bias) or ‘unclear’. Any disagreement between the review authors was resolved by discussion, including input from a third review author (MvM). A study with a low risk of bias was defined as fulfilling six or more of the criteria items. In case the number of shared studies would allow proper interpretation (≥10 studies), funnel plots were considered for evaluation of publication bias.
Supplementary file 1
Data analyses
First, heterogeneity of the eligible studies was determined for the primary outcomes, using a two-stage meta-analysis approach in Review Manager V.5.3. In case of high heterogeneity (I2 index >50), sensitivity analyses without data from trials causing the heterogeneity were planned. Second, a descriptive comparison between studies was performed. We assumed missing data to be missing at random. Therefore, missing data for covariates and outcome measures were imputed, using multiple imputation methods, within each original study. Outcomes measured on different scales were standardised in order to pool the data. Predefined subgroup factors were dichotomised, based on consensus of the OA Trial Bank Steering Committee. For this, descriptive statistics of the subgroup variables for each of the five trials were shared with the Steering Committee, together with proposed cut-off values, based on literature, data separation in the available trials and previous IPD meta-analysis by the OA Trial Bank.10
The primary outcome measures were pain severity in the short-term (3–6 months) and at long-term (≥1 year) follow-up. Secondary outcomes were physical function and all forms of structural changes at these time points.
A one-stage multilevel regression analysis was performed to estimate the magnitude of the effect (estimated pooled mean differences) of glucosamine over the control intervention over all included studies and in the different subgroups with the individuals nested within each study. A single covariate was added to the regression models to indicate the study (fixed factor), in order to adjust for possible residual confounding by study differences. To assess possible subgroup effects, a random-effects linear regression model was used to determine interaction effects. This model included the dependent variable (primary or secondary outcome measure), the independent variable (treatment group), the effect modifier (subgroup indicator) and an interaction term (independent variable × effect modifier). All analyses were adjusted for age sex, BMI, Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) pain at baseline and were performed with and without stratification for type of glucosamine and with and without stratification for the affected joint. Comparisons and subgroup analysis for which only one RCT was available were not taken into account, since main effects were already studied in the original publication, and individual trials usually were not powered for subgroup analysis. A p value <0.05 was regarded as statistically significant in all analyses, using IBM SPSS software V.22.
Results
The literature search resulted in 1377 abstracts. After screening, 58 publications were evaluated in full-text and 18 fulfilled all inclusion criteria,12–29 with two additional trials identified from the references of the included trials30 31 (figure 1). Searching the clinical trial registries resulted in one additional potentially eligible trial (NCT01074476). All 21 corresponding authors of these trials were contacted for participation. After multiple efforts to contact all data owners of the eligible trials, authors/institutes of six studies agreed to participate and delivered trial data to the OA Trial Bank.14–16 24 28 29 Corresponding authors of two trials indicated that trial data were no longer available.13 23 Two corresponding authors did reply positively to the initial request for data sharing, but a signed licence agreement was never received.12 20 One corresponding author was not interested in participation.17 No contact was established with any of the authors nor the research institutes of five studies,18 21 26 30 31 and the one study identified in the clinical trial registry. Four data owners indicated that they were not permitted to share their data by the study sponsor.19 22 25 27 See table 1 for full details of all eligible studies.

Study flow chart. IPD, individual patient data; OA, osteoarthritis; RCT, randomised controlled trials.
Characteristics of all eligible and contacted studies (stratified for authors’ reply on data sharing request)
Five out of the six studies willing to participate involved knee OA participants,14–16 24 29 while only one involved hip OA participants.28 Follow-up duration in the six trials ranged from 3 to 24 months. Three studies evaluated glucosamine sulfate (GS)15 16 28 and two glucosamine hydrochloride (GH).14 29 The publication of the remaining study stated that the first 163 subjects received GS but that the subsequent subjects received GH.24 However, after extensive communication with the trial owner, the order of glucosamine type was deemed to be a typographical error, since the supplier of the glucosamine for the latter part of the participants (Rottapharm) is renowned for its GS. Data on participants within this trial were allocated to the stratified analysis for glucosamine type based on this new insight of the glucosamine type provided. With the exception of the trial by Coulson et al that used green-lipped mussel extract as comparison,15 all studies compared their glucosamine substrate against placebo. The trial by Coulson et al was therefore not included in the subgroup analysis (mean change in WOMAC pain −1.6 (−3.7 to 0.6) on a 0–20 scale in favour of glucosamine (p=0.157)).15 The trial by Sawitzke et al29 presented long-term follow-up from the Clegg et al,14 but since both publications report on different outcome measures of interest (clinical data and radiography vs clinical data only) and risk of bias could be assessed for both publications separately, both were indicated as separate trials. No important issues were identified when checking shared trial data, but for the trial by McAlindon24 for which data of the first 199 (out of 205 in the original publication) could be retrieved by the trial owners. No relevant differences in baseline characteristics for the subjects with shared data and the published data were observed. Percentages of missing data for the main baseline characteristics and all outcome measures for each of the five individual trials are presented in online supplementary table 2 . All listed variables were used in the multiple imputation by the SPSS software package, creating 20 imputed data sets for each trial.
Supplementary file 2
The five trials included in the analysis included a total number of 1625 participants (64% women), 815 randomised to glucosamine and 810 to placebo. This reflected 55% of the participants randomised in the 17 published RCTs on glucosamine versus placebo. Pain was measured in all five studies using the ordinal WOMAC questionnaire.32 Scores were rescaled to a 0–100 scale and defined at short-term (closest to a minimal of 3 months follow-up) for the trials by McAlindon et al.,24 Clegg et al,14 and Rozendaal et al28 and long-term (2 years follow-up) for Fransen et al.,16 Sawitzke et al,29 and Rozendaal et al.28 Physical function was also measured in all five studies using the WOMAC questionnaire and was rescaled and defined in an identical matter. Figure 2 presents the overall mean differences of these five trials for the primary outcome at short term and long term, based on the imputed data sets.
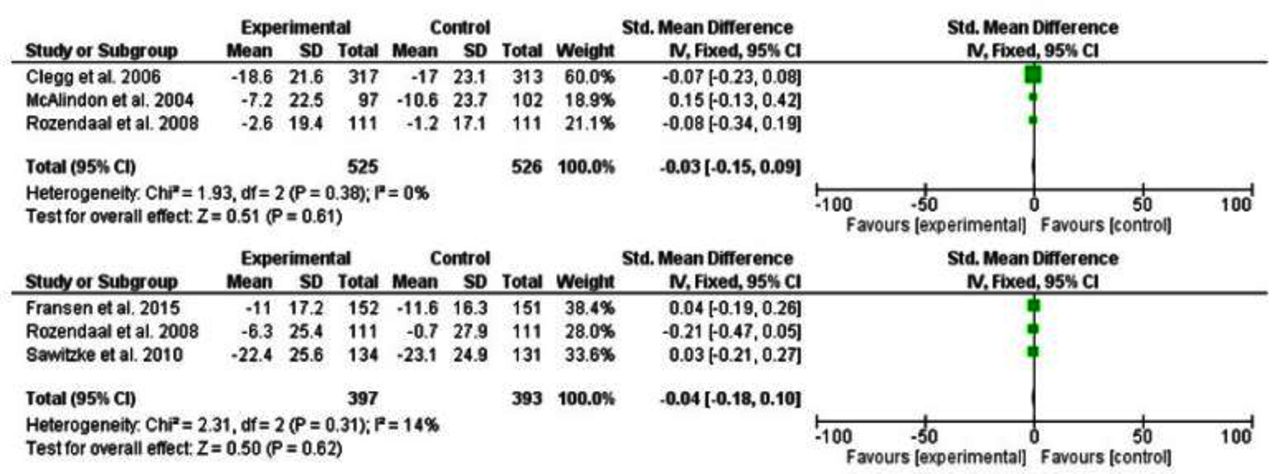
Forest plots for mean change in WOMAC pain at short-term (upper panel) and long-term (lower panel) on a 0–100 scale for studies that shared trial data.
The following subgroups were defined: WOMAC pain <70 versus ≥70, BMI <27 kg/m2 versus ≥27 kg/m2, Kellgren and Lawrence grade33 (KL-grade) 0–2 versus KL3-4 and presence versus absence of inflammation. Presence of inflammation was defined as either presence of swelling/effusion on clinical examination14 29 or an elevated erythrocyte sedimentation rate (ESR),28 defined as ESR ≥20 mm/h for men aged ≥50 years, ESR ≥15 mm/h for men aged <50 years, ESR ≥30 mm/h for women aged ≥50 years and ESR ≥20 mm/h for women aged <50 years. Inflammation data were only available when combining data from one knee OA14 29 and one hip OA trial.28 Therefore, no additional stratification was possible. Baseline Kellgren and Lawrence grades were only available in one knee OA trial with short-term outcomes,14 two knee OA trials with long-term outcomes16 29 and the one hip OA trial28 with short-term and long-term outcomes. Given this lack of consistency, stratification of the subgroup analysis was done for knee OA trials only on long-term outcomes.
Risk of bias and heterogeneity
All five studies were defined as having a low risk of bias (table 2) and heterogeneity was low (I2=0 for main effects on pain at short and I2=14 for long-term follow-up, see figure 2), so no sensitivity analyses were performed.
Risk of bias assessment of studies included in glucosamine versus placebo comparison
Overall intervention effects
Estimated pooled differences for the primary and secondary outcome measures are presented in table 3. No statistical significance main effects were found for glucosamine over placebo.
Estimated pooled differences (95% CI) between glucosamine and placebo on a 0–100 scale (positive values indicate a greater reduction in the outcome measure for glucosamine) and p values for treatment–subgroup interactions
Subgroup effects
None of the interaction terms of the predefined subgroups reached statistical significance (see table 3). Estimated pooled differences within each subgroup for the primary outcomes over all eligible trials are presented in figure 3. Within the stratified analyses among studies using GS for knee OA, the number of subjects with high baseline pain was too small for the software to test the pooled interaction term for the baseline pain severity subgroup.

{kind=link}
{kind=link}
{kind=link}
Estimated pooled differences between glucosamine and placebo within predefined subgroups for all eligible trials. Positive values indicate a greater reduction in the outcome measure for glucosamine. Red figures represent low pain (WOMAC pain <70), low BMI (<27 kg/m2), male sex, K&L grades 0–2 and absence of inflammation subgroups, respectively. Blue figures represent high pain (WOMAC pain ≥70), high BMI (≥27 kg/m2), female sex, K&L grades 3–4 and presence of inflammation subgroups, respectively. BMI, body mass index; K&L, Kellgren and Lawrence grade.
Discussion
To our knowledge, this is the first IPD meta-analysis to examine potential subgroup effects of oral glucosamine for people with OA. Within the five trials where the authors were willing to share their data, 1625 patients with knee or hip OA were analysed. This represents 55% of all available participants from the placebo controlled trials for this product. The main findings are: (1) overall, glucosamine was no better than placebo for both pain and function outcomes; (2) in subgroup analyses, glucosamine was no better than placebo according to baseline pain severity, BMI, gender, structural abnormalities and presence of inflammation; and (3) the majority of trials were knee OA (four trials, 1403 patients), and the analysis based on knee OA only had similar results.
Several systematic reviews and network meta-analyses have shown that as the number of high-quality and industry-independent studies on the effectiveness of glucosamine for OA increased over time, the results of earlier studies that showed beneficial effects of glucosamine were viewed as less credible.3–5 8 34 35 It is therefore not surprising that the present IPD meta-analysis also showed no significant main effects, especially since previous studies showed a low risk of bias to be associated with small, non-significant effect sizes for glucosamine over placebo3 8 34 and the fact that all included studies had a low risk of bias. Present results of overall treatment effects within the trials that shared data and over the different stratifications ranged from −0.43 to 2.02 on the 0–100 WOMAC pain scale, which is comparable with the overall treatment effects for industry independent studies (0.1 (95% CI −0.2 to 0.5)) for visual analog scale (VAS) pain on a 0–10 scale) presented by the meta-analyses of Wandel and colleagues.3 In the literature, overall beneficial effects of treatment have been reported in studies using the glucosamine compound produced by Rottapharm4 5 8 34; however, these trials were not made available to the study team for the current analyses.
Extending previous initiatives, the present study also evaluated treatment effects of glucosamine over placebo for several clinically relevant subgroups of OA, made possible by the IPD from the collaborating trials. Despite the large number of participants incorporated in the IPD meta-analysis, none of the interaction terms reached statistical significance. The interactions with BMI among knee OA patients receiving GS on short-term function (p=0.12) and on long-term pain (p=0.10) were the only outcomes for which further research may be warranted. However, given the number of analyses performed in the study, incidental findings are certainly possible.
The currently used cut-off for the baseline pain severity subgroup is somewhat comparable with the strata used in the Clegg et al study14 to test for different effects within subjects with mild pain (WOMAC pain scores 0–60) versus those with moderate to severe pain (WOMAC pain scores 60–80). The Clegg et al study was not powered to show subgroup effects, but the non-significant effects of glucosamine over placebo within both subgroups is corroborated by the present results.
The current study has several limitations. Despite all efforts, data from only six of the 21 identified studies were acquired. Of those studies not included in the present study, the largest groups were those not responding to any of the requests for data sharing (six studies) and those not permitted by the commercial study sponsor to share data (four studies) (see table 1). Although missing data for the main baseline characteristics within the data shared with the OA Trial Bank were limited, multiple imputation methods were needed to deal with the missing data in the outcome measures that ranged from 2% to 46%. Within the trials that shared data, only a few measured the predefined subgroups based on structural abnormalities and presence of inflammation. The available data for these subgroups combined studies evaluating different glucosamine substances for different OA joints. Therefore, rigorous stratification of the analysis was not possible with the available data.
Open access to data of clinical trials has been proposed and debated for several years.36-38 Nevertheless our experience, in common with others, suggests that currently this is far from accepted practice.39 Thus, the full potential and use of completed clinical trials is not reached and only part of the clinical evidence is available to clinicians and patients, thus threatening the appropriateness of recommendations for clinical decision making.39 Once initiatives such as the OA Trial Bank, which appropriately use existing data for scientific purposes, become more established and generally accepted, authors and commercial parties involved in clinical research may become more confident in data sharing. The OA Trial Bank plans to update publications every 5 years and will again approach data owners that chose to not share their data to the OA Trial Bank in the first initiative.
The aim of the present study was to perform an IPD meta-analysis on all available RCTs on glucosamine in people with OA. After performing the systematic search of the literature and clinical trial registers, it took 18 months to reach as many data owners as possible and to collect and check all data of those willing to deliver their trial data. For a systematic review, one might argue that an update of the search strategy is warranted. However, given the time-consuming efforts of sharing data between research institutes, this was not feasible for the present study.
In conclusion, the current IPD on the efficacy of glucosamine for subgroups of OA based on pain severity, BMI, sex, radiographic structural changes and presence of inflammation, using data from 55% of the participants available in literature and using data from low risk-of-bias trials only, did not identify a subgroup for which glucosamine showed any significant beneficial effects over placebo for pain or function in either the short term or long term. Stratification only for participants with knee OA or for type of glucosamine did not result in any differences in outcomes. Therefore, currently, there is no evidence to support the use of glucosamine for treatment of hip or knee OA in general and an absence of evidence to support the use of glucosamine for clinically relevant subgroups of OA according to baseline pain severity, BMI, sex, structural abnormalities and presence of inflammation.
Acknowledgments
All data owners (researchers and institutes) are to be acknowledged for providing their data to the OA Trial Bank.
References
Footnotes
Handling editor Tore K Kvien
Contributors JR, MvM, HJWB, MD, KSD, LSL, TM, WZ and SBZ have substantially contributed to the conception and design of the work. JR and RMR have substantially contributed to the acquisition of the data and drafted the manuscript. All authors contributed to the analysis and interpretation of the work, revised the manuscript critically for important intellectual content, approved the final version of the manuscript and agreed to be accountable for all aspects of the work.
Funding The current project received funding by the Dutch Arthritis Foundation (BP12-1-161). KSD is part funded by the National Institute for Health Research (NIHR) Collaborations for Leadership inApplied Research and Care West Midlands and by a Knowledge Mobilisation Research Fellowship (KMRF-2014-03-002) from the NIHR. This paper presents independent research funded by the National Institute for Health Research (NIHR). The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health. WZ is supported by a grant from Arthritis Research UK. TEM is supported by grants from Sanofi Aventis, Abbvie, Fidia, Samumed and Pfizer and personal fees from Flexion Therapeutics, Samumed, Plexxikon Inc, Regeneron, Orthogen and McNeil Consumer HC. LSL is supported by personal fees from Galapagos NV, FlexionTherapeutics, Johnson & Johnson, Regeneron, Össur and Samumed.
Competing interests None declared.
Patient consent Two representatives of patient and public involvement (members of the Arthritis research UK OA Research Users Group) are official members of the Steering Committee of the OA Trial Bank. These representatives provided feedback on the design of the study, including study selection, selection and definitions of subgroups, and outcome measures. Also for dissemination activities of OA Trial Bank and for prioritisation of future research questions, the input from patient and public involvement is obtained.
Provenance and peer review Not commissioned; externally peer reviewed.