Article Text

Abstract
Purpose The aim of this study was to compare the outcome of hip arthroscopy for femoroacetabular impingement (FAI) between athletes and non-athletes.
Methods The authors prospectively collected data on 122 patients, the largest comparative series reported, who underwent hip arthroscopy for FAI. Of these, 80 actively participated in sporting activities (athletes), while 42 did not (non-athletes). Patients were asked to complete questionnaires for the modified Harris hip score (MHHS), non-arthritic hip score (NAHS), patient satisfaction on a visual analogue scale (VAS). This was collected immediately before surgery, and at 6 weeks, 6 months and 1 year after the procedure. The responses to the MHHS questionnaire were used to calculate the quality-of-life (QoL) score using the Rosser index matrix.
Results A significant improvement in the MHHS, NAHS and QoL was observed at 6 weeks, 6 months and 1 year after surgery (p<0.001). The 6-week MHHS (p=0.01) and NAHS (p=0.04) for the athletes were significantly better as compared with non-athletes. However, the 6-month and 1-year MHHS, NAHS and QoL scores were statistically similar for both groups.
Conclusions In this large, prospective series of patients we have demonstrated the positive impact of arthroscopic surgery for FAI in both the athletic and non-athletic population. Arthroscopic management of FAI is thus not the sole domain of the athletic patient. Non-athletes can do just as well.
Statistics from Altmetric.com
Introduction
Hip arthroscopy is an established intervention for the treatment of hip pathologies in the sporting and general population.1–9 An acetabular labral tear is described as the most common pathology for which hip arthroscopy may be indicated, and selective debridement of these tears, without addressing the impingement, leads to satisfactory 10-year results in more than 80% of patients.10 Although there is no evidence on the prevention of osteoarthritis, the early clinical data suggest that by resolving bony impingement, prevention of further labral and chondral damage is possible, and the progression of osteoarthritis may be delayed.11 Even in the patients with milder degrees of preoperative degenerative change on their radiographs, after osteochondroplasty for femoroacetabular impingement (FAI), an improvement in pain and function has been demonstrated at short-term follow-up.12
Labral preservation with osteochondroplasty for FAI in a professional sportsperson can lead to a high patient satisfaction rate and prompt return to sports.13 ,14 In a 10-year follow-up of 15 athletes, Byrd and Jones7 reported that 87% returned to sports, but five of these patients required hip replacement at a mean of 6 years. In the general population, arthroscopic management of FAI leads to a good or excellent result in up to 75% of patients at 1 year.15 ,16
However, most studies have been within an athletic population. No studies exist for the non-athlete who, in reality, represents a significant portion of the community. In particular, there is no comparative study looking into the difference in outcome between the athletes and non-athletes. This was an area we considered to be critical to the development of hip arthroscopic surgery and we wished to investigate the issue further. Our null hypothesis was that there is no difference between athletes and non-athletes after arthroscopic labral preservation and osteochondroplasty for FAI.
Methods
We report the results from a single surgeon's prospective series of patients. We wished to explore the benefits of hip arthroscopic intervention for FAI and associated pathology, with particular attention to the difference in outcome between those who engage in sporting activities (athletes) and those who do not (non-athletes). We have prospectively collected the modified Harris hip score (MHHS), the non-arthritic hip score (NAHS)17 and a patient satisfaction score using a visual analogue scale (VAS) from 0 (no pain) to 100 (maximum pain). We used previously described techniques to calculate quality-of-life (QoL) scores from the responses from the MHHS.18 ,19 The qualitative nature of responses allows them to be translated to Rosser distress (pain) and disability (function) categories (box 1), which can be applied to the Rosser index matrix20 (table 1) to derive QoL scores. The Rosser index matrix20 allocates scores from −1.486 to 1.000. A score of 1 indicates complete normality while death is given a score of 0. Negative scores indicate health states thought to be worse than death. The scores were collected immediately preoperatively on the day of surgery and postoperatively at 6 weeks, 6 months and 1 year.
The Rosser index20
Disability
-
No disability
-
Slight social disability
-
Severe social disability and/or slight impairment of performance at work
-
Choice of work or performance at work severely limited
-
Housewives and old people able to do light housework only, but able to go shopping
-
-
Unable to undertake any paid employment
-
Unable to continue any education
-
Old people confined to home except for escorted outings and short walks and unable to do any shopping
-
-
Confined to chair or wheelchair or able to move around in the house only with support from an assistant
-
Confined to bed
-
Unconscious
Distress
A. No distress; B. Mild; C. Moderate; D. Severe.
The Rosser index matrix (Gudex and Kind, 1988) showing a quality of life (QoL) score for each disability/distress combination31
This is a consecutive series of 122 patients with FAI with a minimum follow-up of 1 year. The patients were asked before surgery to declare if they participated in sporting activities or not. We have excluded patients who had surgical indications other than FAI and re-arthroscopies. The diagnosis of FAI was made on the basis of the clinical findings corroborated by the radiographic and MRI imaging. Hip arthroscopy was offered to patients who had symptoms, which were restricting their life style and affecting their day-to-day activities. The surgery was performed in the lateral position with the patient under general anaesthesia, under image intensifier control and traction. The central compartment was accessed first followed by the peripheral compartment after releasing the traction. Details of the senior author's surgical technique have been described elsewhere.21 Surgery involved removal of the impingement lesion (femoral and/or acetabular) and, where appropriate, repair of chondral/labral/chondrolabral lesions. This was by microfracture, labral reattachment or chondrolabral repair using either sutures or fibrin adhesive. Labral preservation was the central philosophy in dealing with all the cases. All patients received an identical, standardised physiotherapy regimen in the postoperative period.
Statistical analysis
The statistical analysis was performed using the SPSS V.15 statistical program (SPSS Inc., Chicago, Illinois, USA). In order to determine whether the data were significantly different from the normal distribution, a Kolmogorov-Smirnov test was used. If p<0.05, the data were treated as non-parametric. To compare continuous variables, two sample t-tests were used for parametric data and the Mann-Whitney U test for non-parametric data. All the tests were two tailed and a significance level of p<0.05 was maintained throughout. A χ2 test was used to compare categorical data.
Results
The mean age of the patients at the time of surgery was 35.4 (14–59) years. There were 74 (61%, N=122) male patients, 80 athletes and 42 non-athletes.
Table 2 outlines the demographics of the two groups.
Demographics of the two groups
Outcome
The MHHS increased from a mean of 61 (6 to 91) before surgery to a mean of 73 (34 to 91) at 6 months (p<0.001) and 80 (42 to 91) at 1 year (p<0.001) after surgery. The trend of mean MHHS and the difference between the two groups is depicted in figure 1. The 6-week postoperative score was significantly (p=0.01) better for the athletes as compared with non-athletes; however, the 6-month (p=0.54) and 1-year (p=0.30) scores for both groups were statistically similar.

Trend of mean modified Harris hip score (MHHS) and bar graph showing the difference between the two groups. MHHSPreop, preoperative MHHS; MHHS6wk, 6-week postoperative MHHS; MHHS6mth, 6-month postoperative MHHS; MHHS1yr, 1-year postoperative MHHS. This figure is only reproduced in colour in the online version.
The NAHS increased from a mean of 67 (21 to 97) before surgery to 80 (41 to 100) at 6 months (p<0.001) and 85 (44 to 100) (p<0.001) at 1 year after surgery. The trend of the mean NAHS and the difference between the two groups is depicted in figure 2. The 6-week postoperative score was significantly better (p=0.04) for the athletes as compared with non-athletes; however, the 6-month (p=0.39) and 1-year (p=0.79) scores after surgery for both groups were statistically similar.

Trend of mean non-arthritic hip score (NAHS) and bar graph showing the difference between the two groups. NAHSPreop, preoperative NAHS; NAHS6wk, 6-week postoperative NAHS; NAHS6mth, 6-month postoperative NAHS; NAHS1yr, 1-year postoperative NAHS. This figure is only reproduced in colour in the online version.
The overall patient satisfaction for surgery improved on a VAS (0 to 100) from 74% at 6 weeks to 79% at 6 months and 82% at 1 year after surgery. There was no statistical difference (p>0.05) between the two groups at any stage of follow-up.
Quality of life
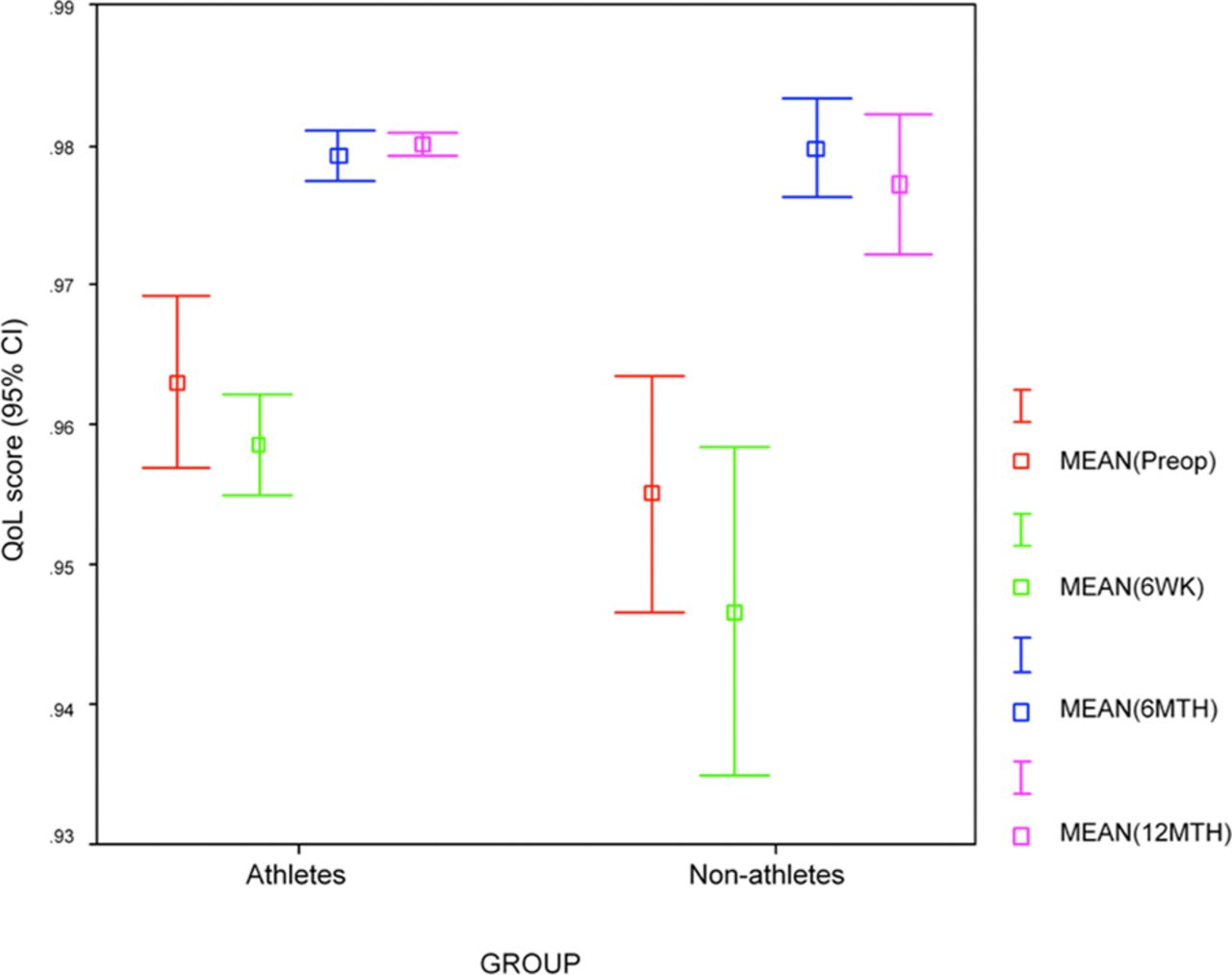
The QoL scores improved from a mean of 0.961 (0.7 to 1) preoperatively to 0.979 (0.87 to 1) at 6 months (p<0.001) and 0.982 (0.9 to 1) at 1 year (p<0.001) after surgery. The trend of the mean QoL score and the difference between the two groups is depicted in figure 3. The QoL scores at 6 months (p=0.77) and 1 year (p=0.12) after surgery for both groups were statistically similar.

{kind=link}
{kind=link}
{kind=link}
Trend of mean QoL scores and bar graph showing the difference between the two groups. QoLPreop, preoperative QoL score; QoL6mth, 6-month postoperative QoL score; QoL1yr, 1-year postoperative QoL score. This figure is only reproduced in colour in the online version.
Discussion
In a large prospective single-surgeon series of patients, we have shown that the overall outcome (MHHS, NAHS) and QoL improves after arthroscopic intervention for FAI. We have found that the scores for athletes were significantly (p<0.05) better than for non-athletes at 6 weeks’ follow-up but similar (p>0.05) at 6 months and 1 year.
FAI and any associated labral pathology is a common cause of hip discomfort in young adults.22 It has been blamed on the abnormal axial or torsional forces placed on the hip during high-output athletic activities. Recently, a better understanding of the pathomechanics and morphological abnormalities in the hip has implicated FAI as a possible factor in early osteoarthritis.23–26 Although the literature is replete with short-term evidence to support surgical treatment, there are currently no long-term prospective data or natural history studies examining the implications of FAI and effects of early intervention.22 The role of early intervention in preventing the progression of disease2 and its benefit in an early return to sporting activities has been recognised.8 ,27 ,28 When compared with open surgical dislocation, arthroscopic treatment has a lower complication rate and faster rehabilitation.29 A descriptive epidemiological study30 of adults under the age of 50 years presenting with mechanical hip pathology in the French population has revealed that 62% of patients have osteoarthritis of the hip, 70% participate in sports with 30% being high-level athletes. This may not be consistent with other population groups, and possibly is different for the other populations, but is clearly indicative of the fact that the problem is not confined to the athletes. Work to date, however, has not established if the outcome after surgery is better for the athletic population as compared with non-athletes. This was the issue that led to our present study being performed.
We have noted that although the recovery is quicker for the athletes (better scores at 6 weeks), non-athletes have a similar outcome at the 6-month and 1-year follow-up. The physiotherapy regimen for both the groups was identical. The difference in early outcome is perhaps because of the preoperative level of fitness of the two groups.
Hip arthroscopy with labral preservation and osteochondroplasty improves the QoL of patients with FAI. The functional scores (MHHS, NAHS and QoL scores) continue to improve up to 1 year after surgery. On a VAS from 0 to 100, 82% patient satisfaction was noted at 1 year after hip arthroscopy. We believe this information to be crucial during the consenting process for arthroscopic surgery for FAI.
Our study is limited by a relatively short follow-up of 1 year, but our intention was to compare the trend of recovery during the early phase of rehabilitation between athletes and non-athletes. In addition, this is a single-surgeon series of a high-volume hip arthroscopy surgeon, and may not necessarily reflect the practice of low-volume or less-experienced surgeons.
Conclusions
In a prospective series of 122 patients comparing athletes and non-athletes, the largest reported to date, we have demonstrated the positive impact of arthroscopic surgery for FAI in both athletes and non-athletes. There was no significant difference in the outcome between these two groups at 6 months and 1 year after surgery although better scores were seen in the athletes during the early period of rehabilitation. However, what is clear as a conclusion is that hip arthroscopic FAI surgery is not solely the domain of the athlete. Non-athletes can do just as well. This finding is critical to the future development and expansion of hip arthroscopic surgery for FAI.
What this study adds
-
Only comparative study looking at difference in outcome between athletes and non-athletes.
-
Results at 1 year similar in both groups.
-
Six-week functional scores better for athletes.
References
Footnotes
-
Contributors AM analysed the data and prepared the first draft. GHS analysed the data, did literature search and helped in preparing the final draft. RNV conceived the idea, contributed the cases and approved the final draft.
-
Competing interest None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
▸ References to this paper are available online at http://bjsm.bmjgroup.com