Article Text

Abstract
This article systematically reviews the available literature to improve our understanding of the physiological basis for orthoses under the kinematic, shock attenuation and neuromotor control paradigms. The propositions made under these three paradigms have not been systematically reviewed collectively, and as such, there is no single-point synthesis of this clinically relevant body of evidence and somewhat disparate findings. Our comprehensive search strategy yielded 22 papers. Under each paradigm, the role of orthoses with different design features including combinations of posting, moulding and density was analysed. Where possible, data have been pooled to provide an increased level of confidence in findings. The main findings in the kinematic paradigm were that posted non-moulded orthoses systematically reduced peak rearfoot eversion (2.12° (95% CI 0.72 to 3.53)) and tibial internal rotation (1.33° (0.12 to 2.53)) in non-injured cohorts. In the shock attenuation paradigm, it was found that non-posted moulded and posted moulded orthoses produced large reductions in loading rate and vertical impact force when compared with a control and to a posted non-moulded orthosis. The neuromotor control paradigm seems to be the least conclusive in its outcome. Based on our review, this paper concludes with rudimentary guidelines for the prescription of orthosis, that sports medicine practitioners may use in their clinical decision-making process. The need for further research focusing on the role of injury, particularly in neuromotor control modification and long-term adaptation to orthoses, was highlighted.
Statistics from Altmetric.com
Inshoe foot orthoses are frequently used by clinicians1,–,3 in the management of overuse injuries. The Australian Podiatry Council and American College of Foot and Ankle Orthopedics and Medicine3 define “an orthosis as an appliance to support, align, correct deformity or motion of parts of the body.”1 The conventional kinematic paradigm, on which these definitions are founded, is based on the hypothesis that abnormal pronation of the subtalar joint contributes to lower limb injuries and that orthoses normalise pronation and subsequent coupled movements (eg, internal tibial rotation).4,–,6 However, this has been questioned.7,–,11
In addition to the kinematic paradigm, two other major paradigms have been proposed8 9 12 13; which are essentially the shock attenuation and neuromotor control paradigms. The former is based on the concept that the magnitude of force during impact is a major contributor to overuse injuries14,–,16 and orthoses are proposed to reduce impact force by acting as a cushioning interface between the ground and foot. More recently, the neuromotor control paradigm has been proposed, whereby an orthosis may optimise performance and minimise muscle activity and fatigue by providing input through the sole of the foot.8 9 17
A source of confusion for both the researcher and clinician is the array of materials with various properties (type, density or hardness/firmness) that are either custom moulded or prefabricated into various shapes, which can be further customised by the addition of posting or wedging so as to tilt the device from the horizontal. A systematic review of the literature is timely to provide a critically evaluative synthesis of the physiological basis for orthosis therapy during gait under the kinematic, shock attenuation and neuromotor control paradigms. There is no other single source of evidence of the data synthesised from these paradigms, although there are isolated systematic reviews without meta-analyses available.8 12 18,–,21 This will assist clinicians in their prescription and fitting of orthoses and highlight areas for future research.
Methodology
Search strategy
We undertook a comprehensive, sensitive literature search strategy of Sportsdiscus, Medline, Cinahl, PubMed, Cochrane and Pedro databases from 1971 to September 2008 (fig. 1). Keywords used in the search strategy focused on the three identified paradigms: “ortho*, insole, shoe, foot, electromyography (EMG), muscle activity, biomechanics, kinetic, kinematic, shock attenuation, shock absorption, overuse injur*, leg, lower limb,” with no language restriction. Reference lists of reviews in similar topics and papers that met the inclusion criteria were hand searched (K.M.). Titles and (where necessary) abstracts retrieved by initial search were screened (K.M.), with only clinical trials meeting initial criteria considered for further review.

Search strategy; *, three studies categorised in both kinematic paradigm and shock attenuation; one study categorised in both kinematic and neuromotor control paradigm.
Inclusion and exclusion criteria
Included studies focused on the mechanism of action, rather than efficacy. Excluded were cohorts with neurological (eg, cerebral palsy), systemic (eg, diabetes and rheumatoid arthritis) and degenerative (eg, osteoarthritis) conditions, because these may complicate the analysis of gait.
For each paradigm, papers examining tasks other than gait were excluded because the kinematics, kinetics, muscle activity and shock attenuation in activities such as landing, step-ups, single-leg squats and balance assessments are too dissimilar to gait and often too heterogeneous for pooling.22 23 Papers studying three-dimensional kinematics were only included because with two-dimensional analysis, movement in the frontal plane is strongly affected by the alignment of the foot in the transverse plane.4 24,–,26
Quality assessment
Since there is no validated quality assessment tool suitable for the repeated-measures, laboratory-based study designs included in our review, we adapted the Quality Index,27 which is purported to be superior because it encompasses a profile of scores for rating: reporting, internal validity, power and external validity.27 However, we only used relevant items, such as the reporting items, external validity items 11–13, internal validity (bias) items 14–16 and 18–20 and internal validity (confounding) items 26 and 27. A score for participant characteristics (item 3) was only recorded if studies described participants' injury type, physical activity levels and foot posture. Randomisation (item 23), as described in the Quality Index, was not applicable to all studies (eg, within- participants), so we quarantined it from the overall score and modified it, awarding studies a point if the order of intervention(s) and control were randomised. The maximum score obtainable was 28 from the index.
Data synthesis
Quantitative data synthesis was conducted using Cochrane Review Manager (V.5) with data extracted directly from the papers, and when not available, we attempted to contact the authors. Mean difference between orthosis and comparator conditions and its 95% confidence interval (CI) was calculated. CI containing “0” represents a null effect. Estimates of the treatment effect are also provided in the form of an effect size (ES; difference in mean scores divided by pooled SD),28 and classified as trivial (0–0.2), small (0.2–0.6), moderate (0.6–1.2) and large (>1.2),28 thereby allowing a common metric across all measures.
Results
Search results
Twenty-two papers that studied 30 different designs of orthoses on 34 kinematic and 18 kinetic variables were included (table 1). Analysis only included kinematic or kinetic variables that were investigated by more than three papers.
Studies included in the review
We categorised orthoses into three categories: (1) posted non-moulded, which refers to orthoses that were not contoured to the participant's foot (eg, flat) but with added posting; (2) non-posted moulded, which refers to orthoses that were custom made or contoured to the individual but with no posting; and (3) posted moulded that had both custom-contouring and additional posting. Density was not included in this categorisation, nor orthoses that had an irregular surface (several inbuilt raised areas), but were reported separately.
Studies were further categorised with regard to injury status of the cohorts: (1) no history of injury; (2) history, where participants were injured before orthosis prescription but were improving or asymptomatic during the study; and (3) currently injured. In addition, gait was divided into walking and jogging. Data pooling was conducted when investigations were the same across orthosis design, injury status and gait (ie, walking or jogging). Comparisons were also made either between an orthosis and a control (shoe, running sandal, flat ethylene-vinyl acetate (EVA) insert) or between two orthoses with different designs (posting; moulding; density; location of posting, eg, anterior, lateral, posterior, medial; height of posting, eg, inverted, 4°, etc).
Quality
Quality index scores ranged from 17 to 24, of a possible 28 (mean 20.4; table 2). Studies scored similarly in their reporting styles. Sixteen of the 22 papers presented sufficient data to extract and calculate point estimates of effect (eg, mean and SD/error or ES). Only eight studies attempted to describe adverse or longer-term effects of wearing orthoses. For internal and external validity, all studies performed poorly in three items: (1) generalisability of the sample (item 12), (2) blinding participants (item 14), and (3) blinding assessors (item 15). Thirteen papers randomised the order of intervention(s) and control.
Quality index score
Kinematic effects on the foot and shank
Fifteen papers presented kinematic and kinetic outcomes, studying 29 different orthosis designs, with kinematic variables of rearfoot eversion, tibial internal rotation, and rearfoot eversion velocity (tables 3–5) and kinetic variables of maximum ankle inversion moment and maximum knee external rotation moment (table 6).
Rearfoot eversion results where point estimates of effect and confidence intervals were able to be calculated
Tibial internal rotation comparisons of studies where point estimates of effect and confidence intervals were able to be calculated
Rearfoot eversion velocity comparisons for studies where point estimates of effect and confidence intervals were able to be calculated
Kinematic outcomes for comparisons where point estimates of effect and confidence intervals were able to be calculated
Orthoses versus control
Rearfoot eversion
We found 38 comparisons of an orthosis versus a control. Of these, 28 involved orthoses of various posting and moulding designs. A further four comparisons investigated a semicustom orthosis described as a “mould-of best-fit,”29 five comparisons involved different density materials and one comparison involved an orthosis with irregular surface. Nineteen comparisons measured peak rearfoot eversion and 19 measured rearfoot eversion excursion (table 3). Results of four papers detailing 11 comparisons did not provide enough data to calculate point estimates of effect.
The effect of orthoses on peak rearfoot eversion seems dependent upon design. For posted non-moulded orthoses, pooled data from two studies of participants with no history of injury revealed a 2.12° (95% CI 0.72 to 3.53) reduction in peak rearfoot eversion during jogging (fig. 2).11 30 This finding is in line with the overall tendency for there to be a reduction in peak rearfoot eversion in four non-pooled comparisons during jogging11 30 31 and two of the three that studied walking.32

Forest plot of data pooling for rearfoot eversion and tibial internal rotation. Filled diamonds represent pooled data.
For posted moulded orthoses, pooled data from two studies5 33 of currently injured participants revealed a 1.95° (0.1 to 3.79) reduction in peak rearfoot eversion. This finding is in line with two of the three comparisons involving currently injured cohorts which reported moderate (non-significant, eg, CI contained 0) effects in favour of the orthoses.5 33
Of non-pooled data, only one comparison reported a statistically significant effect. A posted non-moulded orthosis produced a 2.3° (0.78 to 3.82) reduction of moderate effect (ES 0.92).30 One comparison evaluated the irregular surfaced orthosis (ES 0.28) and another made five comparisons of different material density, where authors did not provide enough information for point estimates of effect, showing small non-systematic effects (table 3).33 34
With regard to rearfoot eversion excursion, two comparisons examined the effect of inverted orthoses in cohorts with a history of injury. One study evaluated an inverted orthosis that was posted between 15° and 30° (often called a Blake orthosis),35 the other inverted the posting an additional 5° from neutral.36 In both studies, the individuals had been wearing their inverted orthoses for a minimum of 6 weeks. Pooled data revealed that the inverted orthoses had no effect (0.21° (−1.81 to 2.23)) on rearfoot eversion excursion. This finding contrasts that of MacLean et al,37 who examined a pragmatic prescription of their custom-moulded device (±posting) and qualitatively reported a significant but small (ES 0.32) reduction in rearfoot eversion excursion between 15% and 50% of stance. The lack of any substantial effect is in line with all other comparisons regardless of orthosis' design or injury status. Eng and Pierrynowski38 reported near-significant moderate reductions in the midstance phase of walking (ES 0.82) and contact phase of jogging (ES 0.73) in 10 adolescents with diagnosed patellofemoral pain syndrome.
Tibial internal rotation
There were 24 comparisons between orthoses and a control involving tibial internal rotation, four made during walking. Eighteen provided enough information to calculate point estimates of effect and confidence intervals (table 4). The majority of comparisons were based on different posting and moulding designs, one used an orthosis with irregular surface and five comparisons were made between a control and orthoses of different densities.
Three sets of pooling were possible. Pooling from two comparisons11 30 involving participants with no history of injury wearing posted non-moulded orthoses showed a decrease of 1.33° (0.13 to 2.53) in tibial internal rotation when jogging (fig. 2). Likewise, pooled data from two comparisons33 38 involving currently injured participants, also wearing posted non-moulded orthoses, found a reduction of 1.66° (0.2 to 3.13) in tibial internal rotation after touchdown during walking gait (fig. 2). Pooling of two comparisons involved cohorts with a history of injury who had worn their inverted posted moulded orthoses for a minimum of 6 weeks.35 36 Wearing the inverted orthoses did not change tibial rotation during jogging (2.22° (−0.83 to 5.26); fig. 2).
From data that were not pooled, Stacoff et al11 found a posted non-moulded orthosis, consisting of a medial post placed under the calcaneus added to a prefabricated orthosis, decreased tibial internal rotation by 1.59° (0.21 to 2.97) when jogging. Eng and Pierrynowski38 also observed a significant reduction during the touch-down phase of walking gait (1.9° (0.35 to 3.45) using a similar posted non-moulded device. These finding are of large (ES 1.43) and moderated effect (ES 1.07), respectively.
Five qualitative comparisons between orthoses of different densities and a control found that each of the 12 participants responded differently to different orthoses with a tendency towards a reduction in tibial rotation.34
Rearfoot eversion velocity
We found 19 comparisons over eight studies that examined the effects of orthoses on rearfoot eversion velocity (table 5).
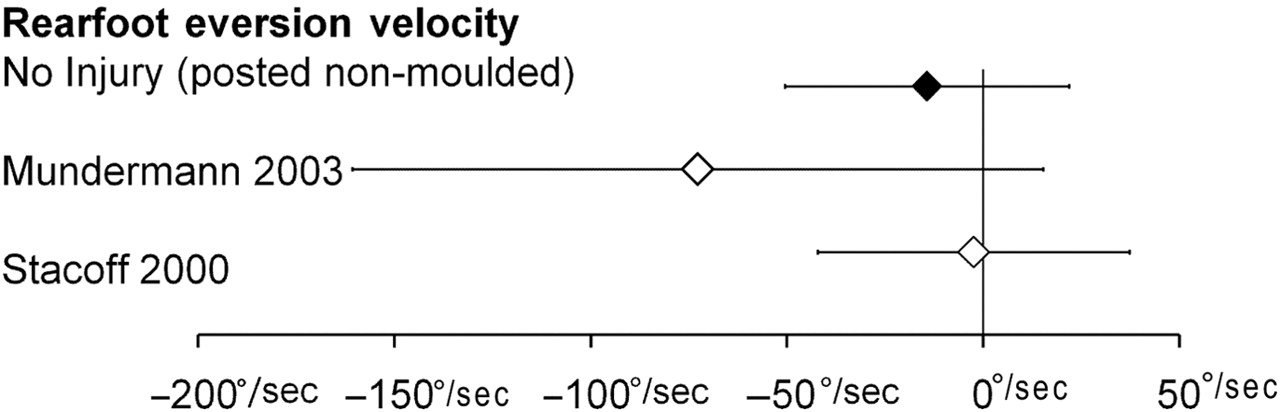
Two comparisons11 30 that examined the effect of posted non-moulded orthoses on healthy cohorts during jogging were pooled and showed that orthoses had no effect on rearfoot eversion velocity (−14.16°/s (−50.34 to 22.03); fig. 3). This finding is in line with data that were not pooled across all orthoses' designs,5 29 30 33 39 with the exception of two comparisons. MacLean et al37 reported that a posted moulded orthosis cast to calcaneal vertical produced a moderate (ES 0.95) reduction in velocity during the first 15% of stance phase. A later study reported a tendency for an inverted orthosis to increase velocity (38.66°/s (−22.44 to 99.76), ES 0.51) on initial use by individuals with a history of injury.36

{kind=link}
{kind=link}
{kind=link}
Forest plot of data pooling for rearfoot eversion velocity. Filled diamonds represent pooled data.
Maximum ankle inversion moment
We found 16 comparisons between orthoses and controls measuring maximum ankle inversion moment; in 10 of which, we could generate point estimates of effect and confidence intervals (table 6). No pooling was possible, and results were conflicting between studies where point estimates of effect could and could not be calculated.
Of the 10 comparisons where point estimates of effect could be calculated, only two significant effects were found. In a healthy cohort, a posted non-moulded orthosis significantly reduced maximum ankle inversion moment with moderate effect (6 Nm (1.28 to 10.72), ES 0.77) when jogging.30 However, no effect was found using an orthosis of similar design in a currently injured cohort.33 An inverted Blake orthosis35 had a moderate reducing effect on maximum ankle inversion moment by 0.14 Nm/kg/m (−0.25 to −0.03 (ES 1.06)).
Of the six comparisons where the point estimate of effects could not be calculated, MacLean et al37 and Stackhouse et al39 reported that their posted moulded orthoses produced a significant reduction in ankle inversion moment between 5% and 75% of stance phase and, on average, 24% throughout stance, respectively. Similarly, Nigg et al31 reported that orthoses with either a full length or half length medial post both significantly reduced inversion moment.
Maximum knee external rotation moment
Twelve comparisons were found, five of which provided enough data to calculate effect and confidence intervals, but pooling was not possible (table 6).30 36
Where point estimates of effect and confidence intervals were calculated, orthoses had no effect on maximum knee external rotation moment regardless of design.30 36 Six of the remaining comparisons supported these findings. In one comparison between an orthosis with a full-length 4.5-mm medial post and control, the authors reported increased maximum knee external rotation moment (27.6%) but did not provide enough data to enable the calculation of confidence intervals.31
Between-orthoses comparisons
Orthoses of differing designs (eg, Cobra, Blake inverted, biplanar, moulded, posted, irregular surface) have been compared. Data pooling was not possible because of the large variability in design features of the compared orthoses.
Rearfoot eversion
We found 11 comparisons investigating the effects of differing orthoses on peak eversion and four on rearfoot eversion excursion. The majority (seven) of comparisons were between orthoses of different posting and moulding designs. Other comparisons included an irregularly surfaced orthosis, two posted moulded orthoses (one custom-made and the other “mould-of-best-fit”) and different posting placement and amount.
With peak rearfoot eversion, a posted moulded orthosis was more effective than a posted non-moulded orthosis (3.3° (1.53 to 5.07), ES 1.83) and the irregular surface orthosis (2.4° (0.44 to 4.36), ES 1.2) in a currently injured cohort.33 In participants with no history of injury, the posted non-moulded orthosis was more effective (3.2° (1.28 to 5.12), ES 1.01).30
No orthosis design, degree or placement of posting seemed to be more effective in influencing excursion.
Tibial internal rotation
Of the eight between-orthosis comparisons (table 4), only one reported a moderate non-significant effect (ES 1.07). A reduction of 1.05° (−0.16 to 2.26) in tibial internal rotation occurred when a non-moulded orthosis with a medial post placed under the calcaneus was compared with a post placed under the medial arch.11 It would seem that no design feature is more effective at reducing tibial internal rotation.
Rearfoot eversion velocity
We found seven between-orthosis comparisons for rearfoot eversion velocity. Six involved different posting and moulding features20 30 32 and the other compared a posterior post with an anterior post (table 5).11
Jogging in a posted non-moulded orthosis was found to have a moderate effect over posted moulded orthoses (91.5°/s (7.98 to 175.02), ES 0.66) and non-posted moulded orthoses (ES 0.6) when participants had no history of injury.30 No other significant results were found.
Maximum ankle inversion moment
Of the seven between-orthoses comparisons for maximum ankle inversion moment, there were six between orthoses of different moulding and posting designs and another between a moulded-inverted orthosis to a moulded orthosis with a 4° post (table 6). The latter showed a small tendency for the inverted posted moulded orthosis to reduce maximum ankle inversion by 0.07 Nm/kg/m (−0.04 to 0.18) over the comparator (ES 0.58).35
Shock attenuation
The search strategy yielded 42 comparisons, from six studies on shock attenuation.30 36 40,–,43 Orthoses were compared on the basis of density (22), with or without rearfoot stabilisation, or variations of posting and moulding (20). The outcome measures consisted of tibial acceleration (3), loading rate (19), vertical impact force (16) and vertical ground reaction force (4) (table 7).
Shock attenuation paradigm comparisons when point estimates of effect and confidence intervals were able to be calculated
Tibial acceleration
Three comparisons involving two densities and a control showed no differential effects on tibial acceleration (ES 0.01–0.16).41
Loading rate
Comparisons were divided into those investigating density (11),32 40 43 and those investigating design (7).30 36 The former did not differentiate on loading rate,43 regardless of the presence of rearfoot stabilisation. When orthoses differed in design, non-posted moulded and posted moulded both had significant moderate effects over the control (ES 0.69 and 0.95, respectively) and a posted non-moulded orthosis (ES 0.76 and 1.01, respectively).30 These results were found in participants without injury. A reduction in loading rate brought about by a posted moulded orthosis was also reported in participants with a history of injury (−19.56 BW/s (−37.24 to −1.88)), but only after 6 weeks.36
Vertical impact force
We found three studies of vertical impact force with 16 comparisons of orthoses differing in density and design.30 36 43 Varying the material densities, irrespective of rearfoot stabilisation, had no effect on impact force. Large interparticipant variability was again found.43
In terms of design, a significant moderate attenuating effect was found in favour of a posted moulded orthosis compared with a posted non-moulded orthosis (167.1 N (15.72 to 318.48), ES 0.67) in uninjured participants.30 No difference existed between a posted moulded orthosis compared with control in a cohort with history of injury.36
Vertical ground reaction force
Miller et al42 reported that their posted moulded orthosis produced less vertical ground reaction force at 10% and 20% of the total stance phase. This effect was not apparent when a medially posted (10°) high-density EVA orthosis and a laterally posted (10°) high-density EVA orthosis was compared with control.40 Insufficient information was presented to calculate point estimates of effect.
Neuromotor control
Eight comparisons were found fitting the inclusion criteria. Orthoses were of different designs, including an irregularly surfaced orthosis, and were compared with a control condition. Of these comparisons, two studies (two comparisons) provided enough information to calculate point estimates of effect and their confidence intervals (table 8).44 45 The main outcome measure was the amplitude of EMG signal of several muscles of the shank (tibialis anterior (TA), peroneus longus (PL), medial gastrocnemius (MG), lateral gastrocnemius, soleus (Sol), tibialis posterior (TP)) and the thigh (vastus lateralis, vastus medialis, rectus femoris, biceps femoris (BF)). Tomaro and Burdett45 also measured the duration of TA EMG signal.
Neuromotor control paradigm comparisons where point estimates of effect and confidence intervals were able to be calculated
Shank muscles
Five comparisons were made for each TA, PL and MG. Jogging in a posted moulded orthosis produced significant increases in TA and PL amplitudes and a significant decrease in the amplitude of MG for uninjured participants.46 For these participants, posted non-moulded and non-posted moulded orthoses were reported to increase both PL and MG in different phases of gait and EMG bandwidths.46 Walking in a moulded orthosis posted to 15° produced an increase of 19% maximum voluntary contraction (MVC) in PL for participants with no injury.47 For participants with current injury, a posted moulded orthosis also significantly increased TA amplitude (37% of MVC (5.44 to 68.56), ES 0.67).44 Walking studies found no effect on MG. Tomaro and Burdett45 studied individuals with a history of injury who had worn, for a minimum of 6 months, posted moulded orthoses. They reported no difference between the orthoses and control in TA and PL amplitude as well as no change in TA duration (2.6% (−2.89 to 8.09), ES 0.41).
Comparisons were also made for Sol and TP. No change in Sol amplitude was reported when participants with no history of injury walked in moulded orthoses posted to 15° compared with walking in a control.47 Similarly, no systematic results were found in TP amplitude in currently injured individuals walking in posted non-moulded, posted moulded and irregular surface orthoses.33
Thigh muscles
Four comparisons were made for the quadriceps and BF. When participants with no history of injury jogged in posted moulded orthoses, all four muscles significantly increased in amplitude during various phases of gait and across different EMG bandwidths. Similar increases were also present in BF when participants wore either posted non-moulded and non-posted moulded orthoses.46 These findings are in discordance with a study of currently injured individuals wearing posted moulded orthoses. BF amplitude significantly and moderately (ES 0.68) reduced by 11.1% of MVC (1.89 to 20.31) throughout stance, and there was no change in the activity of vastus medialis or vastus lateralis.44
Discussion
Research has primarily focused on the kinematic paradigm and least on neuromotor control. To the extent that synthesis was possible, data pooling revealed that posted orthoses that were not moulded reduced peak rearfoot eversion and tibial internal rotation in non-injured, whereas moulded orthoses with or without posting produced large reductions in loading rate and vertical impact force.
Data pooling of the kinematic paradigm showed a relatively small effect (∼2°) in reducing rearfoot eversion and tibial internal rotation using skin markers to record motion, which may well be an overestimate of actual bone motion.48 It is currently unknown whether this small motion reduction is clinically beneficial, although Nawoczenski et al6 posited that such small changes may be clinically relevant in injured runners because of the potential for cumulative effects from the high volume of repetitive/cyclical motion. More importantly, individual studies showed large confidence intervals, which indicates that practitioners should tailor their approach to each individual's clinical presentation and apply sound clinical reasoning skills when considering this pooled data.
An interesting and unexpected outcome of shock attenuation data was that altering material density had no systematic effect on tibial acceleration, loading rate or vertical impact force,41 43 whereas orthosis' moulding reduced loading rate30 36 and may favourably affect vertical impact and ground reaction forces.30 36 42
Only two neuromotor control studies reported data sufficient to derive point estimates of effect, but pooling was not possible (cohorts too dissimilar). Orthoses seem to increase TA and PL activity, variably influence MG activation levels depending on speed of gait and differentially change MG and thigh muscles contingent on injury status.44 46 47 Further study is urgently needed in this paradigm.
The methodological quality assessment of the studies in this review identified the main issue as being the non-specific categorisation of injury type. Studies investigating cohorts with past and current injuries included a range of lower limb injuries, thereby making it difficult to apply pooled results to a specific injury in practice.
We only reviewed studies using three-dimensional motion analysis (excluding two-dimensional) because we believe that doing so ensured the most accurate representation of motion. A limitation of this approach is that we may have overlooked meaningful data, though it would seem that this is not the case.25 26 49 We also only pooled data from studies using similar orthoses. It must be acknowledged that not all orthoses are exactly the same, so that our pooled point estimates of effect may be underestimates. However, this should be counterbalanced by the increased precision gained by pooling data from a number of studies. Using similar orthoses for pooling strengthens the findings for specific commonly used features of orthoses, such as posting and moulding.
Summary
The major conclusion of this review is that there is a large amount of variability with regard to how patients respond to orthoses. Meta-analysis showed that an orthosis that is posted without any customisation (or individual moulding) produces greater motion control at the rearfoot and tibia than a control. Orthoses that have been individually contoured are more effective at attenuating loading rate and vertical impact force than if only posted. The majority of the evidence base has been derived from individuals with no history of injury but are likely still useful as rudimentary clinical guides for sports medicine practitioners. Future research needs to focus on neuromotor control effects, especially in those with injury.
Acknowledgments
K. Mills and Dr AR Chapman are supported by the Australian Research Council. Financial support for this research was received from the Australian Research Council (Australian Research Council Linkage Project Grant LP0668233).
References
Footnotes
-
Funding Australian Research Council, Linkage Project Grant LP0668233, first Floor, 8, Brindabella Circuit, Brindabella Business Park, Canberra Airport Act 2609, Australia.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.