Article Text

Abstract
Objective To determine the association between cam impingement, which is hip incongruity by a non-spherical femoral head and development of osteoarthritis.
Methods A nationwide prospective cohort study of 1002 early symptomatic osteoarthritis patients (CHECK), of which standardised anteroposterior pelvic radiographs were obtained at baseline and at 2 and 5 years follow-up. Asphericity of the femoral head was measured by the α angle. Clinically, decreased internal hip rotation (≤20°) is suggestive of cam impingement. The strength of association between those parameters at baseline and development of incident osteoarthritis (K&L grade 2) or end-stage osteoarthritis (K&L grades 3, 4, or total hip replacement) within 5 years was expressed in OR using generalised estimating equations.
Results At baseline, 76% of the included hips had no radiographic signs of osteoarthritis and 24% doubtful osteoarthritis. Within 5 years, 2.76% developed end-stage osteoarthritis. A moderate (α angle >60°) and severe (α angle >83°) cam-type deformity resulted in adjusted OR of 3.67 (95% CI 1.68 to 8.01) and 9.66 (95% CI 4.72 to 19.78), respectively, for end-stage osteoarthritis. The combination of severe cam-type deformity and decreased internal rotation at baseline resulted in an even more pronounced adjusted OR, and in a positive predictive value of 52.6% for end-stage osteoarthritis. For incident osteoarthritis, only a moderate cam-type deformity was predictive OR=2.42 (95% CI 1.15 to 5.06).
Conclusions Individuals with both severe cam-type deformity and reduced internal rotation are strongly predisposed to fast progression to end-stage osteoarthritis. As cam impingement might be a modifiable risk factor, early recognition of this condition is important.
Statistics from Altmetric.com
Introduction
Osteoarthritis is the most frequently occurring chronic joint disease and its main characteristics are pain and dysfunction.1 Symptomatic osteoarthritis affects 9.6% of men and 18% of women aged 60 years or older and, with an ageing population, the prevalence of osteoarthritis will increase substantially.2 Although osteoarthritis implies an increasing economic burden and detrimental impact on quality of life,3 no methods are available to prevent the disease or delay its progression. If modifiable risk factors can be identified at an early stage of the disease, preventive measures might be implemented.4
Many cases of idiopathic hip osteoarthritis may be secondary to minor variations in the morphology of the proximal femur.5 These minor variations in shape were described by Ganz et al,6 who introduced the concept of femoroacetabular impingement (FAI). FAI is a condition of abnormal contact between the femoral head–neck junction and the acetabulum, due to a bone shape abnormality on either the femoral or acetabular side. Two types of FAI can be distuingished,6 cam impingement and pincer impingement. Pincer impingement is caused by overcoverage of the acetabulum relative to the femoral head, and cam impingement is caused by extra bone formation (a cam-type deformity) in the anterolateral head–neck junction.7 ,8 Such a deformity can develop in response to sporting activities during adolescence.9 ,10 These cam-type deformities may cause impingement against the acetabular rim, especially during flexion and internal rotation of the hip (figure 1). Subsequently, a cascade of structural damage (including labral tears and cartilage delamination) may occur, which might gradually lead to osteoarthritis of the hip.11 Therefore, cam impingement has been proposed as a biomechanical risk factor for the development of hip osteoarthritis.12 ,13

Mechanism of cam impingement. A normal spherical-shaped femoral head (A) provides the hip with a physiological range of motion without impingement (B). A cam-type deformity as seen on an anteroposterior view (C) may cause impingement against the acetabular rim causing cartilage damage (arrowheads) (D). This figure is only reproduced in colour in the online version.
However, there are no cohorts combining radiographic and clinical parameters of cam impingement to study the risk of the development of osteoarthritis. Furthermore, due to the lack of prospective studies on this topic, no causal relationship between cam impingement and the development of osteoarthritis has been established.14 Interestingly, cam impingement is a potentially modifiable risk factor of osteoarthritis, as a cam-type deformity can be treated surgically and diagnosed before the onset of severe hip damage.
Assuming an association between cam impingement and the development of osteoarthritis, we examined the association between clinical and radiographic parameters suggestive of cam impingement at baseline and the risk of developing osteoarthritis within 5 years.
Methods
Study design and participants
All subjects were extracted from the Cohort Hip and Cohort Knee (CHECK) cohort. CHECK is a nationwide prospective cohort study of 1002 individuals with early symptomatic osteoarthritis of knee or hip. On entry, all participants had pain or stiffness of knee or hip and were aged 45–65 years; they had not yet consulted their general practitioner for these symptoms, or the first consultation was within 6 months before entry. Participants with a pathological condition that could explain the symptoms were excluded (for hip: trauma, rheumatoid arthritis, dysplasia, Perthes disease, subluxation, osteochondritis dissecans, fracture, septic arthritis, Kellgren and Lawrence (K&L) grade 4 or total hip replacement, previous hip surgery, and individuals having only symptoms of bursitis or tendinitis).15
Radiographs and clinical examination were obtained from 10 (general and university) hospitals. General practitioners were invited to refer eligible persons to one of those centres; advertisements in local newspapers were also used. Of the 1002 individuals, 865 individuals (1730 hips) were included in the present study because they had anteroposterior radiographs obtained at baseline (from October 2002 to December 2005) and at the 5-year follow-up (from November 2007 to December 2010); the mean (SD) follow-up was 5.06 (0.17) years. The study was approved by the medical ethics committees of all participating centres, and written informed consent was obtained from all participants.
Radiographs
Weight-bearing anteroposterior pelvic radiographs and faux profil oblique view radiographs were obtained according to a standardised protocol at baseline, and at 2 and 5 years follow-up.16 For anteroposterior radiographs, feet were positioned such that the medial side of the distal part of the first phalanx touched and a wedge was used to assure 15° internal rotation. The tube to film distance was 100 cm and the beam was centred at the top of the pubic symphysis.
Radiographic measurements
The shape of the proximal femur and acetabulum on the anteroposterior radiographs was outlined using statistical shape modelling (SSM) software (ASM tool kit, Manchester University, Manchester, UK). The shape on the anteroposterior radiographs is given by a set of landmark points that are positioned along the surface of the bone in the image. Each point is always placed on the same landmark of the outline, to allow comparison between the shapes. The α angle was automatically calculated from the points set of the SSM software (figure 2), using Matlab (V.7.1.0).
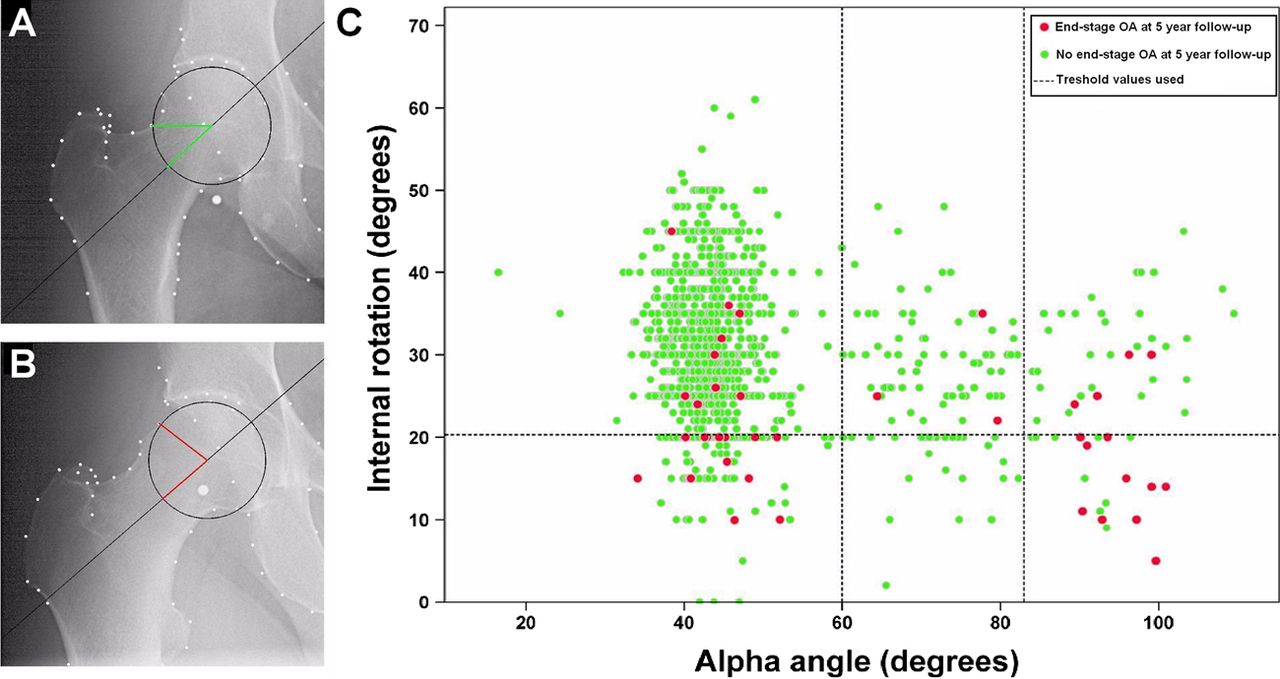
Cam impingement associates with end-stage osteoarthritis of the hip. (A) A spherical femoral head with an α angle of 43°; (B) a cam-type deformity resulting in an α angle of 78°; and (C) scatterplot of baseline measurements of the α angle and internal hip rotation in 90° of flexion (the red dots indicate hips that developed end-stage OA within 5 years). This figure is only reproduced in colour in the online version.
The α angle measures the extent to which the femoral head deviates from spherical and is a measure mostly applied to quantify a cam-type deformity. It is measured by first drawing the best fitting circle around the femoral head, then a line through the centre of the neck and the centre of the head. From the centre of the femoral head a second line is drawn to the point where the superior surface of the head–neck junction first departs from the circle. The angle between these two lines is the α angle.17 We defined the radiographic presence of a cam-type deformity by an α angle greater than 60° and and greater than 83°.18 ,19
At baseline, and at 2 and 5 years follow-up, all anteroposterior pelvic radiographs were scored for osteoarthritis according to the K&L classification (grade 0–4).20 In addition, superior and inferior joint space was determined on faux profil radiographs (grade 0–3).16 The development of incident osteoarthritis was defined by K&L grade 2 at 5-year follow-up, and the development of end-stage osteoarthritis was defined by K&L grades 3, 4, or a total hip replacement (THR) within 5 years.
Clinical measurements
All individuals were clinically examined by measuring the range of motion (ROM) of the hip. The ROM was measured in flexion, internal rotation, external rotation, abduction and adduction. The presence of reduced internal rotation (in 90° of flexion) is suggestive of impingement. We used a threshold value of 20° or less.21 Furthermore, the presence and severity of hip pain were assessed using validated self-report questionnaires, including the Western Ontario and McMaster University osteoarthritis index (WOMAC, pain subscale) and the visual analogue scale.22 ,23
Reliability of the α angle
The points of the SSM software were positioned in all radiographs by three investigators who were unaware of any follow-up data. To examine interobserver reliability, the point set was positioned twice by each investigator in 25 randomly selected radiographs with an interval of 2 months. Intra-observer reliability was tested for each investigator in 10 randomly selected radiographs.
Statistical analysis
Reliability of the α angle was assessed using intraclass correlation coefficient (ICC) (two-way random, absolute agreement). Univariable differences in baseline characteristics between included and excluded hips, and between hips that developed osteoarthritis and normal hips, were evaluated by the Mann–Whitney test for continuous variables, by the χ2 test for sex and by generalised estimating equations (GEE) for K&L score. The strength of the independent relationship between cam impingement parameters at baseline and the development of osteoarthritis was calculated using GEE and expressed in terms of OR. Using GEE allowed to model the correlation between the left and the right hip. To adjust for confounders, in the GEE model, K&L classification and sex were entered as a factor, and body mass index and age as a covariate. Hips with end-stage osteoarthritis at 5-year follow-up were excluded from analysis when incident osteoarthritis was used as an outcome measure. The positive predictive value of cam impingement parameters for osteoarthritis was also calculated. Differences in pain scores and ROM between individuals with and without radiographic cam-type deformity were calculated using the Mann–Whitney test and GEE, respectively, the latter adjusted for K&L grade at baseline. All statistical analyses were performed in SPSS V.15.0.
Results
Participants
Of the 1002 individuals in the CHECK cohort, 89 were lost to follow-up, 16 were not able to visit the hospital during the 5-year follow-up, and 32 refused to undergo radiographs or had missing radiographs. For this study, 865 individuals (682 women, 183 men; aged 45–65 years) were included. At baseline, these 865 individuals (1730 hips) were included in the CHECK cohort because of the first onset of pain in their hip (n=148), knee (n=354), or both (n=363). Anteroposterior hip radiographs (instead of anteroposterior pelvic radiographs) were obtained in the first 124 individuals of the CHECK cohort. These individuals were excluded from baseline measurements because an anteroposterior hip view is known to influence the α angle.24 Radiographs of insufficient quality were also excluded (figure 3). To calculate the OR, all hips with an anteroposterior pelvic radiograph of sufficient quality were included (n=1411 hips). Excluded individuals did not differ on any baseline characteristic from the included individuals. Table 1 presents baseline demographic data of the participants stratified for the absence or presence of osteoarthritis at follow-up.
Baseline characteristics of the participants, stratified by the absence or presence of end-stage osteoarthritis and incident osteoarthritis

{kind=link}
{kind=link}
{kind=link}
Flow of subjects from the start of the cohort to the final study population.
Osteoarthritis classification
Of the 1411 included hips, 4.25% (n=60) developed incident osteoarthritis and 2.76% (n=39) end-stage osteoarthritis within 5 years follow-up. THR patients did not have other hip pathology than osteoarthritis nor other hip surgery during follow-up.
At baseline, the K&L grade could be scored reliably in 1389 hips. Of these hips, 76% had no signs of radiographic hip osteoarthritis (K&L grade 0) and 24% had doubtful radiographic hip osteoarthritis (K&L grade 1). On the faux profil view, superior joint space narrowing was scored as grade 0 in 94%, grade 1 in 5% and grade 2 in 1% (n=1379), and inferior joint space narrowing as grade 0 in 95% and grade 1 in 5% (n=1378). Of those hips having K&L grade 0 on the anteroposterior view, 2% had a superior and 5% an inferior joint space narrowing grade 1 on the faux profil view.
Association between cam-type deformity and osteoarthritis
When adjusted for confounders, only hips with a moderate cam-type deformity (α angle >60°) were significantly associated with the development of incident osteoarthritis OR=2.42 (95% CI 1.15 to 5.06, p=0.020, see supplementary table S1, available online only). The positive predictive value was 12.2%.
A cam-type deformity at baseline was strongly associated with end-stage osteoarthritis (table 2 and figure 2). In particular, the OR for a severe cam-type deformity (α angle >83°) was high (9.66, 95% CI 4.72 to 19.78, p<0.00001). Furthermore, the positive predictive value for end-stage osteoarthritis when having a cam-type deformity as determined by an α angle greater than 83° and greater than 60° was 25.0% and 10.9%, respectively.
Association (n=1411 hips) between cam impingement parameters and end-stage osteoarthritis (n=39) at 5-year follow-up
Reduced internal rotation of 20° or less at baseline was significantly associated with the development of end-stage osteoarthritis, expressed by an adjusted OR of 7.13 (95% CI 3.38 to 15.04, p<0.00001). The positive predictive value for end-stage osteoarthritis was 10.3%. Data on ROM and pain scores in hips with cam-type deformity compared with normal hips are presented in supplementary table S2 (available online only).
There was a strong association between the combination of clinical and radiographic parameters suggestive of cam impingement and end-stage osteoarthritis. Individuals with both an α angle greater than 83° and internal rotation of 20° or less at baseline were at high risk of end-stage osteoarthritis within 5 years (table 2 and figure 2). The strength of this association by means of an adjusted OR was 25.21 (95% CI 7.89 to 80.58, p < 0.00001) and the positive predictive value was 52.6%.
Reliability and reproducibility of the α angle
The ICC score for interobserver reliability was 0.73 for the α angle. ICC scores for intra-observer reliability ranged from 0.85 to 0.99.
Discussion
This first prospective study on cam impingement shows a strong association between cam impingement in radiographically non-arthritic individuals presenting with the first onset of pain complaints at baseline, and the development of osteoarthritis within 5 years. The results indicate that hip incongruity by a cam-type deformity is highly predictive of especially fast progression to end-stage osteoarthritis.
The data suggest that the risk of end-stage osteoarthritis is higher when the cam-type deformity is more pronounced. This is in line with a study reporting a correlation between the magnitude of the α angle and the severity of acetabular cartilage damage as measured with delayed gadolinium-enhanced contrast MRI of cartilage.25 Another group examining the relationship between morphological parameters and the risk of receiving THR within 19 years, concluded that the α angle was significantly associated with THR in women, independent of the presence of radiographic hip osteoarthritis at baseline; they reported an adjusted OR for receiving a THR of 1.052 for every degree increase in the α angle.26
Cross-sectional studies have shown a positive association between cam morphology and osteoarthritis. One study showed an estimated OR of 2.2 for having a non-spherical femoral head and osteoarthritis as defined by a minimum joint space width of 2 mm or less.27 Another group found an estimated OR (adjusted for confounders) of 6.95 (95% CI 4.64 to 10.41) for the association of a visually scored non-spherical femoral head with osteoarthritis in a case–control study.12 This latter value lies within the range of our findings for a radiographic cam-type deformity.
In those studies it was noticed that a non-spherical head could also partly be a consequence of rather than a cause of osteoarthritis. However, in the present study, as all hips had only doubtful or no signs of radiographic osteoarthritis at baseline, we could exclude a cam-type deformity from being a consequence of osteoarthritis. In addition, we found no increase in cam-type deformity over time, as the α angle at 5 years follow-up did not differ from that at baseline in either normal hips or hips that developed osteoarthritis. This indicates that cam-type deformity is probably not a consequence of a dynamic remodelling process in this adult cohort, but is a more or less static phenomenon. There is some evidence that this deformity develops during puberty by (over)active participation in certain sports.9 ,10
As only four hips had a K&L score of 3 or greater, most of the hips were judged to be end-stage osteoarthritis based on having received a THR. Although THR is a validated and clinically relevant osteoarthritis outcome measure,28 some concern might rise as to whether end-stage osteoarthritis was truly the reason for surgery and not pain caused by the cam-type deformity itself. At baseline, subjects with a cam-type deformity did not have more pain (see supplementary table S2, available online only). Nor did we find any difference in pain scores between the subjects with a cam-type deformity and a normal hip within the group that underwent THR. Furthermore, of all the hips that underwent THR within 5 years, the hips with a cam-type deformity demonstrated a more severe osteoarthritis score than normal hips already after 2 years of follow-up. Together, this suggests that the reason for a THR in individuals with a cam-type deformity was most likely the fast progression of osteoarthritis, and not pain due to impingement. This is further supported by the fact that two of the four hips with a K&L score of 3 or greater also had a cam-type deformity at baseline.
Because there is no consensus on how to quantify a cam-type deformity, we used two threshold values. Osseous abnormalities below the threshold value of 60° are suggested to pose less of a risk for developing hip pain.18 A value of 83° was defined as a pathological threshold value based on anteroposterior radiographs in a large cross-sectional cohort of 2803 asymptomatic individuals.19 Interestingly, in our cohort, when studying the distribution of the α angle at baseline, hips with a cam-type deformity (α angle >60°) appear to be a clearly different cluster from hips with a normal α angle (figure 2).
The main limitation of the present study is the use of anteroposterior radiographs only. Because cam-type deformities are located in the anterolateral head–neck junction and might be missed on an anteroposterior radiograph, the prevalence of cam-type deformities might have been underestimated.7 ,29 Of the hips that developed end-stage osteoarthritis, at baseline 12 hips had clinical signs suggestive of impingement but no radiographic cam-type deformity; three of these hips were non-clinical forms of hip dysplasia as seen by a dysplastic appearance on the anteroposterior radiograph (centre–edge angle <25°). The remaining nine hips might have had a cam-type deformity not visible on the anteroposterior view. Cohorts using MRI might elucidate this uncertainty.30 Nevertheless, anteroposterior radiographs are extensively used in clinical practice; on these radiographs, a simple measure to predict the risk of end-stage osteoarthritis in individuals with hip complaints would be of considerable value. Moreover, anteroposterior radiographs are a simple and inexpensive tool for use in large cohorts and are the only validated imaging modality for the assessment of osteoarthritis progression in the hip.31
It is important to note that having a radiographic cam-type deformity will not always cause impingement. To distinguish between those who have cam impingement and those who do not, the presence of decreased internal rotation is a useful clinical tool. The combination of clinical and radiographic measures, which can be simply obtained in an outpatient setting, results in an extremely positive prediction for end-stage osteoarthritis. Although the lower CI limit is still 7.89, one should be aware of the wide CI. Furthermore, decreased internal rotation might also be a sign of clinical osteoarthritis, because it is part of the American College of Rheumatology criteria for clinical osteoarthritis.32 However, decreased internal rotation due to clinical osteoarthritis would be more likely in a more advanced stage of the disease than in our cohort at baseline. In addition, it has been shown that internal rotation of the hip is largely determined by the osseous structures of the hip, which makes impingement a plausible explanation for decreased internal rotation.21
Individuals with symptomatic cam impingement are eligible for treatment of the deformity in an open or arthroscopic surgical procedure in which the femoral head is shaved to its normal congruity.33 Such a treatment is currently performed with increasing frequency in an attempt to relieve complaints and to halt the destructive cascade. The short-term and mid-term results of this treatment show a relief in pain and an increase in hip function; however, no randomised (placebo) controlled trial is available and the long-term results on the prevention of osteoarthritis are unknown.34 The findings of the present study justify further study on the treatment of cam impingement, and indicate that follow-up periods of a few years seem sufficient to show a potential effect of treatment.
In conclusion, cam impingement is strongly related to the development of hip osteoarthritis. Our results indicate that individuals who present with the first onset of pain complaints, and have both a radiographic cam-type deformity and reduced internal hip rotation, are at high risk of fast progression to end-stage osteoarthritis. A cam-type deformity might be a modifiable risk factor that can be diagnosed before severe hip damage is present, providing an opportunity to prevent hip osteoarthritis.
Acknowledgments
The authors would like to thank C Vermeulen and J van Egmond for their involvement in positioning the landmark points on the radiographs for the SSM, as well as all the participants of the CHECK cohort. CHECK cohort study is initiated by the Dutch Arthritis Association and performed within Erasmus Medical Center Rotterdam, Kennemer Gasthuis Haarlem, Leiden University Medical Center, Maastricht University Medical Center, Martini Hospital Groningen/Allied Health Care Center for Rheumatism and Rehabilitation Groningen, Medical Spectrum Twente Enschede/Ziekenhuisgroep Twente Almelo, Reade, formerly Jan van Breemen Institute/VU Medical Center Amsterdam, St Maartens-kliniek Nijmegen, University Medical Center Utrecht and Wilhelmina Hospital Assen.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement - Online tables
Footnotes
-
Contributors SMAB-Z and HW supervised the study design; RA, SMAB-Z and JHW performed data collection; RA and JHW conducted data analysis; RA, MPH, SMAB-Z, JANV, HW and JHW contributed to data interpretation and preparation of the manuscript.
-
Funding The CHECK study was funded by the Dutch Arthritis Association.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval The study was approved by the medical ethics committees of all participating centres.
-
Provenance and peer review Not commissioned; externally peer reviewed.