Article Text

Abstract
Objective An imbalance of neuroactive kynurenine pathway metabolites has been proposed as one mechanism behind the neuropsychiatric sequelae of certain neurological disorders. We hypothesized that concussed football players would have elevated plasma levels of neurotoxic kynurenine metabolites and reduced levels of neuroprotective metabolites relative to healthy football players and that altered kynurenine levels would correlate with post-concussion mood symptoms.
Methods Mood scales and plasma concentrations of kynurenine metabolites were assessed in concussed (N=18; 1.61 days post-injury) and healthy football players (N=18). A subset of football players returned at 1-week (N=14; 9.29 days) and 1-month post-concussion (N=14, 30.93 days).
Results Concussed athletes had significantly elevated levels of quinolinic acid (QUIN) and significantly lower ratios of kynurenic acid (KYNA) to QUIN at all time points compared with healthy athletes (p's<0.05), with no longitudinal evidence of normalization of KYNA or KYNA/QUIN. At 1-day post-injury, concussed athletes with lower levels of the putatively neuroprotective KYNA/QUIN ratio reported significantly worse depressive symptoms (p=0.04), and a trend toward worse anxiety symptoms (p=0.06), while at 1-month higher QUIN levels were associated with worse mood symptoms (p's<0.01). Finally, concussed athletes with worse concussion outcome, defined as number of days until return-to-play, had higher QUIN and lower KYNA/QUIN at 1-month post-injury (p's<0.05).
Conclusions These results converge with existing kynurenine literature on psychiatric patients and provide the first evidence of altered peripheral levels of kynurenine metabolites following sports-related concussion.
Statistics from Altmetric.com
Introduction
There is a growing body of literature that suggests that a history of sports-related mild traumatic brain injury (mTBI) may lead to long-term behavioural and neuroanatomical abnormalities in young and older adults,1–3 despite the fact that the majority of acute incidents of concussion typically recover within 7–10 days.4 Thus, there is an urgent need to identify the acute neuropathophysiological sequelae of concussion that may predispose some individuals to the development of these negative long-term consequences. In this work, we assess acute and subacute postconcussion alterations in the kynurenine (KYN) metabolic pathway that has been associated with a variety of psychiatric and neurodegenerative disorders, including severe TBI.5 ,6
Concussion, or mTBI, results in a cascade of pathophysiological changes, including metabolic deregulation and a rapid and sustained elevation of proinflammatory cytokines.7 ,8 One potential consequence of this cascade is increased production of neuroactive KYN pathway metabolites via induction of indoleamine 2, 3-dioxygenase (IDO).9 IDO is activated by proinflammatory cytokines, shifting the catabolism of tryptophan to increase KYN production (see online supplementary figure S1). Proinflammatory cytokines also enhance the activity of the enzyme kynurenine-3-monooxygenase (KMO), which shifts the catabolism of KYN away from kynurenic acid (KYNA) toward 3-hydroxykynurenine (3HK). 3HK, a potent free radical generator, is subsequently metabolised into quinolinic acid (QUIN), a potentially excitotoxic N-methyl-d-aspartate (NMDA) receptor agonist.9 In contrast, KYNA is believed to promote neuroprotection at normal physiological concentrations due in part to its competitive antagonism of ionotropic excitatory amino acid receptors.
Abnormalities in KYN pathway metabolites have been associated with a variety of psychiatric and neurodegenerative diseases.5 For example, we have reported reduced peripheral levels of the ratio of KYNA/QUIN, a putatively neuroprotective index, in subjects with major depressive disorder (MDD)10 and bipolar disorder,11 with KYNA/QUIN levels inversely correlating with anhedonic symptoms in MDD.12 Furthermore, a reduction in KYNA and an elevation in QUIN have been observed in the cerebrospinal fluid (CSF) of suicide attempters13 and increased QUIN has been observed in the brain postmortem following suicide.14 Finally, an elevation of QUIN has also been observed in the CSF acutely (ie, days) following severe TBI.15 ,16 The extent to which KYN pathway abnormalities are present following less severe head injuries, such as concussion, is currently unknown.
To address this knowledge gap, we longitudinally assessed plasma levels of KYN pathway metabolites in a sample of collegiate football players at approximately 1-day, 1-week and 1-month postconcussion. We hypothesised that concussed players would have higher levels of 3HK and/or QUIN, and lower levels of KYNA in the acute phase (ie, days) relative to healthy athletes, with recovery toward normal levels at the subacute phase. Moreover, given the previously observed relationships between KYN abnormalities and mood symptoms, and the fact that mood symptoms are commonly observed following concussion,17 we hypothesised that KYN abnormalities would correlate with mood symptoms in concussed athletes.
Methods
Participants
A total of 36 male student-athletes from a single NCAA Division I American rules football programme with no reported past or current mood disorders, anxiety disorders, alcohol abuse or substance abuse were referred by sports medicine professionals and participated in the current study. Eighteen football players participated within 3-days (T1, mean=1.61 days, SD=0.61) following a concussion that was diagnosed by physicians trained in sports medicine at the time of injury. Fourteen of these concussed football players participated in a follow-up visit approximately 1-week postconcussion (T2, mean=9.29 days, SD=2.23), and fourteen participated in a follow-up visit approximately 1-month postconcussion (T3, mean=30.93 days, SD=4.58). Eleven athletes participated in all three visits and 6 athletes participated in the initial visit and one follow-up visit. Concussion diagnosis was determined independently of the study based on clinical judgment following recommended guidelines18 using a clinical examination assessing symptoms, a cranial nerve check, manual muscle testing for strength deficits, the Rhomberg's test for balance deficits, on-field cognitive testing developed by the UPMC Center for Sports Medicine, and the King-Devick test. An additional eighteen healthy collegiate football players from the same athletic team participated in the study and served as healthy controls. Healthy athletes with a concussion history were at least 7 months removed from the most recent concussion, which was on average 27 months prior to the study date. All participants provided written informed consent approved by institutional review boards. Behavioural data from an overlapping cohort was previously included in an investigation of cerebral blood flow.19
Behavioural assessments
A health history interview was used to assess self-reported concussion history, defined as previous concussions that were diagnosed at the time of injury, and the number of years of tackle football experience across all levels of competition. Postconcussion mood symptoms were assessed using structured interviews for the Hamilton Anxiety Rating Scale (HAM-A) and the Hamilton Depression Rating Scale (HAM-D), the primary measures of interest. The cognitive battery and self-reported symptom inventories obtained as part of the Automated Neuropsychological Assessments Metrics Version 4 Sports Medicine Battery (ANAM) were used as secondary measures of interest (see online supplementary material).20 Finally, the number of days that athletes were withheld from competition was independently determined by physicians trained in sports medicine following recommended guidelines18 and was used to operationalise concussion outcomes.
Blood biomarkers
A non-fasting venous afternoon blood sample was drawn from each subject in K2 EDTA BD Vacutainer tubes (Becton, Dicknson and Company, Franklin Lakes, New Jersey, USA). Blood was centrifuged at 1300 g for 10 min at room temperature and plasma was collected. Plasma was then either aliquoted into microfuge tubes and stored at −80°C that day, or stored at 4°C overnight, and then aliquoted into microfuge tubes and stored at −80°C the next morning. Plasma samples from participants at multiple time points were processed identically, the proportion of samples frozen immediately did not differ between groups and processing had no effect on KYN metabolites (see Results). Frozen plasma samples were shipped overnight on dry ice to Brains Online, LLC for analysis of KYN metabolites. Concentrations of KYN, QUIN, 3HK and KYNA in plasma were determined using high-performance liquid chromatography with tandem mass spectrometry detection according to their standard protocol.
Statistics
All statistical analyses were performed using SYSTAT. The number of previously reported concussions was square root transformed following addition of a constant to better the approach to a normal distribution. Two-tailed independent sample t tests were performed to determine if age, education, body mass index (BMI), the number of years of tackle football experience or the number of previously diagnosed concussions differed between groups. Cross-sectional behavioural measures were assessed using two-tailed independent sample t tests. In order to control for false positives and limit the number of tests, a multivariate analysis of variance was performed to determine if the concentration of KYN metabolites differed between groups. Investigated metabolites included KYN, KYNA, QUIN, 3HK and based on our previous findings, the ratios of KYNA/QUIN and KYNA/3HK.10 Finally, a χ2 analysis was performed to determine if the proportion of plasma samples frozen immediately differed between healthy athletes and concussed athletes at T1, and a multivariate analysis of variance was performed to determine if the concentration of KYN metabolites differed due to time of plasma freezing. A significance level of p<0.05 was considered for all analyses.
Repeated measures analyses were performed using linear mixed-effects (LME) modelling with a random intercept and compound symmetry to account for missing data. LME models with time as fixed effect were conducted for each behavioural measure. A LME model with time, kynurenine metabolite and the interaction of time×kynurenine metabolite was conducted. In this model, a significant interaction indicates differences in recovery slopes between kynurenine metabolites. Follow-up LME models with time as a fixed effect and random intercept were conducted following significant interactions at p<0.05. Pairwise comparisons of time points were performed following significant LME models at p<0.05. Finally, a priori Spearman correlations were conducted to determine whether KYN metabolites identified in the multivariate analysis of variance (MANOVA) as differing between groups were associated with postconcussion mood symptoms at each time point.
Results
Demographics
Demographic information is listed in table 1. There were no differences between concussed and healthy football players in age (t(34)=−0.26, p=0.80), education (t(34)=−1.11, p=0.28), BMI (t(34)=−0.71, p=0.48) or tackle football experience (t(34)=1.42, p=0.16). However, concussed football players self-reported a greater number of prior concussions than healthy football players (t(34)=2.77, p=0.009). The median number of days that the concussed athletes were withheld from competition was 12.5 days (range: 4 to indefinite).
Demographic information for healthy and concussed athletes
Behavioural measures
Repeated measures analyses demonstrated that scores on the HAM-A and HAM-D significantly changed over time postconcussion (F(2,26)=24.34, p<0.001, and F(2,26)=25.32, p<0.001, respectively; figure 1). Pairwise comparisons showed that HAM-A and HAM-D scores were significantly higher at T1 relative to both T2 (p's<0.01) and T3 (p's<0.001). T3 scores were significantly improved relative to T2 scores for both the HAM-A and HAM-D (p's<0.01). There was also a significant effect of time postconcussion on self-reported symptom frequency and the cognitive composite score (p's<0.001), with worse scores at T1 relative to T2 and T3 (p's<0.005) but no differences between T2 and T3 (see online supplementary figure S2).

Primary behavioural measures: depression (HAM-D) and anxiety (HAM-A) symptoms significantly improved from 1-day (T1) to 1-week (T2) and 1- month (T3) postconcussion. HAM-D and HAM-A scores were higher in concussed athletes at T2, and HAM-D scores were higher at T3 relative to healthy athletes (HA). Notches indicate 95% CI of the median, and whiskers represent data within 1.5 IQR. HAM-A, Hamilton Anxiety Rating Scale; HAM-D, Hamilton Depression Rating Scale.
Two-tailed independent sample t tests demonstrated that concussed football players at T1 had significantly higher HAM-A (t(34)=6.73, p<0.001) and HAM-D scores (t(34)=6.15, p<0.001) than healthy football players. Additional analyses confirmed that HAM-A (t(30)=5.10, p<0.001) and HAM-D scores (t(30)=5.83, p<0.001) were also significantly higher at T2 relative to healthy athletes. HAM-D scores were still significantly higher at T3 relative to healthy athletes (t(30)=2.13, p=0.041), while HAM-A scores at T3 did not differ from healthy athletes (t(30)=1.57, p=0.13). Self-reported symptoms and cognitive performance were also worse in concussed athletes at T1 (p's<0.005), but not at T2 or T3 when compared to healthy athletes (see online supplementary material).
Kynurenine pathway measures
The proportion of plasma samples that were frozen immediately or kept overnight at 4°C, and frozen the next morning did not differ between groups (χ2(1)=0.11, p=0.74), and time of freezing had no multivariate effect on KYN measures (λ=0.93, F(6,29)=0.38, p=0.88).
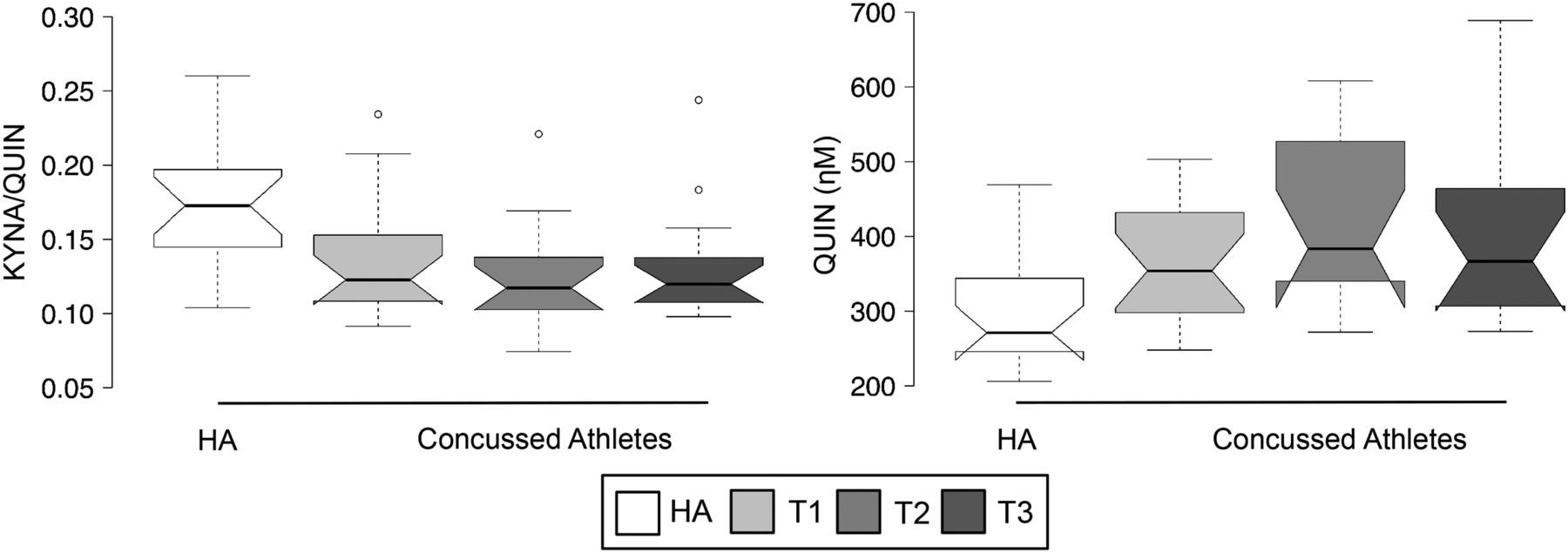
Repeated measures analyses found no significant main effect of time (F(2,241)=1.10, p=0.34) or interaction between time and kynurenine metabolite (F(10,241)=1.11, p=0.36), indicating kynurenine metabolite concentration did not change over time postconcussion. However, there was a significant multivariate effect of group (T1 vs healthy athletes) on KYN metabolites (λ=0.63, F(6,29)=2.84, p=0.027). Follow-up univariate analyses demonstrated that concussed players had significantly higher plasma concentrations of QUIN (F(1,34)=5.91, p=0.021) and a significantly lower ratio of KYNA/QUIN (F(1,34)=6.48, p=0.016) relative to healthy athletes (figure 2). No other KYN metabolites differed between groups (p>0.10; see online supplementary figure S3). Two-tailed independent samples t tests confirmed that QUIN levels remained significantly elevated at T2 (t(30)=3.62, p=0.001) and T3 (t(30)=2.97, p=0.006) relative to healthy athletes. Similarly, KYNA/QUIN ratio was still significantly lower in concussed athletes at T2 (t(30)=−3.30, p=0.003) and T3 (t(30)=−2.67, p=0.012) relative to healthy athletes.

Alterations in kynurenine pathway metabolites: concussed athletes had significantly elevated quinolinic acid (QUIN) and lower kynurenic acid (KYNA)/QUIN at approximately 1-day (T1), 1-week (T2), and 1- month (T3) postconcussion relative to healthy athletes (HA). Notches indicate 95% CI of the median, and whiskers represent data within 1.5 IQR.
Correlation analyses
A priori correlation analyses were conducted to test the hypothesis that altered KYN metabolites identified in the MANOVA analysis (QUIN and KYNA/QUIN) would be associated with mood measures in concussed players. There was no significant relationship between QUIN and HAM-A or HAM-D scores (p's>0.10) at T1. However, there was a significant inverse correlation between KYNA/QUIN and HAM-D scores at T1 (r(s)=−0.48, p=0.04), and the relationship between KYNA/QUIN and HAM-A scores at T1 was trending towards significance (figure 3; r(s)=−0.46, p=0.06). There was no significant relationship between mood scores and KYNA/QUIN or QUIN at T2 (p's>0.10), or between mood scales and KYNA/QUIN at T3. However, QUIN was significantly correlated with both HAM-A (r(s)=0.70, p=0.005) and HAM-D scores at T3 (r(s)=0.80, p<0.001).

{kind=link}
{kind=link}
{kind=link}
Relationship between mood symptoms and kynurenic acid (KYNA)/quinolinic acid (QUIN): Concussed athletes with lower KYNA/QUIN ratios had significantly greater depression symptoms (HAM-D) and a trend towards greater anxiety symptoms (HAM-A) at T1 (top panel). Concussed athletes with elevated QUIN had significantly more depression and anxiety symptoms at T3 (lower panel). HAM-A, Hamilton Anxiety Rating Scale; HAM-D, Hamilton Depression Rating Scale.
Exploratory correlations were conducted to determine if QUIN and KYNA/QUIN were associated with concussion outcome due to the observed correlations with mood measures. No significant associations were observed at T1 or T2 (p's>0.10). However, the number of days that concussed athletes were withheld from competition was significantly associated with T3 levels of QUIN (r(s)=0.60, p=0.02) and KYNA/QUIN ratios (r(s)=−0.62, p=0.02).
Discussion
The major finding of this study is that concussed athletes had significantly elevated plasma levels of the potentially neurotoxic QUIN and decreased levels of KYNA/QUIN at the acute (ie, days) and subacute phase (ie, week to 1-month) of injury compared to uninjured student-athletes who did not differ in sport, tackle football experience, sex, age and education. Importantly, lower KYNA/QUIN ratios and higher levels of QUIN were associated with more severe anxiety and depression symptoms in concussed athletes at multiple time points postconcussion. In addition, concussed athletes with worse outcome had higher levels of QUIN and lower levels of KYNA/QUIN at 1-month postconcussion.
Consistent with previous work, concussed athletes had more severe mood symptoms, more self-reported symptoms and worse acute cognitive performance following concussion than healthy athletes.4 ,17 In addition, we observed both cross-sectional and longitudinal evidence of recovery from self-reported symptoms and cognitive deficits by 1-week postconcussion, which converges with previous large-scale studies that document typical recovery from these symptoms by 7–10 days postconcussion.4 However, mood symptoms, which are common following TBI regardless of severity,17 ,21 remained elevated at 1-week, while depressive symptoms remained elevated at 1-month postconcussion in this sample. These data suggest that mood symptoms may recover more slowly than the other postconcussion symptoms. Alternatively, differences in symptom-metrics (self-report vs interview) could explain why mood measures remained elevated at later time points relative to self-report. In addition, we cannot exclude potential bias in the structured interviews, as raters were not blinded to diagnoses or time since concussion.
Our observation of increased plasma levels of QUIN and decreased KYNA/QUIN following concussion is consistent with previous reports of increased QUIN levels in the CSF of severe TBI patients.15 ,16 However, contrary to our hypothesis, we did not observe recovery of QUIN or KYAN/QUIN by 1-month postconcussion. Rather, QUIN was significantly higher and KYNA/QUIN was significantly lower relative to healthy athletes at each time point assessed in the current study. In the aforementioned severe TBI work, elevated QUIN was measured in CSF within the first week postinjury,15 with one study observing a peak in QUIN levels at approximately 3-days postinjury.16 However, chronic alterations in peripheral KYN metabolites have been documented in severe TBI patients at least 1-year postinjury. Specifically, chronic TBI patients had higher KYN/tryptophan ratios, indicative of IDO activity and lower KYNA/KYN ratios.22 Our data suggest that alterations in the KYN pathway extend beyond 1-month following sports-related concussion, though we are unable to determine the time course for recovery from these alterations.
Alterations in the KYN pathway, specifically the elevated levels of QUIN and the reduced KYNA/QUIN observed here, may provide some insight into the acute neuropathophysiological consequences of concussion. In the central nervous system, QUIN is produced by infiltrating macrophages and activated microglia, and is thought to have neurotoxic properties via glutamate-mediated excitotoxicity due to its agonism of NMDA receptors.23 Conversely, KYNA is thought to exert neuroprotective effects through general antagonism of excitatory amino acid receptors.24 For example, direct administration of KYNA to the hippocampus 30 min prior to an experimental brain injury reduces both microglia and astrocyte response25 and intravenous injection of KYNA reduces hippocampal oedema, neuronal loss, and cognitive dysfunction following experimental brain injury.26 ,27 Given their seemingly opposing effects, the ratio of KYNA/QUIN has been proposed as a putative neuroprotective marker that reflects the general balance of the KYN pathway.10 The results presented here are the first evidence of elevated levels of putatively neurotoxic kynurenine metabolites and decreased levels of putatively neuroprotective kynurenine measures following mTBI or concussion.
Importantly, plasma kynurenine metabolite levels were significantly associated with mood symptoms in concussed athletes in the current sample at multiple time points postconcussion. The inverse correlation between KYNA/QUIN and mood symptoms at T1, and the positive correlation of QUIN and mood symptoms at T3 are consistent with previously reported relationships between mood symptoms and KYNA and QUIN levels in psychiatric patients. For example, reduced KYNA and elevated QUIN was documented in CSF of suicide attempters for over a period of 18 months, and the ratio of peripheral KYNA/QUIN was inversely correlated with anhedonia in patients with MDD.10 ,12 ,13 Here, concussed athletes with the highest QUIN levels 1-month postconcussion also had the poorest outcome, as determined by clinicians trained in sports medicine following recommended guidelines. Currently, diagnostic and prognostic decisions following concussion are based on clinical judgment informed by a variety of metrics. However, physicians must rely on patient self-report for many postconcussion symptoms, such as mood symptoms, which are susceptible to intentional under-reporting.28 ,29 This is the first evidence of a relationship between KYN abnormalities, mood symptoms and outcome following concussion. We are unable to identify a causal relationship between these factors. It is possible that concussion alters KYN pathway metabolites, which in turn drive mood changes. Alternatively, psychological changes surrounding the concussive event (eg, concern about return-to-play and overall health) could also promote changes in the KYN pathway. Nevertheless, these data suggest that the measurement of KYN metabolites in the periphery might be one potential target for the development of objective markers to aid clinical management of concussion.
Abnormalities in the KYN pathway have been previously observed in a variety of psychiatric disorders and neurodegenerative diseases associated with chronic behavioural and neuroanatomical abnormalities.5 We have previously demonstrated relationships between KYN abnormalities and hippocampal volume loss in patients with MDD and bipolar disorder.10 ,11 Hippocampal volume loss has also been documented in athletes with a history of concussion.1 ,2 Furthermore, behavioural deficits have been observed in athletes with a history of concussion, with multiple concussions significantly increasing the risk for the development of depression and mild cognitive impairment.30 ,31 Repeated acute alterations in the KYN pathway, such as increases in QUIN and decreases in KYNA/QUIN, may provide one potential mechanism behind long-term changes observed in a subset of athletes with a history of concussion; however, additional studies are needed to support this hypothesis.
These results must be interpreted within the limitations of the current data set. First, although we hypothesise that the observed KYN differences are a consequence of concussion, it is plausible that these are associated with pre-existing factors that predate the current incident. For example, concussed football players self-reported a greater number of prior concussions than healthy football players, and we are not able to separate the cumulative effect of repeated concussions from the effects of the latest concussion. In addition, two concussed athletes had a self-reported history of attention deficit hyperactivity disorder, which could also partially confound the current results. Additional factors that may influence results include genetic predisposition to psychiatric or neurodegenerative diseases, substance use or other trait characteristics. Future studies longitudinally assessing KYN metabolites pre and postconcussion are needed to confirm our hypothesis. Second, the extent to which peripheral levels of KYN metabolites reflect brain levels is uncertain. However, similar findings have been observed in MDD in CSF and the periphery.10 ,13 Moreover, compromised blood–brain barrier integrity is observed in animal models of mTBI,32 which would allow biomolecules, including KYN metabolites, to pass in both directions. In addition, multiple a priori correlations were performed between mood measures and KYNA/QUIN and QUIN in concussed athletes; thus, we cannot rule out the possibility of type I error. However, strict multiple comparison correction for these analyses would be overly conservative due to the fact that both the kynurenine metabolites and the mood measures are not independent. Finally, although the relationship between inflammation and the KYN pathway has been established,9 inflammatory measures for the current sample are not available. Thus, we are not able to determine whether KYN abnormalities are a direct result of a postconcussion inflammatory response.
Conclusion
This work constitutes the first evidence of KYN pathway abnormalities in concussion as well as the first demonstration of an association between KYN pathway abnormalities, postconcussion mood symptoms and concussion outcomes. Alterations of the KYN pathway may constitute a biomarker for depressive symptoms following concussion and may also provide insight into the potential mechanisms underpinning the long-term behavioural and neuroanatomical sequelae of repeated concussions. Well-controlled, large-scale studies are needed to investigate the potential relationship between acute KYN pathway dysregulation and the development of long-term consequences associated with repeated head injuries.
Acknowledgments
The authors thank the psychiatric assessment team at the Laureate Institute for Brain Research for their assistance in data collection and Christopher Nerio, Dr Thomas Allen and Dr Lamont Cavanagh for athlete referral and injury oversight. Blood samples were processed and stored with assistance from Ashlee Taylor at the University of Oklahoma Integrative Immunology Center and processed by Marieke van der Hart at Brains On-Line (http://www.brainsonline.org). This article was prepared while Patrick SF Bellgowan was employed at The National Institute of Neurological Disorders and Stroke. The opinions expressed in this article are the author’s own and do not reflect the view of the National Institutes of Health, the Department of Health and Human Services, or the United States government.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Contributors RS was responsible for acquisition, analysis of data; drafting of work and final approval. JS was responsible for interpretation of data; revising of work and final approval. TKT was involved in conception, interpretation of data; revising of work and final approval. DWP was involved in interpretation of data; revising of work and final approval. ARM was responsible for interpretation of data; revising of work and final approval. PSFB was responsible for conception, design, acquisition, interpretation of data; revising of work and final approval. TBM was involved in design, acquisition, analysis,and interpretation of data; drafting and revising of work; final approval.
Funding This research was conducted using internal funds from the Laureate Institute for Brain Research, which is supported by The William K Warren Foundation.
Competing interests JS declares no competing interests but has received research funding from Janssen Pharmaceuticals for an independent study and a lecture honorarium from University of Kansas–Wichita.
Ethics approval Institutional review boards.
Provenance and peer review Not commissioned; externally peer reviewed.