Article Text

Abstract
Background Anterior cruciate ligament (ACL) ruptures are among the most severe musculoskeletal soft tissue injuries. However, the exact mechanisms which cause these acute injuries are unknown. Recently, sequence variants within two genes, namely COL1A1 and COL5A1, which code for the α1 chains of types I and V collagen respectively, were shown to be associated with ACL ruptures. Type XII collagen, similarly to types I and V collagen, is a structural component of the ligament fibril and is encoded by a single gene, COL12A1.
Objective The aim of this study was to investigate whether sequence variants within COL12A1 are associated with ACL ruptures.
Methods One hundred and twenty-nine (38 female) participants with clinically and surgically diagnosed ACL ruptures, as well as 216 (83 female) physically active controls participants (CON) without any history of ACL injury were included in this case-control genetic association study. All participants were genotyped for the AluI and BsrI restriction fragment length polymorphisms (RFLPs) within COL12A1.
Results The AA genotype of the COL12A1 AluI RFLP was significantly over-represented in the female (OR=2.4, 95% CI 1.0 to 5.5, p=0.048), but not male (p=0.359) ACL participants. There were no genotype differences between the ACL and CON group for the BsrI RFLP.
Conclusion The COL12A1 AluI RFLP is associated with ACL ruptures among female participants in this study. The results suggest that females with an AA genotype are at increased risk of ACL ruptures. These initial genetic association studies should be explored further and, if repeated, incorporated into multifactorial models developed to identify predisposed individuals.
Statistics from Altmetric.com
Introduction
It has been estimated that the incidence of anterior cruciate ligament (ACL) ruptures are approximately 35 ACL ruptures per 100 000 citizen years within the general population.1 2 Although relatively low, the majority of ACL ruptures occur in young athletes, with young female athletes at greater risk than their male counterparts.3 4 An ACL rupture is not only one of the most severe injuries sustained in sports,5 but also places the individual at up to 105 times greater risk of osteoarthritis.6 A significantly increased risk of ACL ruptures has been shown to be associated with regular participation in sport, particularly among sports requiring change in direction and rapid deceleration during cutting, pivoting and landing.7 8 Around 70% of ACL ruptures occur as a result of a non-contact mechanism,9 which is defined by the American Orthopaedic Society for Sports Medicine as “Forces applied to the knee at the time of injury resulted from the athlete's own movements and did not involve contact with another athlete or object”.3
Although the exact aetiology of ACL ruptures are poorly understood, various intrinsic and extrinsic risk factors have been identified.4 Recent evidence suggests that a familial predisposition,10 and specific genetic sequence variants,11,–,13 should also be included as intrinsic risk factors for ACL ruptures. Two independent studies have shown that the rare TT genotype of the COL1A1 Sp1 binding site polymorphism is under-represented in participants with shoulder dissociations and/or cruciate ligament ruptures.11 12 A third study has suggested that this rare COL1A1 genotype is also under-represented in participants with Achilles tendon ruptures,14 suggesting that this COL1A1 genotype is a common risk factor for all acute soft tissue ruptures.15
In addition, the COL5A1 BstUI restriction fragment length polymorphism (RFLP) has also been shown to be associated with ACL ruptures in females.13 The COL1A1 and COL5A1 genes encode the α1 chains of types I and type V collagen, respectively. Types I and V collagen, together with the fibrillar type III collagen, form heterotypic collagen fibrils, the basic functional unit of ligaments.16 Unlike the fibrillar collagens, types XII and XIV collagen are associated with the surface of the collagen fibril and are members of the Fibril Associated Collagens with Interrupted Triple helices (FACITs) subfamily.17 Type XII collagen is a homotrimer consisting of 3 α1(XII) chains and is encoded by a single gene, COL12A1, mapped to chromosome 6q12–q13.18 Similar to type V collagen, type XII collagen is believed to regulate fibril diameter (fibrillogenesis).19,–,21
Previous research from this laboratory has investigated the association of the COL12A1 AluI and BsrI RFLPs with Achilles tendon injuries. It was interesting to note that, although not significant, both the rare CC and GG genotypes of the COL12A1 BsrI and AluI RFLPs respectively, were absent in participants with Achilles tendon ruptures. Since tendons and ligaments have a similar hierarchical structure,22 and as mentioned, previous work has suggested that there might be common genetic risk factors for acute soft tissue ruptures,15 the COL12A1 gene is therefore an ideal candidate gene as a possible additional genetic risk factor for ACL ruptures.
The aim of this study was therefore to determine if the previously described23 COL12A1 AluI and BsrI RFLPs are associated with ACL ruptures. A further aim of this study was to determine if there was any gender-specific associations between the two selected COL12A1 gene variants and increased risk of ACL ruptures.
Materials and methods
Participants
One hundred and twenty-nine (38 females and 91 males) Caucasian participants with surgically diagnosed ACL ruptures were recruited for this study from the Sports Science Orthopedic and Sports Medicine Clinics in Cape Town, South Africa, as previously described.12 13 In addition, 216 (83 females and 133 males) apparently healthy, unrelated, physically active Caucasian participants, without any self-reported history of ACL injury, were recruited as control (CON) participants from sports and recreational clubs within the greater Cape Town area of South Africa as previously described.13 The controls participated in similar sports as the ACL group.
In addition, each participant completed personal details, medical history, personal and blood relative (family) ligament and tendon injury history, as well as a sports participation questionnaire. Sports participation was categorised into contact sports, non-contact jumping sports, non-contact non-jumping sports, as previously defined,10 with slight modification.13
This study was approved by the Research Ethics Committee of the Faculty of Health Sciences within the University of Cape Town, South Africa (reference number 164/2006).
DNA extraction and COL12A1 genotyping
Approximately 4.5 ml of venous blood was obtained from each participant by venipuncture of a forearm vein and collected into an EDTA vacutainer tube. Blood samples were stored at 4°C until total DNA extraction. DNA was extracted using the procedure described by Lahiri and Nurnberger24 and modified by Mokone et al.25 Two previously characterised non-synonymous single nucleotide polymorphisms (SNPs), located within exons 29 (rs240736, T1738I) and 65 (rs970547, S3058G) of COL12A1 were selected for investigation.23 Both SNPs are located within the region of the COL12A1 gene which encodes the short XIIB-1 isoform predominantly expressed in tendons and ligament (Supplementary figure 1).26
Primer pairs were designed to amplify the DNA fragments containing each of the two selected SNPs as previously described.23 PCR amplification of these fragments was performed in 60 μl volumes containing approximately 200 ng genomic DNA; 20 pmol of each primer; 2.0mM MgCl2; 50mM KCl; 10mM Tris-HCl (pH 8.3); 200μM dATP, dCTP, dGTP, and dTTP and 0.5 U Taq DNA polymerase (New England Biolabs, Ipswich, Massachusetts, USA). Amplifications were conducted by denaturing for 1 cycle at 94ºC for 3 min, followed by 30 cycles at 94ºC for 30 s, 55ºC for 30 s, and 72ºC for 1 min, followed by a final extension of 1 cycle at 72ºC for 5 min on a thermal cycler (Hybaid; PCR Express, Middlesex, UK).
The 673 bp fragment (containing SNP rs240736 or the BsrI RFLP) generated from primer pairs COL12-2F 5′-GAG CTC ATG ACA TGC ATC AG-3′ and COL12-2R 5′-GTC TTG GAC TTC TCA GCC TC-3′ was digested with restriction endonuclease BsrI to produce 57 bp, 616 bp sized fragments for the T allele and 57 bp, 366 bp, 250 bp sized fragments for the C allele. The 615 bp fragment (containing SNP rs970547 or the AluI RFLP) generated from primer pairs COL12-1F 5′-GAG AAT CCA GAA CAG C–TC CAC CAG-3′ and COL12-1R 5′-CAT GGC TAG TAT GGG ACA G-3′ was digested with restriction endonuclease AluI to produce 16 bp, 599 bp sized fragments for the G allele and 16 bp, 139 bp, 460 bp sized fragments for the A allele. The COL12-1F primer was designed to contain a mutated nucleotide (underlined in the primer sequence) which introduces and additional restriction recognition site (AG/CT) for the AluI restriction endonuclease. The resultant fragments were separated, together with a 100 bp DNA ladder of known size markers (Promega Corporation, Madison, Wisconsin, USA) and SYBER® Gold nucleic acid gel stain (Invitrogen Molecular Probes, Oregon, USA), on 6% non-denaturing polyacrylamide gels. The gels were photographed under UV light using a Uvitec photodocumentation system (Uvitec Limited, Cambridge, UK) and genotypes were determined based on the sizes of the DNA fragments.
Statistical analysis
Data were analysed using STATISTICA Version 8.0 (Statsoft Inc, Tulsa, Oklahoma, USA) and Graphpad InStat Version 3 (Graphpad Software, San Diego, California, USA) statistical programs. A one-way analysis of variance was used to determine any significant differences between the characteristics of the ACL and CON group. A χ2 analysis or Fisher's exact test was used to analyse any differences in the genotype and allele frequencies, as well as other categorical data between the groups. Significance was accepted when p<0.05. Hardy–Weinberg equilibrium was established using the program Genepop web version 3.4 (http://genepop.curtin.edu.au/).
Results
Participant characteristics
The female and male CON and ACL groups were matched for age, height and country of birth (table 1). In addition, the female CON and ACL groups were also matched for weight and BMI. The male participants within the ACL group were significantly heavier, with a significantly higher BMI when compared to the CON group (table 1). The exact mechanism of injury could only be identified in 21 female (55.7%) and 67 male (73.6%) participants. The general characteristics of the 36 (53.7%) male and 18 (85.7%) female participants who had ruptured their ACL via a non-contact mechanism were similar to the ACL group and was previously reported.13
Characteristics of the female and male participants within the asymptomatic control (CON) group and the anterior cruciate ligament ruptures (ACL) groups
The relative frequency of the self-reported history of any other (excluding ACL) ligament and other knee ligament injuries were significantly higher in the female ACL group when compared to the female CON group (p=0.004 and p=0.029, respectively) (table 2). Among the male participants the frequency of other knee ligament injuries was significantly higher (p=0.045) in the ACL group when compared to the CON group. The other knee ligament injuries included injury to either the posterior cruciate ligament (PCL), the lateral collateral ligament (LCL) or the medial collateral ligament (MCL). Furthermore, a family history of any ligament injury at the time of recruitment was significantly higher (p=0.003) in the female ACL group when compared to the female CON group.
Self-reported personal and family (blood relative) history of soft tissue injuries within the asymptomatic control (CON) and the anterior cruciate ligament ruptures (ACL) groups in the female and male participants
Sports participation
The relative frequency of participation in non-contact jumping sports was greater (p=0.035) in the female ACL group, when compared to the female CON group. Among the male participants, the relative frequency of participation in contact sports were higher (p=0.001) in the ACL group, when compared to the CON group (table 3). In addition, significantly more males had participated in contact sports for a significantly greater number of years (p<0.001). A significantly greater relative number of females had also participated in non-contact jumping sports (p<0.001) in this study.
Sports participation according to type of sport within the asymptomatic control (CON) and the anterior cruciate ligament ruptures (ACL) groups for all female and male participants
COL12A1 genotype and allele frequencies
The AluI RFLP
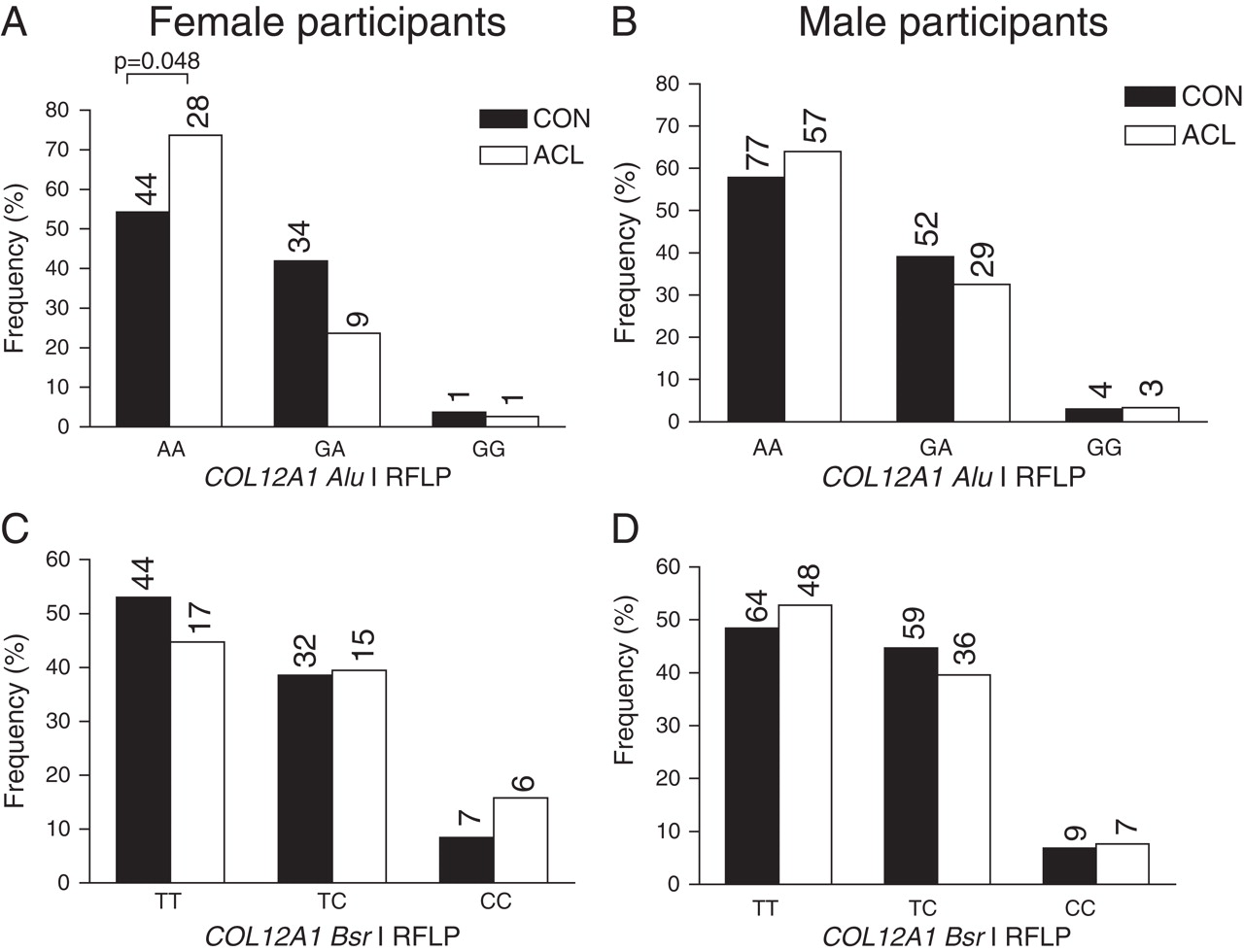
When the female and male participants were analysed together, there were no significant differences in genotype or allele frequencies between the CON and ACL groups (genotype, p=0.067; allele, p=0.122). However, when the female participants were analysed separately, the AluI RFLP AA genotype was significantly over-represented (AA vs GT + GG; OR 2.4; 95% CI 1.0 to 5.5; p=0.048) in the ACL group when compared to the CON group (figure 1A). The AluI RFLP was not associated with ACL ruptures when only the males were analysed (AA vs GT + GG; p=0.359) (figure 1B). All groups were in Hardy–Weinberg equilibrium for the AluI RFLP (data not shown).

The relative genotype frequency of the COL12A1 gene AluI and BsrI restriction fragment length polymorphisms (RFLP) within the asymptomatic control (CON; black bars) groups, the anterior cruciate ligament rupture groups (ACL; white bars) in all female (A and C) and male (B and D) participants. The number of participants (n) within each group is shown in parentheses. Because of the small sample size of the AluI RFLP GG genotype (A and B), the AA genotype was compared to the combined GA and GG genotypes. (A) The AluI RFLP genotype distributions within the female participants. CON versus ACL, p=0.044 (AA vs GA + GG). (B) The AluI RFLP genotype distributions within the male participants. CON versus ACL, p=0.359 (AA vs GA + GG). (C) The BsrI RFLP genotype distributions within the female participants. CON versus ACL, p=0.433. (D) The BsrI RFLP genotype distributions within the male participants; CON versus ACL, p=0.746.
Although the sample size was small, the genotype distribution of the COL12A1 AluI RFLP was similar for both the female participants who had ruptured their ACL via a non-contact mechanism (n=18, 72.2% AA, 22.2% GA, 5.5% GG) and the female ACL group.
The BsrI RFLP
When the female and male participants were analysed together, there were no significant differences in genotype or allele frequencies between the CON and ACL groups (genotype, p=0.665; allele, p=0.730) for the BsrI RFLP (data not shown). There were also no significant differences in the COL12A1 BsrI RFLP genotype (figure 1C, 1D) or allele (female, p=0.230; male, p=0.749) frequency distributions between the female or male CON and ACL groups. All groups were in Hardy–Weinberg equilibrium for the BsrI RFLP (data not shown).
AluI RFLP genotype effects on family history of ligament injury
An additional analysis of this study divided all participants into two separate groups; participants who had self-reported a family history of any ligament injury, and those whom had self-reported no family history of any ligament injury. An interesting finding of this additional analysis was that there was an observed trend for the AA genotype to be over-represented (AA vs GA + GG; p=0.082) in female participants with a family history of ligament injury (figure 2A). There was however no significant differences among the male participants (figure 2B).

{kind=link}
{kind=link}
The relative genotype frequency of the COL12A1 gene AluI restriction fragment length polymorphism (RFLP) when all female (A) and male (B) participants in the study were divided into those with and without a family history of ligament injuries. (A) The AluI RFLP genotype distribution within the female participants; AA versus GA + CC, p=0.082; (B) The AluI RFLP genotype distribution within the male participants; p=0.854.
Discussion
The main finding of this study was that the AA genotype of the AluI RFLP within the terminal exon 65 of the COL12A1 gene was associated with a 2.4 times increased risk (OR=2.4; 95% CI 1.0 to 5.5; p=0.048) of ACL ruptures in female, but not male participants. The upstream BsrI RFLP, within exon 29, was however not associated with ACL ruptures in neither the female nor the male participants. The finding of an increased family history of ligament injury among participants in the ACL group investigated in this study was previously reported.13 An additional finding of this study was that there was a trend (AA vs GA + GG; p=0.082) for the AA genotype of the AluI RFLP to be over-represented in female participants with a family history of any ligament injury.
The main finding, that females with an AA genotype for the COL12A1 AluI RFLP had an increased risk of ACL ruptures, has not been previously reported. The COL12A1 gene encodes the α1 chains of the various long (XIIA) and short (XIIB) homotrimeric isoforms of type XII collagen.26 The short XIIB-1 isoform is predominantly expressed in both tendons and ligaments in response to mechanical loading.26 The AluI RFLP within exon 65, is a non-synonymous coding variant, which changes the amino acid at position 3058 from a serine to a glycine. Although the wild-type serine amino acid is a neutral polar amino acid with a larger side chain than the substitute non-polar neutral glycine amino acid, this change in amino acid sequence has no known functional consequence. The findings from this study do however suggest that the A>G substitution of this variant possibly results in an altered type XII collagen protein and although speculative, this may alter the biomechanical properties of the collagen fibril. Further research is therefore required to test this hypothesis.
A previous study from our laboratory investigated the COL12A1 AluI and BsrI RFLPs within participants with Achilles tendon injuries. In this study the CC genotype of the COL12A1 RFLP and the GG genotype of the BsrI RFLP were not identified in participants with Achilles tendon ruptures. In the current study, the AA genotype was over-represented in female participants with ACL ruptures. These findings collectively suggest that the COL12A1 gene might have a broader function in the development of acute soft tissue injuries, and therefore this gene needs to be further investigated.
The BsrI RFLP of type XII collagen, which involves the amino acid substitution at position 1738 from isoleucine to threonine, was however not associated with ACL ruptures in male or female participants. Furthermore, the AluI and BsrI RFLPs were previously shown not to be in linkage disequilibrium.23 The genotype frequencies of the AluI and BsrI RFLPs within the control participants in the current study are similar to previously reported values.23
The main finding of this study is in agreement with the previously published finding from our laboratory which noted the association between the CC genotype of the COL5A1 BstUI RFLP and ACL ruptures among the female, but not the male participants.13 As previously discussed,13 the reasons for these gender-specific associations are currently unknown. Specific to the gender association of the COL12A1 AluI RFLP and ACL ruptures, there are no known previous reports of the effects of the female sex hormones on the regulation of COL12A1 or any gene–gene interactions which could explain this observation. Both genes encode for quantitatively minor structural components of the collagen fibril, the major building block of the ligament.16 27
It has been widely reported that females are at increased risk of ACL ruptures when compared to males.28 A number of intrinsic risk factors classified as either anatomical, hormonal, or neuromuscular, have been linked to this observed phenomenon.29 30 The gender-specific association found in this study, as well as the previously published COL5A1 study,13 may indicate that genetic variants alter structure and/or biomechanical properties of the ACL which may compromise this ligament. Therefore, it remains possible that even though the biomechanical properties of the ACL were influenced by the AluI RFLP in male and females participants, it did not alter the risk of ACL ruptures in the male participants significantly enough to demonstrate an association in this study. For this reason, a larger group of homogenous male participants with non-contact ACL ruptures and exposure matched controls are required for further investigation.
The additional finding of this study, that there was a trend for the AA genotype of the AluI RFLP to be over-represented in female participants with a family history of ligament injury, provides support that this gene variant may alter the mechanical properties of ligaments. It is however unknown why this trend was only observed among the female participants.
The respective female and male control and ACL ruptures groups in this study were not similarly matched for participation in physical activity. Briefly, the female participants in the ACL group had participated in non-contact jumping sports for a significantly longer period of time while the male participants had participated in contact sports for a significantly longer period of time. Furthermore, the BMI of the male ACL group and NON subgroup were both significantly higher than the CON group. These differences in non-genetic factors between the control and ACL ruptures groups may be possible confounding variables in determining injury risk, and are thus limitations to the current study. A further limitation of this study was the small sample size of the female participants. The primary aim of this study was not designed to investigate gender-specific genetic risk factors and therefore further research is required to confirm this finding in a larger group of female participants.
What is already known on this topic
▶ ACL ruptures are multifactorial disorders that are associated with various extrinsic and intrinsic (including genetics) risk factors.
▶ Recently, genetic sequence variants within the COL1A1 gene and the COL5A1 gene have been shown to be associated with risk of ACL ruptures.
What this study adds
▶ The AA genotype of the COL12A1 AluI RFLP was associated with risk of ACL ruptures in female participants.
▶ Combining the results from this study, and the previous study reporting the association of the COL5A1 gene, provides an additional estimate of risk for ACL ruptures in females.
In conclusion, the AA genotype of the AluI RFLP within exon 65 of the COL12A1 gene is associated with an increased risk of ACL ruptures among female participants in this study.
Acknowledgments
This study was supported in part by funds from the National Research Foundation (NRF) of South Africa (grant nos FA2005021700015 and FA2007032700010), University of Cape Town and the South African Medical Research Council (MRC). AVS was supported by the postdoctoral innovation award from the NRF.
References
Footnotes
-
Competing interests None.
-
Ethics approval This study was conducted with the approval of the Research Ethic Committee of the Faculty of Health Sciences, University of Cape Town.
-
Patient consent Obtained.