Article Text

Abstract
Objectives: To describe the demographics and nature of injuries occurring on or around horses, to examine the nature of protective clothing in relation to these injuries, and to compare our data with previously published work in this area.
Methods: Patients were identified using the term “sports injury–horse riding” from the departmental database for one calendar year from February 2000. Data were collected regarding demographics, injuries, protective clothing, and outcome. The data were then analysed and compared with the previously published literature.
Results: 260 patients’ records were analysed. The patients were mostly young (median age 26) and female (84.6%). The majority of patients had a single injury (88.8%). Seventeen per cent had an isolated head injury, all of which proved to be minor. Multiple injuries including the head accounted for 8.5% of all injuries. These again proved minor, bar one fatality where the helmet came off before impact. Upper limb injuries accounted for 29.2% of all injuries of which 61.8% sustained a fracture of which 36.2% were to the wrist. When compared with previous work the incidence and severity of head injury continues to decline while the relative number and severity of upper limb injuries increases.
Conclusions: The majority of head injured riders are wearing approved helmets and sustaining only minor injury. There is currently no protective gear recommended for the upper limb and more specifically the wrist. This paper identifies the potential need for research and development of such protection.
- horse injuries
- protection
Statistics from Altmetric.com
Equestrian related injuries have received considerable media attention in the past two years with five deaths in eventing and serious injuries to several leading jockeys.1 Injuries related to equestrian accidents form only a small percentage of attendances to the accident and emergency (A&E) department. Lloyd noted that in 1984 it amounted to 0.3% of 78 000 attendances 2 and Muwanga found that 2.6% of all admitted head injuries were horse related.3 Whitlock, in a study of 21 A&E departments in 1986, found that horse riding injuries accounted for 1.43 injured persons per 1000 new attendances. One of the hospitals in Whitlock’s thesis, Warwick, covers a demographic catchment area that could be considered similar to Guildford. At Warwick 179 injuries were collated and this represented 6.5 per 1000 new attendances.4
Limb injuries have been considered the most common type of injury with approximately one third to the upper limb; Whitlock,4 Goulden,5 Lloyd,2 but few papers have discussed these in detail apart from Whitlock,4 and Regan.6
The risk of a serious head injury has been well documented.2–5,8,9 It would seem, however, that there has been a reduction in head injuries over the past 20 years. Barber in 1971 noted 66% of admissions were attributable to a head injury 7 and when Chitnavis 8 repeated the study in 1991 this figure was reduced to 26%. Edixhoven in 1979 9 found that head injury admissions in a mainly professional group of jockeys was 40% and Lloyd in 1984 50%.2 Gleave recorded 162 admissions to a regional neurosurgical unit over a 12 year period until 1975, compared with 132 rugby injuries.10 Whitlock found that 23% of all admissions in a mixed population were attributable to a head injury and 3% of these needed neurosurgical intervention, with 3 of 5 deaths being attributable to a head injury.4
The main reason for the reduction in head injuries has been given as improved protective helmet design. The BS 3686 helmet 11 was first introduced in 1963, but studies have mainly noted whether a helmet was worn and did not mention if it was to a recognised standard. In the Oxford study 42% wore some form of helmet in 1971 7 and 73% in 1991.8 In Muwanga’s study in Nottingham in 1983 all riders wore a helmet, but there was one death and six fractures to the skull.3 Ilgren, in 1984, also highlighted the inadequate protection of helmets in a study of six fatalities, comparing them to five non-fatalities where the standard of helmet was higher.12 Some studies reported many riders not wearing any headwear. McGhee found that in one half of skull fractures documented 50% were not wearing any form of head protection.13 He concluded that in the other 50% the helmet was inadequate.
In 1972 an improved protective helmet was introduced for professional jockeys and D’Abreu of the Jockey Club noted a reduction in head injuries from 46 in the 1967–8 season to 27 in the 1973–4 season.14 Mills in 1988 was concerned that this helmet was still not providing enough protection. Many of the injuries he investigated were to the side of the head where protection provided by the helmet was minimal.15 The European standard (CEN) was introduced in 1996 and all protective helmets worn in this country have to at least conform to the minimum performance requirements.16
There has not been a publication investigating equestrian injuries in a district hospital without neurosurgery on site for over 10 years. There has also been no study to determine if the new helmet standard has continued to cause a reduction in head injuries. This paper is intended to determine whether the pattern and severity of injuries has changed. It also will provide the only information on the incidence of injuries in the Guildford hospital catchment area.
METHODS AND LIMITATIONS
Patients attending the A&E Department of the Royal Surrey County Hospital between February 2000 and February 2001 were identified from the “Oasis” patient record system by using the term “sports injury–horse riding”. The following data were extracted and entered onto a spreadsheet (Excel); demographics, mechanism of injury, anatomical location of injury, type of injury, treatment, and disposal. The wearing of protective clothing was noted if documented in the records. Patients who were admitted had their inhospital records retrieved and analysed for outcome. This process was fully anonymised. Ethical approval was granted by the Royal Surrey County Hospital Trust Ethics Committee.
It should be recognised that this is a retrospective study, but the relative large numbers and the manner in which the information was collected suggest that the data are accurate.
RESULTS
The total number of new attenders in the A&E department during the study period was 46 517. There were 2653 (5%) with a sport related injury and of these 276 (10.4%) had a riding related injury. This represents a risk of 5.9 patients per 1000 new attendances. There was one fatality.
It was only possible to analyse 260 records. The majority were women; 220 (84.6%). The majority of patients were aged between 10 and 35 years (66.3%). The median age was 26 with a range of 1 to 65 (see fig 1). There were more injuries in the spring and summer; 75 and 89 respectively.
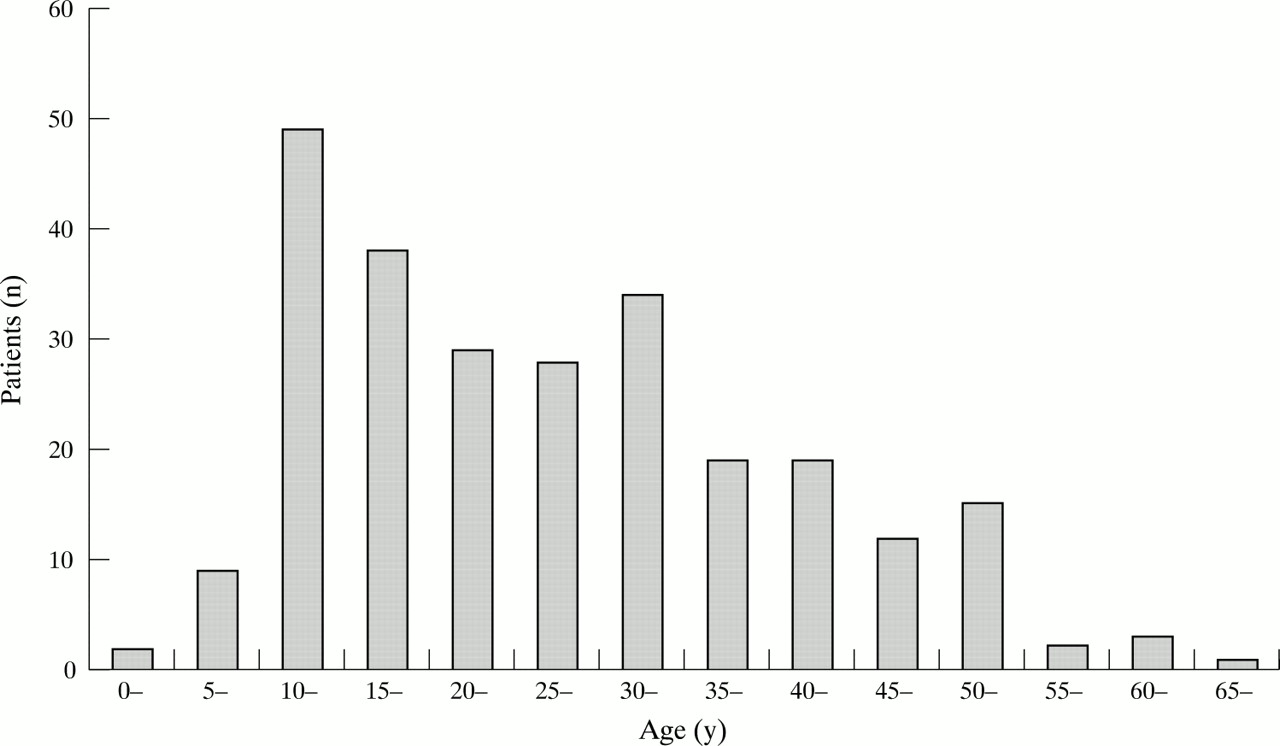
Distribution of patients by age.
In 205 patents (78.8%) the mechanism of injury was a fall, the mechanism in the remainder being kicks 29 (11.1%), bites 2 (0.8%), being trodden on 14 (5.4%), and injury while leading the horse 8 (3.1%). Figure 2 shows the anatomical distribution of injuries.

{kind=link}
{kind=link}
Anatomical distribution of injuries (percentage).
Isolated head injuries constituted 45 (17.3%) of the patients. Thirteen of these (28.9%) had a simple contusion/abrasion, 24 (53.3%) had a cerebral injury, four (8.9%) had a laceration, two (4.4%) sustained a fracture (facial fractures requiring admission), and a further two (4.4%) had multiple injuries to the head. Of those with a cerebral injury, five (20.8%) were admitted. None of these patients required neurosurgical intervention. Helmets were worn by 36 (80%), who all fell from the horse, whereas the nine without helmets were not actually riding when injured.
Twenty nine (11.2%) of patients presented with more than one injury. Of these only three were admitted, one having a thoracic spine fracture (with no neurological sequelae), one having head and facial injuries requiring imaging and observation, and one who sustained a traumatic subdural haematoma as well as pulmonary contusion (this patient was the only fatality in our series). The helmet this rider was wearing came off before impact. A total of four patients were sent to the fracture clinic, two with upper limb and two with lower limb injuries. Twenty two of the 29 patients had sustained a head injury as part of their clinical picture (all 29 were wearing a helmet).
There were only eight (3.1%) patients with isolated neck injuries and one half of these required a radiograph. There were no fractures and no neurological sequelae. All were discharged home from the department.
There were 28 (10.8%) patients with thoracolumbar (including chest) injuries. Twenty four (85.7%) patients suffered contusions, three had fractures, and one had a delayed presentation with a haemothorax. Only three patients in the group were admitted.
There were three (1.2%) patients who sustained isolated abdominal injuries. Two had soft tissue injuries and were discharged and one was admitted for observation following a negative CT scan.
Isolated pelvic injuries accounted for 13 (5.0%) of all the injuries. Ten patients had soft tissue injuries while three had fractures. Two patients with a fracture were admitted, one having a fractured neck of femur sustained when knocked over by a horse and the second had a sacroiliac joint disruption.
There were 76 (29.2%) patients with isolated upper limb injuries, 65 (85.5%) of whom sustained the injury falling from the horse. A total of 47 (61.8%) sustained a fracture. There were 15 distal radial fractures, 11 fractures in the hand, 8 fractures to the clavicle, 8 fractures of the humerus, 2 scaphoid fractures, 2 shoulder fractures, 1 shoulder dislocation, and 1 radial head fracture. Five patients were admitted, two with distal radial fractures, one with a shoulder dislocation, one with a finger fracture, and one humeral fracture. The remainder of the fractures were followed up in fracture clinic. There were 58 (22.3%) isolated lower limb injuries and of these 13 (22.4%) sustained a fracture. Five were in the foot, five in the ankle, two in the tibia, and one neck of femur. A total of six patients were admitted and a further seven went to fracture clinic.
DISCUSSION
This study shows that the number of equestrian injuries collected over a one year period is higher than any other hospital over the past 30 years, but if this is taken as numbers per 1000 attendances it compares favourably with Whitlock’s study in 1986.4 The incidence of admissions has decreased (10.4%) compared with the studies in other hospitals.
In 1984 Lloyd noted that 50% of admissions were from a head injury 2 and at Oxford it had reduced from 66% in 1971 to 26% in 1991.7,8 Muwanga found that six riders wearing a helmet had a skull fracture.3 McGhee found that all the severely injured had a skull fracture despite the wearing of a helmet.13 In our study isolated head injuries accounted for only 17.3% of all injuries and only 15.6% of these were admitted. One can conclude that as most riders are wearing a helmet conforming to the European Standard (or equivalent), it is reducing the incidence of a skull fracture and the severity of the injury.
The relative incidence of upper limb injuries would appear to be increasing when compared with other studies. Whitlock found that 24.3% of injuries affected the upper limb with 42.3% having sustained a fracture.4 In our study 29.2% had upper limb injuries of which 61.8% sustained a fracture. Fractured wrists/scaphoids accounted for 22.4% of the upper limb injuries whereas Whitlock found only 10.8% to have a fracture.
Protective equipment to date has concentrated on the head and body but not the upper limb, especially the wrist. In contrast there is a proposed new standard for roller-blading that includes wrist protection.17 This may prove suitable for horse riders.
CONCLUSION
Horse riding is an extremely popular leisure activity in the United Kingdom, especially in the more rural environment. Equestrian activities can lead to a multitude of injuries ranging from the very minor to the fatal. Our study shows an increase in the number and severity of upper limb injuries relative to head injuries, which continue to decline. We therefore recommend that further research needs to be undertaken looking at the use of protective equipment for the upper limb and especially the wrist.
Acknowledgments
The authors wish to thank Sarah Thompson (Trust Information Analyst) for her invaluable help in collating the data.
Contributors Dr M R Whitlock is guarantor for the paper. Dr M R Whitlock helped Dr Moss with his original proposals. Mr Wan gave assistance in gaining approval from the local ethical committee.
REFERENCES
Footnotes
-
Conflicts of interest: none.
-
Funding: none.