Article Text

Abstract
Objective To determine the effectiveness of exercise and soft tissue massage either in isolation or in combination for the treatment of non-specific shoulder problems.
Methods Database searches for articles from 1966 to December 2011 were performed. Studies were eligible if they investigated ‘hands on’ soft tissue massage performed locally to the shoulder or exercises aimed at improving strength, range of motion or coordination; non-surgical painful shoulder disorders; included participants aged 18–80 years and outcomes measured included pain, disability, range of motion, quality of life, work status, global perceived effect, adverse events or recurrence.
Results Twenty-three papers met the selection criteria representing 20 individual trials. We found low-quality evidence that soft tissue massage was effective for producing moderate improvements in active flexion and abduction range of motion, pain and functional scores compared with no treatment, immediately after the cessation of treatment. Exercise was shown by meta-analysis to produce greater improvements than placebo, minimal or no treatment in reported pain (weighted mean=9.8 of 100, 95% CI 0.6 to 19.0) but these changes were of a magnitude that was less than that considered clinically worthwhile. Exercise did not produce greater improvements in shoulder function than placebo, minimal or no treatment (weighted mean=5.7 of 100, 95% CI −3.3 to 14.7).
Conclusion There is low-quality evidence that soft tissue massage is effective for improving pain, function and range of motion in patients with shoulder pain in the short term. Exercise therapy is effective for producing small improvements in pain but not in function or range of motion.
Statistics from Altmetric.com
Introduction
Shoulder pain is an important medical and socioeconomic problem in the western world, with between 7% and 26% of the population reporting shoulder problems at any one time.1 The presence of pain and stiffness in the shoulder can lead to an inability to work and/or to carry out domestic and recreational activities, thus creating a high burden of disease for both the individual and society. Information on the costs associated with healthcare use and loss of productivity in patients with shoulder pain is scarce but thought to be considerable.2 For many people, shoulder complaints are not self-limiting: almost 40% of patients who visited a general practitioner for shoulder pain reported complaints that had persisted for more than 12 months.3 Most shoulder pain experienced has no clearly defined pathology or physical signs and as such has been termed as ‘non-specific shoulder pain’.4
Up to 50% of patients with shoulder pain are referred to a physiotherapist for treatment.5 with soft tissue massage and exercise being the most common treatments. A recent study in the Netherlands found that therapists used soft tissue massage techniques to treat 91.6% of 119 patients with shoulder complaints, and exercise for 96.6% of patients. In 85% of cases, these treatments were used in combination.6 Similarly, a recent survey of experienced shoulder physiotherapists in Australia found that exercise was considered an essential component of effective treatment by 100% of respondents and soft tissue massage by 66%.7 Despite this, there has been no previous systematic review specifically investigating the effectiveness of soft tissue massage for the treatment of non-specific shoulder pain. A number of systematic reviews have evaluated the effectiveness of exercise for shoulder disorders3 ,8–19 with conflicting conclusions. None conducted a meta-analysis, which would provide an indication of the magnitude of the overall effect of exercise through statistically combining the effects of all studies.
The aim of this study, therefore, was to conduct a systematic review of the effectiveness of soft tissue massage and of exercise for non-specific shoulder pain when these interventions were compared with placebo, no treatment, another active treatment or when soft tissue massage or exercise were added as a supplement to other interventions. Meta-analysis was conducted where possible.
Methods
Criteria for inclusion of trials
To be included in the review, studies had to be randomised controlled trials reported in any language. Participants were adults with symptoms in the shoulder region that were labelled with the following diagnoses: rotator cuff tendonitis, rotator cuff tendinopathy, rotator cuff tear, impingement syndrome, bursitis, adhesive capsulitis, periarthritis and ‘frozen shoulder’. In addition, studies in which participants were not given a specific diagnosis but rather classified as having non-specific shoulder pain were included. Trials that included participants with the following diagnoses were excluded: infection, neoplasm, fracture, instability, dislocation, hemiplegia, postoperative or perioperative shoulder pain or inflammatory disease.
Treatments included were soft tissue massage or exercise, administered in isolation or in conjunction with other therapies. To be included in this review, trials of massage had to implement techniques aimed at the muscular structure and soft tissues local to the shoulder including applying fixed or movable pressure. Similarly, trials of exercise therapy had to include the performance of physical activity in order to improve health. This included therapeutic exercises that aimed to improve muscle strength, power, endurance, control, range of motion or flexibility, proprioception, cardiorespiratory fitness and tolerance to activity.
Measures of at least one of the following outcomes had to be reported: disability, pain, return to work, number of episodes, global perceived effect or health-related quality of life. To be included in the review, trials had to present sufficient data to be able to estimate effect sizes.
Identification and selection of trials
Searches were conducted of the electronic databases of MEDLINE (1966 to December 2011), EMBASE (1974 to December 2011), CINAHL (1982 to December 2011), SPORTDiscus (1800 to December 2011), Web of Science (to December 2011), EBM reviews (to December 2011) and PEDro (to December 2011). Terms for searches included a combination of subject headings and text words related to the domains of randomised controlled trials and shoulder pain as described by Green et al3 and Furlan et al20 Specific search terms based on Medical Subject Headings (MeSH) for this review are presented in Appendix 1. The protocol for this review was assessed externally and independently by a researcher not involved in this study.
Two reviewers independently screened search results for potentially eligible studies. Any disagreement on the inclusion of trials was resolved through consensus discussion. Researchers currently involved in the area were identified from bibiolographic searches as well as through the knowledge of the authors and were contacted to ensure that no trial had been missed by our searches. In addition, trial registers were checked to ascertain whether there were new trials currently being conducted or unpublished data. Citation tracking was performed by manually screening reference lists of eligible trials as well as reviewing reference lists from other systematic reviews evaluating the effectiveness of massage and exercise for the treatment of relevant shoulder pain.
Assessment of quality of the evidence
The GRADE (Grades of Recommendation, Assessment, Development and Evaluation) system for grading evidence for systematic reviews was used to evaluate the overall quality of the evidence and the strength of the recommendations.21 This system evaluates the quality of the evidence for a specific outcome based on five principal measures: (1) limitations (eg, study design), (2) consistency of results, (3) directness (eg, generalisability of the findings), (4) precision (eg, sufficient data) and (5) other considerations, such as reporting bias.
The overall quality of the evidence was considered to be high when randomised controlled trials with a low risk of bias demonstrate consistent, generalisable and precise results for a particular outcome.22 Single studies were considered to provide ‘low-quality evidence’ if associated with a low risk of bias or ‘very low-quality evidence’ if associated with a high risk of bias (table 1).
Levels of evidence21
Assessment of risk of bias of included studies
Two reviewers working independently (PV and either KMR or PHF) assessed the risk of bias and performed data extraction. Risk of bias was assessed using the criteria list advised by the Cochrane Back Review Group, which consists of 12 items evaluating internal validity. Items were scored as positive if they fulfilled the criterion, negative when bias was likely or marked as inconclusive if there was insufficient information. Differences in the scoring and data extraction were discussed during a consensus meeting. A study with a low risk of bias was defined as fulfilling six or more of the validity items.22
Analysis of effect size of treatment for individual trials
For continuous outcomes we extracted the mean and SD for the between-group difference of the end points.23 When dichotomous data were provided, relative risk was calculated.24 We used the formulae for binary and continuous data calculations described by Fleiss.25
Effect size for pooled estimates from multiple trials
When trials were considered sufficiently clinically and statistically homogeneous they were grouped according to treatment comparisons and outcomes (disability, pain, number of episodes, global perceived effect and return to work). Pooled estimates were obtained using a random effects model using RevMan 5 software.26 Pain, disability and quality-of-life scales were converted to 0–100 scales. Individual data were presented following the definition of short (≤3 months), intermediate (>3 and <12 months) and long-term (≥12 months) follow-up based on the proposal by the Cochrane Back Review Group.22
For shoulder pain, previous studies have demonstrated that the minimal clinically important difference in pain is around 14% improvement27 and at least 12% improvement for function.28 These figures were used in this review to determine whether any changes were of a magnitude considered to be clinically worthwhile for patients.
Results
Included trials
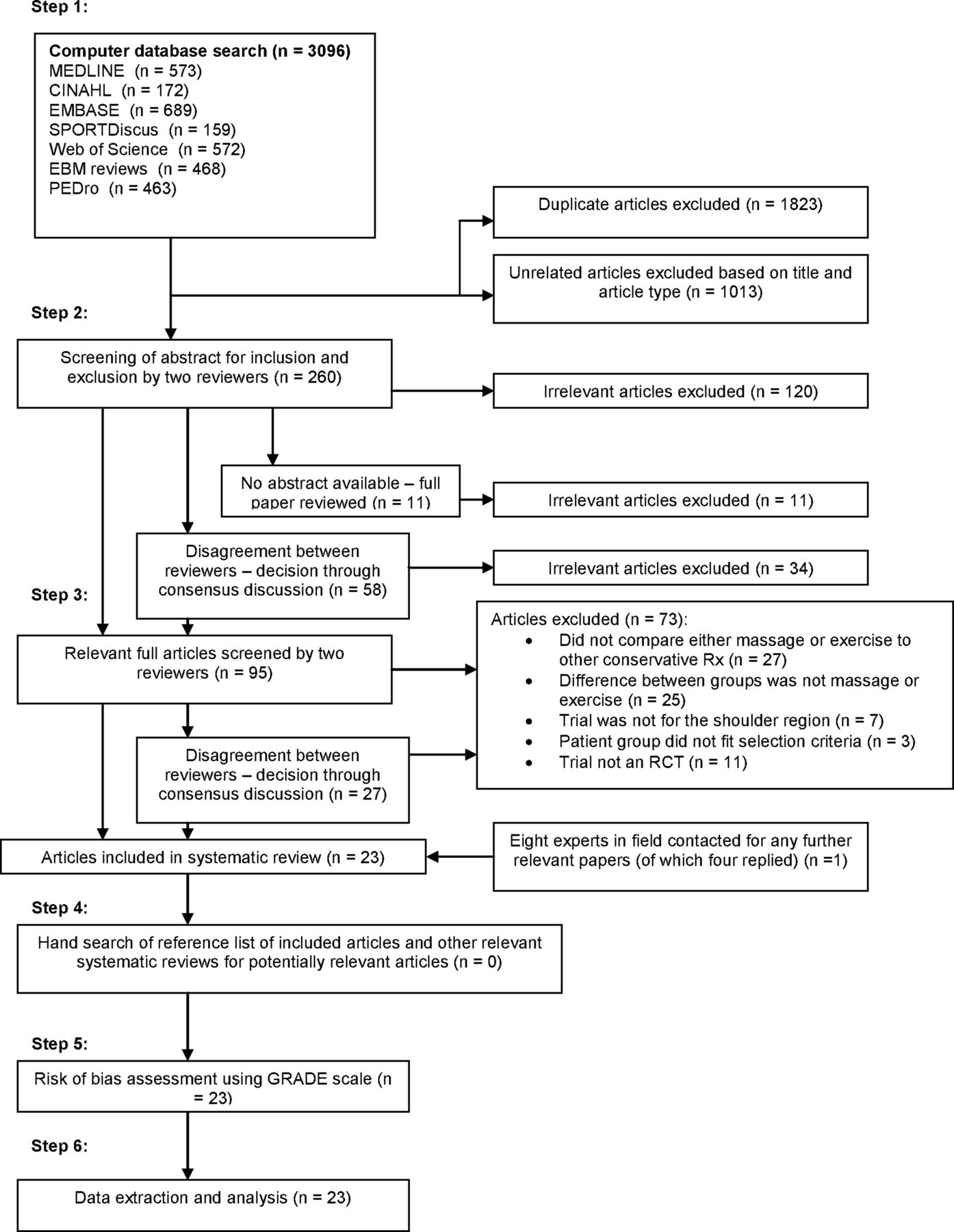
Database searches identified 3096 studies; abstracts of 260 studies suggested that 95 articles were potentially eligible for inclusion but only 23 met the inclusion criteria. Of the 23 included articles three sets of two articles shared data from the same trials giving a total of 20 discrete trials with sufficient data to estimate effect sizes (table 1). The most commonly assessed outcomes were pain (19 trials) and function (19 trials) although in three articles these outcomes could not be extracted from the global shoulder outcome measures used that combined pain, disability and range of motion scores. The process for inclusion into this study is summarised in the flow chart of the study selection according to the recommendations of the PRISMA statement29 in figure 1.

PRISMA statement of study selection process.
Risk-of-bias assessment
Risk-of-bias scores (table 2) ranged from 6 to 11 points out of a maximum of 12 points (mean±SD, 8.8±1.5; table 2). The most common risks of bias were failure to blind therapists (all 22 trials) which is expected in trials examining the effectiveness of hands-on therapy, failure to blind participants (18 trials) and failure to conceal allocation (11 trials). All trials scored more than 6, indicating low risk of bias.22 A summary of the trials investigating the use of soft tissue massage for the treatment of shoulder pain can be found in table 3, for exercise in supplementary table S1 and for soft tissue massage combined with exercise in table 4.
Risk-of-bias assessment
Summary of trials of soft tissue massage for the treatment of shoulder pain
Summary of trials of soft tissue massage and exercise combined for the treatment of shoulder pain
Effectiveness of soft tissue massage
Soft tissue massage versus no treatment
One study was located that compared massage with no treatment. This study, conducted by one of the authors (PV) of this paper (risk-of-bias score=9),30 delivered six treatments of soft tissue massage over 2 weeks to the lateral border of the scapula in end-of-range flexion, posterior deltoid in end-of-range horizontal flexion, anterior deltoid in end-of-range hand behind back and pectoralis major in the stretch position. This study found that soft tissue massage was more effective for improving active flexion (mean improvement 26.1°, 95% CI 10.8 to 41.4), pain (mean improvement 22.0 out of 100, 95% CI 2.8 to 41.2) and functional scores (mean improvement 24.0 out of 100, 95% CI 7.4 to 40.6) with greater effectiveness for improving active abduction (mean improvement 44.5°, 95% CI 25.1 to 63.7°) compared with no treatment (figure 2).

Forest plot of effect sizes of STM studies. ROM scores are in degrees except for Godges 2003 where flexion was measured in improvement in centimetre reached up a wall. Function and pain scores are out of 100. Figures are a comparison of scores at reassessment. The centre of each shape represents the mean with the size of the shape indicating relative size of the study population. Horizontal lines for each result indicate the 95% CI. PNF, proprioceptive neuromuscular facilitation; ROM, range of motion; STM, soft tissue massage.
In summary, based on the single study located with low risk of bias, there was low-quality evidence that soft tissue massage is effective for improving range of motion, function and pain immediately following treatment.
Soft tissue massage to the gleno-humeral region versus active controls
One study (risk-of-bias score=7)31 with 59 participants compared 15 sessions of sustained digital pressure to trigger points in supraspinatus, deltoid, infraspinatus and biceps tendon with sustained digital pressure to trigger points in the cervical and upper thoracic regions. The authors found improvements in combined pain and function scores in a combined pain and functional rating scale (mean improvement 41.5 out of 100, 95% CI 15.7 to 34.9).
Thus, there is low-quality evidence that soft tissue massage to the gleno-humeral region is more effective for improving combined pain and function than soft tissue massage to the cervical and upper thoracic region.
Another trial (risk-of-bias score=8)32 demonstrated that 2 weeks of Cyriax-type deep frictions and mobilisation to the supraspinatus and infraspinatus muscles failed to improve active flexion but improved external rotation (mean improvement 21.6°, 95% CI 9.3 to 33.9°), active internal rotation range of motion (mean improvement 10.6°, 95% CI 2.8 to 18.4) and pain on movement (mean improvement 12.1 out of 100, 95% CI 0.0 to 27.3) immediately after treatment compared to treatment of hot packs and short wave diathermy (figure 2).
In summary, there is low-quality evidence that Cyriax-type deep frictions and mobilisation in combination are effective for producing an immediate improvement in pain on movement, external and internal rotation range of motion but not flexion range of motion.
Effectiveness of exercise
Exercise versus no treatment/placebo
Eight papers33–40 investigated the use of exercise for the treatment of non-specific shoulder pain compared with no treatment or placebo treatment. Two of these papers33 ,34 (risk-of-bias score=9) described data from the same trial with 80 participants, resulting in six discrete studies35–41 (risk-of-bias scores 9, 10, 8, 7 and 6 respectively; participants range 9–77). Where there were common outcome measures between these studies and sufficient information was available, data were extracted to perform meta-analysis (figure 3). One study39 did not provide any measures of variability for the outcomes while another study40 did not report baseline measures and thus were both excluded from the meta-analysis.

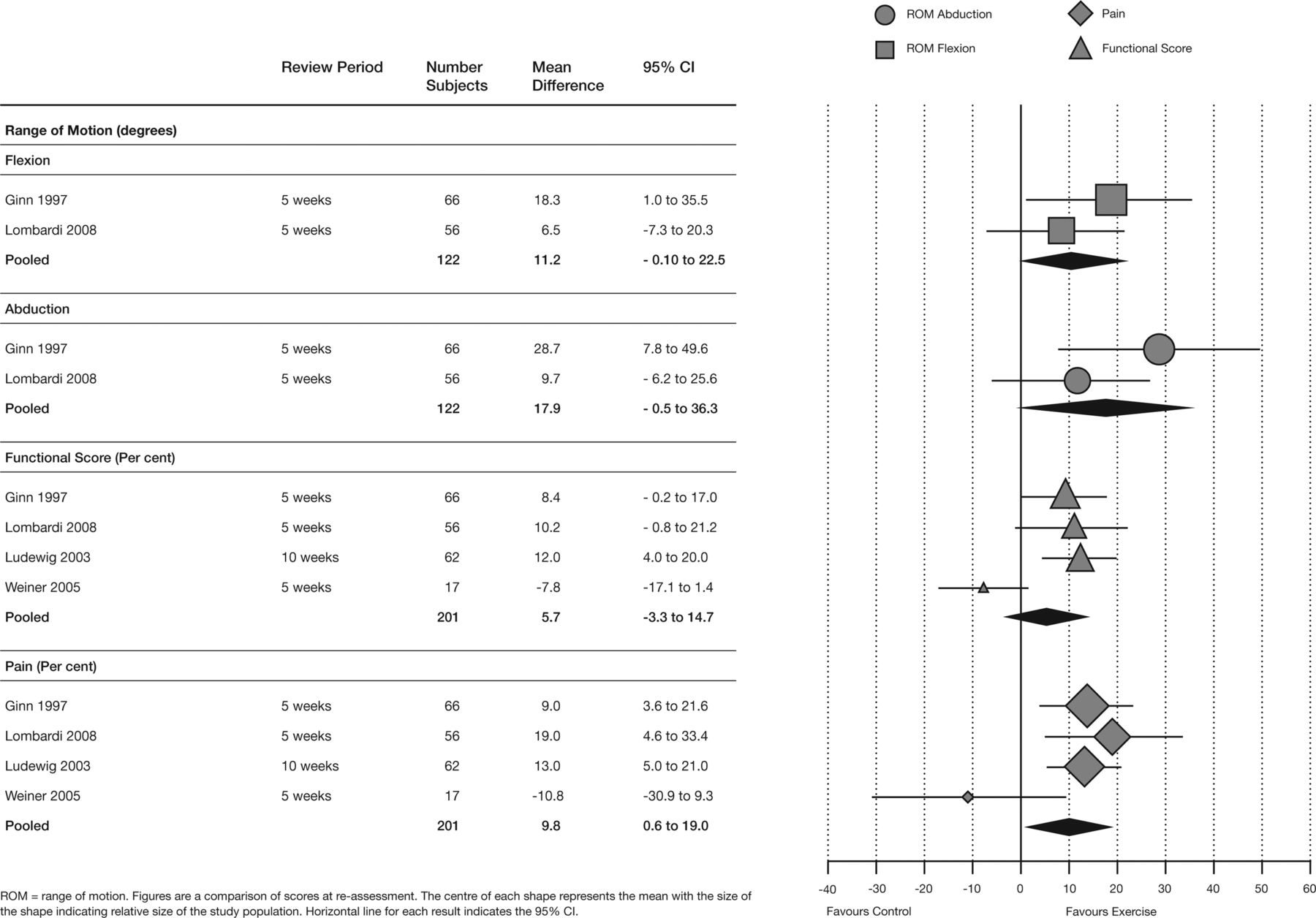
Exercise versus no treatment/placebo/minimal care—meta-analysis of improvements in the range of motion, functional scores and pain—immediate to short term. ROM scores are in degrees. Function and pain scores are out of 100. Figures are a comparison of scores at reassessment. The centre of each shape represents the mean with the size of the shape indicating relative size of the study population. Horizontal lines for each result indicate the 95% CI. ROM, range of motion.
Function
Six studies35–40 with low risk of bias investigated the effectiveness of exercise compared with no treatment, placebo treatment or minimal care for improving function in the immediate to short term. Two studies36 ,40 included their functional scores in overall measures of effectiveness, rendering extraction of these results impossible. Meta-analysis of the remaining four studies showed no statistical difference between exercise and the comparison intervention (pooled mean 5.7 points on a 100-point scale, CI −3.3 to 14.7) for improving function (figure 3).
Thus, there is high-quality evidence that exercise treatment is not effective for producing improvements in function compared to no treatment, placebo or minimal care in patients with non-specific shoulder pain.
Pain
Five studies35–39 with low risk of bias investigated the effectiveness of exercise for pain reduction immediately after treatment and in the short term. Data could not be extracted for one study: Walther et al38 provided data in a figure with no measure of variability. Meta-analysis demonstrated improvement in pain in the remaining studies (pooled mean 9.8 points on a 100 point scale, 95% CI 0.6 to 19.0) (figure 3). Thus, there is high-quality evidence that exercise treatment is effective for producing small improvements in pain in the short term compared to no treatment, placebo or minimal care for shoulder pain.
Range of motion
Four studies35–38 with low risk of bias investigated the effectiveness of exercise on pain in the immediate to short term. Data could not be extracted for two studies, one because mean pain data38 were provided in a figure only with no measure of variability, and the other35 because data were combined in a global rating scale and could not be extracted. For the two remaining studies36 ,37 meta-analysis was conducted on the common outcome measures of flexion (pooled mean 11.2°, 95% CI −0.1 to 22.5°) and abduction range of motion (pooled mean 17.9°, 95% CI −0.5 to 36.3°) (figure 3). Thus, there is high-quality evidence that exercise is not effective for improving range of motion in patients with shoulder pain compared to no treatment.
Exercise versus passive control
One trial, reported over two papers41 ,42 (risk-of-bias score=8), with 104 participants investigated the effects of a 12-week-graded exercise programme based on relearning normal movement patterns and endurance exercises compared with 4–6 weeks of physiotherapist administered extracorporeal shockwave treatment (figure 4). There was no difference between groups in outcomes for disability or pain between these two approaches at 6, 12 and 18 weeks and 12 months. Thus, there is moderate evidence that exercise therapy is no more effective for improving pain or function than extracorporeal shockwave therapy.
Forest plot of effect sizes of exercise studies. ROM scores are in degrees. Function and pain scores are out of 100. Figures are a comparison of scores at reassessment. The centre of each shape represents the mean with the size of the shape indicating relative size of the study population. Horizontal lines for each result indicate the 95% CI. PNF, proprioceptive neuromuscular facilitation; ROM, range of motion.
Exercise versus active control
One trial (risk-of-bias score=6)43 with 40 participants with shoulder impingement syndrome found no difference in reported pain or flexion, abduction, internal or external rotation range of motion between participants treated with hot packs and strengthening exercises and participants treated with either proprioceptive neuromuscular facilitation exercises or mobilisations to the shoulder (figure 4). Thus, there is low-quality evidence that exercises are not more effective than mobilisations or a combination of hot packs and theraband exercises for the treatment of shoulder impingement syndrome.
Another trial (risk-of-bias score=8)44 with 138 participants found no differences in either pain or functional scores between the use of a specific programme of exercises aimed at restoring dynamic stabilising mechanisms and coordination at the shoulder and a combination of physical modalities (electrophysical modalities, passive joint mobilisation and range of motion exercises) over a 5-week period (figure 4). Thus, there is low-quality evidence that exercises aimed at restoring dynamic stabilising mechanisms and coordination at the shoulder are no more effective than a combination of physical modalities.
Exercise and mobilisation versus no treatment
One study45 (risk-of-bias score=6) with 87 participants with idiopathic adhesive capsulitis were randomly allocated to either a group prescribed active exercises up to and beyond pain threshold, passive stretching and manipulation or to a no-treatment control group. At the end of 2 years, 89% of participants in the no-treatment group had normal or near-normal painless shoulder function (Constant score ≥80). In contrast, of the group receiving intensive physical therapy treatment, only 63% reached a Constant score of 80 or higher after 24 months.
Thus, there is low-quality evidence that no treatment provides better outcomes in patients with adhesive capsulitis than intensive exercise and mobilisation.
Behavioural approach graded exercise programme versus active control
One study, reported in two papers (risk-of-bias score=1046 ,47) with 176 participants with chronic shoulder complaints (>3 months) demonstrated that an operant behavioural and time-contingent graded exercise therapy programme designed to improve functional ability irrespective of pain provided no additional improvement in self-rated functional ability, perceived recovery, reported pain or quality of life at either 12 weeks or 1 year when compared to usual care from the patient's general practitioner (figure 4). There is, therefore, low-quality evidence that a graded exercise programme does not offer additional benefits to usual care from a general practitioner for the management of chronic shoulder pain.
Effectiveness of soft tissue massage and exercise versus no treatment
One trial (risk-of-bias score=7)48 found improvements in active external rotation range of motion (mean improvement 15.5°, 95% CI 12.0 to 19.0) but no improvement in forward reach up a wall following a single treatment of soft tissue mobilisation to the subscapularis and proprioceptive neuromuscular facilitation exercises for the shoulder rotators when compared with a no-treatment control group.
Thus, there is low-quality evidence that soft tissue massage combined with proprioceptive neuromuscular facilitation exercises improves external rotation range of motion but not forward flexion.
Effectiveness of soft tissue massage and joint mobilisation and exercise versus active control
One trial49 (risk-of-bias score=6) with 77 participants found no differences in night pain, rest pain or pain with movement, reported function or strength between a supervised exercise programme combined with joint and soft tissue mobilisation, supervised exercise in isolation or a home-based rehabilitation programme at either 4 or 12 weeks follow-up.
Thus, there is low-quality evidence that soft tissue massage in combination with joint mobilisation and exercise does not result in improvements in pain, reported function or strength compared with exercise alone.
Effectiveness of soft tissue massage and multimodal treatment versus placebo
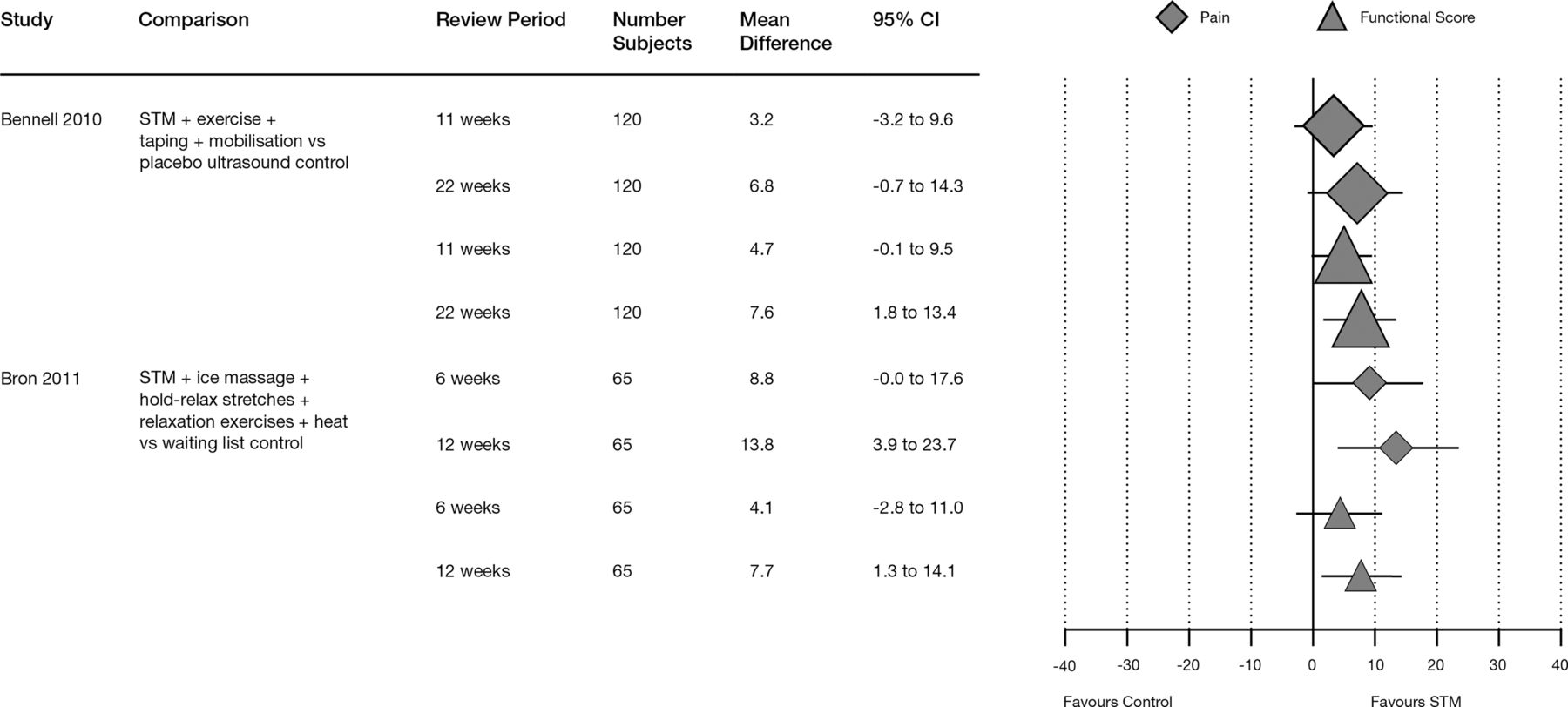
Two studies50 ,51 with low risk of bias were identified that investigated the effects of soft tissue massage combined with exercise approaches in combination with other physical modalities.
One study50 (risk-of-bias score=11) with 120 participants examined the effectiveness of soft tissue massage, scapular retraining, postural taping, gleno-humeral mobilisation and home exercises for the treatment of non-specific shoulder pain compared to placebo ultrasound over a 10-week period. The patients in this study had chronic shoulder pain, with those in the massage group having pain for a median of 24 months (IQ range (IQR) 6–54) and 14 months (IQR 6–24) in the placebo group. At 11 weeks, no difference was found between groups for either change in shoulder function or pain. At 22 weeks follow-up there was a statistically significant improvement in function in favour of soft tissue massage and exercise combined (mean improvement 7.6 of 100, 95% CI 1.8 to 13.4). There was no change at 22 weeks for pain (figure 5).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot of effect size of STM and exercise combined studies. Function and pain scores are out of 100. Figures are a comparison of scores at reassessment. The centre of each shape represents the mean with the size of the shape indicating relative size of the study population. Horizontal lines for each result indicate the 95% CI. STM, soft tissue massage.
Another study51 (risk-of bias score=10) with 65 participants investigated the effectiveness of manual compression on trigger points along with deep stroking massage, ice massage, hold-relax stretches, stretches, relaxation exercises and home heat packs compared with no treatment for 12 weeks. At the end of the treatment period, pain (mean improvement 13.8 of 100, 95% CI 2.6 to 25.0) and function (mean improvement 7.7 of 100; 95% CI 1.2 to 14.2), were significantly improved in the treatment group (figure 5).
In summary, there is high-quality evidence that soft tissue massage in combination with exercise, passive joint mobilisation and other physical modalities results in small improvements in function with conflicting evidence concerning improvements in pain compared with no treatment or placebo.
Discussion
There is low-quality evidence that soft tissue massage is effective for improving the range of motion, function and pain in patients with non-specific shoulder pain immediately following treatment. Exercise approaches in the treatment of non-specific shoulder pain improve pain immediately following treatment and in the short term although this change does not appear to be clinically worthwhile. Exercise does not improve reported function or range of motion.
This review is the first to specifically examine the effectiveness of soft tissue massage for the treatment of non-specific shoulder pain.52 We found that there were very few trials in this area with all these trials having small sample sizes and short follow-up period. The greatest improvements with soft tissue massage, targeted treatment towards the lateral border of the scapula in end-of-range flexion, the posterior deltoid region in end-of-range horizontal flexion, anterior deltoid in end-of-range external rotation (measured as hand behind back) and pectoralis major in the stretch position.30 This demonstrated moderate improvements in active flexion (mean improvement 22.6°) and abduction (mean improvement 42.2°) ranges of motion, pain levels (mean improvement 26.5 mm on a 100 mm visual analog scale) and functional scores (mean improvement 28.7%). Soft tissue massage is also effective for improving external range of motion in patients with adhesive capsulitis. Thus, soft tissue massage techniques are able to produce clinically significant improvements in patients with non-specific shoulder pain in the short term and should be considered as an important form of therapy. No reports of adverse effects of soft tissue massage treatment could be found.
The studies utilising soft tissue massage included in this review described a range of techniques including stroking massage, trigger point therapy and ice massage. It is difficult to demonstrate how these techniques differ from each other, and indeed how they may differ from other techniques, such as manual therapy, as some authors have suggested.53 Further research into the similarities or differences between these techniques and the structures they may affect would be beneficial to therapists.
This review is the first to pool the results of exercise studies for the treatment of non-specific shoulder pain in a meta-analysis. This demonstrated that exercise produces changes in pain of a magnitude less than that considered to be clinically worthwhile by patients (mean pain improvement 9.8 of 100). Meta-analysis did not demonstrate that exercise was effective in producing changes in either self-reported functional scores or flexion or abduction range of motion. On the basis of the trials available, we found no evidence that exercise therapy is harmful or that it provoked harmful side effects. However, these trials provided little or no information on the safety aspects of exercise therapy. This may represent inadequate reporting of adverse effects. Generally, the trials provided poor description of specific exercise approaches and intensity of training; however, the greatest improvements in pain were demonstrated through the application of a strengthening exercise regimen focusing on flexion, extension, and internal and external rotation which was carried out twice weekly for 8 weeks up to 70% of the patient's six repetition maximum threshold.38 This higher level of exercise dose concurs with a recent study54 which demonstrated that high-dose exercise regimens were superior to low-dose exercise regimens for improving both pain and function in patients with subacromial pain. Other approaches that employed specific stretches to shortened muscles around the glenohumeral joint and moderately high-intensity strengthening exercises in multiple planes of motion for muscles assessed as being weak36 ,37 demonstrated improvements in flexion and abduction range of motion but no changes in functional scores and small improvements in pain scores when compared with no treatment. This effect was not seen when the same exercise approaches were compared to a combination of electrophysical modalities, passive joint mobilisations and range of motion exercises.
From this review it still remains unknown as to whether exercise therapy should be included in a supervised or an unsupervised programme or a combination of the two. More research is also needed to investigate how the short-term effectiveness of exercise therapy can be maximised or how it can be maintained in the long-term. Programmes or methods with which clinicians could encourage greater compliance with home exercises and motivate them to continue their exercises into the future would also be very useful. Further studies examining the effectiveness of both soft tissue massage and exercise with longer follow-up periods and larger participant numbers would assist in strengthening the work in this area. Clearer description of treatment approaches would also be beneficial.
Conclusion
Soft tissue massage to the gleno-humeral musculature appears to be effective for improving pain, function and range of motion in patients with non-specific shoulder pain in the short term. Strengthening exercises are effective for producing small changes in pain but not function or range of motion. The most effective exercise therapy included high-dose strengthening exercises in multiple planes of motion. Including soft tissue massage in a treatment programme for non-specific shoulder pain will improve the range of motion and pain.
What is known about this topic
-
Between 7% and 26% of the population have shoulder pain at any one time.
-
Almost 40% of patients who visited a general practitioner for shoulder pain reported complaints that had persisted for more than 12 months.
-
Up to 50% of patients with shoulder pain are referred to a physiotherapist for treatment. Soft tissue massage and exercise are the most common treatments.
-
A number of systematic reviews have evaluated the effectiveness of exercise for shoulder disorders with conflicting conclusions. None have conducted a meta-analysis.
-
No systematic review has specifically evaluated the effectiveness of soft tissue massage for shoulder disorders.
What this study adds
-
This study is the first systematic review to specifically examine the effectiveness of soft tissue massage for non-specific shoulder pain.
-
This is the first systematic review of the effectiveness of exercise for treatment of shoulder pain that has conducted a meta-analysis.
-
There is low-quality evidence that soft tissue massage is effective for improving pain, function and range of motion in patients with shoulder pain in the short term.
-
Exercise therapy is effective for producing small improvements in pain but not in function or range of motion.
Acknowledgments
The authors would like to acknowledge ProfessorRobert Herbert for his assistance in the design of this systematic review.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix
- Data supplement 2 - Online table
Footnotes
-
Contributors PV and KMR had the idea for the article. PV performed the literature search and wrote the article. KMR and PHF independently rated articles for the review and provided guidance and editing. KMR is the guarantor for the article.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement Data extracted from the articles included in this systematic review (means and measures of variability) is available to interested researchers on request by contacting the corresponding author, PV at pvan0651@uni.sydney.edu.au.