Article Text

Abstract
Background Structured, regular exercise is recommended to improve health outcomes. Exercise takes many forms and varies in type, intensity, duration and frequency. The authors used the example of exercise for chronic health conditions to examine how exercise programmes are described and summarised in systematic reviews.
Methods Two independent reviewers conducted a review of exercise reporting practices using the evidence of exercise effects for chronic conditions as the source material. Inclusion criteria: systematic reviews that summarised the effects of exercise programmes for adults with chronic health conditions. Exclusion criteria: reviews of studies of children and adolescent populations, and non-English publications.
Results Seventy-three reviews were included. Data on sample size, number of included trials, interventions, comparisons, programme characteristics, exercise components, author conclusions and recommendations were extracted. Seventy-one per cent of reviews reported being unable to adequately describe the exercise programmes, because the required information was not reported in included trials. Using key exercise descriptors from the included reviews, the authors developed criteria for reporting to a level that enables replication.
Conclusions All included reviews recommended better and standardised reporting. Incomplete exercise programme descriptions limit confidence in the accurate replication of effective interventions and limits critical appraisal of interventions when conflicting outcomes are reported. The evaluation and implementation of physical activity and exercise research would be facilitated if exercise programmes are comprehensively described. The authors propose that systematic reviews/meta-analysis and clinical application of the outcomes of exercise therapy research would be enhanced if authors used an exercise reporting grid that includes a detailed description of the programme components.
Statistics from Altmetric.com
Background
Exercise has emerged on the global stage as an integral component of health promotion and a key ingredient for health across the lifespan. Systematic reviews,1,–,4 clinical practice guidelines5,–,7 and position stands8,–,11 recommend exercise and advice to stay active for the management of many chronic conditions. Different types of exercises are intended to produce different outcomes for specific populations (eg, strength training following stroke). Smidt et al (2005) summarised systematic reviews of exercise for a range of chronic conditions till 2002, and concluded that exercise is beneficial for people with cystic fibrosis, chronic obstructive pulmonary disease, intermittent claudication, knee osteoarthritis and low back pain.1
Exercise is a non-specific term. It includes activities that vary in type, frequency, intensity, mode and environmental requirements. It may be conceptualised as a series of specific movements to train or develop the body with routine practice or as any kind of physical training to promote physical health.12,–,14 Exercise can vary with respect to the type of muscle contraction, load, speed and range of movement, number of repetitions and sets, order of exercises and rest times. It is used to enhance strength, endurance, flexibility, function or achieve specific skill acquisition.15,–,18 These features combine to render ‘exercise’ an umbrella term for a variety of quite different interventions.
The WHO defines chronic diseases as those of long duration and generally of slow progression. WHO has responded to the significant burden associated with chronic conditions, such as cardiovascular disease, respiratory conditions, type 2 diabetes, obesity, osteoarthritis and osteoporosis, by developing a Global Strategy for diet and physical activity (http://www.who.int/gbwha/e/e_wha57.html#Resolutions). The four main goals are promotion of physical activity, increased awareness of the positive impact of physical activity, development and implementation of policies to increase the physical activity and support of physical activity research (http://www.who.int/dietphysicalactivity/goals/en/print.html).
Plowman and Smith (2008) describe eight important elements in the design of training programmes: specificity or exercise modality, overload (exercise frequency, intensity and duration), rest/recovery/adaptation, progression, retrogression/plateau/reversibility, maintenance, individualisation and warm-up/cool-down.19 These are consistent with the American College of Sports Medicine (ACSM) Position Stands on progression models in resistance training, exercise for cardio-respiratory and muscular fitness, and physical activity for older adults.20,–,23 These statements recommend defining programme characteristics such as exercise types and sequences, repetitions, resistance, intensity, speed, progression rules, progressive overload, rest periods, frequency for novice, intermediate and advanced training. Models exist for strength training, muscle hypertrophy, muscle power, local muscular endurance and motor performance.20 Although these recommendations appear comprehensive, it is not clear whether they define the full set of exercise characteristics or whether they are referred to when programmes are described. Standardised reporting of exercise programme components would advance the practice of exercise prescription and research into exercise effects.
Through the review of published work on exercise for chronic health conditions, we aimed to identify elements in the design of programmes that are required for programme replication in exercise prescription and research reports. The aim of this work was to describe and summarise the characteristics of exercise programmes that have been reported in the systematic reviews of exercise for any chronic condition.
Methods
A structured review process was adapted from the Cochrane Collaboration Back Review Group updated systematic review guidelines and PRISMA guidelines.24,–,26 Before conducting searches of electronic databases, a priori inclusion and exclusion criteria were established and applied to the search yield using a standardised form.
Inclusion criteria
Systematic reviews and meta-analyses of observational studies and randomised controlled trials (RCTs) were included when they (1) were English language reports available in full text, (2) reported on the content of exercise programmes and (3) summarised the effects of exercise programmes on health outcomes for adults with any chronic health condition.
Exclusion criteria
Systematic reviews of paediatric and adolescent chronic health conditions were excluded because there are additional variables to consider in the reporting of exercise programmes for children such as parental guidance and support.
Review identification and selection
The Cochrane Database of Systematic Reviews, Medline and NCBI PubMed and PEDro databases were searched without date limit until June 2009 using key search terms such as chronic health conditions, chronic diseases, exercise, aerobic exercise, strengthening, resistance training and synonyms. The full search strategy is available from the first author on request. The first author (SS) applied the inclusion criteria to the search yield and this was independently confirmed by the second author (JK).
Data extraction and synthesis
Data extraction guidelines were developed to systematically extract data from each included review under the following headings: the condition or population studied, the nature of intervention and comparison treatments, number of included trials and total sample size, author conclusions regarding the effects of exercise and author recommendations. In addition, a focus of this review was to extract any information about exercise interventions such as (but not limited to) design, delivery, individualisation, progression, adverse events and monitoring. Review quality was not assessed as it was the description of exercise, not the credibility of review conclusions, which was the focus of this work.
Results
Review identification and selection
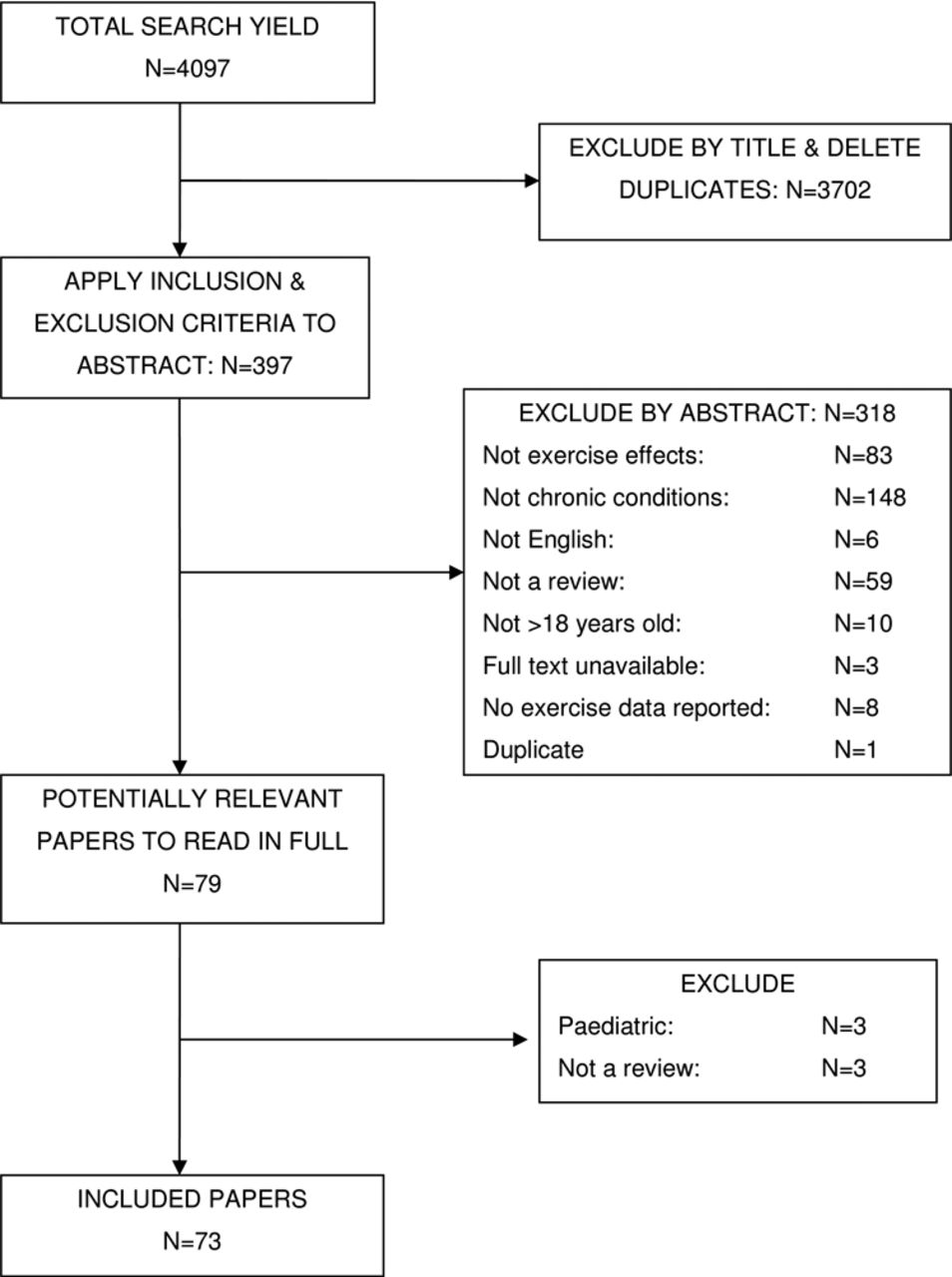
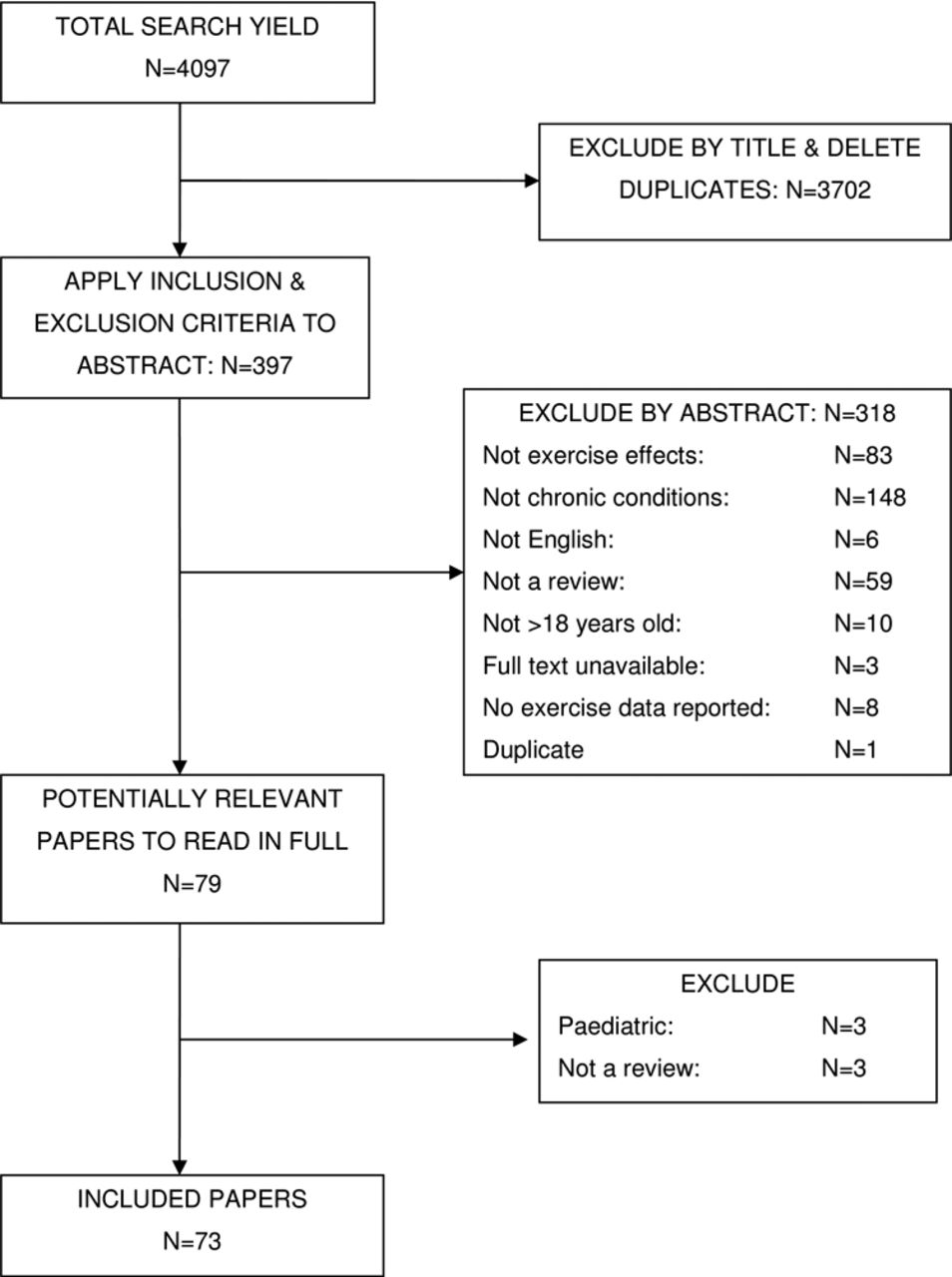
The search yielded 4097 titles: 3702 were excluded as they were clearly unsuitable (eg, exercise was not an intervention) or were duplicates. A further 318 were excluded by title and abstract because they were reviews of pharmaceutical or dietary interventions, review protocols, narrative reviews, reviews of conditions affecting paediatric populations or editorial/author narrative opinion. The flow chart of selection into the review is presented in figure 1.
{kind=link}
Flowchart of selection into the review
Data extraction and synthesis
The remaining 79 reviews were read in detail and a further six were excluded (three because they were paediatric populations and three because they were narrative summaries without data on exercise effects). Seventy-three reviews were finally included for data extraction and analysis. Information on the exercise programmes and review conclusions were then systematically extracted from each review. Data on review type, the number of included studies, the total sample size across included studies, interventions and comparisons are presented in online supplementary table S1.
There were 32 Cochrane reviews from the Cochrane Collaboration database and 41 non-Cochrane reviews published in peer-reviewed journals. Included reviews were sorted into eight categories: (1) cardiovascular; (2) metabolic, endocrinology and immunology; (3) musculoskeletal; (4) neurology; (5) oncology; (6) psychology and psychiatry; (7) respiratory; and (8) rheumatology. Fifty-four of the 73 reviews stated that the included RCTs had method quality limitations and recommended further robustly designed research. When included reviews reported the method quality of included studies to be good or high (20/73), the effects of exercise were reported to be positive.
Seventy-one per cent of the review authors reported that they were unable to comprehensively document exercise programme components and characteristics because these were not adequately reported in the included trials. Eight reviews (four Cochrane and four non-Cochrane) of exercise therapy in cardiovascular disease concluded that exercise reduced mortality and improved exercise capacity but that programmes were not reported in enough detail to enable replication.27,–,34 Sixteen reviews (eight Cochrane and eight non-Cochrane) of exercise therapy for metabolic, endocrine and immunodeficiency conditions such as diabetes, obesity, osteoporosis and HIV/AIDS reported short-term benefits and recommended more robustly designed RCTs using standardised outcome measures and explicit exercise description.35,–,49 Sixteen reviews (6 Cochrane and 10 non-Cochrane) evaluated exercise therapy for musculoskeletal conditions including osteoarthritis, tendinopathy, knee pain and chronic low back and neck pain, and concluded that, while exercise may be beneficial, the best type of exercise requires systematic evaluation.2 ,3 ,50,–,64 Fifteen reviews (5 Cochrane and 10 non-Cochrane) concluded that strengthening and aerobic exercise are beneficial for neurological conditions but that long-term follow-up and standardised outcome measures are required.65,–,79 Six reviews (two Cochrane and four non-Cochrane) of exercise interventions for cancer concluded that resistance training and aerobic exercise can improve mood and reduce fatigue.80,–,85 Three reviews (two Cochrane and one non-Cochrane) concluded that resistance training and aerobic exercise may reduce depression.86,–,88 Five reviews (three Cochrane and two non-Cochrane) of a range of respiratory conditions concluded benefits in exercise capacity and breathing control with inspiratory muscle training and aerobic exercise.89,–,93Two Cochrane reviews of aquatic and aerobic exercise for rheumatological conditions concluded small benefits for pain and function.94 ,95
Data on programme characteristics, exercise components and author recommendations were extracted from 73 reviews and are reported in online supplementary table S2. Data that described exercise programmes were extracted, coded and assembled. Codes were assembled under themes, and reviews reporting against each theme were noted. Adverse events were monitored (5%), motivation strategies were included (5%), exercise was group-based (9%), exercises were individualised (27%), rest periods in exercise programmes were described (9%), education was incorporated into interventions (10%), rules for exercise progression were described (11%), exercise compliance was measured (15%), a home programme was included (18%); the number or exercise repetitions and sets (27%), exercise intensity (33%), exercise speed (33%), stretching or range of movement was included in the programme (27%); exercises were supervised (31%) and programme drop-outs were reported (33%).
On the basis of the reported information, confident replication of exercise programmes would be possible using the information provided in 29% of the included reviews (online supplementary table S2). Aerobic exercise programmes were typically more comprehensively reported than strengthening or resistance training programmes.
Discussion
The most appropriate exercise programme for specific conditions, including the very basic elements such as session duration, exercise intensity and the number of repetitions, was typically not reported.
The reviews generally stated that meta-analyses were limited by the variability in participants, uncertainty about exercise programme content and variable outcome measures and co-interventions. Programme duration varied considerably indicating little consensus on how long it takes for exercise to effect a positive change. For example, exercise programmes for cardiovascular conditions had a mean duration of 19 weeks (SD 16 weeks) and range of 6–120 weeks; for metabolic, endocrine and immunodeficiency conditions, the programmes had a mean duration of 34 weeks (SD 38 weeks) and a range of 5–260 weeks. Review outcomes, while frequently recommending exercise, do not reliably assist clinicians in designing exercise programmes and limit the use of published data for advising patients about the probability of success.
A recurring recommendation in the included reviews is that reports of the effects of exercise should include specific descriptions of the following programme components. Areas that should specifically be reported include the type of exercise, frequency, duration, repetitions, sets, intensity, progression rules, degree of supervision, whether performed by an individual or in a group, a system to monitor adverse events and reasons for withdrawal, measures of adherence and compliance, a standardised and accepted set of outcome measures, whether a dose–response relationship can be expected, rules for progression of exercise prescription and best ways to determine a response to the programme. It would enable researchers and clinicians to replicate programmes if an explicit reporting format were adopted for programme reporting.
No standardised reporting structure has been recommended. We propose a method for reporting and presenting data on exercise design that might enable programme replication. Online supplementary table S3 presents reporting categories assembled using those reported or recommended in the included systematic reviews of exercise,2 ,3 ,27,–,95 our previous systematic reviews of exercise effects for NSCLBP,96 ,97 those arising from our previous focus group research98,–,101 and those recommended in the ACSM models for exercise prescription.20,–,23
The proposed reporting grid provides a platform for reporting exercise design that enables easy overview and accurate replication of reported exercise programmes and includes column headings that cover explicit exercise descriptions, whether exercises are generic or individualised, the type of exercise equipment used, the exercise starting position and the programme starting point, the degree of load or resistance, rules for exercise progression, motivation/adherence/compliance strategies and exercise duration/repetitions/sets/sequence.
Researchers and healthcare providers continue to prescribe exercise for chronic conditions, but the basis for decisions regarding best practice is not clear. When exercise is effective, clear and unambiguous data on the effects of exercise on health and explicit descriptions of the components and characteristics of programmes are required for the application of research findings in clinical care. To prescribe exercise that has been reported to be effective, clinicians need explicit descriptions of the components and characteristics of programmes. To monitor the effects of exercise, clinicians need clear and unambiguous information regarding the health domains that are likely to show improvement, and how changes in these are best measured. Simple, direct messages need to be communicated on the quantity and quality of physical activity that is typically sufficient to provide important health benefits. This requires that research reports include definitive information against a comprehensive set of items such as those summarised in online supplementary table S3.
A limitation of this work is that the search strategy for reviews of chronic conditions was not exhaustive. If a report was not meta-tagged as ‘chronic condition’, it would not have appeared in our search results. We have nevertheless harvested a wealth of representative evidence that supports the argument that trials of exercise are reported variably, that core elements in exercise programmes that need to be reported to enable replication are inconsistently defined and that many reviewers have explicitly raised this as an issue. It is therefore likely that the argument is made as well with the literature that we have assembled as it would be made with a slightly different search strategy.
Immediately prior to submission for publication, we re-ran a search of systematic reviews of exercise for any condition published in 2010–2011, and our findings remained unchanged; no one has defined a set of parameters that should be reported when trials of exercise are reported, and the authors continue to call for explicit descriptions of programmes.
Conclusions
Review findings demonstrate the highly variable nature of exercise reporting. This conceals a view of the elements in exercise programmes that are associated with the reported effects. All included reviews recommended better and standardised reporting of trials of exercise therapy for a range of chronic health conditions. Incomplete programme descriptions limit confidence in accurate replication of exercise programmes clinically and in the research setting, and limit the ability of researchers to build on promising interventions. All included reviews recommended that future studies be more specific in reporting exercise characteristics. It would advance the science of exercise prescription to have details that enable replication. To facilitate the evaluation and implementation of physical activity and exercise research results, it appears incumbent upon the researchers and scientific journals to embrace transparent reporting of exercise programmes at a level that allows replication in practice settings. An exercise reporting format is proposed in online supplementary table S3 as a starting point for discussion about formalising the reporting parameters.
Recommendations
The systematic review process and the clinical application of the outcomes of trials of exercise therapy would be enhanced if journal editors implemented, as policy, the completion of the exercise reporting grid. It could be part of the checklist in instructions to the authors, a format to be used by reviewers and a pro forma to guide intervention design in trials of exercise.
Acknowledgments
The authors acknowledge the National Health and Medical Research Council (NHMRC) PhD Scholarship (Biomedical) funding and a Monash University Postgraduate Publication Award assisted with this research and manuscript development.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Web Only Data - This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Web Only Data - This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Web Only Data - This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.