Article Text

Abstract
Purpose The aim of the present study was to investigate the effect of the JUMP-in programme on sports participation, overall physical activity (PA), shuttle run score and body composition in 6–12-year-old children.
Methods JUMP-in is a school-based strategy combining environmental policy, neighbourhood, parents- and personal components. A controlled trial was carried out in 19 primary schools including 2848 children (50% boys). Measures were performed at the beginning of the first school year (T0: 2006) and repeated at the end of the first (T1: 2007) and second school year (T2: 2008).
Results A significant beneficial intervention effect was found on organised sports participation (OR 2.8 (2.2 to 3.6)). Effects were stronger for girls (OR 3.6 (2.3 to 5.6)), and for Moroccan (OR 4.2 (3.6 to 5.7)) and Turkish children (OR 3.2 (1.9 to 5.2)). Participation in organised sports was associated with increased shuttle run score. No significant intervention effects on overall daily PA rates and body composition were observed.
Conclusion The present study proves that a school-based strategy combining environmental and personal interventions was successful in improving structural sports participation among children.
Statistics from Altmetric.com
Background
Physical inactivity and overweight are two major public health issues with severe health consequences.1,–,3 Dutch children living in socio-economically deprived areas seem to have the lowest levels of physical activity (PA) and the highest rates of overweight.4 5 The regular curriculum of school physical education (PE) does not provide the opportunity to reach the entire amount of recommended daily PA.6 Luepker,7 for example, pointed out that primary-school-aged children spend only 6% of their time in PE class in aerobic activities. Extracurricular programmes and family involvement are therefore needed to ensure that children engage in adequate amounts of PA. Nonetheless, the school environment provides various opportunities for intervention.8 Major advantages of school-based interventions are as follows: (1) the relatively easy access to children through the schools; (2) changes in the school environment are relatively easy to implement and monitored; and (3) school-based interventions reach all schoolchildren of all social classes.
JUMP-in is a primary-school based multilevel intervention primarily aimed at the promotion of PA and sports participation among children in socially and economically deprived areas in Amsterdam. JUMP-in incorporates policy, environmental and individual components, and involves primary schools, municipal authorities, local sport services, sports clubs and youth healthcare. Longer-term objectives are the prevention of overweight and improvement of physical fitness through increased PA levels. The development of JUMP-in started in 2002, based on the Precede Proceed model.9 10 The Intervention Mapping protocol11 was applied in order to systematically design the intervention. Results from a JUMP-in pilot study showed that JUMP-in prevented the decrease in PA normally seen with increasing age. Among the 12-year-old children in the pilot study, instead of a 30% decrease in PA in the control group, the intervention group showed a 2% decrease only.12 The outcomes of the pilot study were translated into an improved programme and intervention organisation. The stepwise development of JUMP-in has been described previously, including the pilot outcomes, the programme components and strategies, and hypothesised working mechanisms.9 11,–,14 Table 1 provides an overview of the improved JUMP-in components.
Overview of the main JUMP-in components and responsible implementers
The aim of the present study was to evaluate the effectiveness of this improved JUMP-in programme on sports participation, overall PA, aerobic fitness and body composition in 6–12-year-old children. Further, we hypothesised that increased sports participation leads to an increase in aerobic fitness. Should we be able to confirm these hypotheses, implementation of the JUMP-in PA and sports promotion programme will help to improve the health and fitness of schoolchildren with the obvious potential to reduce direct healthcare costs and indirect costs later in life.
Methods
Participants
The study is a controlled trial carried out in 19 primary schools among a total of 2848 boys and girls in grades 3–8 (aged 6–12 years, 50.4% boys). To be included in the trial, schools needed to have: (1) a certified PE teacher; (2) a majority of pupils with low socio-economic status; and (3) a gymnasium, either in the school or in the direct vicinity of the school. A passive informed consent procedure15 was applied: all parents received a letter describing the study procedures, with the option to sign and return the form if they did not want their child or themselves to participate. The Medical Ethics Committee of VU University Medical Center approved the study protocol.
Recruitment of schools
Nine intervention schools were recruited in two city districts that planned to start the implementation of JUMP-in. Random assignment of schools to a control or intervention group was not possible because of prolonged preparations needed for a successful adoption and implementation of JUMP-in: a school- and environmental scan had to be carried out and commitment had to be built among school staff and local partners in sports, care and prevention. Further, networks had to be created among participating organisations, and organisational practices had to be prepared for the implementation of the programme and related protocols.
Ten comparable control schools were recruited from geographically separated city districts to limit the possibility of contamination between intervention and control schools. The control schools were asked to continue their usual curriculum during the study period. Children and parents were unaware of the existence of intervention and control schools. They were told that the aim of the study was the assessment of sports and leisure time physical activities among children in Amsterdam. Regular contact with the management and educational personnel of the schools took place to promote their continued participation. The control school staff were offered the JUMP-in programme at the end of the study. The city districts in which control schools were located supported the study and declared to support the implementation afterwards.
Measurements
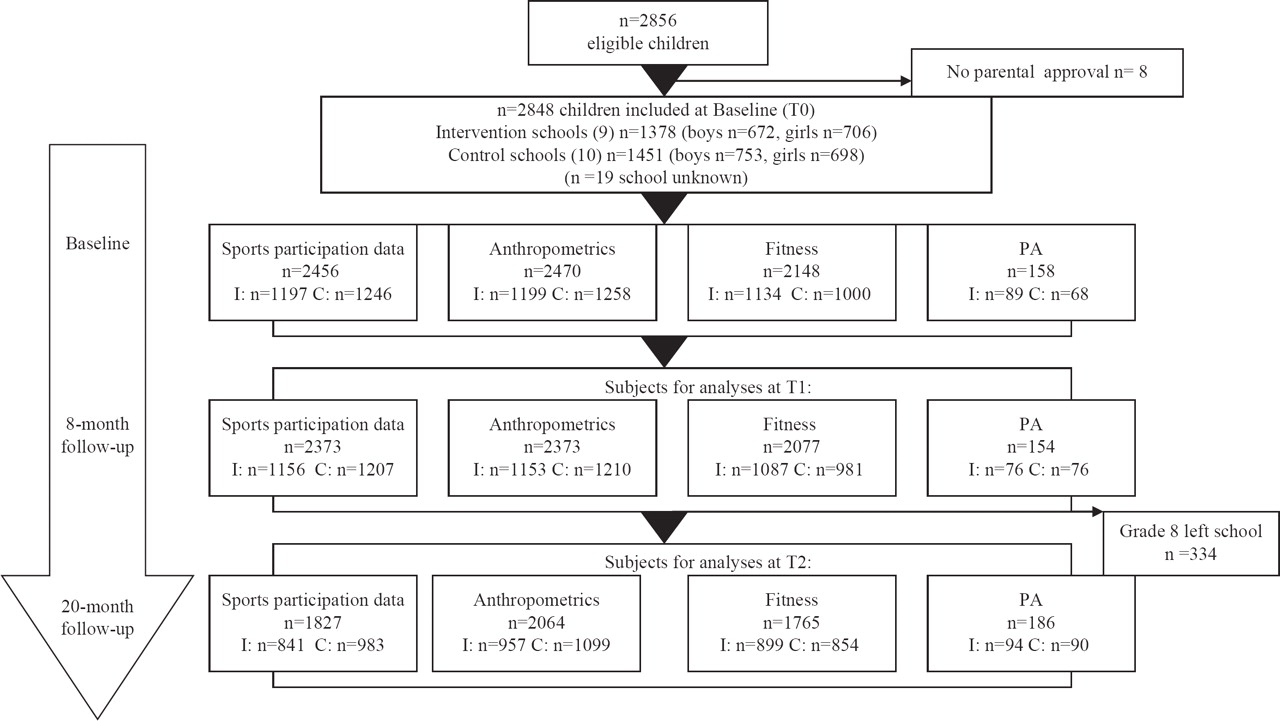
Measures were performed at the beginning of the first school year (T0: September to October 2006) and at the end of the first school year (T1: May to June 2007), and repeated at the end of the second school year (T2: May to June 2008). All measurements took place at school and were performed according to standardised procedures by trained testers. The intervention duration was 8 months in the first year (from November to June) and 9 months in the second year (September 2007 to May 2008). Figure 1 presents the flow diagram of subjects through the measurements. Since the children from the highest grade left school after 1 year, these children were not measured at T2.

{kind=link}
Flow of participants through the study.
Demographics
Demographics (gender, date of birth, country of birth for child, mother and father) were assessed by questionnaires completed by the children and parents. Age was calculated based on the self-reported birth date. Classification of ethnicity was based on the classification criteria of the Central Bureau of Statistics in The Netherlands (CBS 2000). If at least one parent or the child itself was born in Africa, Latin America, Asia (except Japan and Indonesia) or Turkey, a child was classified as non-Western. All other children were classified as Western. ‘Dutch,’ ‘Turkish,’ ‘Moroccan’ and ‘Surinamese’ were included in the analyses as separate groups, because those ethnicities were most prevalent in the sample. The remaining ethnicities were coded as ‘other western’ or ‘other non-Western.’
Primary outcome measures
Sports participation
Sports participation was assessed in a personal interview. Trained interviewers asked whether the child participated in organised sports activities at least once a week for a minimum of 3 months (yes or no). Following the results in the pilot evaluation, an interview was the most reliable way to classify sports participation, compared with questionnaires and attendance lists.
Daily PA
PA was measured in all children in grade 4 (n=351 mean age 7) using accelerometers. Two trained research assistants fitted the children with an Actigraph accelerometer (Actigraph 7164 or Actigraph GT1M). Participants received the accelerometer on a Tuesday afternoon during school hours, with actual registration starting Tuesday at midnight. The delay in registration was opted for, because research by De Vries et al5 showed children to be significantly more active on the first day of wearing an accelerometer than on the second day. Children were instructed to wear the accelerometer during all waking hours, except when bathing, showering or swimming. An information brochure for parents was given to the children to take home. After 5 full days of registration, on the subsequent Monday, the accelerometers were reassembled, data were downloaded to a personal computer, and accelerometers were reinitialised for renewed distribution on Tuesday. The data were stored in 60 s epochs, which indicates a storage of the mean activity intensity every 60 s.
The mean number of counts per minute was used in the statistical analysis. Actigraph data were excluded if (1) less than 10 h a day were measured; or (2) when less than 3 days of complete data (>10 h/day) were available. Hours between 21:00 and 7:00 were excluded, as were periods of at least 20 consecutive minutes with output equal to zero, assuming the accelerometer was not being worn during these periods. Because of children's sickness, loss of accelerometers, technical problems and incomplete data, a final sample of 158 subjects with on average 4 days of complete accelerometer data files was available at baseline. A sample of 154 and 186 subjects was available at T1 and T2, respectively (see figure 1).
Secondary outcome measures
Anthropometry
Weight and height were measured by trained research assistants using a standard measurement protocol. Children's weights (in underwear) were measured with a calibrated balance (Care 2 Move Medical, Marsden MS-230; Marsden, the weighing company, Henley-on-Thames, Oxfordshire, UK). Height was measured with a folding length yardstick with a pedestal (Care 2 Move Medical, Marsden MH-226; Marsden, the weighing company, Henley-on-Thames, Oxfordshire, UK). The measurements were carried out in a private room, in underwear and bare feet. Body mass index (BMI) was calculated by dividing the weight (kg) by height (m) squared (kg/m2). Weight status was divided into normal weight, overweight and obesity based on internationally acknowledged BMI cut-off points for children as defined by Cole et al.16 Waist and hip circumference were measured with a flexible band (Seca) to an accuracy of 0.5 cm. The anatomical landmark for the waist circumference was laterally midway between the lowest portion of the rib cage and the iliac crest.
Aerobic fitness
Aerobic fitness was measured by the shuttle run test (SRT). In this study, the distance between the two lines was set at 18 m instead of the usual 20 m, owing to the fact that most primary school gyms were too small for a 20 m SRT. The SRT was conducted in small groups of 10 children. Participants repeatedly ran from one fixed line to the opposite fixed line and had to arrive before they heard a beep. During the test, the time between the sound signals decreased every minute, thereby increasing the running speed. Every child was told that they could stop when feeling too tired to continue, and was ordered to stop by a member of the research team when they failed twice successively to reach the line before the beep. The test results were expressed as the number of laps at which a child stops. One lap is one way and back. According to Boreham et al17 and Van Mechelen et al,18 the SRT is a valid test to assess aerobic fitness.
Statistical analyses
Descriptive statistics were used to describe participant characteristics for the intervention and control group at baseline. Independent t test or χ2 tests were carried out to explore and quantify subgroup differences at baseline regarding gender, age, weight status, sports participation, fitness and daily PA.
Linear and logistic multilevel auto regression analyses were used to estimate the effect of the intervention. Using the multilevel technique with two levels (ie, individual and school), regression coefficients could be adjusted for the clustering of observations within one school and individual.
The parameters of interest are the regression coefficients (b) indicating the difference between intervention and control group. In the crude model, the outcome value at 20 months was adjusted for baseline value and for the value at 8 months. Effect modification by gender, age, ethnicity and BMI was checked. All analyses were performed according to the intention-to-treat principle.
Sample-size calculation was based on changes in daily PA and sports participation. A relative difference in daily PA of 10% between the intervention and control group after 21 months was considered to be clinically relevant. The study also focused on effects within subgroups for gender or ethnicity. Based on this, we needed 375 subjects per group to be able to detect a difference of 10% between conditions with a power of 90% and an α of 5%, taking into account the clustering within schools and a dropout rate of 10%. A sample size of 2000 subjects was required. We increased the sample size to allow for a higher dropout rate. Grade 8 subjects were lost at T2, because they left school.
The association between changes in sports participation and changes in shuttle run score were analysed using multilevel autoregressive analysis, in which the outcome variable shuttle run score was adjusted for its values at T0 and T1, gender, age, BMI and ethnicity. The independent variable, sports participation, was recoded into three dummy variables, with children who were inactive at both T0 and T2 as reference group. Dummies were defined based on the change in sports participation; group (0) children inactive at T0 and T2; group (1) children inactive at T0 and active at T2; group (2) children active at T0 and inactive at T2; group (3) children active at T0 and active at T2.
Results
Study population
A total group of 2848 children were available for the baseline measurements and were included in the study (T0). Of the included children, 2442 (86%) participated in the sports participation interview at baseline, 2363 (83%) after 8 months (T1) and 1824 (66%) after 20 months (T2). From responders excluded at baseline and T1, 14 (0.005%) refused to participate. The most common reasons for dropout were absence due to illness or transfer to another school.
At baseline, anthropometrics were obtained from 2457 children (87%). The follow-up rates at T1 and T2 follow-up were 83% and 72%, respectively. The dropout at T2 was mainly due to the highest grade leaving school to go to secondary school.
From all included subjects, 2134 participated in the SRT (75%). The follow-up rates were 73% and 62%, respectively. Accelerometer data were only available from grade 4 (mean age 7). At baseline, 351 subjects were included. Reasons for dropout were illness, moving to another school or moving to another class/grade.
Figure 1 shows the flow of subjects through the trial and the available measurements at baseline (T0), after the first period and after the second period (T1+T2). Dropouts were not significantly different from participants regarding the outcome measures.
Table 2 presents the ethnicity of the intervention and control group, and table 3 the baseline characteristics for intervention and control schools. The mean age of the subjects was 8.6 years, and 50% (1435) were male. Analyses comparing baseline characteristics between control and intervention schools showed some statistically significant differences. Significantly more subjects in the control condition were participating in sports (for boys 50% vs 37% and for girls 25% vs 18%), and subjects in the intervention condition scored significantly higher at the SRT (boys 6.3 vs 5.8 and girls 5.1 vs 4.6).
Ethnicity of the study population
Baseline characteristics in the intervention and control schools
Intervention effects
Table 4 shows the values (uncorrected means (SD's) or percentages) for all outcome measures at baseline and the two follow-up measurements. A significant intervention effect was found on organised sports participation among the total study sample (OR 2.8 (95% CI 2.18 to 3.62)) (table 4). No intervention effect was observed on daily PA behaviour (b=40 CPM; (95% CI −27 to 106)), BMI (b=0.07 kg/m2 (95% CI −0.02 to 0.16)), hip (b=0.1 cm (95% CI −0.32 to 0.42)), waist circumference (b=0.3 cm (95% CI −0.15 to 0.75)) and shuttle run score (b=0.02 laps (95% CI −0.26 to 0.29)).
Means (SD) for outcome measures at baseline (T0), 8 months' (T1) and 20 months' follow-up (T2)
Subgroup analyses
Gender and ethnicity were found to be effect modifiers. The intervention effect on organised sports participation was found to be stronger in girls than in boys (OR 3.6 (95% CI 2.3 to 5.6) and 2.2 (95% CI 1.7 to 2.8), respectively) and stronger in Moroccan and Turkish children (OR 3.2 (95% CI 1.9 to 5.2) and 4.2 (95% CI 3.6 to 5.7), respectively (table 5)).
Intervention effects on organised sports participation per subgroup
Relationship between sports participation and shuttle run score
Children who started participating in organised sports and children who maintained participating in organised sports between T0 and T2 had a significantly higher score on the SRT at the end of the intervention period (table 6).
Relationship between sports participation and shuttle run score
The association between changes in sport participation and changes in shuttle run scores is analysed using multilevel autoregressive analysis, in which the outcome variable shuttle run score is adjusted for its values at T0 and T1, gender, age, BMI and ethnicity. The independent variable, sports participation, was recoded into three dummy variables, with children who were inactive at both T0 and T2 as a reference group.
Discussion
The purpose of the present study was to evaluate the intervention effects of JUMP-in on sports participation, daily PA, BMI, hip and waist circumference and shuttle run score. After 20 months, the intervention group showed a significant increase in structural sports participation, especially in girls and Turkish and Moroccan children. Within the JUMP-in intervention approach, these groups were specifically targeted as high-risk groups, because they show the lowest levels of sports participation, have the lowest socio-economic background and are usually most difficult to reach by any preventive intervention that is not included in the regular school curriculum.19
Schools have been identified as a key setting for health promotion.20 However, an overview of the literature shows that, generally, school-based interventions aimed at the promotion of PA had no effect on overall leisure-time PA rates. Further, extracurricular school-based interventions often had problems with low attendance.21,–,23 Although evidence is sparse, environmental strategies (interventions that change policy and practice) appear to promote PA in elementary schools effectively.20 21 The present study proves that our intervention was successful in improving sports participation through a school-based strategy combining environmental and personal interventions.
A strength of the present study is the fact that the intervention was implemented by the school staff, city district and local partners in healthcare and sports themselves. JUMP-in was integrated into existing local initiatives and proved to be feasible and applicable in real-world settings and ethnically diverse and socio-economically deprived schools. Another strength was the objective measurement of PA by accelerometers. Further, sports participation was assessed in personal interviews by trained testers. Previous experiences in the pilot study pointed out that this method is much more reliable and prevents response bias and over-reporting of PA levels.
Our trial also has some limitations. First, randomisation of schools was not possible, as the adoption and organisation in the intervention schools had to be prepared several months before the intervention started. However, children and parents were not aware of the existence of the other condition, which could have biased the results. Second, we modified the SRT by setting the lines at 18 m instead of the usual 20 m, because most primary school gyms were too small for a 20 m SRT. However, this was the same in intervention and control schools. Third, the accelerometers for PA measurement were used in a very small portion of the sample. Fourth, not all testers could be blinded to group assignment of the children.
We hypothesised that increased sports participation would lead to increased shuttle run scores. Although the intervention did not significantly improve shuttle run scores, we observed that children who started organised sports participation and children who remained active in organised sports had a higher shuttle run score at the last follow-up measurement than children who did not participate in organised sports at both measurements.
We found no intervention effect on anthropometrics. This may be explained by the fact that JUMP-in was primarily aimed at PA behaviour and did not include dietary behaviour. However, to offer overweight children tailored care, JUMP-in uses the Amsterdam ‘Overbruggingsplan,’ an intervention for overweight children carried out by the municipal youth healthcare.24 For overweight children detected by the pupil follow-up system in JUMP-in schools, extra care is available; obese children in all grades are directly referred to youth obesity clinics, and overweight children in grade 4 of JUMP-in schools are invited by the school nurse for one or more extra ‘consultations.’ Results of the Amsterdam youth healthcare monitor indicate that the prevalence of overweight has decreased over the period 2006–2009.25 These findings suggest that the Amsterdam youth healthcare is successful in decreasing of overweight and obesity. Therefore, JUMP-in continued the intensive collaboration with this youth healthcare intervention.
Based on the results of the present study and the process evaluation, we adapted the contents and organisation of JUMP-in in 2009. To be able to reach a decrease in the prevalence of overweight, the new JUMP-in programme was extended, including improving dietary habits of children, school policies regarding healthy nutrition, and promotion of fruit and vegetable intake. To enhance PA behaviour, we planned activities promoting active transport to school and adaptations of school playgrounds to promote active playing in lunch breaks. Further, collaborations between disciplines in sports, welfare and care are intensified and institutionalised, and selective prevention and care for children at risk (overweight, inactive or motor deficiencies) is embedded in the organisational structures of local partners and local policy.
The effects of JUMP-in on organised sports participation and the resulting improvement in fitness are of great importance for the combat against the complex problems of youth obesity and inactivity.
References
Footnotes
-
Competing interests None.
-
Patient consent Obtained from the parents.
-
Ethics approval Ethics approval was provided by Medical Ethics Committee of VU medical Center of Amsterdam.
-
Provenance and peer review Not commissioned; externally peer reviewed.