Article Text

Abstract
Objective To determine if the dietary supplements, glucosamine and/or chondroitin, result in reduced joint space narrowing (JSN) and pain among people with symptomatic knee osteoarthritis.
Methods A double-blind randomised placebo-controlled clinical trial with 2-year follow-up. 605 participants, aged 45–75 years, reporting chronic knee pain and with evidence of medial tibio-femoral compartment narrowing (but retaining >2 mm medial joint space width) were randomised to once daily: glucosamine sulfate 1500 mg (n=152), chondroitin sulfate 800 mg (n=151), both dietary supplements (n=151) or matching placebo capsules (n=151). JSN (mm) over 2 years was measured from digitised knee radiographs. Maximum knee pain (0–10) was self-reported in a participant diary for 7 days every 2 months over 1 year.
Results After adjusting for factors associated with structural disease progression (gender, body mass index (BMI), baseline structural disease severity and Heberden's nodes), allocation to the dietary supplement combination (glucosamine–chondroitin) resulted in a statistically significant (p=0.046) reduction of 2-year JSN compared to placebo: mean difference 0.10 mm (95% CI 0.002 mm to 0.20 mm); no significant structural effect for the single treatment allocations was detected. All four allocation groups demonstrated reduced knee pain over the first year, but no significant between-group differences (p=0.93) were detected. 34 (6%) participants reported possibly-related adverse medical events over the 2-year follow-up period.
Conclusions Allocation to the glucosamine–chondroitin combination resulted in a statistically significant reduction in JSN at 2 years. While all allocation groups demonstrated reduced knee pain over the study period, none of the treatment allocation groups demonstrated significant symptomatic benefit above placebo.
Trial Registration ClinicalTrials.gov identifier: NCT00513422; http://www.clinicaltrials.gov
- osteoarthritis knee
- glucosamine
- chondroitin
- pain
- disease progression
Statistics from Altmetric.com
Osteoarthritis (OA) continues to be one of the leading causes of ‘years lived with disability’ worldwide.1 ,2 Symptomatic knee OA is highly prevalent among people aged 50 years and over in most parts of the world.3 To date there is no known cure for OA and no intervention has been unequivocally demonstrated to slow disease progression or delay time to joint replacement surgery.
Glucosamine and chondroitin are naturally occurring compounds in the body; they are the principal substrates in the biosynthesis of proteoglycan, a compound essential for maintaining cartilage integrity. While glucosamine and chondroitin were developed as prescription drugs for OA in Europe and Asia, in the USA and Australia they are available as over-the-counter products. Glucosamine and/or chondroitin are purchased by many people in the hope that these supplements will relieve joint pain and slow the rate of joint destruction and cartilage loss. In the population-based ‘The 45 and UP Study’ of more than 260 000 people in New South Wales, Australia, 22% reported using glucosamine ‘in the past month’.4
A Cochrane systematic review evaluating the effects of glucosamine identified 25 randomised clinical trials, and concluded that only studies using the original prescription formulation of glucosamine sulfate showed superiority against placebo on pain and function.5 For chondroitin, a recent systematic review of 20 controlled trials determined that ‘no robust evidence supports the use of chondroitin in osteoarthritis’ as trial quality was generally poor.6 A later review demonstrated a small but significant reduction in joint space narrowing (JSN) in a pooled analysis of three studies of at least 2 years’ duration.7 The GAIT study, which is the only published large randomised clinical trial evaluating a glucosamine hydrochloride–chondroitin sulfate combination regimen for symptomatic knee OA, found no overall long-term symptomatic or significant structural benefit.8 ,9 However, an exploratory analysis of participants with moderate to severe pain at baseline did suggest symptomatic benefit from the glucosamine–chondroitin combination.
International guidelines for the management of OA remain equivocal in their recommendations for glucosamine and chondroitin.10 ,11 Significant heterogeneity of outcomes and considerable evidence of publication bias favouring positive studies has been noted.10 However these dietary supplements, taken either singly or in combination, remain very popular among people with joint problems. The primary objective of the Long-term Evaluation of Glucosamine Sulfate (LEGS) study is to determine whether glucosamine sulfate, chondroitin sulfate or the combination of both of these dietary supplements, limit or reduce structural disease progression (cartilage loss) or provide pain relief to people with chronic knee pain due to OA.
Methods
We undertook a double-blind randomised placebo-controlled trial, the LEGS study. Participants were recruited through general media advertising and primary care centres in New South Wales, Australia, over a period of two years (2007–2009). Informed consent was obtained from all study participants and approval for the study was granted by the Human Research Ethics Committee, University of Sydney (No 8821). The LEGS study was registered with ClinicalTrials.gov (NCT00513422).
Participants
Potential participants were initially screened by telephone to confirm: knee pain for more than 6 months; knee pain on most days of the past month (or taking analgesics); not having rheumatoid arthritis, bilateral knee replacements or unstable diabetes; no allergy to shellfish; no lower limb surgery in the past 6 months; not planning to have a knee replacement in the next year; no intra-articular injection for knee pain in the past 3 months; and ‘worst pain’ experienced in left and right knee over the past week rated as 4 or more on a scale of 0–10. Individuals with diabetes or taking warfarin were provided with written advice encouraging increased vigilance with glucose or INR monitoring.
Weight-bearing magnification-controlled semi-flexed radiographs were taken of both knees at one of four specific radiology centres,12 using the strictly standardised metatarsophalangeal protocol and foot maps.13 The study protocol allowed a single repeat, increasing the angulation of the beam, if the medial tibial inter-rim distance (TIRD) was >2.0 mm.14 To be eligible, a sufficiently symptomatic knee needed to demonstrate reduced medial tibio-femoral compartment joint space width, compared with the lateral compartment, but retain at least 2.0 mm minimum medial joint space width.
Clinic assessment (baseline, year 1, year 2)
On each assessment occasion height, weight, history of knee surgery or significant trauma, self-reported presence of pain or ‘arthritis’ in other joints, presence of Heberden's nodes, responses to the Self-Administered Co-morbidity Questionnaire15 and all current medications were evaluated. Knee pain and physical function was assessed using the Western Ontario and McMaster Universities (WOMAC) OA Index, a well validated, disease-specific questionnaire which includes two subscales—pain (0–20) and physical function (0–68)—with higher scores indicating greater pain or loss of physical function.16 Health-related quality of life was measured using the Medical Outcomes Study Short Form (SF-12v2) questionnaire, which provides two summary measures: the Physical Component Summary Scale Score (PCS) and the Mental Component Summary Scale Score (MCS).17 The PCS and MCS are population norm-based scores with a mean (SD) of 50 (10), higher scores indicating better health-related quality of life. Participants also completed a 50-foot walk time, with the instruction to ‘walk as fast as you safely can’.18
Run-in, randomisation and masking
On completion of the baseline assessment, potential participants were provided with a 2-week supply of placebo study capsules (blinded to content) and the 7-day LEGS study participant diary. Only participants returning a completed 7-day participant diary and confirming ongoing study commitment were randomised. The randomisation schedule was based on randomly permuted blocks of different sizes generated by an independent statistician and placed in a password-protected file unavailable to study staff responsible for screening and recruitment. All assessments were conducted by researchers blinded to treatment allocation.
Study treatments
In this 2×2 factorial design clinical trial, all participants were randomly assigned (1 : 1) to take, once daily, two capsules each of: glucosamine sulfate potassium chloride or matching placebo; and chondroitin sulfate or matching placebo. Each glucosamine sulfate capsule contained 753 mg glucosamine sulfate as a water-soluble white powder. Each chondroitin capsule contained 400 mg of bovine-derived, low molecular weight chondroitin sulfate. The chondroitin was manufactured by TSI Health Sciences (Australia) in accordance with the Therapeutic Goods Administration (TGA) of Australia requirements to minimise the risk of transmitting transmissible spongiform encephalopathies. Placebo capsules were indistinguishable from their active comparator in look, taste, smell and packaging. All other study treatment capsules (including placebo) were supplied by Sanofi-Aventis Consumer Healthcare (formerly Symbion Consumer) and manufactured under Good Manufacturing Practice conditions where the quality reference for ingredients is the United States Pharmacopoeia. Chemical analysis of purity and active ingredient content of a randomly selected sample of the active study treatment capsules was conducted by an independent laboratory (Chemika, Australia) immediately after delivery of each batch of study treatment capsules to the dispatching centre. At each analysis, purity and stated active ingredient content was confirmed. Participants were contacted by telephone or email every 2 months to verify delivery address and report any medical adverse events.
Participant diary
The 7-day participant diary was sent every 2 months with the study treatment capsules for 2 years (see online supplementary appendix S1). Participants were to start reporting on the day the participant diary was received:
-
At its worst, how much pain did you have in your knee today?’ (numeric rating scale, 0–10). The maximum score recorded over 7 days was used.
-
Considering all the ways your knee arthritis affects you, how would you say your knees are today? (excellent 0, very good 1, good 2, fair 3, poor 4). The average score over 7 days was dichotomised with values >2.5 designated a ‘poor’ global assessment.
-
Did you participate in any moderate or vigorous recreational exercise that lasted longer than 20 min today? (yes/no). Less than 5 of the 7 recorded days participation was considered ‘inadequate’ recreational exercise.
Main outcomes
Disease progression
Medial tibio-femoral JSN was evaluated from the three annual knee radiographs. Minimum medial tibio-femoral joint space width (mm) was measured using digitised image analysis software (Holy's software, UCLB, Lyon, France) for each participant at one time by an assessor (MF) blinded to treatment allocation, but not date sequence (baseline, year 1, year 2).19 It was decided, a priori, that for valid estimates of JSN, a TIRD of ≤1.7 mm at each time point was required for an x-ray to be included in JSN analyses. We also chose a rigorous cut-point of ≤0.2 mm difference in TIRD between two x-ray time points (baseline to year 2; baseline to year 1; year 1 to year 2) as the second inclusion criteria for a valid assessment of JSN.20
Knee pain
A mean of the maximum knee pain score (0–10) for each of the six bimonthly participant diaries collected during year 1 was the main symptomatic outcome.
Statistical issues
Two independent primary outcomes are considered in this study: the medial tibio-femoral JSN measured at 2 years, and a 0–10 point pain scale, a symptomatic outcome measured over 12 months. We made the following assumptions: JSN mean (SD) is 0.25 (0.45) mm in the placebo group, the use of either glucosamine or chondroitin alone lowers the mean JSN to 0.13 mm; baseline mean (SD) pain score is 5 (2.5) in the placebo group, the use of either dietary supplement results in a 20% reduction in pain. The sample size calculation is based on a 2-way analysis of variance (F-test) with two-sided α=0.05, power (1−β) >80% for any of the two main effects. Furthermore, we assumed an additive model without interaction. Under these conditions a sample size of 440 (4×110) is needed. After adjustment for loss to follow-up and non-adherence, a sample size of 608 (4×152) was considered necessary. This calculation is essentially driven by JSN (power achieved for the pain score is >90%).
We conducted F-tests, the Kruskal–Wallis test and Pearson's χ2 test across treatment groups on JSN, knee pain and the secondary outcomes (WOMAC pain, WOMAC physical function, SF12-PCS, SF12-MCS, 50-foot walk time) where appropriate. We examined JSN among treatment groups unadjusted and then adjusted for factors associated with disease progression9 such as gender, body mass index (BMI), baseline joint space width, Kellgren–Lawrence (KL) grade <221 and the presence of Heberden’s nodes using standard regression techniques. It has been recently demonstrated that a JSN ≥7% over 2 years was highly predictive of knee replacement surgery within the next 2–5 years.22 The number needed to treat (NNT) to avoid this outcome will be calculated. Following OARSI-OMERACT recommendations, the proportion of participants demonstrating >0.5 mm JSN over 2 years will also be reported as a further secondary analysis of structural disease progression.
For maximum knee pain (bimonthly participant diary), adjustment for baseline pain and repeated measurements over time was done using a linear mixed model with subject as random effect. All analysis were carried out at the 5% level of significance and analyses of both primary outcomes were on an intention-to-treat basis: valid available sets of x-rays were analysed regardless of treatment completion or adherence, with no imputation of missing data; conversely, the last-observation-carried-forward approach was adopted for symptomatic results. Statistical analysis was carried out using R V.2.14.2 (http://www.r-project.org/).
Results
From an initial 2288 telephone enquiries, 605 people proceeded to randomisation (October 2007–November 2009) (figure 1). A total of 502 (83%) participants completed both the year 1 and year 2 clinic assessments (figure 1) by November 2011. Of the 502 participants with complete clinic assessment follow-up, 23 (5%) had withdrawn from study treatment over the 2-year period: placebo (n=11), glucosamine (n=3), glucosamine–chondroitin (n=5), chondroitin (n=4). The completed participant diary returns ranged from 98% for participant diary 1 to 80% for participant diary 6 (end of year 1) and 77% for participant diary 12 (end of year 2), with no difference between the allocation groups.
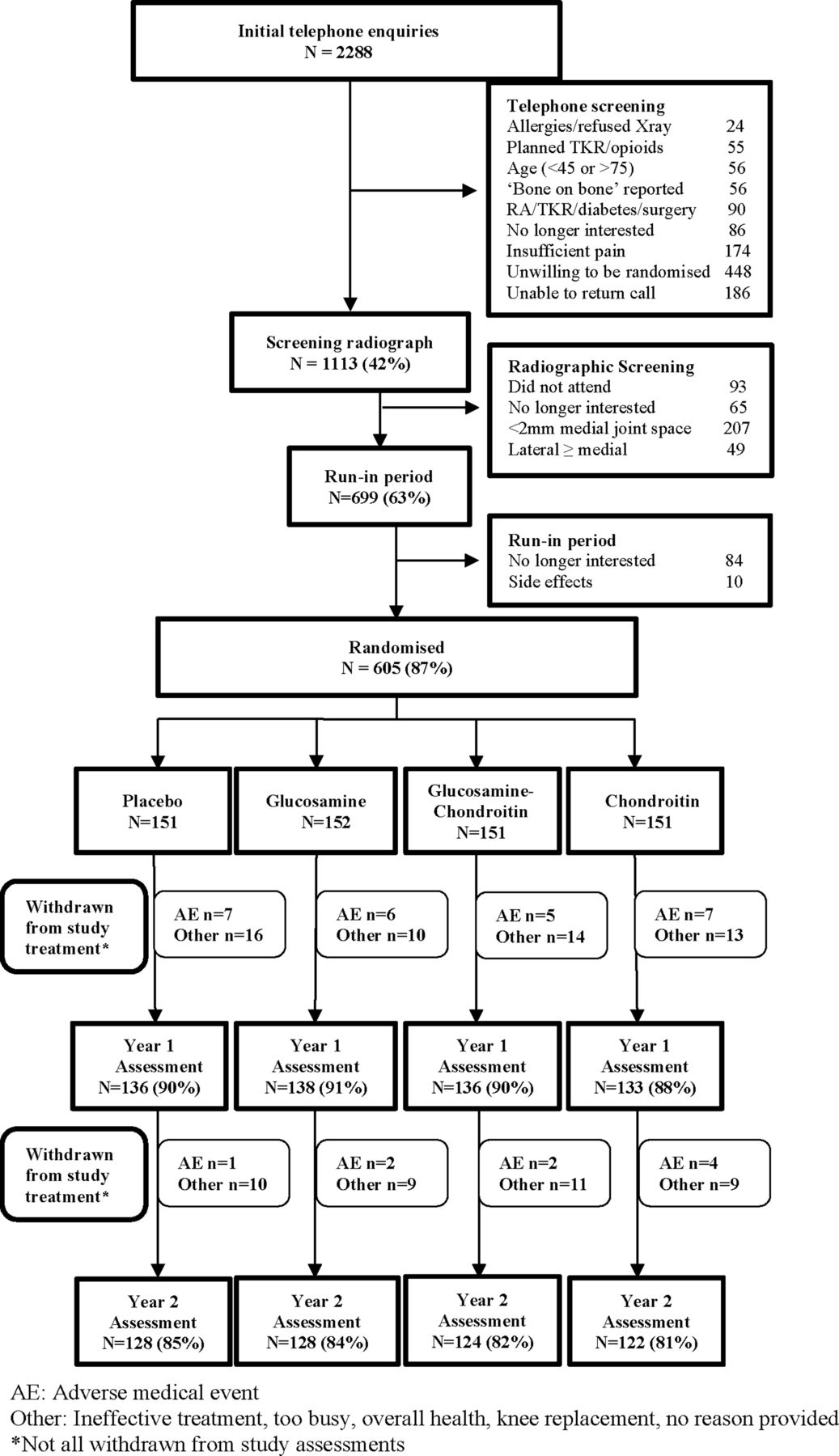
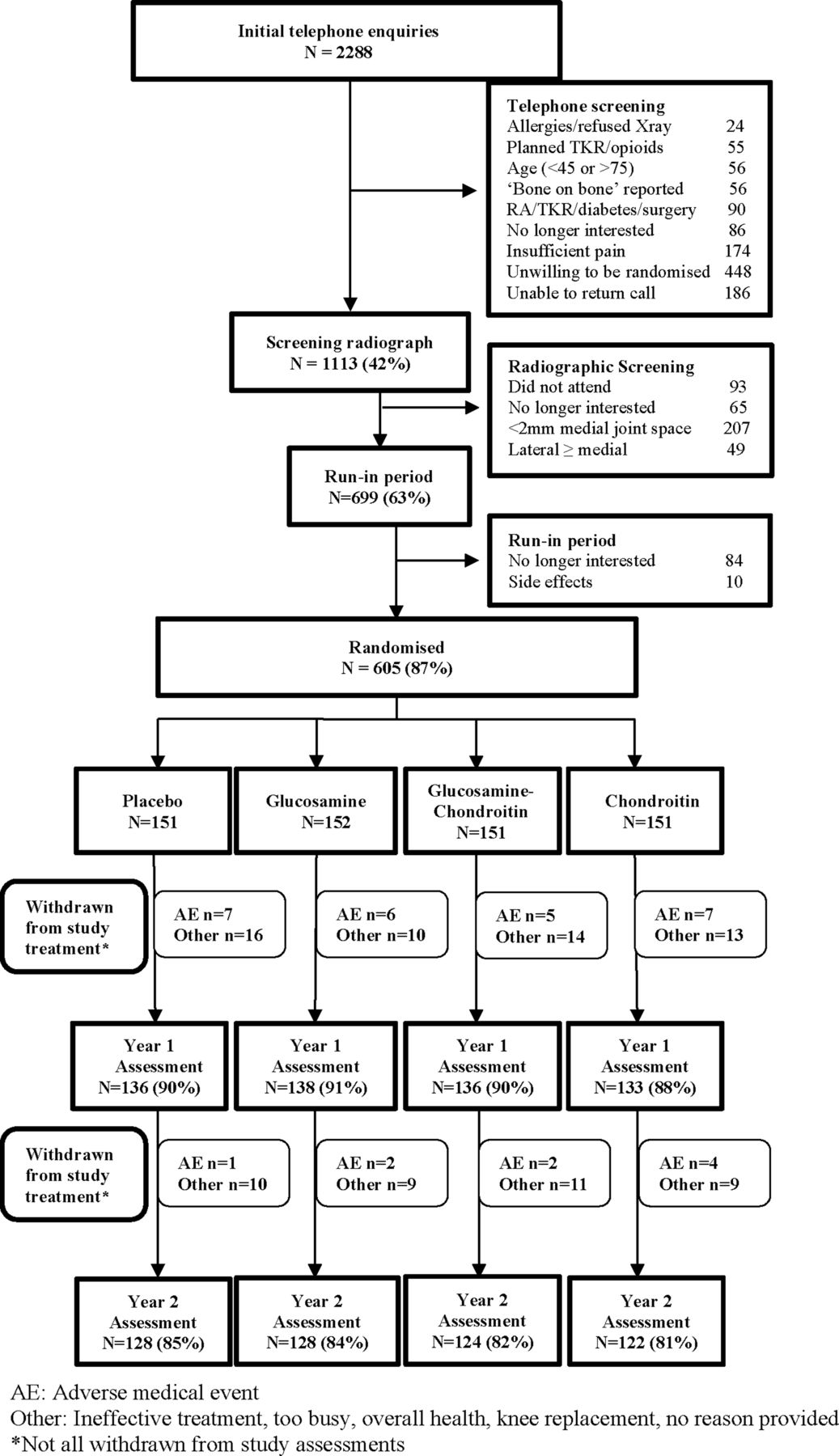{kind=link}
The Long-term Evaluation of Glucosamine Sulfate (LEGS) study. AE, adverse medical event. Other: ineffective treatment, too busy, overall health, knee replacement, no reason provided. *Not all withdrawn from study assessments.
At baseline, the mean age of participants was 60 years; just over 50% were female and 36% were obese (table 1). The majority of participants were aged 50 years and over (90%) and fulfilled, for the study knee, American College of Rheumatology clinical criteria for the diagnosis of knee OA. About half of the participants had only mild radiographic disease (KL grade <2) in their study knee.21 A total of 449 (74%) study participants reported at least 90% treatment adherence to four capsules daily over the 2-year study period. At the final clinical assessment, participants were asked if they considered they had been allocated to active (single or double) or placebo capsules. Of the 499 participants responding, 233 (47%) reported ‘don't know’ while 168 (34%) estimated ‘active’ and 95 (19%) placebo allocation. The demonstrated proportion of true active (66%) and true placebo (44%) estimates is approximately consistent with the 75% active treatment and 25% double placebo treatment allocations of our study.
Baseline demographics
Safety
During the 2-year follow-up, 126 (21%) participants withdrew from study treatment, only 34 (6%) for possibly-related medical events, with no major differences between the allocation groups (figure 1). A description of the adverse events leading to withdrawal from study treatment is detailed per allocation group (see online supplementary appendix S2).
Joint space narrowing
For the main structural outcome, 303 (50%) sets of knee x-rays were evaluated as valid for the measurement of 2-year JSN (table 2). There was no significant interaction demonstrated between the study treatments (p=0.24). There were no notable differences between participants with and without valid 2-year follow-up knee x-ray data in any of the baseline demographic variables reported in table 1. A further 193 (32%) participants had either a valid baseline and year 1, or a year 1 and year 2 x-ray set for the measurement of 1-year JSN. There was no difference in JSN (year 1 and year 2, n=496) between the four treatment allocation groups (F test p= 0.106). Accounting for gender, BMI, medial tibio-femoral joint space width at baseline, KL grade and presence of Heberden's nodes, allocation to the combination treatment (glucosamine and chondroitin) resulted in a statistically significant (p=0.046) decrease in 2-year JSN of 0.10 mm (95% CI 0.00 to 0.20 mm), compared with placebo (table 2). The 7% absolute risk reduction for ≥7% JSN found in this study (table 2) equates to an NNT of 14, or 14 people would need to take glucosamine–chondroitin for 2 years to avoid one knee replacement surgery within the following 2–5-year period. There were no significant effects on JSN for any of the single study treatment allocations (glucosamine or chondroitin) compared to placebo after accounting for gender, BMI, KL grade <2, baseline joint space width or presence of Heberden's nodes in linear regression model analysis.
Joint space width all x-rays, joint space narrowing (JSN) x-rays available for valid assessment of structural disease progression, mean (SD) JSW and JSN, 95% CI difference with placebo
Knee pain
For the main symptomatic outcome, no significant treatment interaction was demonstrated between the study treatments (p=0.57) and no significant effect on maximum knee pain over year 1 (diaries 1–6) was demonstrated for the three treatment allocations, compared with placebo (table 3). Over year 2, we observed a further reduction in maximum knee pain among all treatment allocations. However, there were no differences between the four allocations (F test p=0.494) and there was no significant difference in knee pain reduction between any of the treatment groups and placebo after adjusting for baseline values (table 3). Among the subgroup of 221 (37%) participants with severe knee pain (≥6/10) at baseline, there were no significant differences with respect to their maximum knee pain or global assessment and score across different treatment groups.
Maximum knee pain (0–10), participant diaries year 1 and year 2, mean (SD or 95% CI)
Secondary outcomes
There were no significant differences between the four allocation groups at year 1 or year 2 for any the secondary outcome measures (all p>0.05), except for inadequate exercise at baseline) (table 4). Mean BMI, 50-foot walk time and the use of analgesia (simple or NSAIDs/opioids) remained fairly consistent during the 2-year follow-up in all allocation groups. Knee pain and physical function (WOMAC) improved between baseline and year 1, with no further improvements from year 1 to year 2, in all allocation groups.
Mean (SD) secondary outcome measures and potential confounders
Discussion
The results of this study suggest that taking glucosamine sulfate (1500 mg) in combination with low molecular weight chondroitin sulfate (800 mg) daily for 2 years provided a meaningful reduction in JSN among people with symptomatic knee OA and evidence of mostly mild radiographic disease. The mean JSN among people allocated to the combination treatment was approximately half of that demonstrated in the placebo group after 2 years of treatment. If this reduction in JSN were to be sustained over a clinically meaningful period of OA development (eg, 10 to 15 years), then it would be very meaningful indeed. In the experimental conditions of this study, a significant reduction in JSN was not achieved for glucosamine or the chondroitin alone. With the same caveat, there were no significant reductions in knee pain detected for glucosamine or chondroitin alone, or in combination, over the 2-year follow-up period versus placebo.
For JSN, our finding for this combination did not support the overall findings of the GAIT study, the only other long-term randomised clinical trial evaluating an over-the-counter glucosamine–chondroitin combination on disease progression.9 However, 20–30% of GAIT participants had moderate–severe radiographic disease (KL grade 3), compared with only 5% in the current study. As concluded in the GAIT study structural progression results, participants with less severe radiographic disease severity appeared to be more responsive to these dietary supplements, in terms of slowing disease progression.9 Further, our rigorous criteria for selecting x-rays available for valid assessment of JSN markedly reduced measurement error. Recent studies have demonstrated that a small TIRD, and minimal differences in TIRD between two measurements of joint space width, is critical to avoid erroneous assessments of JSN.20 Another explanation for our positive findings for JSN may be that our once daily dosage regimen (compared with three divided doses per day) is likely to enhance full dosage treatment adherence and improve the pharmacokinetics of the active ingredients.23
Symptomatic benefits for the individual dietary supplements, or their combination, were not detected over the first year of follow-up in this study or in the 6-month GAIT study symptomatic results.8 Both studies demonstrated small ongoing reductions in knee pain, compared with baseline, for placebo and active treatment allocations over a 2-year follow-up period.24 Interestingly, the only randomised clinical trials to demonstrate significant, albeit small, symptomatic benefit of glucosamine for people with knee OA, had 3-year follow-up periods (and excluded patients who were obese).25 ,26 We had originally stated in the study registration that reduction in the use of NSAIDs would be the main symptomatic outcome measure. Our main symptomatic outcome measure was changed (and registered) to self-reported pain after recruitment of the first 200 participants demonstrated that only about 20% were using NSAIDs. Further, we felt that the specific focus of knee pain (‘at its worst’) for the daily 7-day numeric rating scale of the participant diary would be less vulnerable to a ‘floor effect’ among our study participants with mostly mild radiographic disease, and more likely to detect the ‘short episodes of more intense pain’ experienced by many people with knee OA.27 Interestingly, the mean WOMAC pain scores at baseline were low compared with the numeric rating scale scores, possibly precluding the detection of treatment benefit using this measure in a mildly symptomatic population.
This was an investigator-initiated, rigorously conducted randomised clinical trial.28 Two-year follow-up was excellent, with additional careful monitoring of concomitant analgesia use, BMI and physical activity, variables with potential to confound the association between study treatment and outcomes. The active treatment capsules were independently tested to ensure appropriate content of glucosamine and chondroitin. We recruited participants most likely to be responsive to these dietary supplement, that is, mostly early tibio-femoral radiographic disease.29 All participants had evidence of JSN in the medial tibio-femoral compartment and at least osteophytic lipping at baseline. However, for many participants the ‘definite osteophyte’ required for KL grade 2 may have been missed by only having a single posterior-anterior knee x-ray, resulting in a probable underestimate of the number of participants with KL grade 2 in this sample. The main limitations of this study were that follow-up was restricted to 2 years, and that we were unable to recruit participants with more severe pain at baseline. People presenting with more severe pain were mostly excluded due to radiographic ineligibility, that is, <2.0 mm of medial compartment joint space width. Further, although we were able to consider the vast majority of the x-rays throughout the study, only around 50% could be considered at the most important endpoint after 2 years.
While it is conceivable that glucosamine and chondroitin can improve cartilage composition and resilience, it is difficult to interpret a rationale for a short-term analgesic mode of action in nociceptive-free cartilage. However, reduced joint swelling among people with early radiographic disease, decreased subchondral bone resorption and reduced bone marrow lesions at 12 months have been demonstrated for chondroitin sulfate. These biological mechanisms would need a longer follow-up period to become clinically detectable.30–32 Glucosamine and chondroitin have several similar actions in articular cartilage, such as increasing proteoglycan synthesis and inhibiting cytokines and proteases.33 The demonstrated benefit in terms of disease modification may simply be due to achieving a biologically meaningful dosage with the combined treatment, a dosage that is not achieved using the glucosamine or chondroitin alone products utilised in this study.34 ,35 The fact that both the glucosamine and chondroitin contained sulfate may be a biological mechanism driving the superior results for the combination treatment allocation in this study, as sulfate depletion has been demonstrated to inhibit proteoglycan synthesis in human cartilage.36 ,37 The clinical significance of the study findings is highlighted by the demonstrated increased risk of knee joint replacement surgery with increased annual JSN or cartilage volume losses.22 ,38 ,39
Overall, the LEGS study could not detect significant symptomatic benefit for these dietary supplements over a 2-year follow-up period. Future research should allow for a lengthier study period. However, the LEGS study demonstrated that in this cohort of participants with mostly early radiographic disease, the combination of glucosamine sulfate and chondroitin sulfate did achieve a meaningful reduction in tibio-femoral JSN over 2 years, compared with placebo.
Acknowledgments
Emeritus Professor Charles Bridges-Webb (deceased), general practitioner, who was a highly influential chief investigator responsible for the design and implementation of the study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
Handling editor Tore K Kvien
Collaborators The following are members of the LEGS (Long-term Evaluation of Glucosamine Study) Collaborative Group: Maria Agaliotis, Lisa Bridgett, Chris Buckland-Wright (UK), Charles Bridges-Webb (deceased), Richard Day, John Edmonds, Stephen Jan, Stephane Heritier, Marlene Fransen, Graeme Jones, Lyn March, Lillias Nairn, Robyn Norton, Phillip Sambrook (deceased), Catherine Speechly, Steve Su, Eric Vignon (France), Milana Votrubec, Mark Woodward. The LEGS Collaborative Group also includes the study radiographers (Australia): Gorica Jovanovic, Shila Jeram, Mitchell Dowd, Mandy Champion, Sarah Grealy, Deanne Watson (Royal Prince Alfred Hospital, Camperdown), Anton Vrataric, Cecil Johnson, Rose White, Paul O'Connell (North West Radiology, Westmead), Fay Milwraith, Danielle Kennedy, Christine Faulkes, Olivia Bulton (St George Hospital, Kogarah) Kathleen Johnson (North Shore Radiology, St Leonards).
-
Contributors All authors have contributed to the conception and design of the study, acquisition of data or analysis and interpretation of the data. Further all authors have contributed to either the drafting of the article or revising it critically for important intellectual content. All authors have given final approval of the version published.
-
Funding This study was funded through the National Health and Medical Research Council of Australia (ID 402511), the Department of Health and Aging (Australia) (ID 402781) and by some supplementary funding (<15% total) from Sanofi-Aventis Consumer Healthcare Pty Ltd, Australia. The funders had no role in the design or conduct of the study; collection, management, analysis, or interpretation of the data; or preparation, review, or approval of the manuscript.
-
Competing interests None.
-
Ethics approval University of Sydney Human Research Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement Willing to consider reasonable requests to share de-identified data collected as part of this study.