Article Text

Abstract
Background There are many possible predisposing factors for Achilles tendon disorders suggested in the literature but their pathogenetic relevance is not proven in most cases. The asymmetric mechanical load distribution within the Achilles tendon during locomotion is frequently addressed as a major risk factor for Achilles tendon disorders. The spatial orientation of the subtalar joint axis (STA) may influence the Achilles tendon loading possibly leading to overload injuries.
Hypothesis There is a significant difference between the orientation of the STA in subjects with and without Achilles tendon pathologies.
Materials and methods 614 subtalar joint axes determined in 307 long-distance runners with and without Achilles tendon disorders were included. Achilles tendon disorders were defined as any Achilles tendon–related pain during or following running, existing for more than 2 weeks in the past. Motion analysis of the foot was performed using an ultrasonic pulse-echo-based measurement system. The orientation of the STA was expressed by two angles.
Results The mean inclination angle was 42±16° and the mean deviation angle was 11±23°. There was a significant difference (p=0.002) between the mean deviation angle measured in subjects with Achilles tendon pathologies (18±23°) and those without (10±23°).
Conclusions The results demonstrate a wide interindividual variability of the spatial orientation of the STA. In addition, the mean deviation angle in people with Achilles tendon pathologies is significantly more oblique than in people without. This finding indicates that the spatial orientation of the STA is related to the incidence of overuse injuries of the Achilles tendon in the investigated sample.
Statistics from Altmetric.com
Introduction
Achilles tendon pathologies are of major importance in sports. Five to eighteen per cent of long-distance runners were affected.1,–,3 Foot anatomy,4 poor vascularity,5 training errors,6 age, bodyweight,7 or ankle kinematics8 are discussed in the literature as intrinsic risk factors for Achilles tendon pathologies but their pathogenetic relevance is not proven.7 However, the mechanical loading of the Achilles tendon during locomotion is likely a main pathologic agent.6 9 10
The subtalar joint axis (STA) runs from anterodorsomedial to posteroplantarlateral through the foot and is proposed to be a constant anatomical factor primarily resulting from the bony structures constituting the subtalar joint.11 In the literature, there is a great interindividual variability of the STA's orientation noticed.11,–,13 This means that in some cases, the STA passes through the Achilles tendon while in other cases it runs outside the Achilles tendon (figure 6). In principle, the Achilles tendon antagonises the pronation movement at heel strike and in the initial stance phase. During toe-off, the Achilles tendon is the main plantar flexor and additionally inverts the rear foot.10 It can be assumed that the stress in the Achilles tendon is connected to the orientation of the STA.9 It is conceivable that a specific orientation of the STA causes asymmetrical tensile loads in the Achilles tendon, which can be regarded as a reason for Achilles tendon pathologies.7 14 15 The variation of the distance between specific Achilles tendon fibre insertions and the subtalar axis likely results in different torques acting on these fibres during locomotion. The crucial problem is to locate the STA.
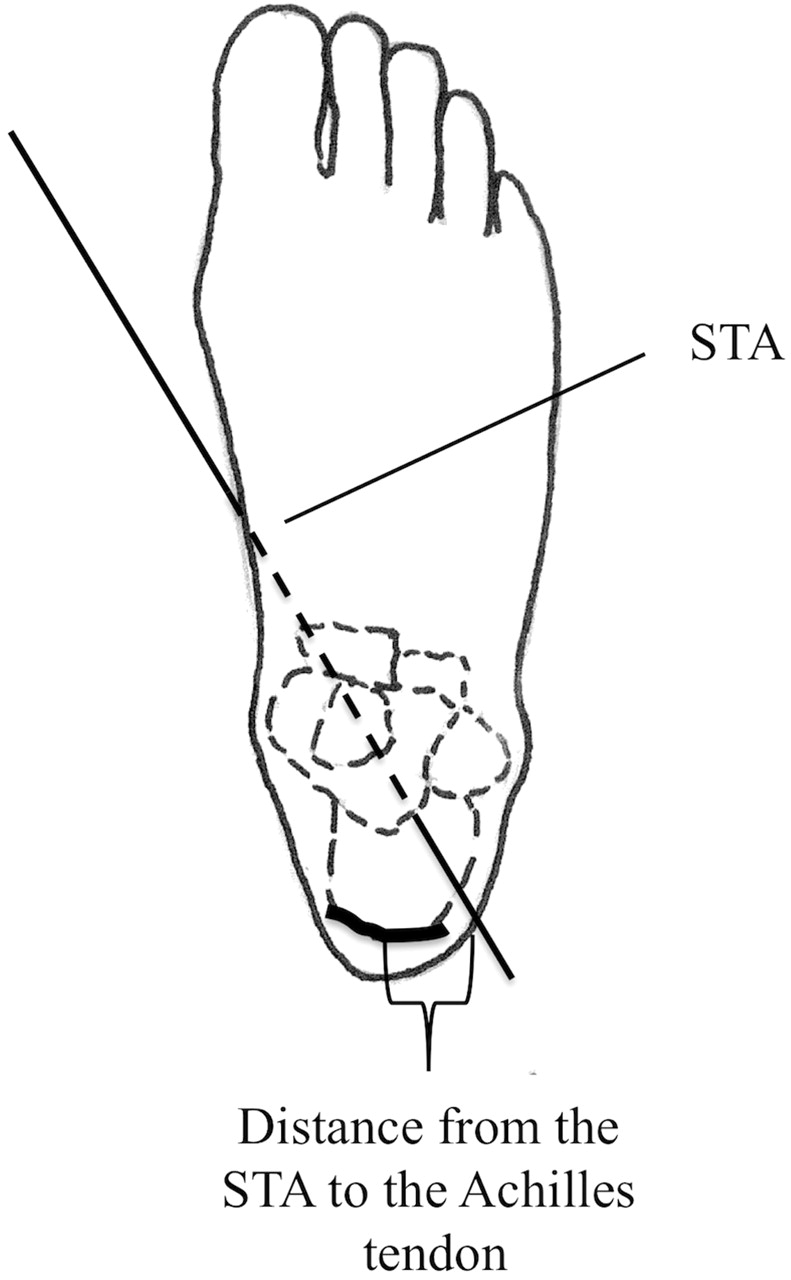
Right angle with the subtalar joint axis (STA) viewed from above demonstrating the distance between the Achilles tendon and the penetration point of the STA through the skin.
In the literature, the STA is discussed to be associated with acute or chronic overuse injuries.16 17 However, because of methodical limitations and the small number of subjects, previous studies do not satisfactorily shed light on the dependence between the STA orientation and overuse injuries. Most methods previously used to analyse the spatial orientation of the STA are restricted to in vitro11 18 or invasive application.19 20 MRI-based methods and techniques in vivo are expensive and time consuming.20 21 The in vitro measurement technique described by Isman et al11 determines the STA on the basis of the shape of articulating surfaces. Ligaments, tendons and the capsule of the joint are disregarded in this case. A capable method has to be suitable for field application and has to allow inexpensive, in vivo, non-invasive measurements. To meet these recommendations, an ultrasonic pulse-echo–based measurement system was developed to determine the spatial orientation of the STA. Specific software and mathematical methods have been developed for this device. According to existing in vivo procedures for the determination of the ankle axis, this method is based on motion analysis of the subtalar joint.21,–,23 The method allows to capture a great number of subjects in vivo, non-invasively, in real time and on the field.
The purpose of this study was to assess the spatial orientation of the STA in a large cohort of runners. The relation between chronic Achilles tendon problems and the spatial orientation of the STA was retrospectively analysed.
Materials and methods
Subjects
The study was approved by the ethics committee of the Medical Department, University of Tübingen, Germany.
Power analysis has been done by calculating (GPower Version 3.0.5) sample size of two independent groups (two-tailed question) using an estimated medium effect size, d, of 0.4, α-error probability of 0.05 and power of 0.80. Therefore, a minimum size of 100 subjects in each group has been calculated.
In this study, 495 mainly long-distance runners with a running performance of at least 25 km per week and a running history of at least 3 years were included. An acute injury of the lower limb during the last year or a reduced range of motion in the subtalar joint was a criterion for exclusion. One hundred and eighty-eight subjects had to be excluded due to the disability of these subjects to reproducibly move their ankle and subtalar joint. Three hundred and seven subjects were included. Anthropometric data, information about previous injuries and running performance were collected by using a questionnaire (table 1). We focused on Achilles tendon pathologies by asking the question: ‘Did you have any Achilles tendon–related pain during or following running existing over more than two weeks in the past?’ A specific physical examination was not performed. Therefore, the terms Achilles tendon disorder or Achilles tendon pathology include different lesions like Achilles tendinitis, paratenonitis, paratenonitis with tendinitis, insertional tendinitis and retrocalcaneal bursitis.24
Anthropometric data from 307 subjects with average and effect size for the significant data pairs
STA determination
The STA of the right and the left foot of all 307 included subjects were measured in vivo, non-invasively and in real time. For this, an ultrasonic pulse-echo–based measurement system was used (Isny Germany; Zebris technology). This measurement system is based on motion analysis of the rear foot in relation to the tibia. The mathematical procedure used regards the movement of the subtalar joint as pure rotation.11 20 22 Thus, the mathematical analysis can be reduced to two dimensions of freedom problem. For the computation of the finite ankle joint axis and the centre of rotation, the mathematical method needs at least three coordinates from an ultrasonic marker. Two ultrasonic markers are indirectly fixed at the rear foot with a modified shoe (figure 2A).

(A) Ultrasonic pointer pointing at the Achilles tendon. (B) Ultrasonic pointer pointing to one point at the tibia border.
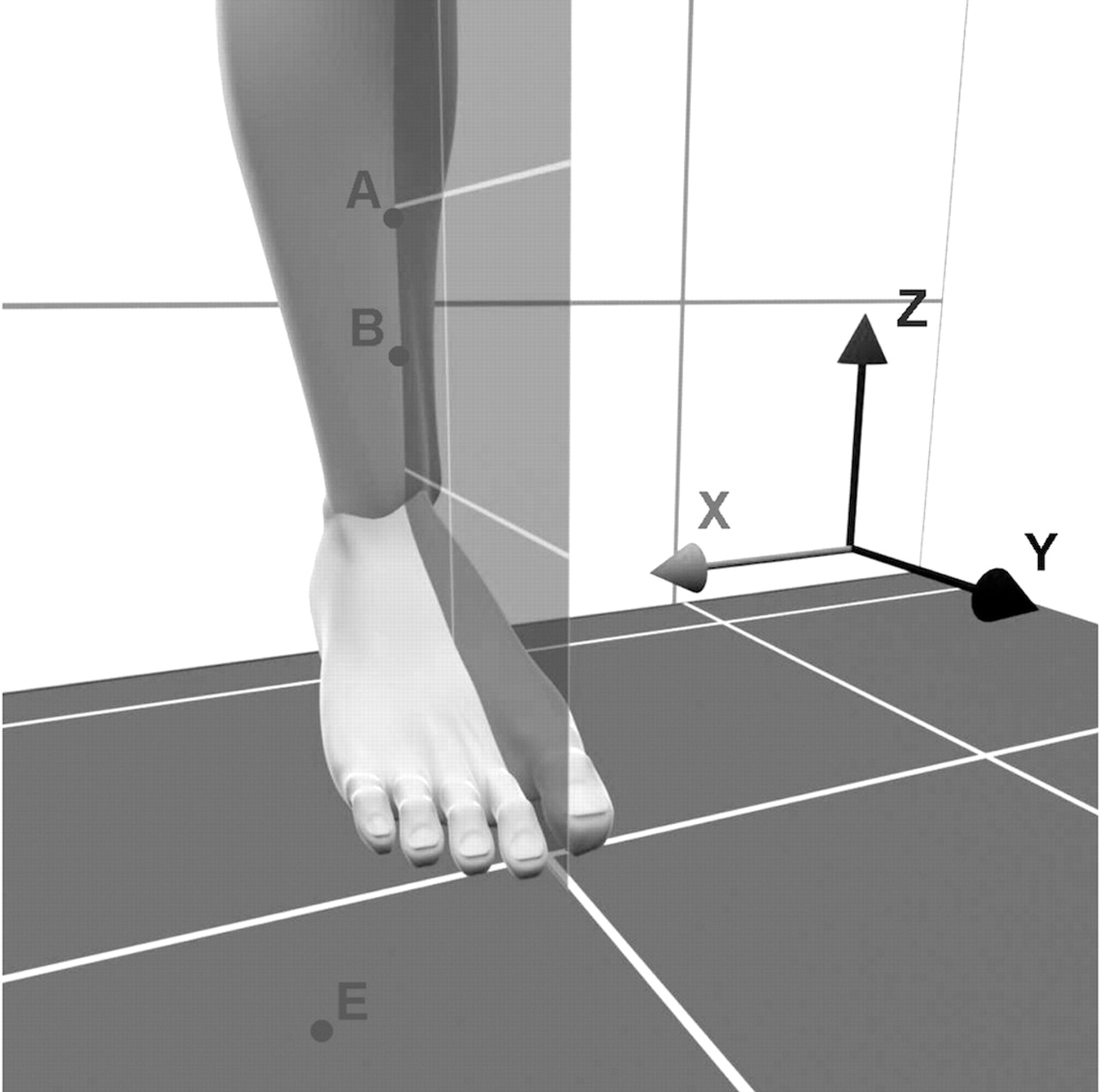
This construction enables to record rear foot motion. The ultrasonic waves emitted by the ultrasonic markers are received with an ultrasonic receiver fixed to the tibia. Before each measurement, a so called tibia-coordinate-system has to be determined. So all measured motions have been calculated relatively to this coordinate system. A custom-built ultrasonic pointer was used to record prominent anatomic landmarks (figures 2 and 3). To compute the tibia coordinates, two points on the anterior tibial border (A and B) and an additional point in the middle of the Achilles tendon (C) have to be detected. A fourth point at the ground (E) helps to define the origin of the tibia-coordinate-system (figure 1). All points have to be recorded with the subject standing upright in a neutral body position with the feet positioned hip width. From the two points, A and B, at the tibia it is possible to calculate the z-axis of the tibia-coordinate-system. By implementing point C (Achilles tendon) and the lower point B (tibial border), the x-axis can be calculated by the aid of the cross product of their vectors. The cross product of the vectors of the x-axis and the z-axis delivers the y-axis. The origin of the tibial-coordinate-system is point C at the Achilles tendon projected to the ground by means of point E. All results are displayed relative to the tibial coordinates. The sampling rate was 300 Hz.

Tibia-coordinate-system with points A and B at the tibial border and point E at the ground. Point C at the Achilles tendon is not visible here.

Detailed drawing of the ultrasonic pointer with the heads for marking the AT (4) and the other points for the tibia-coordination-system (1) as well as the two ultrasonic markers (2 and 3).
After determination of the tibia-coordinate-system, the measurement starts with the subject standing in an upright position with the feet positioned hip width. In this position, the neutral position of the ankle joint is recorded by the ultrasonic system. After this, the subject takes a seat and moves his/her foot in a maximal dorsiflexed position. This position is recorded too. In this maximal dorsiflexed position, the subject has to perform six consecutive inversion and eversion movements. It was assumed that in the maximum dorsiflexion, the talus is fixed in the ankle mortise and pure rotation around the STA occurs. The researcher fixes the foot with his/her hand in the maximum dorsiflexed position and in the maximum eversion and inversion positions to make sure that the positions are correctly reproduced and that the foot is in maximum dorsiflexion during the whole procedure (figure 4). The inversion and eversion movements are recorded as trajectories by means of the ultrasonic system. On the basis of these trajectories, the software calculates the spatial orientation of the STA by the single-point method. The program uses three predefined positions from the marker to calculate the STA: one position from the marker in maximal eversion, one in maximal inversion and one in between (figure 4). As the rear foot movement around the STA was assumed to be a movement in one plane, these three points are lying on that plane and each of them has the same distance to the centre of rotation. The STA is perpendicular to this plane and intersects the centre of rotation. The whole measurement takes between 5 and 10 min.

Ultrasonic pulse-echo-based measurement system at a right foot in maximal dorsiflexion (A), maximal dorsiflexion and maximal eversion (B) as well as maximal dorsiflexion and maximal inversion (C).
Following the six repeated measurements, the software immediately shows the mean and SD of an individual's STA. According to the literature, the orientation of the STA is expressed by the inclination and the deviation angle.11 The inclination angle is defined as the angle between the STA and the horizontal plane projected into the sagittal plane. The deviation angle is defined as the angle between the STA and the sagittal plane projected to the transversal plane. Based on the displayed SD, the quality of the performed movements can be estimated by calculation of the error of measurement. If the SD from six repeated measurements was more than 5°, the measurement was excluded.
The entire diagnostic method had to pass several validity and reliability tests. A mechanical model was used to calculate the error for the measurement system. The measurement was repeated 10 times and mean and SD have been calculated. The calculated error for the reliability tests using the mechanical model was less than 0.9°. In addition, the reliability was checked in vivo by repeating 10 measurements in 10 different subjects. The error concerning the in vivo tests was less than 2.5°. The in vivo error is higher than the error using the mechanical model. This difference is most likely the result of skin movements and less accurate movement of the subject's foot in maximum dorsiflexion. Each measurement was performed by the same investigator to avoid interobserver bias.
The validity was checked in the mechanical model and by MRI in vivo investigation. The axis of the mechanical model was given. So the results from the measurements could be compared with the known axis. The error was ±0.85° for the inclination angle and ±1.34° for the deviation angle. One subject underwent two subsequent in vivo MRI recordings (G-Scan, 0.25 Tesla, ESAOTE, Biomedica Deutschland GmbH, Neufahrn) in maximum dorsiflexion combined with maximum eversion and inversion, respectively. The position of the talus from the two recordings was compared and differences were less than 1 mm. Consequently, in maximal dorsiflexion there is no movement in the talocrural joint and the measured movement can be assumed as an isolated movement of the subtalar joint as described in the literature23 and was checked in vitro.22
Statistics
χ2 2 × 2 Contingency tables were used for analysis of sex discrepancy between the locations of injuries. Average and SD of the inclination and deviation angles from six repeated inversion–eversion movements were calculated from the STA-determination software immediately. Average and SD of the inclination and deviation angles across all subjects were calculated at the end of the experimental phase. Mean differences of the inclination and deviation angles between symptomatic and asymptomatic Achilles tendons and between males and females were compared by an independent t test. A p value lesser than 0.05 was regarded as significant. Also effect size d was calculated and d≤0.2 was regarded as a small, 0.2<d≤0.5 as a medium and d>0.8 as a big effect.25
Results
The mean inclination angle of all 614 STA was 42±16° and the deviation angle was 11±23° (figure 5A). The mean inclination angle in females and males was 45±17° and 41±16° (p<0.006), respectively. The mean deviation angle in females and males was 6±22° and 13±23° (p<0.001), respectively (table 2).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Results of the subtalar joint axis—total sample, subjects with Achilles tendon disorders and uninjured subjects with average and effect size for significant data pairs
Of the 307 analysed subjects (table 1), 211 (69%) had previously been injured. A total of 664 injuries were reported. Fifteen per cent (n=95) of these injuries were related to the Achilles tendon. Men were significantly more frequently affected than women (men 18%, n=80 and women 8%, n=15, p<0.001).
Compared with the non-injured group, (table 1) people with Achilles tendon disorders were taller (p=0.03), heavier (p<0.001) and older (p<0.001). People and generally men with Achilles tendon disorders had a significantly higher mileage than women (p=0.015) and uninjured persons (p<0.001).
A significant mean difference was found between the deviation angle of subjects with Achilles tendon pathologies and subjects without (p=0.002) (figure 5B and table 2). Men with Achilles tendon disorders had a 6° higher deviation angle (more oblique) than uninjured men (p=0.034) and the deviation angle in women with Achilles tendon disorders was 10° more oblique than in uninjured women (table 2).
Discussion
In this study, we determined the inclination and deviation angle of the STA in a large cohort using a recently developed in vivo method. Besides a great interindividual variability of the STA,12 13 26,–,28 a significant mean difference of the deviation angle has been calculated for people with and without Achilles tendon pathologies. This is true for the total sample as well as for men and women. This finding is strengthened by the gender discrepancies; women had a significantly smaller deviation angle and were affected significantly infrequently than men.
A more oblique STA seems to be associated with overload injuries of the Achilles tendon. A greater deviation angle could cause an asymmetrical loading of the Achilles tendon. We assume that the distance between the penetration point of the STA through the skin of the heel and the Achilles tendon is responsible for individual variations in the load distribution within the Achilles tendon during locomotion (figure 6).
In the literature, asymmetric Achilles tendon loads have often been discussed as factors causing injury.10 29 During the ground contact phase of gait, the Achilles tendon moves in three planes. It is conceivable that due to a more oblique STA, the Achilles tendon becomes more twisted during pronation and supination. Pronation includes eversion of the calcaneus combined with abduction and dorsiflexion of the foot.8 When deviation is increased, the STA passes more laterally through the Achilles tendon creating a longer moment lever arm for the fibres within the medial Achilles tendon column. Tractive load within these fibres therefore may rise inducing the degenerative pathway.
The anthropometric data from this study support the previously postulated relation between Achilles tendon disorders and body height, weight, age and mileage. Foot size and body height are associated and larger feet are subjected to longer levers during the stance phase of running, and therefore possibly producing more torques. Weight, in general, increases the load during foot contact while age negatively influences the biomechanical properties of the Achilles tendon and mileage may induce a tendon ‘wear out’.5 However, these relationships could be spurious, because subjects with Achilles tendon disorders were predominantly men, and men were significantly higher, heavier and ran significantly more than women. Age was previously discussed in the literature as a risk factor for Achilles tendon disorders.30 The presented data indicate that the incidence of Achilles tendon disorders is most probably a multifactorial problem and anatomical factors like the orientation of the STA seem to act as predisposing agents.
The method for determination of the subtalar axis used in this study is not as accurate as other methods that use MRI21 23. The motion sequence especially influences the accuracy of measurement. Furthermore, for wider clinical application of this measurement approach, between-rater and between-days reliability needs to be established. However, the advantage of our device over more accurate methods is that it is easy and non-invasive to apply. The present study demonstrated its usefulness for capturing a large number of subjects needed to statistically prove the relationship between the spatial orientation of the STA and proposed risk factors for overuse injuries using the example of Achilles tendon pathologies. With a dataset of that size, this study by far outranges all previously reported investigations, which measured the spatial orientation of the STA.21,–,23
What is known about the topic
The spatial orientation of the STA has been discussed as an injury-causing factor, but due to methodical limitations, this question has not been investigated previously.
What this study adds
This is the first study demonstrating a relationship between Achilles tendon overload injuries and the spatial orientation of the STA. Standard textbook descriptions of the subtalar axis should possibly be revised.
Although evaluating STJ axis orientation may assist in identifying those at risk for Achilles tendon pathology, applicability in the clinic may be limited by the requirement of equipment and expertise currently not available for a sports medicine practitioner. In addition, the time it takes to complete such a measurement is 5–10 min.
A number of limitations need to be acknowledged: use of a retrospective design, use of a non-specific Achilles tendon pathology diagnosis relying on historical recall of participants to identify previous injury and absence of a physical examination to exactly indentify Achilles tendon pathology. Therefore, prospective investigations should be designed to definitely prove the postulated relationship between the orientation of the STA and specific Achilles tendon disorders.
Better understanding of the foot mechanics may be possible if based on the spatial orientation of the STA. Without understanding the complex interactions between anatomy, statics and biomechanics of the lower extremity, the reason for chronic overuse injuries of the lower extremity can hardly be clarified. Research should be concentrated on the aetiology and the mechanism of chronic overuse injuries to implement effective preventive strategies.31
Conclusion
This study adds to our understanding of Achilles tendon pathologies proposing asymmetrical Achilles tendon loading depending from the torque produced by the individual relation of the Achilles tendon fibres with the STA. Patients at risk for Achilles tendon disorders consequently could be identified by determining their STA. Conservative treatment actively (by training) and/or passively (by specific shoes or orthotic insoles) could possibly be designed following determination of an individual's STA. Research on individual ankle replacement might be influenced as well.
References
Footnotes
-
Funding The study was funded by the German Institute of Sport Science. This sponsor had no involvement in the discharge or organisation of the study.
-
Ethics approval This study was conducted with the approval of the local ethics committee of the Medical Institute of Tübingen, Germany.
-
Provenance and peer review Not commissioned; externally peer reviewed.