Article Text

Abstract
Background The medial hamstring muscle has the potential to prevent excessive dynamic valgus and external rotation of the knee joint during sports. Thus, specific training targeting the medial hamstring muscle seems important to avoid knee injuries.
Objective The aim was to investigate the medial and lateral hamstring muscle activation balance during 14 selected therapeutic exercises.
Study design The study design involved single-occasion repeated measures in a randomised manner. Sixteen female elite handball and soccer players with a mean (SD) age of 23 (3) years and no previous history of knee injury participated in the present study. Electromyographic (EMG) activity of the lateral (biceps femoris – BF) and medial (semitendinosus – ST) hamstring muscle was measured during selected strengthening and balance/coordination exercises, and normalised to EMG during isometric maximal voluntary contraction (MVC). A two-way analysis of variance was performed using the mixed procedure to determine whether differences existed in normalised EMG between exercises and muscles.
Results Kettlebell swing and Romanian deadlift targeted specifically ST over BF (Δ17–22%, p<0.05) at very high levels of normalised EMG (73–115% of MVC). In contrast, the supine leg curl and hip extension specifically targeted the BF over the ST (Δ 20–23%, p<0.05) at very high levels of normalised EMG (75–87% of MVC).
Conclusion Specific therapeutic exercises targeting the hamstrings can be divided into ST dominant or BF dominant hamstring exercises. Due to distinct functions of the medial and lateral hamstring muscles, this is an important knowledge in respect to prophylactic training and physical therapist practice.
Statistics from Altmetric.com
Introduction
In recent years, a huge step is taken towards prevention of serious sports injuries like anterior cruciate ligament (ACL) injuries. Several high-quality studies have documented that specific prophylactic training can reduce the incidence of ACL injuries.1 ,2 The majority of validated training protocols involve balance, coordination, strength and plyometric exercises.1 ,2 However, it is not known how each exercise challenges the neuromuscular system. In order to further optimise prophylactic training, an extensive exercise evaluation is needed based on an anatomical and biomechanical rationale. Thus, there is a strong need to gain knowledge about the muscle activity pattern during exercises used in both ACL prevention and rehabilitation interventions.
During forceful dynamic movements, coactivation of the hamstrings is important to provide dynamic knee joint stabilisation and to prevent excessive ACL shear forces.3 ,4 Thus, the hamstring muscles are considered ACL-agonists, and great attention has been directed towards this muscle group in the prevention of ACL injury.5
The hamstring muscles comprise the biceps femoris muscle caput longus (BFcl) and brevis, the semimembranosus muscle and the semitendinosus muscle (ST). Anatomically, the hamstrings are a two-joint muscle group acting at the knee and hip joint. Differences in muscle architecture and insertion sites between the medial and lateral hamstring muscles translate into distinct functions.6 ,7 Consequently, in prevention of ACL injury it is important to distinguish between the different muscles comprising the hamstrings.8
The ST seems important in respect to prevention of ACL injury. Contraction of the ST has the potential to compress the medial knee joint compartment and thereby reducing the risk of dynamic knee joint valgus.9 Dynamic knee joint valgus during a landing phase has been shown to predispose for an ACL injury among female athletes.10 Concordantly, low-ST electromyographic (EMG) activity during sidecutting – a movement associated with the incidence of non-contact ACL injury – in combination with high vastus lateralis (VL) activity may increase the risk for sustaining ACL injury.8 Finally, a neuromuscular programme shown to reduce the incidence of ACL injury among female athletes1 was found to induce a selective upregulation of ST activation during sidecutting.11
Common strength exercises for the leg muscles such as squats, leg presses and knee extensions show high levels of muscle activity in the quadriceps along with a preferential higher lateral compared with medial hamstring muscle coactivation.12 Focusing primarily on these exercises may predispose for knee injury. Thus, from a prophylactic perspective it is relevant to evaluate the ST-BFcl activation balance during commonly used therapeutic exercises.
The aim of this study is to evaluate the level of medial and lateral hamstring muscle activation during selected exercises used in prophylactic and/or rehabilitating interventions.
Method
Subjects
Sixteen young females (mean age: 23±3 year; mean height: 170.2±6.4 cm; mean weight: 66.2±7.4 kg) with no previous history of knee injury or hamstring injury participated in the study. The subjects were either elite handball players (n=8) or elite soccer players (n=8), and had a training frequency of 4.7±0.7 sessions/week. Subjects had in average participated in their respective sports for 15.6±4.1 years, and regular strength training for 5.4±2.4 years.
The study was approved by the local ethical committee (HC2008103) and conformed to the Declaration of Helsinki. All subjects were informed about the purpose and content of the project and gave written informed consent to participate in the study.
Test procedure
On a separate day before the actual test, participants were familiarised with the full protocol. On the day of testing participants performed three maximal voluntary isometric muscle contractions for the hamstring muscles (MVCs) with strong verbal encouragement, and we used the highest value of the three attempts for the normalisation. Participants warmed up before the MVC's. The participants warmed up during submaximal execution of the respective exercises. MVC of the knee flexors were performed to obtain maximal EMG signal amplitude. Then three trials of each exercise were performed in a randomised manner. The same person instructed the exercises for each individual. A 3 min rest period was prescribed between exercises to avoid fatigue.12 To ensure that fatigue was avoided, the subject was asked to rate perceived exertion on a Borg 10-scale,13 after the exercise protocol was accomplished, which showed a mean value of 2.5±1.1 corresponding to fairly light to moderate perceived exertion.
If a trial was performed incorrectly, in respect to the instruction, it was disqualified and a new trial was performed.
Electromyography
The skin of the subject was shaved with a hand razor and carefully cleaned with ethanol before electrode placement on the preferred push-off leg. Bipolar surface EMG electrodes (Neuroline 720 01-K, Medicotest A/S, Ølstykke, Denmark) were placed according to standardised procedures14 with a 2.0 cm interelectrode distance on the BFcl and ST muscles representing the lateral and medial hamstring muscle groups, respectively (figure 1A). Interelectrode resistances were ensured to be less than 10 kΩ. Due to the more profound nature of semimembranosus, we are not able to detect valid EMG signals for the present muscle with the use of surface electrodes.

(A) The surface electromyographic electrode placement on the examined muscles; biceps femoris muscle caput longus (BFcl) and semitendinosus (ST). (B) Maximal voluntary contraction for the knee flexors was obtained in an isokinetic dynamometer with the subject in a prone position.
The EMG signals were preamplified, band-pass filtered (5–450 Hz) and sampled (16-bit) with frequency of 1000 Hz. The digitised EMG recordings were high-pass filtered at a cut-off frequency of 10 Hz, rectified and low-pass filtered using a second order two-way Butterworth filter with a cut-off frequency corresponding to a running average window size of 200 ms.15
Maximal voluntary contraction
EMG activity was obtained during maximal voluntary isometric muscle contraction (MVC) for the hamstrings in a Biodex Medical isokinetic dynamometer (System 3 Pro, Brookhaven R&D Plaza, New York, USA). The subject was in a prone position with a hip joint angle of 10° of flexion and the knee joint angle locked in a 45° position from full extension (0°) (figure 1B).
Off-line signal processing
For each exercise trial, the filtered EMG signals were normalised to EMG recordings obtained during MVC. Peak levels of the filtered, normalised EMG were determined as the average of three trials performed for each examined exercise. The term peak nEMG refers to the peak levels of the filtered normalised EMG.
Electromagnetic motion analysis
Kinematics was measured with a magnetic tracking device (Ascension Tech Model 3D Guidance Trakstar, Ascension Technology Corp., Burlington, VT, USA), which included a system electronics unit, a mid-range transmitter, and three sensors (model 800). The measurement rate was 33 Hz. The transmitter was positioned on a wooden stand next to the subject's knee and the sensors were attached on the preferred push-off leg using double-sided tape. The sensors were positioned on the iliac crest, the distal femur and on the proximal part of fibula. Hip and knee flexion angles were obtained from the rotational matrix of the three sensors. Reference angles were achieved by an initial trial in which the subject was standing in normal upright position.
Figure 2A,B illustrate examples of the raw EMG – with corresponding hip joint angles – and the nEMG, respectively, during the execution of one of the exercises (kettlebell swing; exercise procedures are described below).

The raw electromyographic (EMG) and the nEMG, respectively, during two different single kettlebell swings. (A) A typical example of raw EMG activity during kettlebell swing. Grey line represents semitendinosus (ST), black line represents biceps femoris (BF) and dotted line represents hip joint angle. (B) A typical example of the nEMG during kettlebell swing. Grey line represents ST and black line represents BF.
Exercises protocol
The exercise protocol included nine strength and five balance/coordination exercises as described below. The exercises were chosen based on experiences from clinical practice and training as well as prevention programmes presented in the literature.
Balance/coordination exercises
The selected balance/coordination exercises have been used in ACL prevention programmes,1 ,2 and rehabilitation interventions after ACL injury.16
A balance mat (40×50 cm; 7 cm thick; Alusuisse Airex, Sins, Switzerland, 2000) was used in three of the five balance/coordination exercises.
One-leg jump onto balance mat (FJU)
The subject makes a one-legged forward jump onto a balance mat. The subject must focus on stabilising the knee in the frontal plane – the knee over toe position – in the landing and maintaining stability for 3 s (figure 3A).

The examined exercises. (A) FJU, one-leg jump onto balance mat, LU, one-leg landing from box on balance mat, DJU, one-leg drop jump on balance mat, FJ, one-leg forward jump, SJ, one-leg side jump. (B) SPL, supine pelvis lifts, KS, two-hand kettlebell swings, NH, nordic hamstring lowers, SuLC, supine one-leg curls. (C) HE, hyperextensions off table, HEB, hyperextensions off table with barbell, RD, Romanian deadlift, SeLC, seated leg curl in Biodex isokinetic dynamometer, PrLC, prone leg curl in biodex isokinetic dynamometer.
One-leg landing from box on balance mat (LU)
The subject steps down from a 37.5 cm high box with a one-leg landing on a balance mat, focusing on a flexed hip and knee posture in the landing. The subject must focus on stabilising the knee in the frontal plane – the knee over toe position – in the landing and maintaining stability for 3 s (figure 3A).
One-leg drop jump on balance mat (DJU)
The subject ‘steps’ down on one leg from a 37.5 cm box onto a balance mat and immediately jump straight up as high as possible before finally landing again on the balance mat on the same leg. In the final landing, the subject must again focus on stabilising the knee in the frontal plane – the knee over toe position – in the landing and maintaining stability for 3 s (figure 3A).
One-leg forward jump (FJ)
The subject jumps forward focusing on stabilising the knee in the frontal plane – the knee over toe position – in the landing and maintaining stability for 3 s. The subject jumps backwards to the starting point focusing on knee stabilisation and balance (figure 3A).
One-leg side jump (SJ)
The subject stands on one leg and then jumps sideways between two fixed points focusing on stabilising the knee in the frontal plane – the knee over toe position – in the landing and maintaining stability for 3 s (figure 3A).
Strength exercises
Two-hand kettlebell swings (KS)
The kettlebell swing was performed with either a 12 kg or 16 kg kettlebell according to strength level of the respective subjects. The kettlebell weight corresponds to the weight the subject can swing 20 times with proper technique as described below.
The subject stands in front of the kettlebell with their feet parallel a shoulder width apart. By flexing the hips and knees while keeping the spine in a neutral position, the subject reaches down and grasps the kettlebell with both hands. The upper body is at this point is parallel to the floor and the knees are slightly flexed (∼10–15°). The subject forcefully swings the kettlebell back between the legs and quickly reverses the direction with an explosive extension of the hips swinging the kettlebell out to chest level where the hips and knees are extended and the subject is standing upright (figure 3B). Kettlebell swings (KS) exercise has been used to relief neck/shoulder and low-back pain among adults with musculoskeletal pain symptoms.17
Nordic hamstring lowers (NH)
The subject is kneeling on a balance mat while the partner holds the ankles. The subject leans the upper body slowly forward, using the hamstrings to resist falling forward as long as possible (figure 3B). Nordic hamstring lowers (NH) exercise is used both in ACL prevention programmes,2 and in hamstring injury prevention interventions.18 ,19
Supine one-leg curls (SuLC)
The subject is lying supine on the floor with the arms by their sides. The hips are extended and lifted off the floor and one leg is straightened. The other leg – which is the working leg – is kept on the floor with the foot on a carpet tile which can slide easily on the floor. The subject now slides the foot backwards and forwards (figure 3B).
Supine pelvis lifts (SPL)
The subject is lying supine on the floor with arms by the sides. The knee of the working leg is bent with the foot kept on the floor. The other leg is bent and crossed over the working leg. The hips are lifted off the floor until knees, hips and shoulders are in a straight line (figure 3B).
The supine pelvis lifts (SPL) and SuLC exercises are believed to strengthen and rehabilitate the hamstring and gluteus muscles, and are commonly used for patients with hip and knee injuries.12 ,16
Romanian deadlift (RD)
The subject is standing close to the barbell (weight corresponding to 12 RM) with the feet parallel a shoulder width apart. By flexing the hips and pushing them backwards while keeping the upper body straight, the subject reaches down and grasps the bar. At this point, the knees are slightly flexed (∼10–15°). The bar is lifted by extending at hips and knees until standing upright (figure 3C). Deadlift has been suggested as an effective closed kinetic chain exercise for strength athletes to be used during knee rehabilitation.20
Hyperextensions off table (HE)
The subject is placed prone with the legs fixated on a table and the hip and upper body off the table's edge. The body is lowered by bending the hip until a stretch is felt in the hamstrings. The upper body is raised again until the hip is fully extended and the upper body is kept straight throughout the entire movement (figure 3C).
Hyperextensions off table with barbell (HEB)
The exercise is performed as above but with a barbell (weight: 13.3 kg) placed in a wide grip in the hands for added resistance (figure 3C).
Seated leg curl (SeLC)
The subject is seated in a Biodex Medical isokinetic dynamometer (System 3 Pro, Brookhaven R&D Plaza) with 80° of flexion in the hip joint (refer figure 3C). With the back of her calf, she pushes against the padded arm of the dynamometer and performs maximal voluntary concentric contraction at 60° per second. The range of motion (ROM) is set at 80° starting from a 10° flexion in the knee to 90° flexion.
Prone leg curl (PrLC)
The subject is placed prone in a Biodex Medical isokinetic dynamometer (System 3 Pro, Brookhaven R&D Plaza) with no flexion in the hip joint (figure 3C). With the back of her calf, she pushes against the padded arm of the dynamometer and performs maximal voluntary concentric contraction at 60° per second. The ROM is set at 80° starting from a 10 degree flexion in the knee to 90° flexion.
The above mentioned strength exercises – hyperextensions off table (HE), seated leg curl (SeLC) and prone leg curl (PrLC) – are commonly used in resistance training by both novice and experienced individuals,21 as well as in rehabilitation after ACL injury.16
Statistical analysis
Before the main analyses, Shapiro-Wilk testing for normality was performed. For the hamstrings a two-way analysis of variance was performed in SAS (version 9, SAS Institute, Cary, North Carolina, USA) using the mixed procedure to determine whether differences existed in peak nEMG, and knee and hip joint angle at peak nEMG between exercises and muscles. Factors included in the model were muscle (ST and BF) and exercise (14 exercises), as well as the interaction between these. When a significant main effect was found, post hoc analyses were performed to locate differences between muscles, expressed as delta values (Δ). Intraday reliability was assessed by intraclass correlation coefficients (ICC).
The critical p value was set to 0.05.
A priori power analysis showed that 16 subjects in this paired design were sufficient to obtain a statistical power of 80% at a minimal relevant difference between exercises of 10% with an α level of 5%.22 Results are reported as group means (±SD) unless otherwise stated.
Results
Intraday reliability (ICC)
The intraday reliability of peak nEMG was calculated as ICC for the three attempts of each exercise, and ranged from 0.783 to 0.941 (p<0.05).
Level of hamstring muscle activation
Testing of main effects showed a significant effect of the type of exercise on nEMG (F=21, p<0.0001). For the BFcl high levels of muscle activation (ie, above 60% nEMG) were observed during – in ascending order – DJU, FJU, SPL, HE, NH, PrLC, KS, HEB, SeLC, SuLC.
For the ST, high levels of muscle activation were observed during – in ascending order – FJU, HE, RD, SPL, NH, PrLC, SeLC, HEB, SuLC, KS. Levels of muscle activation are summarised in table 1.
Peak normalised EMG (nEMG) activity of ST and BFcl and concomitant joint angles during the examined exercises. Expressed as mean (± SD). *Denotes significant difference between ST and BFcl, p<0.05
Medial-lateral hamstring activation balance
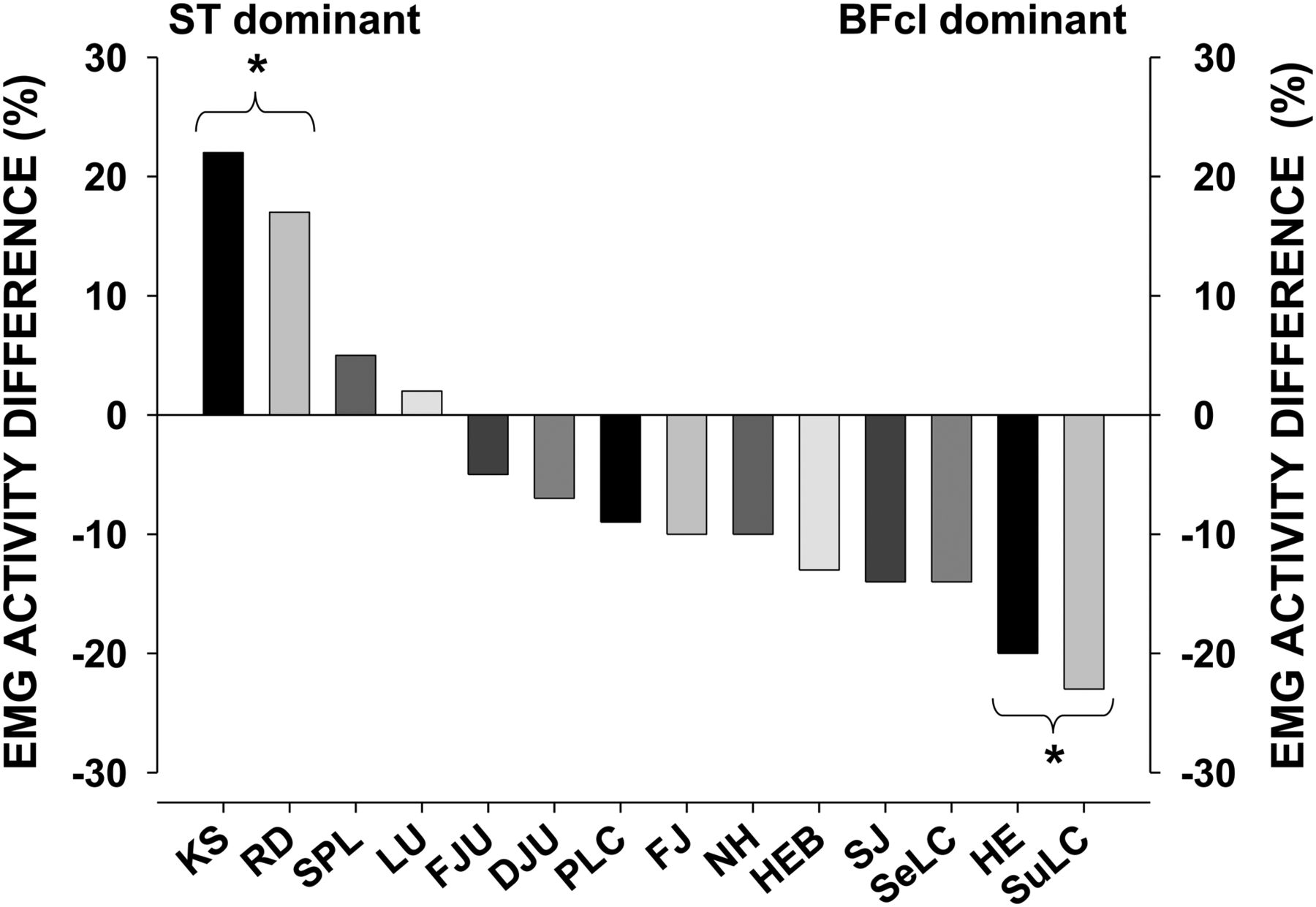
Testing of main effects showed a significant muscle by exercise interaction on peak nEMG (F=1.88, p<0.05). Post hoc analyses revealed a preferential activation of the ST over the BFcl (Δ±SD) during RD (Romanian Deadlift) (Δ 17.3±9.7% peak nEMG, p<0.05) and Kettle Ball Swings (KS) (Δ 22.5±9.7% peak nEMG, p<0.05). A preferential activation of the BFcl over the ST was observed during supine leg curl (Δ 22.9±9.4% nEMG, p<0.05) and hip extension (Δ 20.4±8.8% nEMG, p<0.05). For the remainder of exercises there was no significant difference between nEMG of the ST compared with the BFcl (figure 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Medial-lateral hamstring activation balance. *Denotes significant difference in activation of the semitendinosus and the biceps femoris muscle caput longus during Romanian deadlift (RD), kettlebell swings (KS), supine leg curl (SuLC) and hip extension (HE), p<0.05.
Knee and hip angles at peak nEMG
During the FJU and DJU exercises, peak normalised ST EMG occurred at a more extended knee joint angle compared with BFcl EMG (table 1). For the remainder of the exercises no significant differences in knee or hip joint angles at peak nEMG were observed.
Discussion
The main finding of our study was that specific therapeutic exercises targeting the hamstrings can be divided into ST dominant and BFcl dominant hamstring exercises.
KS and RD targeted the ST specifically and at intensity levels able to stimulate muscle strength gains.23 The ST dominance of the two exercises may partly be explained by the fact that ST is, in contrast to BFcl, parallel fibered with long-fibre lengths and a high number of sarcomeres in series. This arrangement increases the total shortening capacity and absolute velocity of contraction for the ST muscle.24 Thus the potential to shorten at long distances is excellent for the ST muscle. During execution of KS and RD, the hamstrings are extensively stretched with the highest load in the most stretched position – that is hip flexed. Thus, we recommend these exercises when aiming at enhanced ability to recruit ST during forceful movements. In respect to a transfer effect to real-life sports activity, the KS may be superior to RD, due to a high-velocity training component.
In contrast, the Supine Leg Curl (SuLC) and hip extension (HE) specifically targeted BFcl. Hamstring muscle strain injuries are common in sports involving sprinting and jumping.25 Exercises that mostly affect BFcl may be important in respect to prevention of hamstring muscle strain injury since most acute strains involve BFcl.26,–,28 The NH exercise has been shown to decrease the rate of overall, new and recurrent acute hamstring injuries,19 and has been established as an important prophylactic exercise.29 Muscle strain injuries most frequently occur during eccentric muscle contractions.30 Although the medial and lateral hamstrings were equally targeted during the Nordic Hamstring (NH) exercise, the muscles act solely eccentrically which makes this exercise particularly important in relation to prevention of strains.
Isolated leg curls using training machines are widely used and recommended in clinical rehabilitation after knee injury. Leg curl in a prone position (PrLC) has been reported to equally target the medial and lateral hamstring muscle, and the SeLC has been reported to specifically target the ST.31 ,32 Using a Biodex isokinetic dynamometer we did not detect any difference between the prone and seated leg curl (SeLC) in respect to the level of ST and BFcl activation. Thus, differences may exist between isokinetic and isotonic training devices.
The main purpose of the balance/coordination exercises is developing a proper technique in the one-legged landing phase. All the examined balance/coordination exercises displayed an equivalent degree of ST and BFcl activation, and may be proclaimed ‘universal’ hamstring exercises. Thus, the exercises may be important when aiming at establishing – and modifying existing – motor programmes. Although the latency of the ACL ligamentomuscular reflex arc (>100 ms) seems too long to provide a protective mechanism per se for the ACL in acute situations,33 afferent feedback from the ACL potentially plays an important role in the updating and formation of preprogrammed motor patterns for optimising knee joint stabilisation.34 Interestingly, two of the supervised balance/coordination exercises – FJU and DJU – displayed peak ST and BFcl nEMG at different knee joint angles. In respect to execution of the two exercises, ST EMG peaked at more extended knee joint angles – that is earlier in the landing phase – which may represent a protection mechanism against dynamic knee joint valgus. Thus, the present exercises may further optimise preprogrammed motor patterns in respect to the timing of neuromuscular activity. In fact, a re-programming of movement pattern and neuromuscular activity has been found due to coordination/balance and jump exercises,11 when performed as outlined in a study shown to reduce the incidence of ACL injury among female athletes.1
After ACL injury, the ligament is typically reconstructed by harvesting the ST tendon.35 Although the regeneration of the ST tendon has been confirmed in MRI studies, the volume of the ST in the reconstructed limb is significantly smaller than in the normal limb.6 Thus, atrophy and shortening of the ST after its tendon has been harvested, as well as insufficient compensation from the semimembranosus and biceps femoris, due to architectural and functional differences, makes it even more important, in terms of rehabilitating physical therapy, to introduce exercises with preferentially high levels of activation of the medial hamstring. However, to avoid adverse effects in the early phase of rehabilitation, caution must be taken when introducing high-intensity training among ACL reconstructed patients.
What this paper adds
-
The present study finds that specific therapeutic exercises targeting the hamstrings can be divided into semitendinosus dominant or biceps femoris dominant hamstring exercises.
-
Due to the distinct functions of the medial and lateral hamstring muscles, this is an important knowledge in injury prevention and rehabilitation programmes.
Limitations
One limitation of the present study is that the inherent variance in surface EMG measurements makes it difficult to evaluate small differences in muscle activity between exercises. Furthermore, as the present study evaluated the exercises among female athletes, we cannot conclude that the findings presented can be transferred directly to male athletes.
Conclusion
In conclusion, specific therapeutic exercises targeting the hamstrings can be divided into ST dominant (Kettleball Swing and Romanian Deadlift) or BF dominant (Supine Leg Curl and hip extension) hamstring exercises. In respect to the prevention of ACL injury, the ability to activate ST during forceful and explosive movements could be enhanced by ST dominant exercises like the KS. However, further research is needed to examine the transfer effect to real-life sports activity, and to test the efficacy of the exercises in the prevention of injuries.
References
Footnotes
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval The study was approved by the local ethical committee (HC2008103).
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
▸ References to this paper are available online at http://bjsm.bmj.com