Article Text

Abstract
Objective: To compare the efficacy of aerobic walking and home based quadriceps strengthening exercises in patients with knee osteoarthritis.
Methods: The Medline, Pubmed, EMBASE, CINAHL, and PEDro databases and the Cochrane controlled trials register were searched for randomised controlled trials (RCTs) of subjects with knee osteoarthritis comparing aerobic walking or home based quadriceps strengthening exercise with a non-exercise control group. Methodological quality of retrieved RCTs was assessed. Outcome data were abstracted for pain and self reported disability and the effect size calculated for each outcome. RCTs were grouped according to exercise mode and the data pooled using both fixed and random effects models.
Results: 35 RCTs were identified, 13 of which met inclusion criteria and provided data suitable for further analysis. Pooled effect sizes for pain were 0.52 for aerobic walking and 0.39 for quadriceps strengthening. For self reported disability, pooled effect sizes were 0.46 for aerobic walking and 0.32 for quadriceps strengthening.
Conclusions: Both aerobic walking and home based quadriceps strengthening exercise reduce pain and disability from knee osteoarthritis but no difference between them was found on indirect comparison.
- ES, effect size
- RCT, randomised controlled trial
- osteoarthritis
- knee
- aerobic exercise
- strengthening exercise
Statistics from Altmetric.com
Osteoarthritis is the most common condition affecting synovial joints. Osteoarthritis of the knee causes substantial pain and disability, especially in the elderly, resulting in a significant burden on health care provision. The majority of patients with osteoarthritis are managed in primary care, and the prevalence of knee osteoarthritis is such that simple interventions which are effective in a community setting are necessary.
Treatment of osteoarthritis aims to reduce pain and disability. Recent guidelines1,2 for the management of knee osteoarthritis emphasise the central role of exercise. Both aerobic walking and quadriceps strengthening exercises have been shown to reduce pain and disability in subjects with knee osteoarthritis. Quadriceps strengthening, however, can be achieved in a variety of ways and many trials use complex hospital based regimens and sophisticated machinery not readily available to the majority of patients with osteoarthritis. Furthermore, comparatively few randomised controlled trials (RCTs) have directly compared the efficacy of aerobic and strengthening exercises and this issue was not addressed by three recent reviews.3–,5
In this systematic review, our objective was to compare the efficacy of aerobic walking and home based quadriceps strengthening exercises in reducing pain and disability in knee osteoarthritis.
METHODS
Retrieval of published studies
A comprehensive search was undertaken in the Medline, Pubmed, EMBASE, CINAHL, and PEDro databases and the Cochrane controlled trials register to identify RCTs of exercise. Medical subject headings used were “osteoarthritis, knee” combined with “exercise” or “exercise therapy.” Search terms were exploded. Reference lists from retrieved publications and review articles identified by the search strategy above were also searched. The computerised searches covered the period 1966 to September 2003. Hard copies of retrieved publications were obtained.
Inclusion and exclusion criteria
Only RCTs involving subjects with knee osteoarthritis were included. Trials were required to compare exercise therapy with a non-exercise control group. The exercise mode was scrutinised and the trial was only included if the regimen employed involved predominantly aerobic walking or home based quadriceps strengthening exercise. Exercise was considered to be “home based” where it was undertaken exclusively in the subject’s home environment or, where exercise was partly supervised, the regimen was intended to be continued at home unsupervised. The outcome measures of interest were pain or self reported disability or both.
RCTs were excluded if publication was in abstract form only or if the exercise regimen was perioperative. Only English language publications were considered. If an RCT included subjects with osteoarthritis of joints other than the knee and provided only aggregated data, the authors were contacted to request disaggregated data. The study was excluded if disaggregated data could not be provided.
Quality assessment
Two reviewers (ER, WZ) independently assessed the methodological quality of retrieved RCTs using a validated instrument.6 This system assesses randomisation, double blinding, and reporting of withdrawals and dropouts to allocate a quality score out of 5 for the trial.
Data abstraction/statistical analysis
Two reviewers undertook data abstraction independently (ER, WZ). A customised form was used to record the authors’ names, the year of publication, the trial design, the nature of the intervention and control, the duration of trial, the number of subjects in each treatment arm, and the mean age, sex, and body mass index (BMI) of subjects involved (that is, the potential confounding variables).
The primary outcome measure was pain and the secondary outcome measure was self reported disability. The mean and standard deviation (SD) of the baseline and final end point scores for pain and self reported disability were abstracted from each RCT. The mean change score (final end point minus baseline score) for each outcome measure was calculated for each intervention (exercise or control).
Where standard deviations were not provided they were calculated from standard error or 95% confidence intervals. RCTs that did not provide estimates of random variability or presented data as medians were not pooled.
The difference between the mean change score for the exercise and control groups and its standard deviation was calculated for each trial. The effect size (ES) was subsequently calculated.7 For pooling of data, RCTs were grouped according to whether the exercise regimen involved predominantly aerobic or strengthening exercise. For each of these groups, the pooled weighted ES was calculated as described previously.8 The Q statistic for heterogeneity was calculated.9 If RCTs were heterogeneous and no reason could be identified a random effects model was used.
RESULTS
Search of published reports
The search strategy identified 35 RCTs of exercise therapy for knee osteoarthritis.10–,44 The flow of RCTs through the analysis is shown in fig 1⇓. Twenty eight RCTs were potentially appropriate for inclusion17–,44 but seven of these did not include pain or self reported disability as outcome measures.17–,23 The authors of one other RCT were contacted for further information. This study24 gave only composite Western Ontario/McMaster Universities arthritis index (WOMAC) scores and omitted disaggregated scores for pain and physical function. No reply was received from the authors despite repeated attempts to contact them and so the study was excluded.
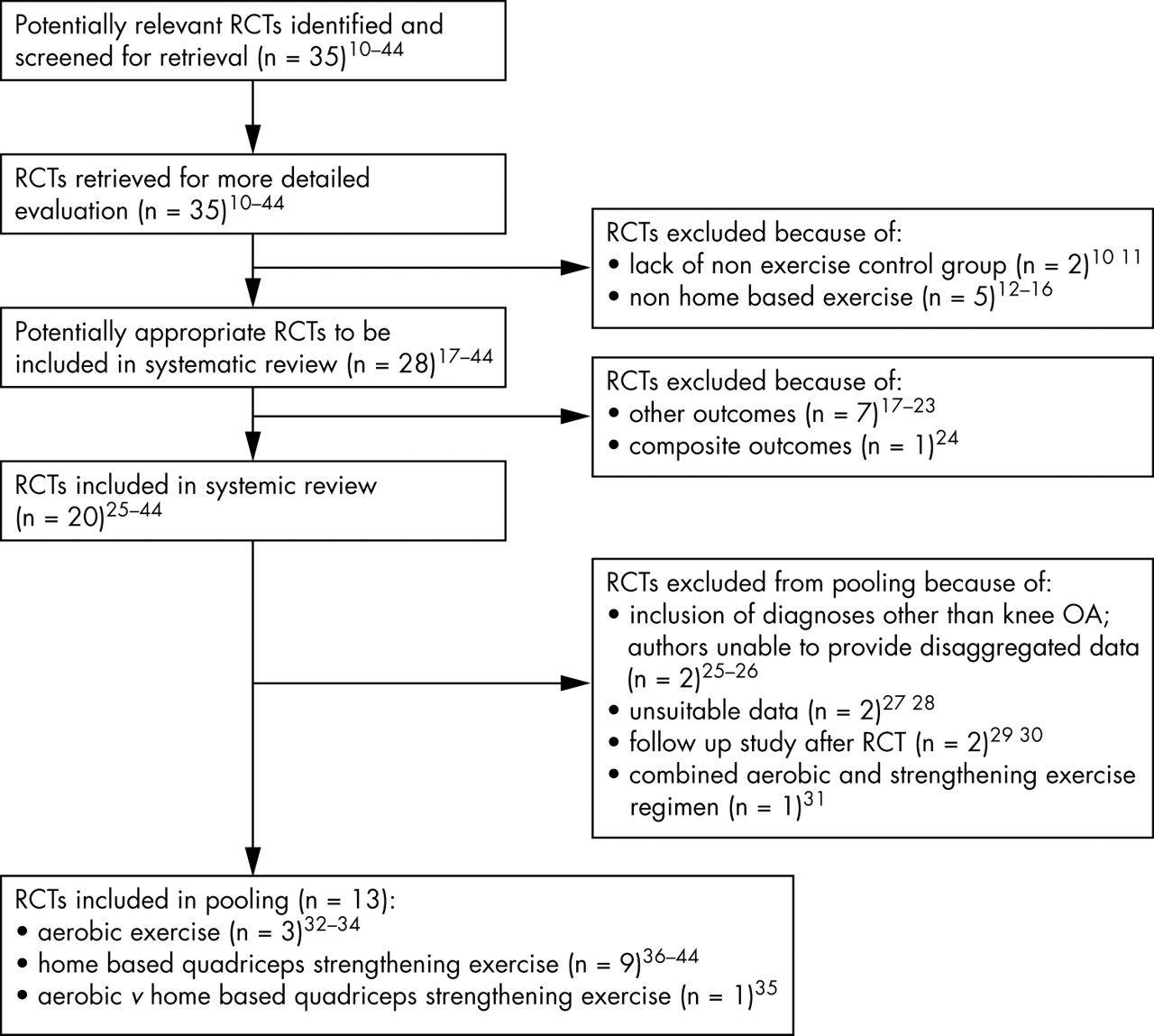
Flow of randomised controlled trials included in the systematic review.
Twenty RCTs therefore met our inclusion criteria. Seven of these were not suitable for pooling subsequently. The authors of one study of aerobic walking and aerobic aquatic exercise in subjects with hip or knee osteoarthritis or rheumatoid arthritis were contacted but were unable to provide data disaggregated for both the type of exercise and the location of the osteoarthritis.25 Contact was made with the authors of a small study of subjects with osteoarthritis of the hip or knee but disaggregated data were unavailable after a period of two months.26 Two studies presented data in a format unsuitable for pooling,27,28 two were long term follow up studies of previous RCTs,29,30 and one studied an exercise regimen which combined aerobic and strengthening exercises.31
The thirteen remaining RCTs were included (table 1⇓).32–,44 The authors of two studies that included subjects with hip or knee osteoarthritis were able to provide disaggregated outcome data.38,44
Characteristics of randomised controlled trials included in the meta-analysis
Interventions
The 13 RCTs included three studies in which the exercise intervention was predominantly aerobic walking32–,34 and one study comparing aerobic walking and home based strengthening exercises with control.35 Nine RCTs evaluated quadriceps strengthening exercises, in four of which exercise was undertaken exclusively in the home36,39,40,42 and in five supervised exercise was continued at home unsupervised.37,38,41,43,44 One study compared dynamic and isometric resistance training.43 Group and individual exercise were compared with control in one RCT37 but no significant difference between the two intervention groups was found and therefore combined data were analysed.
Use of non-steroidal anti-inflammatory drugs (NSAIDs) was an inclusion criterion in one study33 and another RCT prescribed an NSAID, oxaproxin 1200 mg daily, to all participants.40 Three studies specifically stated that NSAIDs were permitted36,43,44 and one study reported that no subjects were taking NSAIDs.32 In the remaining RCTs, it was not specified whether or not analgesic and anti-inflammatory agents were permitted.
Various control interventions were used including education and lifestyle advice,32,34–36,44 support by telephone calls,33 and no intervention.37–39,41–,43 In one RCT, the control group underwent a “sham” exercise programme in an attempt to achieve double blinding.40
Methodological quality
Methodological quality scores are shown in table 1⇑. None of the RCTs achieved a maximum quality score. Six scored three out of five 33,34,37,39,40,44. The most common source of likely methodological bias identified by the scoring system6 was a lack of double blinding, with all 13 studies failing to score on this criterion.
Primary outcome measure – pain
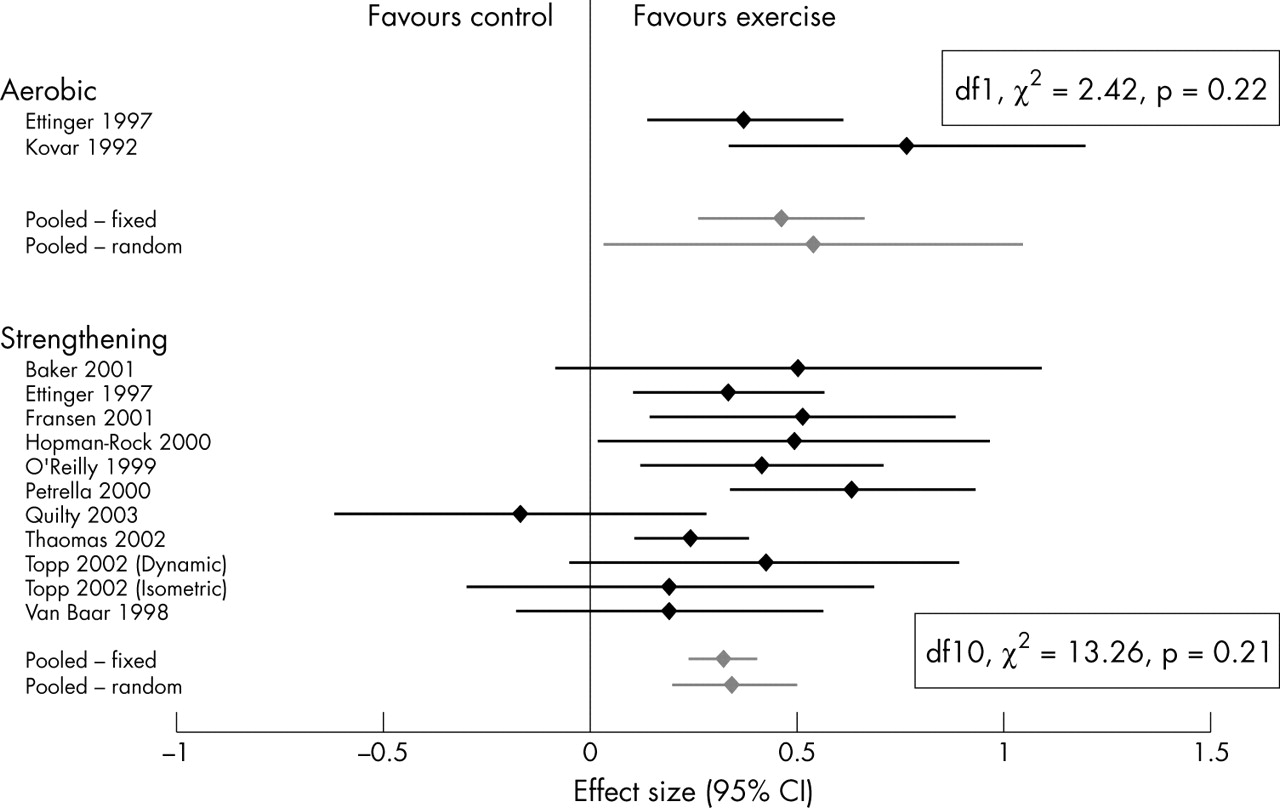
Pooling data for aerobic walking produced a weighted pooled effect size for pain of 0.52 (95% CI, 0.34 to 0.70) (449 subjects). Calculation of the effect sizes for RCTs of strengthening exercise revealed a much larger effect size for one study.40 This study differed from other studies of strengthening exercise in two ways: first, the NSAID, oxaprozin, was prescribed for all participants in both the intervention and control groups; second, subjects in the control group underwent a “sham” exercise programme. The study was therefore not pooled. This had the effect of producing more homogeneous pooled data (χ2 decreased from 43.46 (p<0.0001) to 8.97 (p = 0.44)). A pooled effect size of 0.32 (0.23 to 0.42) (2004 subjects) was seen for home based quadriceps strengthening exercise (fig 2⇓; pooled data excluding data from Petrella et al40).

Effect of exercise on pain.
Secondary outcome measure – self reported disability
Two RCTs of aerobic walking did not include self reported disability as an outcome measure.32,34 Pooling data from the two remaining RCTs produced a weighted pooled effect size for self reported disability of 0.46 (95% CI, 0.25 to 0.67) (385 subjects). For quadriceps strengthening exercise, the weight pooled effect size was 0.32 (0.23 to 0.41) (2004 subjects) (fig 3⇓).

{kind=link}
{kind=link}
{kind=link}
Effect of exercise on self reported disability.
DISCUSSION
Both aerobic walking and home based quadriceps strengthening exercises are effective at reducing pain and disability in subjects with knee osteoarthritis. No advantage of one form of exercise over the other was found on indirect comparison of pooled data. That both interventions are effective has implications for clinical practice. Adherence is a major predictor of response to exercise, and offering patients the choice between two effective interventions has the potential to improve adherence and hence outcome. To make a full comparison of the relative efficacy of aerobic walking and quadriceps strengthening exercise requires an adequately powered RCT, and a factorial design would allow the interaction between both forms of exercise to be investigated.
The RCTs of strengthening exercise produced similar effect sizes for pain, apart from one study which had a much larger effect size of 1.36 (95% CI, 1.03 to 1.69).40 This study differed in its methodology by prescribing the NSAID, oxaprozin, to all participants and also by exposing the control group to a “sham” exercise programme in an attempt to achieve double blinding. This study was not pooled, with the effect that the pooled effect size was reduced slightly from 0.40 to 0.32. The pooled data also became homogeneous on exclusion of this study, allowing the use of a fixed effects model. The study was excluded on similar grounds by the recent Cochrane review.3 Disability data from this study were pooled because they did not appear grossly different from other studies.
A limitation of our study is the small number of RCTs of aerobic walking. This was studied in four RCTs but only two of these included disability as an outcome measure. Furthermore, three RCTs of quadriceps strengthening exercise meeting inclusion criteria had to be excluded on the grounds of unsuitable or insufficient data.24,27,28
A major source of difficulty in RCTs of exercise therapy and other non-pharmacological interventions that require patient participation is the issue of double blinding. None of the RCTs included scored any points for double blinding on assessment of methodological quality. One study is described as double blind on the basis of a “sham” exercise programme in the control group.40 However, points for double blinding were not allocated as we do not believe exercise can be genuinely double blinded like in a placebo controlled trial of a pharmacological intervention. Similarly, six RCTs are described as single blind35,36,38,41,42,44 and, although this does not affect the quality score by the method used,6 we question whether this can be achieved.
Although we have demonstrated that both aerobic and strengthening exercise are effective for knee osteoarthritis, the best way to deliver strengthening exercise is still unclear. There was considerable variation in the content and duration of the exercise programmes included in our systematic review. Length of intervention ranged from eight weeks to two years. There was also variation in the interventions that were combined with strengthening exercise (for example, lifestyle advice, patellar taping, and NSAIDs). Adherence to both aerobic walking and strengthening exercise is a key predictor of response,35,42 and encouraging patients with knee osteoarthritis to maintain exercise programmes beyond a supervised period of instruction is a major challenge.
Conclusions
Both aerobic walking and home based quadriceps strengthening exercise are effective in subjects with knee osteoarthritis. Further direct comparison is required to identify the relative efficacies of aerobic walking and home based quadriceps strengthening exercise and examine any interaction between them.
Acknowledgments
We are indebted to the Arthritis Research Campaign, UK for financial support (ICAC grant D0593; WZ senior lectureship D0565). We would also like to thank Dr Marijke Hopman-Rock and Dr Margriet Van Baar for providing study data disaggregated for site of osteoarthritis.