Article Text

Abstract
Background: Sport and exercise related injuries are responsible for about 5% of the workload in the accident and emergency (A&E) department, yet training in sports medicine is not a compulsory part of the curriculum for Higher Specialist Training.
Aim: To determine how A&E medicine consultants and specialist trainees view their role and skill requirements in relation to sports medicine.
Method: A modified Delphi study, consisting of two rounds of a postal questionnaire. Participants were invited to rate the importance of statements relating to the role and training of the A&E specialist in relation to sports injuries (six statements) and the need for knowledge and understanding of defined skills of importance in sports medicine (16 statements).
Value of research: This provides a consensus of opinion on issues in sport and exercise medicine that have educational implications for A&E specialists, and should be considered in the curriculum for Higher Specialist Training. There is also the potential for improving the health care provision of A&E departments, to the exercising and sporting population.
- sports medicine
Statistics from Altmetric.com
Sport and exercise related injuries are responsible for about 5% of the workload in accident and emergency (A&E) departments,1–4 yet training in sports medicine is not a compulsory part of the curriculum for Higher Specialist Training. There is increasing interest in sport and exercise medicine (SEM) in the undergraduate curriculum, and a recent study of medical schools in Great Britain and Ireland, found that SEM was taught in 13 medical school and a further five intend to begin teaching in the next five years.5 The British Medical Association Board of Science and Education, in their report on sport and exercise medicine, highlight the importance of future postgraduate education.6 There is increasing interest in the US.7 General practitioners have also indicated a need for additional training.8
Up to 80% of sports related injuries are of similar nature and degree to road, home or work accidents,9 but athletes and coaches, are unhappy with the standard of injury management.10–12 There is also the suggestion that improved management of all soft tissue injuries would have wider implications, as such injuries are responsible for as much morbidity and time loss from work as fractures.13
The importance of sport and exercise participation in ensuring regular physical activity, known to improve health and prevent disease,14,15 cannot be underestimated. Therefore every effort should be made to preserve function that will facilitate continued participation.
The aim of this study was to find out how A&E medicine consultants and trainees view the role and skill requirements of the A&E specialist in relation to sports medicine. The objectives were to identify those skills that they considered to be most important in accident and emergency.
METHOD
The study used a modified Delphi technique, a well recognised method for seeking agreement on the role and educational characteristics of medical professionals,16,17 and educational content.18 In a Delphi study, participants are asked for their opinions on a list of statements or characteristics relating to a particular role. In this study, the first draft of statements was developed by the author from the literature: key skills identified from a study of consultant surgeons' opinion of the skills required of basic surgical trainees 19; the curriculum for Higher Specialist Training in Accident and Emergency Medicine 20; the syllabus for the examination of the Intercollegiate Academic Board in Sport and Exercise Medicine 21; and a previous similar study of doctors with an interest in SEM in Northern Ireland.22 This draft was revised after discussion with a consultant in sports medicine, and with two consultants and three specialist trainees in A&E medicine, who were purposefully selected because of their varied experience and interest in sports medicine. The second draft was tested for face validity and content validity, with a convenience group of two consultants and four specialist trainees in A&E medicine. The final list contained two groups of statements relating to: the role and training of the A&E specialist in relation to sports injuries (six statements) and the need for knowledge and understanding of defined skills, of importance in sports medicine (16 statements).
This Delphi survey consisted of two rounds. In round one, participants rated the importance of each statement relating to SEM. In round two the same participants, were given an identical list of statements but, on this occasion, they were also given a copy of their own round 1 scoring, and the most frequently cited response from the entire group, with the percentage of those who gave that response. Participants were invited to reconsider their response and change or maintain their original response as they wished.
The list of statements was administered to all 19 consultants, and 11 specialist registrars in A&E medicine in Northern Ireland and non-responders were reminded by telephone. Three participants were not identified in the first mailing but subsequently included.
At the time of the survey none of the participants held a postgraduate qualification in SEM. Only one A&E consultant was involved in a regular sports injury clinic, which she established in 1981.
The results were analysed using SPSS, and differences between the responses to each round were examined using the Wilcoxon signed ranks test, and differences between the consultants and training grades were analysed using the χ2 test. Consensus was confirmed if there was 50% agreement.23
RESULTS
Seventeen of 19 consultants, and nine of 11 specialist registrars completed round one. Response rate to round two was lower, with 15 consultants and four specialist registrars completing the survey. There was no significant difference between responses to round one and round two, confirming stability of response. Nor was there a significant difference between consultants and those in training grades. The responses to the statements are as shown in figures 1 and 2.
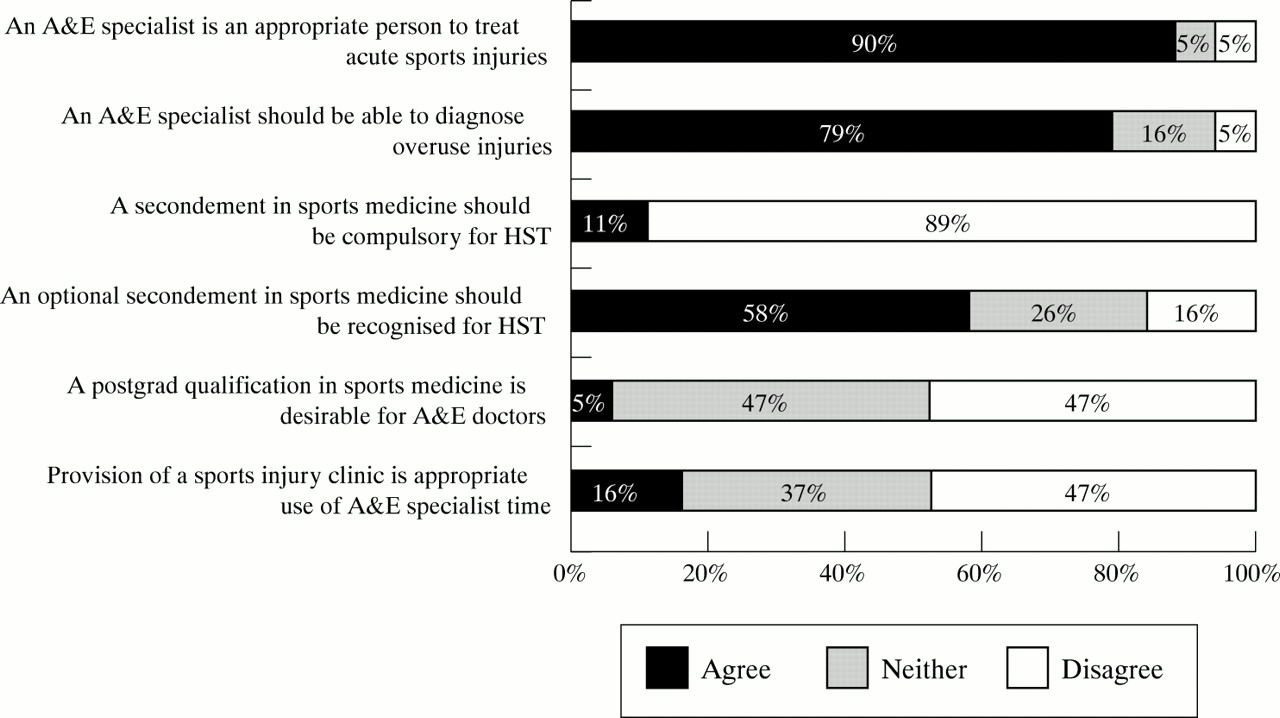
A&E specialist opinion: role and training.

{kind=link}
{kind=link}
Specialist opinion: “the A&E specialist should know and understand”.
There was strong agreement that A&E specialists should treat acute sports injury, and that they should be able to diagnose overuse injuries. Furthermore, the A&E specialist should possess knowledge and skills in all aspects of SEM care with the exception of two domains: how to access “health regulations in sport”, or “drug regulation in sport”, where there was disagreement by 16% and 32% respectively.
In contrast with the agreement on the importance of SEM, participants did not consider that a postgraduate qualification in sports medicine, or compulsory secondment in sports medicine, as part of higher specialist training in A&E medicine, was necessary. Only 5% agreed that a postgraduate qualification in sports medicine was desirable for an A&E specialist. Consensus was just achieved (58%) in recognising sports medicine as an optional secondment for Higher Specialist Training. There was differing opinion (16% agreed; 47% disagreed) on the appropriateness of running sports injury clinics in A&E specialist time.
DISCUSSION
There was widespread agreement on the need for the specialist in A&E to have a role in diagnosis and management of sports injury. There was also agreement that an A&E specialist should have a broad knowledge and understanding of sports medicine issues. Participants believed, however, that qualifications or experience in sports medicine should be optional. This is in contrast with the findings of a study of sports injuries presenting at A&E departments that concluded that A&E staff would benefit from increased training in sports injury management.24 The reason for this anomaly is unknown, but one can speculate that it is because A&E specialists do not consider sports injury to be any different to other soft tissue injuries; or because there have been few opportunities for A&E specialists to experience “the practice of sports medicine”.
Notwithstanding the personal views and the priorities within an A&E department, patients with sports related injury, are an important component of the overall workload within A&E. It seems from the study that sports medicine, a relatively new specialty, which has not yet established a uniform place in undergraduate teaching, deserves special consideration. It is difficult to reconcile the importance attributed to the necessity for knowledge and skills in A&E, when neither group rated education and teaching in this area as important. We recognise that these results identify opinion of a heterogeneous group of A&E specialists in one region only, which may, or may not be representative of the whole of the United Kingdom and Ireland. We hope to confirm our results with a national survey, which is currently underway.
A fundamental question remains about the appropriate training of A&E specialists to deal with sports related problems. A secondment in sports medicine would be an opportunity to acquire “knowledge of the practice”,20 of this related specialty.
Acknowledgments
We wish to thank all A&E consultants and specialist registrars that participated in the survey. We are also grateful to the following for their help with the background of sports medicine in Northern Ireland, the discussion of core ideas, and questionnaire testing: Mr Laurence Rocke, Drs Liz Dowey, Christine Dearden, Mark Bell, Adriel Stewart, Audrey McKelvey, lan Erskine (A&E), and Professor MichaelCullen (Sports Medicine).
Contributors
Liz Abernethy initiated the research, developed the survey tool and wrote the paper. Domhnall MacAuley discussed the study design and edited the paper. Oonagh McNally participated in formatting the study tool, and coordinated data collection. Siobhan O'Neil participated in data analysis and data presentation. Liz Abernethy is guarantor for the paper.
REFERENCES
Footnotes
-
Funding: none.
-
Conflicts of interest: none.
Linked Articles
- Primary Survey