Article Text

Abstract
Objective To identify physical activity (PA) accrued while playing golf and modifiers of PA accrued.
Design A rapid review of primary research studies. Quality was assessed using the National Heart, Lung, and Blood Institute quality assessment tool for cohort and cross-sectional studies.
Methods and outcomes The following databases were searched from 1900 to March 2017: SPORTDiscus, Web of Science, PsycINFO, MEDLINE, Google Scholar, Google Advanced Search, ProQuest, WHO International Clinical Trials Registry Platform. All primary research investigating golf or golfers with any of the following outcomes was included: metabolic equivalent of task, oxygen uptake, energy expenditure, heart rate, step count, distance covered, strength, flexibility, balance, sedentary behaviour.
Results Phase one searching identified 4944 citations and phase two searching identified 170 citations. In total, 19 articles met inclusion criteria. Golf is primarily a moderate intensity PA, but may be low intensity depending on the playing population and various modifiers. Less PA is accrued by those who ride a golf cart compared with those walking the course.
Conclusions Golf can be encouraged in order to attain PA recommendations. Further research is required into the relationship between golf and strength and flexibility PA recommendations and how modifiers affect PA accrued.
PROSPERO registration number CRD42017058237.
- golf
- physical activity
- health
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: http://creativecommons.org/licenses/by/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This study is, to our knowledge, the first systematically conducted review to focus on golf and physical activity (PA).
A comprehensive overview of golf and PA.
Rapid review—streamlined methods are not subject to the same rigour as a systematic review.
There was limited evidence with regard to strength and flexibility outcome measures.
Introduction
Moderate intensity physical activity (PA) is known to provide longevity, physical and mental health benefits.1–4 PA guidelines1 generally recommend, for adults, at least 150 min of moderate intensity activity or 75 min of vigorous PA per week or a combination of the two. In addition, PA to improve muscle strength on at least 2 days a week and efforts to minimise the amount of time spent sedentary are recommended. An estimated 41%–51% of women and 32%–41% of men do not meet these guidelines5 6 in the UK. Furthermore, the proportion of adults meeting guidelines decreases with age—only 7%–36% of adults aged 75 and over meet the recommendations.5 6
Golf is a popular sport played by over 50 million people7 of all ages and abilities in over 200 countries.8 In contrast to most sports, participation is higher in middle-aged and older adults.9–11 Reviews and guideline documents have suggested golf can provide moderate intensity1 12–14 and muscle-strengthening PA.13 These studies have not formally assessed the quality of the evidence.
The frequently cited Compendium of Physical Activities11 is a classification of intensity costs of various physical activities. It lists golf as, on average, providing 4.8 metabolic equivalents of task of PA, a moderate intensity.
A recently published systematically conducted scoping review10 15 provided an overview of golf and health and further highlighted that golf can provide moderate intensity PA. As per standard guidelines for undertaking scoping reviews,16 the relative strengths and limitations of included studies were not assessed. There have been no other reviews found that use systematic methods exploring PA and golf. We therefore aimed to provide a rapid review to identify PA accrued while playing golf.
Murray et al’s10 scoping review noted several factors that influence the intensity of PA while playing golf: use of a golf-cart, course profile, age, weight, sex and baseline fitness of participants.10 Our secondary aim was therefore to report modifiers to the amount of PA accrued while playing golf.
Methods
Our systematic review adhered to our published protocol17 and followed Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.18
Rapid reviews are a streamlined, time efficient and pragmatic approach to synthesise evidence. They have been shown to produce similar conclusions to systematic reviews.19 Variable methodologies have been described20 and therefore guidance was sought as to the best approach.21 A rapid review was conducted due to a short time-frame in which to complete the research. To streamline the process, the search strategy from a recent scoping review10 was used and adapted, there were less exhaustive searches of grey literature and only one reviewer assessed all papers for selection, data extraction and quality assessment compared with a full systematic review. Similar concessions have been described in the literature.22
Search strategy
We adopted a two-phase search strategy. The first phase employed the search strategy used in the recently published scoping review published by team members10—a precursor to this rapid review. The scoping review search was undertaken in November 2015 across the following databases: SPORTDiscus, Web of Science, PsycINFO, MEDLINE, Google Scholar, Google Advanced Search, ProQuest dissertations, WHO International Clinical Trials Registry Platform. The search identified 301 studies relating to the scoping review’s aims—the relationship and effects of golf on physical and mental health. Forty-nine of those studies were found to be specifically related to golf and PA, which will be used in the current review.
The second phase of the search strategy involved adapting and updating the scoping review search. The search was rerun restricting its scope to search for papers related to golf and PA only that were published from November 2015 to March 2017. A focused grey literature search was performed using the modified terms ‘golf AND health’. The full search strategies can be found in online supplementary appendices 1 and 2.
Study selection
One reviewer (JL) selected studies for review first by title and abstract, then by full text review, against inclusion/exclusion criteria with the exception of title and abstract screening of phase two results, conducted by DA. A second reviewer (EJ) independently reviewed a random sample of 10% of the papers by full text review for inclusion or exclusion. Concordance was checked and any discrepancies were discussed and resolved by a team member, either ADM or DA.
Inclusion and exclusion criteria were developed through researcher discussion:
Inclusion criteria
Research articles not limited by geographical location, language or setting.
Research articles published since 1900 up until March 2017.
Research articles discussing any of the following outcomes in relation to golf: metabolic equivalent of task (MET), oxygen uptake, energy expenditure (EE), heart rate (HR), step count, distance covered, strength, flexibility, balance, sedentary behaviour.
Any form of playing golf (including but not limited to 18 holes, 9 holes, driving range) or research involving golfers.
All ages groups and both sexes of participants.
Sources of information including randomised control trials, cohort, case-control and cross-sectional studies, that have been synthesised quantitatively.
Exclusion criteria
Studies focussing exclusively on caddies and/or spectators.
Qualitative studies, reviews, opinion pieces, magazine and newspaper articles, case reports, conference proceedings.
Data extraction
Data were extracted by one reviewer (JL) using a data extraction form. The data extraction form was piloted using 10% of papers and modifications were made. A further random sample of 10% was independently extracted by a second reviewer (EJ) and results compared. Concordance was checked and any discrepancies were discussed and resolved by a team member, either ADM or DA. A sample data extraction form can be found in online supplementary appendix 3.
Supplementary file 3
Quality assessment
Our protocol17 details use of the Effective Public Health Practice Project’s quality assessment tool for quantitative studies23 to assess study quality. After trialling, it became apparent the tool was more suited to interventional studies with groups. As the large majority of included studies are observation cross-sectional design, the tool was not suitable and therefore the National Heart, Lung, and Blood Institute quality assessment tool for observational cohort and cross-sectional studies24 was used. Eligible studies were assessed by one reviewer (JL). A second reviewer (EJ) independently assessed a random sample of 10% of the papers using the same tool. Concordance was checked and any discrepancies were discussed and resolved by a third researcher, either ADM or DA. Studies rated ‘Fair’ or ‘Good’ were included in the review.
Data synthesis and analysis
Due to the wide heterogeneity of included studies in terms of study design, population, setting, outcomes and study quality, data were synthesised narratively with summary tables and figures using the following outcomes: MET, EE, oxygen uptake, HR, steps taken, distance covered, strength, flexibility, balance and sedentary behaviour. Modifiers to PA accrued were noted during data extraction and were also narratively synthesised. There were no principal summary measures due to the studies’ heterogeneity; data were presented using the raw outcome measures.
Results
Study selection
In total, 3550 independent records were identified through our systematic two-phase electronic search. Three thousand three hundred and eighty independent records were identified in phase one.10 Three thousand and fifteen records were excluded on screening of title and abstract, and 64 articles were excluded by full text review. Of the remaining 301 articles, 49 were specifically related to golf and PA. A flowchart detailing the results of phase one of the search can be found in online supplementary appendix 4.
Supplementary file 4
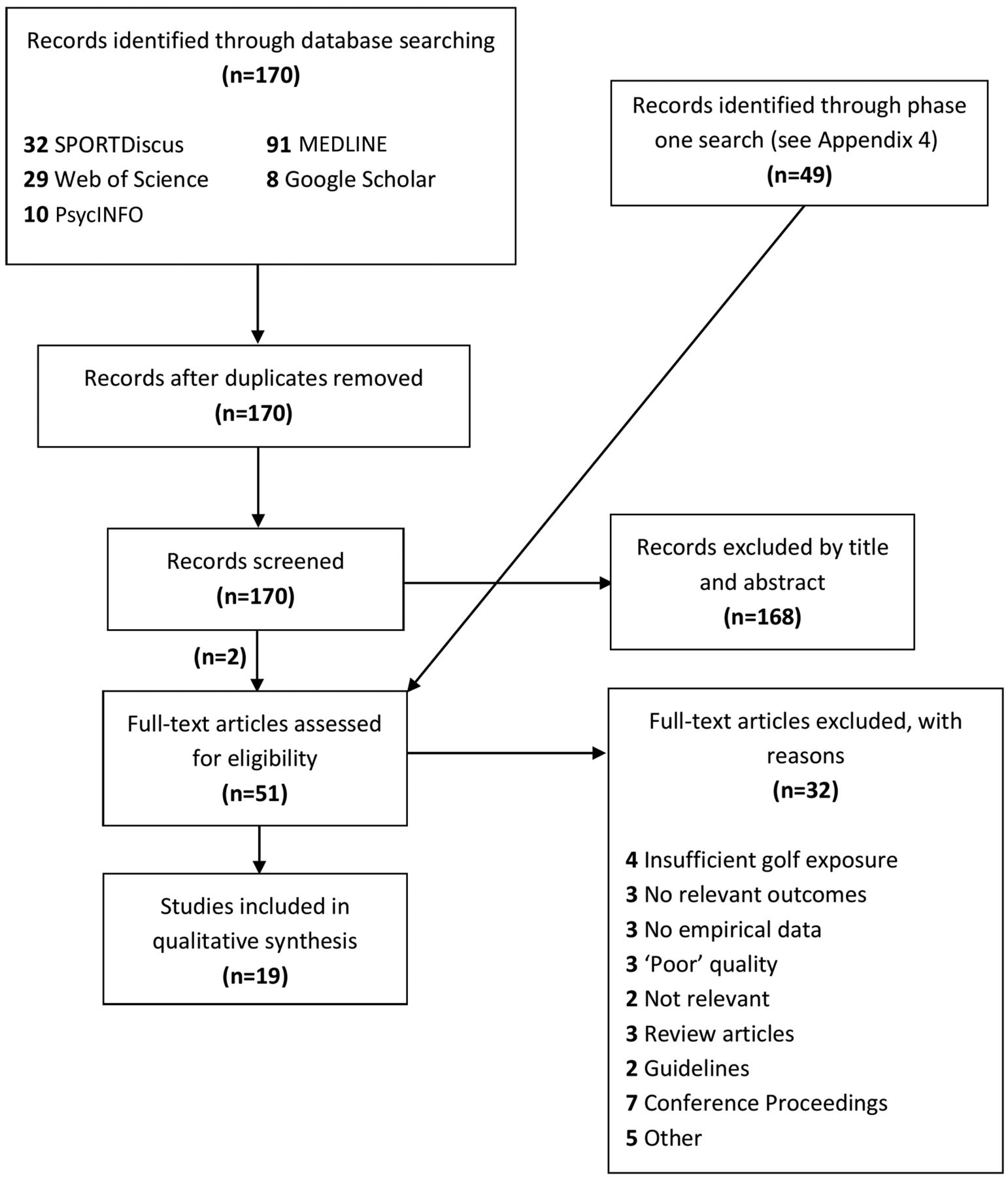
Phase two of the search identified 170 further independent records (figure 1). One hundred and sixty-eight records were excluded by title and abstract. The 49 articles from phase one were included here and assessed for eligibility by full text review. Thirty-two articles were excluded by full text review. Nineteen articles remained that met the inclusion criteria and were included in the review. Citations of included studies can be found in online supplementary appendix 5.
Supplementary file 5
{kind=link}
Results of systematic electronic search.
Study characteristics
Of the 19 included studies, 11 were conducted in USA, 3 in China and 5 in other countries (Germany, Sweden, Austria and Norway). All included studies were cross-sectional design. Sixteen of the identified studies were primary published research papers, and three were published dissertations. The studies’ publication dates ranged from 1970 to 2015. Four of the studies were published pre-2000, and 15 studies were published post-2000.
Ten different outcome measures were used in the review. The most frequently reported were: HR (10 studies), EE (9 studies) and METs (6 studies). No studies reported on sedentary behaviour. Further characteristics of included studies are presented in online supplementary appendix 6.
Supplementary file 6
Quality of included studies
Information on quality assessment of included studies can be found in online supplementary appendix 7. All studies provided a clear objective or research question. Most studies (74%) did not provide a sample size justification, power description or variance/effect estimates. It was unclear in the majority of studies whether outcome assessors were blinded to exposure status of participants (68%). Five studies were rated ‘Good’ and 14 were rated ‘Fair’.
Supplementary file 7
Outcomes
Energy expenditure
Nine studies identified EE as an outcome.25–33 Eight studies were rated ‘Fair’25–31 33 and one rated ‘Good’.32 Results are detailed in table 1. Two studies found significantly higher EE on hillier courses compared with flatter courses. Zunzer et al,32 however, found no significant difference in EE between hilly and flat courses.
EE for a round of golf
Lampley et al 30 noted a significantly higher rate of EE in women. In contrast, two studies32 33 found males expended significantly more energy than females. However, Zunzer et al 32 noted that this is not significant if body mass is accounted for and Tangen et al 33 suggested that this may be due to differences in course distance.
Two studies25 33 found no significant difference in EE in relation to skill level, despite less skilled players taking a larger number of shots in total and on average being less able to advance the ball accurately.
Crowell26 noted the lowest EE when riding a golf cart, then pulling clubs and highest when carrying clubs. Zunzer et al 32 found that those who rode a golf cart had significantly lower EE than those who pulled or carried clubs. Tangen et al 33 found no significant difference in relation to club transportation; however, it is noted that this may be due to small sample size in each group.
Metabolic equivalent of task
Six studies identified MET as an outcome.27–29 32–34 Four of the studies were rated ‘Fair’27–29 33 and two rated ‘Good’.32 34 Results are detailed in table 2. Dobrosielski et al 28 found a significant difference between patients with cardiac disease and healthy adults in average MET (57±2.7; 46%±2.6% peak MET) and peak MET (89±3.3; 77%±3.6% peak MET). However, Unverdorben et al 34 found the same MET value (3.1) for patients with cardiac disease and healthy adults. Zunzer et al 32 noted no significant difference in METs between sexes, whereas Tangen et al 33 found an almost significant difference between men and women (P=0.069). Zunzer et al 32 found no significant difference in METs between hilly and flat golf courses.
MET of a round of golf
Heart rate
Ten studies reported HR as an outcome.25 26 29 31–37 Eight were rated ‘Fair’25 26 29 31 33 35–37 and two rated ‘Good’.32 34 Mean HR and mean percentage of maximum HR (%HRmax) are presented in table 3. In relation to maximum HR, Stauch et al 35 found that most time during a round of golf is spent at 50%–74% HRmax. Tangen et al 33 described that 75% of a golf round is played at <70% HRmax and 25% is >70%. Broman et al 35 found that 70% of total time for elderly men is at >70% HRmax, whereas, for middle-aged and younger men, most time is spent at <70% HRmax. Loy31 estimated that 75.25 min are >60% HR reserve.
Mean HR and percentage of maximum HR during a round of golf
One paper25 noted a significant difference in mean HR and a second paper36 time spent >40% HRmax between hillier and flatter courses. Two papers found no significant difference in mean HR in relation to course profile.32 33 However, Tangen et al 33 found a significantly higher maximum HR on the hillier course.
Two papers found highest HRs when carrying clubs, then pulling clubs and lowest when riding a golf cart.26 36 One of these studies36 found a significant difference in percentage of time spent >40% HRmax between carrying and pulling clubs and riding a golf cart. Similarly, Zunzer et al 32 found that participants who rode a golf cart had significantly lower mean HR than those who carried or pulled their clubs. Stauch et al 37 observed no significant difference in mean or maximum HR in relation to club transportation. However, it is noted that there are significant differences in ages, a possible modifier to PA attained, between groups—this was also observed in another study.32
Crowell26 noted little difference in mean HR in relation to skill level and Burkett et al 25 found no significant difference. In relation to sex, two papers32 33 observed no significant difference in mean HR and one paper,32 minimum, maximum HR or mean percentage HRmax. Broman et al 35 found that older golfers spent significantly more time at higher %HRmax than middle-aged or younger golfers. Tangen et al 33 found that older golfers (>50 years) spent less time at high intensity level (>120 bpm) than younger golfers (<50 years)—but suggested that this may be due to differences in maximum HR. Unverdorben et al 34 observed no significant difference in mean HR between patients with cardiac disease and healthy controls, but noted that the maximum HR of controls was higher and therefore patients with cardiac disease may work harder.
Oxygen uptake
Four studies listed oxygen uptake as an outcome.26 27 31 34 Three were rated ‘Fair’26 27 31and one rated ‘Good’.34 Results are detailed in table 4. Crowell26 found that riding a golf cart required least oxygen uptake per minute, then pulling clubs and carrying clubs required the most oxygen uptake per minute. The study also noted that golfers of lower handicaps (≤10) required less oxygen per minute when pulling or carrying clubs than golfers with higher handicaps (≥11). Dear et al’s27 value of 9.9±1.7 mL kg–1 min–1 equates to 34.4%±9.1% oxygen uptake reserve. Unverdorben et al 34 found that patients with cardiac disease had a significantly higher %VO2max while playing golf compared with healthy controls.
Oxygen uptake during a round of golf
Steps taken
Three articles were found with steps taken as an outcome.29 33 38 All studies rated ‘Fair’ in quality assessment. The included studies all involved an 18-hole round of golf. Studies found that 11245±1351,29 11948±1781,38 16080±1195 (male)33 and 16667±992 (female)33 steps were taken during a round of golf. One study29 found significant negative correlation between number of steps taken and: weight of the golf bag (P<0.05), EE (P<0.01) and minimum HR (P<0.01) of participants.
Distance covered
Five studies detailed distance covered as an outcome.26 27 29 32 33 Four of the studies were rated ‘Fair’26 27 29 33 and one study33 was rated ‘Good’. Results are detailed in table 5. With the exception of Crowell,26 all studies estimated between 8.7 and 11.25 km walked for an 18-hole course and 4.4 and 5.32 km for a 9-hole course. Distance covered is highly dependent on the individual golf course length. The course in Crowell’s study is poorly described, but this may account for the shorter distance. A much shorter distance (3.18 km) is walked riding a golf cart compared with pulling a golf cart or carrying clubs.26 There is no notable difference in distance walked when pulling a golf cart compared with carrying clubs. Males walked longer distances than females. Zunzer et al 32 noted a significant difference between male and female distance walked over 18 holes. However, in both studies32 33 and as is usual on golf courses, the men’s course is longer than the women’s. Tangen et al 33 found that, when course length is accounted for, women (2.13 times the course length) walked significantly longer than men (1.98 times the course length).
Distance covered in a round of golf
Strength
One study listed strength as an outcome39 and rated ‘Good’. Sell et al 39 found that golfers with a lower handicap (<0) had significantly greater strength over a range of measures when compared with handicaps of 0–9 and 10–20. Tables are not listed for strength, flexibility or balance outcomes due to the heterogeneity of measurements.
Flexibility
One study listed flexibility as an outcome39 and rated ‘Good’. Sell et al 39 found that golfers with a lower handicap (<0) had significantly greater range of motion in several measures of shoulder, hip, torso flexibility than golfers with higher handicaps (0–9 and 10–20).
Balance
Five studies listed balance as an outcome.39–43 Three studies rated ‘Good’,39 40 42 and two studies rated ‘Fair’.41 43 Three studies focused on older golfers,40–42 and all papers found elderly golfers had significantly better balance control when compared with controls over a variety of measures. Tsang et al 41 noted that the balance of elderly golfers was comparable to that of young controls (no significant difference).
Sell et al 39 found that golfers with better handicaps (<0) had significantly better single-leg balance than golfers with handicaps 0–9 and 10–20. Schachten et al 43 noted a significant improvement in patients with stroke after participating in a 10-week, 20-session golf putting intervention. However, a significant improvement was also noted in the comparator group and no significant difference was observed between groups.
Discussion
EE for an 18-hole round of golf appears to achieve the America College of Sports Medicine’s (ACSM) recommendation of 1000 kcal week–1,44 and could be separated into two 9-hole rounds. The length of time a round of golf takes can compensate for the low EE per minute. Fifty per cent of MET values stated are within the range of moderate intensity (3–5.9).44 Values for %HRmax are within light intensity (50%–63%) and moderate intensity (64%–76%).14 Using the mean age of golfer in UK (63 year45), the mean range for moderate intensity is 101–119 bpm—the large majority of data fall into this category.
There were varied results in oxygen uptake. In terms of VO2max, studies classified golf as light (37%–45% VO2max), moderate (46%–63% VO2max) and vigorous (64%–90% VO2max).44 Many studies were close to, but did not reach, the moderate intensity threshold of 10.5–20.7 mL kg–1 min–1 (3–5.9 METs) and would therefore be classified as light activity (<10.5 mL kg–1 min–1).
All included studies, on average, attained the often cited 10 000 steps44 during an 18-hole round and, according to Tudor-Locke et al,46 would be classed as moderate-to-vigorous PA. Distance walked is highly variable depending on the course; values range from 6.4 to 11.3 km for an 18-hole round and 4.4–5.3 km for a 9-hole round. In relation to strength, flexibility and balance, greater strength and range of motion were found in those with higher proficiency.39 It is unclear whether this is due to increased volume of play, additional strength/flexibility work or whether these characteristics are likely to lead to a lower handicap. Furthermore, there appears to be better balance control in golfers. The complex motion while swinging a club and/or walking on uneven grounds during golf play may lead to improved stability; however, this cannot be proven due to the methods employed in this study.
Evidence suggests that use of an electric golf cart significantly reduces PA attained in terms of EE, HR and distance covered. Males expend more energy and walk further distances than females. However, it is likely that this difference is due to greater body mass and longer course length played by males. When course length is accounted for, women walk significantly longer.33 Skill level does not appear to affect PA accrued, with the possible exception of strength, balance and flexibility. The evidence is unclear whether course profile and age affect PA accrued.
This study is, to our knowledge, the first systematically conducted review to focus exclusively on golf and PA. It provides a general overview of PA accrued while playing golf. A rapid review was conducted due to time constraints. Rapid reviews make use of streamlined methods and, due to this, are not subject to the same rigour as systematic reviews. For some outcomes, there was little available evidence. Furthermore, the sample sizes of included studies were generally small and ranged from 6 to 257 (median 22).
In agreement with the recent scoping review10 and the Compendium of Physical Activities,11 golf can provide moderate intensity PA. Exercise intensity varies during the game itself. For certain populations, it may be primarily a low-intensity PA. Shortfalls in intensity, however, are compensated for by the length of the game. Therefore, golf is a viable sport by which to achieve the PA recommendations.1 Golfers may find it difficult to play enough during a week in order to reach PA recommendations and may wish to supplement golf with another PA. Clinicians and policy-makers can be encouraged to suggest golf as a form of PA in order to meet recommended levels and attain health benefits.
Further research is warranted to investigate whether strength and flexibility is accrued while playing golf as well as research examining the effect of modifiers such as age, course profile, disease characteristics and carrying or pulling clubs, on PA attained.
Conclusion
This rapid review identified 19 articles that examined golf and PA. Golf is primarily a moderate intensity PA, but may be low intensity or even high intensity depending on the population and various modifiers present. If able, golfers should walk the course, rather than ride a golf cart to maximise health benefits. Course profile, skill level and age may affect the amount of PA accrued, and further research is required.
Supplementary file 1
Supplementary file 2
References
Footnotes
Contributors JL: Lead researcher. Performed study selection, data extraction, quality assessment and narrative synthesis. ADM: Primary supervisor. Provided advice on methods including study selection criteria, data extraction and presentation of data. Performed phase one of the search strategy (previously published). EJ: Independently reviewed 10% of paper for study selection, data extraction and quality assessment. DA: Senior researcher. Performed phase two of search strategy and phase two study selection by title and abstract. Provided advice on methods including study selection criteria, data extraction and quality assessment.
Funding This work was supported by the Medical Research Council (MRC; MR/K023209/1).
Competing interests Although not for this project, ADM has previously received funding to complete research from the World Golf Foundation. The World Golf Foundation committed to publishing whether results were positive, negative or equivocal and had no influence on the conduct of this or previous research.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement There are no additional unpublished data.