Article Text

Abstract
Background Adductor-related groin pain and bony morphology such as femoroacetabular impingement (FAI) or hip dysplasia can coexist clinically. A previous randomised controlled trial in which athletes with adductor-related groin pain underwent either passive treatment (PT) or active treatment (AT) showed good results in the AT group. The primary purpose of the present study was to evaluate if radiological signs of FAI or hip dysplasia seem to affect the clinical outcome, initially and at 8–12 years of follow-up.
Methods 47 patients (80%) were available for follow-up. The clinical result was assessed by a standardised clinical outcome combining patient-reported activity, symptoms and physical examination. Anterioposterior pelvic radiographs were obtained and the centre-edge angle of Wiberg, α angle, presence of a crossover sign and Tönnis grade of osteoarthritis were assessed by a blinded observer using a reliable protocol.
Results No significant between-group differences regarding the distribution of radiological morphologies were found. There was a decrease over time in clinical outcome in the AT group with α angles >55° compared to those with α angles <55° (p=0.047). In the AT group, there was no significant difference in the distribution of Tönnis grades between hips that had an unchanged or improved outcome compared with hips that had a worse outcome over time (p=0.145).
Conclusions No evidence was found that bony hip morphology related to FAI or dysplasia prevents successful outcome of the exercise treatment programme with results lasting 8–12 years. The entity of adductor-related groin pain in physically active adults can be treated with AT even in the presence of morphological changes to the hip joint.
- Groin injuries
- Hip disorder
- Exercise rehabilitation
Statistics from Altmetric.com
Introduction
Groin pain in athletes has been the subject of attention for many years in sports medicine and sports orthopaedics, causing problems in terms of diagnosis, treatment and prevention.1–4 In the traditional perception of groin pain, the anatomical structures considered to be the cause of pain in connection with sport and other types of physical activity are the muscles, tendons, pubic bone and nerves of the groin region.2 ,4–6 During the past decade, the concept of femoroacetabular impingement (FAI) has been refined7 ,8 and the mechanisms of damage to the labrum and cartilage are now considered as additional sources of groin pain and potential joint deterioration in young, physically active patients. In the literature, there is evidence that a pathological centre-edge (CE) angle (less than 25° or above 40°) and morphology causing FAI are significant risk factors for developing early osteoarthritis.9 ,10
Adductor-related groin pain is a well-established entity and a major cause of groin pain in athletes.1 ,4 ,11–16 The coexistence of adductor-related groin pain and bony morphology/pathology such as FAI or hip dysplasia has been demonstrated in previous studies.14 The possible negative influence of hip joint pathology on the treatment outcome in adductor-related groin pain, both in the short term and the long term, is not well understood.
The present study reports the 8–12 years of follow-up of patients included in a level 1 trial on the treatment of long-standing adductor-related groin pain.17 In this randomised controlled trial (RCT), an active treatment (AT) programme consisting of strength training of the adductors, abductors, low back and abdominal muscles in combination with balance and coordination exercises showed significantly better results than traditional passive treatment (PT) without any active training component, in the treatment of long-standing adductor-related groin injuries in athletes. Seventy-nine per cent of athletes who underwent AT could return to their previous level of sport without any groin pain, compared with only 14% in the control group. An 8–12 years of follow-up study found the beneficial short-term effect of the exercise programme used in the original study to be lasting both for the group as a whole and particularly for the large subgroup of soccer players.18 As this study was started in the early 1990s, before specific examination and treatment methods for FAI and hip dysplasia were standard procedure, diagnostic criteria and methods establishing these diagnoses were not included in the index study. Before inclusion in the RCT, the participants were examined radiologically for osteoarthritis, but not evaluated for FAI and hip dysplasia.
The primary purpose of the present study was therefore to use a descriptive and exploratory approach to evaluate if radiological signs of FAI or dysplasia in the original material seem to affect the clinical outcome, initially and at 8–12 years of follow-up.
Material and methods
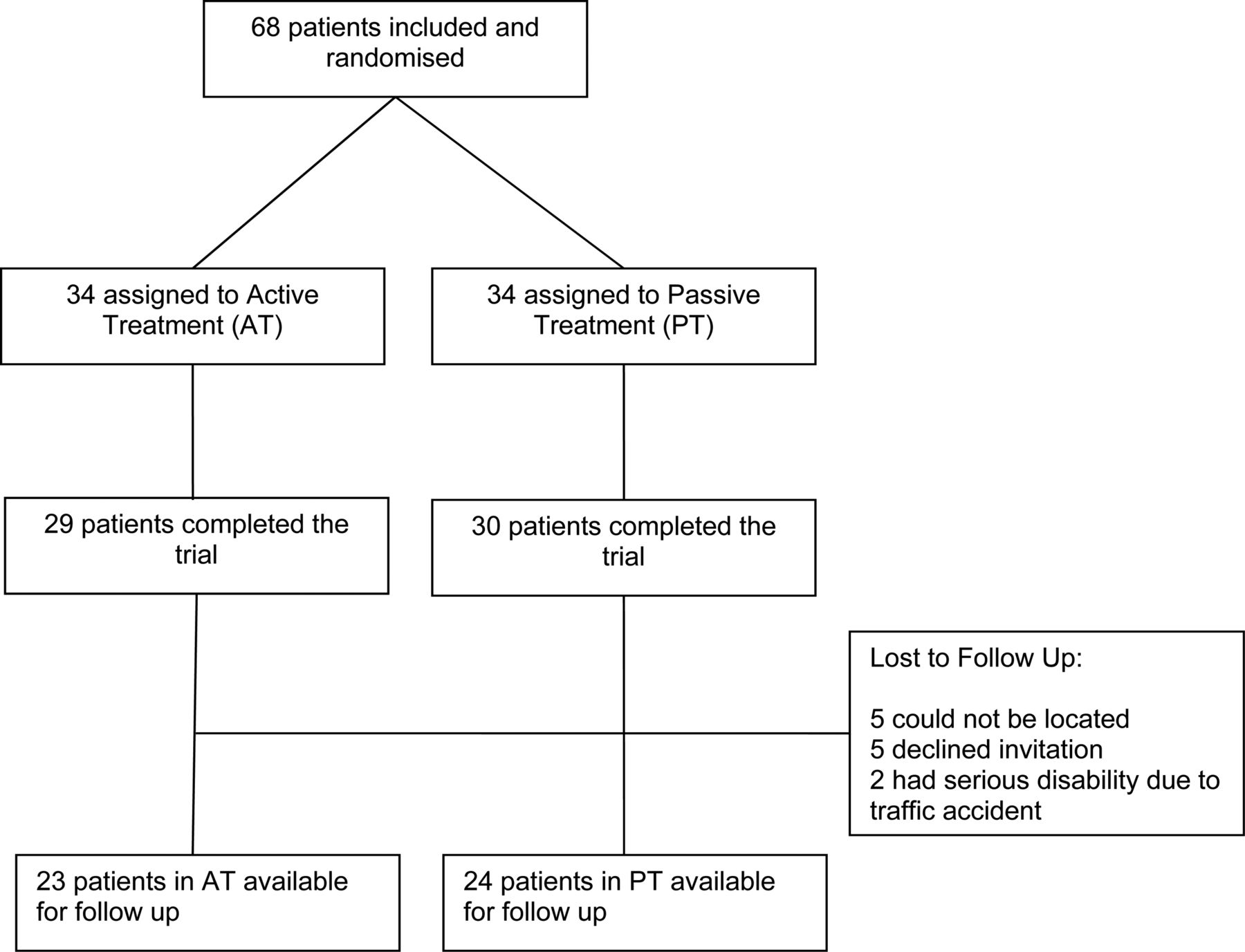
In total, 68 patients included in the original study were all diagnosed with adductor-related groin pain from a set of standardised defined criteria.4 They had groin symptoms for a median of 9 months and 72% had ceased to participate in sports because of the groin pain.17 Of the 59 participants who were assessed for follow-up in the original study, five could not be located. A letter was sent to the remaining 54 persons inviting them to participate in the follow-up study at a median of 10 years after they had participated in the RCT. All of them responded: five were unwilling to participate and two could not participate because they had suffered serious disability due to different accidents. This left a study group for the long-term follow-up of 47 patients (figure 1).
{kind=link}
Consort flow diagram.
The follow-up study was designed using the model of the index study including the standardised self-report and physical examination, as well as a weight-bearing anteroposterior (AP) pelvic radiograph. The investigating physician (PN) was not involved in the original study and was unaware of the original treatment allocation. Prior to the study, all participants were informed in writing not to disclose to which treatment (AT or PT) they were allocated in the original study. On arrival at the physician's office, the participants were again reminded not to reveal this information to the examining physician.
The investigating physician conducted an interview and a questionnaire was completed obtaining information regarding the former and present state of athletic activity, occupational status and demographic data. The questionnaire was designed following the same concept of data collection as in the index study, also seeking relevant information regarding any reduction in sports activity from the time of the index study to the follow-up study and the reasons for this (table 1). No information was sought regarding whether the participants had received any additional treatment during the time since the initial study.
Baseline characteristics of the participants in the AT and PT groups at follow-up
Clinical outcome assessment
All participants were examined using a standardised and reproducible clinical examination protocol, identical to the one used in the original study.17 Prior to the study, the examining physician received specific training in performing the physical examination.18
The primary outcome used in the original study17 evaluating the clinical status of the patients was also used in the present study. The outcome was defined as excellent if the following three criteria were met: (1) no pain at palpation of the adductor tendons and the adductor insertions at the pubic bone and no pain during active adduction against resistance; (2) no groin pain in connection with or after athletic activity in the same sport and at the same level of competition as before the onset of groin pain and (3) return to the same sport and at the same level without groin pain. If two criteria were met, the result was good; if one criterion was met, the result was fair and if no criteria were met, the result was poor.
Return to the same sport and at the same athletic level without groin pain was one of the criteria used in the clinical outcome assessment. The median age at the time of enrolment in the original study was 30 years. Most of the participants in both treatment groups had reduced their athletic activity at the time of follow-up (measured as how many times a week they participated in the sport). The main reason for athletic level reduction was either age or lack of time (table 1). The majority of participants were athletically active on average at one level below their level at the time of the original study and mostly in the same sport that caused the groin injury. The outcome assessment was adjusted accordingly in the follow-up study, decreasing the demand for return to the same level of sport to one level below the original level.
Radiological assessment
A weight-bearing AP pelvic radiograph was recorded at the time of the original examination and at follow-up.19 In two patients from the PT group, the follow-up radiographs were not recorded. The following radiographic parameters were assessed in all hips: the CE angle of Wiberg,20 the α angle,21 the presence of a crossover sign22 and the Tönnis grade of osteoarthritis.23 On the weight-bearing AP pelvic radiographs taken at follow-up, the Tönnis grade of osteoarthritis was assessed.
All the radiographic parameters were assessed by one observer (AT) who was blinded to which sides were affected as well as to the allocation in the RCT. Measurements of the CE angle and the α angle were performed using the angle measurement and circle drawing tools of the Synedra software (Synedra View Personal V.3, Synedra information technologies GmbH). In a subset of 25 pelvic radiographs (50 hips), the CE angle and α angle were read by another blinded observer (JK) and the interobserver variability was assessed. The mean difference of assessed CE angles measured in degrees was −0.4 (SD 1.5) with 95% limits of agreement from −3.3 to 2.5, and the mean difference of assessed α angles measured in degrees was −0.6 (SD 2.6), with 95% limits of agreement from −5.8 to 4.6.24
Femoral head asphericity as seen in cam deformity is in this study defined by the cut-off values of the α angle of 55° and 69°, respectively. Generally, an α angle <55° is considered normal; however, an α angle >69° has been suggested as the cut-off defining definite bony pathomorphology when evaluated on the AP pelvic radiograph. Both the group with α angles> 55° and the group with α angles> 69° are analysed. There is no evidence that an α angle >55° is a valid measure of cam pathology on AP conventional radiographs but only on MRI, however, we chose to analyse this group as well as the concept of an α angle >55° being a sign of cam impingement is commonly adapted among hip arthroscopy surgeons.21 ,25 The crossover sign is present upon crossing of the anterior end posterior acetabular rims assessed on the AP pelvic radiograph.22 A pathological CE angle is defined as less than 25° or above 40°.20
Statistical methods
Both the data manager and the statistician were unaware of treatment allocation.
Data that are normally distributed are presented as mean values with ranges, and comparisons between groups are made using a two-sample t-test. Data that are not normally distributed are presented as median values with ranges, and comparisons between groups are made using the two-sample Wilcoxon rank-sum (Mann-Whitney) test. Binomial data are presented as proportions, and comparisons made by Fisher's exact test where appropriate. Interobserver variability was assessed according to the Bland-Altman method and presented as difference of the mean and 95% limits of agreement.26 ,27 p Values <0.05 are considered statistically significant. Statistical analysis was performed using the STATA statistical package, V.10.1 (College Station, Texas, USA).
Results
Distribution of radiographic signs between the groups
The radiographs from the primary examination in the index study showed no significant difference between the two treatment groups regarding the CE angle, α angle, presence of crossover sign or Tönnis grade (tables 2⇓⇓–5).
Distribution of α angle in the AT and PT groups
Distribution of CE angle in the AT and PT groups
Number of patients with the presence of a crossover sign in the AT and PT groups (the crossover sign could not be measured in one patient in both groups)
Distribution of Tönnis grade in the AT and PT groups at the time of RCT and of follow-up
Of the 14 patients with a pathological CE angle, one had a pathological α angle and none had a crossover sign (table 3).
Effect of radiographic signs on outcome
The distribution of Tönnis grades of osteoarthritis did not differ between the two groups at follow-up (table 5). A total of seven patients (n=47) developed an increase of 1 in the Tönnis grade (table 5).
No development of the Tönnis grade was seen in the 14 patients with a pathological CE angle. Three in the AT group went down 1 level in the clinical outcome and one in the PT group had a poor clinical result and did not improve with time. There was no significant difference in the distribution of Tönnis grades between hips that stayed unchanged or improved and hips that decreased in outcome score within the AT group (table 6).
Changes in the outcome score related to Tönnis grade in the AT group (n=24)
The four patients with an α angle >69 in the AT group had excellent (three patients) or good (one patient) outcome scores after the RCT and their result did not differ from the other 20 patients in the AT group with an α angle <69 (p=0.84). In the AT group, the proportion of patients with a decrease in the overall outcome was significantly higher for patients with an α angle >55° compared with patients with α angles <55° (p=0.047; table 7).
Changes in the outcome score related to α angle in the AT group (n=24)
Discussion
In this cohort of patients with long-standing adductor-related groin pain, we find no evidence that any coexistence of morphological changes in the hip joint prevents a successful result of an exercise treatment programme. Our findings at follow-up indicate that the statistically significant decrease in overall outcome for patients with an α angle >55° is worse when compared with patients with α angles <55° in the group that received the active treatment.
The present study includes athletes with long-standing adductor-related groin pain, which involves patients with symptoms from the adductor longus muscle insertion at the pubic bone. Some of these patients also have radiographic hip joint-related morphological varieties, such as FAI (cam type deformity) and hip dysplasia. They could, as such, be evaluated as ‘hip joint patients’ rather than ‘adductor-related patients’, and one could consider treatment of the bony morphology. This study demonstrates that when the clinical entity of adductor-related groin pain is diagnosed4 and the patient is treated with an exercise programme,17 we find in retrospect no indication of bony morphologies having had any negative influence on the outcome. In other words, it seems possible to treat a muscle tendinous problem in the hip and groin region successfully even in the presence of radiographic signs of hip joint morphological varieties. We found no difference in distribution of the radiographic findings between the two treatment groups, supporting the theory that it was the treatment only that was responsible for the excellent result of the active treatment in the original study.
There did not seem to be any signs that the surgically untreated FAI or pathological CE angle led to the increased development of osteoarthritis during the observation period (8–12 years) in any of the treatment groups (table 4). In the literature, there is evidence that a pathological CE angle (less than 25° or above 40°) and morphology causing FAI are significant risk factors for developing early osteoarthritis.9 ,10 This increased risk of osteoarthritis is probably a result of injuries to the labrum and/or the cartilage of the hip joint. The lack of osteoarthritis development in the current study could reflect that the morphological changes as seen on the radiographs did not result in intra-articular cartilage or labral injuries, and that the symptoms in the original study were related to the extra-articular injuries. The observation time being too short could also be an explanation. The increase seen in the Tönnis grade could, on the other hand, be a reflection of the expected age development. The median age of 42.5 years and the range up to 62 years of the patients at the time of follow-up are factors where one would expect early radiologically verified osteoarthritis to appear.
The slight reduction of the clinical result at follow-up in the group with an α angle >55° seen in the AT group could be a reflection that FAI has resulted in an injury to the joint. Another possibility is that the range of motion restrictions due to FAI creates compensatory patterns that affect extra-articular pelvic structures and could lead to the development of muscle and tendon overload, such as long-standing adductor-related groin pain. 1 ,28 The decrease in range of motion (ROM) that is commonly seen with FAI29 could during sports, especially those with cutting activities, lead to altered recruitment of the muscles and in turn to overuse and an increased risk of injury. A similar analysis was not meaningful in the PT group because of the poor clinical outcome resulting in a floor effect.
The low number of patients and the lack of precise and controlled knowledge of the participants’ activities and additional treatment or crossover between groups during the follow-up period regarding physical activity are the limitations to this study. Information regarding this was not sought since this would be susceptible to reporting bias. The study was not originally designed for examining the possible radiological hip joint morphology and its impact on the result of the exercise treatment. The study is, however, based on a prospective randomised design with blinded independent examiners and a systematic, reproducible and standardised clinical and radiological evaluation.
Conclusion
In this descriptive and exploratory study of a well-defined cohort of patients with long-standing adductor-related groin pain, we find no evidence that the coexistence of bony morphological changes related to FAI or dysplasia prevents the successful outcome of an exercise treatment programme. The findings at follow-up indicate that the presence of an α angle above 55° reduces the clinical result at long-term follow-up in the group receiving the active exercise treatment. There were no signs that a surgically untreated FAI or CE angle led to increased osteoarthritis during the observation period (8–12 years). The entity of adductor-related groin pain in younger physically active adults continues to be a relevant entity for treatment even in the presence of morphological changes to the hip joint.
What are the new findings?
-
It is possible to achieve good results with an exercise programme for adductor-related groin pain in spite of the coexistence of bony morphological changes related to femoroacetabular impingement (FAI) or dysplasia.
-
The presence of an α angle >55° affects the long-term outcome of the results achieved from the exercise treatment of adductor-related groin pain.
-
A surgically untreated FAI or centre-edge angle did not lead to increased osteoarthritis during the observation period (8–12 years) in any of the treatment groups.
How might it impact on clinical practice in the near future?
-
The entity of adductor-related groin pain in physically active adults continues to be a relevant entity for treatment even in the presence of morphological changes to the hip joint.
-
The extra-articular causes of groin and hip pain should be taken into consideration when considering the indication for surgical treatment of the hip joint in the non-arthritic hip.
Acknowledgments
The authors gratefully acknowledge the help of Dr Anna Rosted from the Radiology Department of Amager Hospital in organising the additional pelvic X-rays for the follow-up examination. We thank Dr Adam Weir for his valuable help in editing the language.
References
Footnotes
-
Contributors All authors have substantially contributed to the conception and design, analysis and interpretation of data and drafting of the article or revising it critically for important intellectual content and final approval of the version to be published.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Ethics Committee of Copenhagen County, Denmark.
-
Provenance and peer review Not commissioned; externally peer reviewed.