Article Text

Abstract
Aim To determine whether rotator cuff strength, glenohumeral joint range of motion and scapular control are associated with shoulder injuries among elite male handball players.
Methods A total of 206 players in the Norwegian elite handball league for men were tested prior to the 2011–2012 season. Measures included: (1) glenohumeral internal and external rotation range of motion, (2) isometric internal rotation, external rotation and abduction strength and (3) assessment of scapular dyskinesis. Players were followed prospectively for the entire regular season (30 weeks), with shoulder problems registered bi-weekly using the Oslo Sports Trauma Research Center Overuse Injury Questionnaire. A cumulative severity score was calculated for each player based on their questionnaire responses. This was used as the outcome measure in risk factor analyses.
Results The average prevalence of shoulder problems throughout the season was 28% (95% CI 25% to 31%). The prevalence of substantial shoulder problems, defined as those leading to moderate or severe reductions in handball participation or performance, or to time loss, was 12% (95% CI 11% to 13%). Significant associations were found between obvious scapular dyskinesis (OR 8.41, 95% CI 1.47 to 48.1, p<0.05), total rotational motion (OR 0.77 per 5° change, 95% CI 0.56 to 0.995, p<0.05) and external rotation strength (OR 0.71 per 10 Nm change, 95% CI 0.44 to 0.99, p<0.05) and shoulder injury.
Conclusions Injury prevention programmes should incorporate interventions aimed at improving glenohumeral rotational range of motion, external rotation strength and scapular control.
- Epidemiology
- Injury Prevention
- Sporting injuries
Statistics from Altmetric.com
Introduction
Handball is a sport which places large demands on players’ shoulders due to a high volume of throwing, as well as frequent physical contact. Cross-sectional studies suggest that shoulder injuries are common among elite players.1 ,2 However, as players often continue to train and compete despite the existence of overuse shoulder injuries,1 ,3 prospective cohort studies of handball injuries which have used a time-loss injury definition are unlikely to have captured the true extent of the problem.4–6
We recently conducted a prospective study of overuse injuries among athletes from five different sports, including handball, using a new method designed specifically to record overuse problems.3 We found that shoulder problems among handball players was one of the injury areas with the greatest impact on sports participation and performance. However, the study involved a limited sample and lasted only 3 months. Therefore, the extent and severity of shoulder injuries in elite players during a full competitive season remains unknown.
Several studies have investigated risk factors for shoulder injuries among overhead athletes, with particular focus on glenohumeral joint range of motion (ROM)7–12 and shoulder strength.12–14 While a majority of studies have been on baseball pitchers, these factors have also been linked to injury among handball players.8 ,13 Scapular control impairment, referred to as scapular dyskinesis, is also a commonly proposed risk factor despite a lack of evidence linking it to shoulder injury.15–17
The main objectives of this study were to record the prevalence of shoulder problems among elite male handball players over a full competitive season, and to investigate the relationship between shoulder ROM, isometric strength and scapular dyskinesis and shoulder injury. This information is necessary to inform the development of injury prevention interventions.
Methods
Study design
This was a prospective cohort study involving all teams in the Norwegian elite handball series for men (Postenliga) in the season 2011–2012. We visited each team during a training session in 4 weeks prior to the season and every player present at the session was invited into the study. Players were eligible for participation if they had a contract with a Postenliga club in the season 2011–2012 (N=230), irrespective of whether they had current or previous shoulder pain/injury. All players who consented to participation performed baseline testing and were followed for the duration of the season (September 2011 to May 2012), during which time the extent to which they experienced shoulder problems was monitored bi-weekly using the Oslo Sports Trauma Research Center (OSTRC) Overuse Injury Questionnaire. Written consent was obtained from all participants.
Baseline testing
Fahlström questionnaire
Each player's shoulder injury history and status at the time of testing was assessed using a modified version of the Fahlström questionnaire previously used in studies of elite handball players.1 Each player was also asked whether they had ever undergone shoulder surgery.
Range of motion
Internal rotation (IR) and external rotation (ER) ROM was measured at the glenohumeral joint using a digital inclinometer attached to a 30 cm Perspex ruler (Acumar digital inclinometer, Lafayette Instrument, Lafayette Indiana, USA) with the player in supine with their shoulder abducted to 90°. When necessary, a folded towel was used to ensure that the upper arm was correctly aligned in the frontal plane. The scapula was stabilised by the examiner with their thumb on the coracoid process and four fingers grasping the spine of the scapula posteriorly.18 The end of IR and ER ROM was defined as the point at which the scapula was felt to move. The averages of two repeated measures were recorded as the participant's values for IR and ER. These values were summed to give the total rotational motion (TROM).
Isometric strength
Isometric IR, ER and abduction strength was measured using a digital handheld dynamometer (MicroFET, Hoggan Health Industries, Salt Lake City, Utah, USA). IR and ER strength was measured with the participant in supine with their shoulder in neutral position and their elbow flexed to 90°. Abduction strength was measured with the participant standing with their shoulder in ER and abducted to 30° in the plane of the scapula. Their elbow was extended in a neutral ‘open can’ position. We verbally and manually assisted players to stabilise their scapula prior to initiating abduction. However, no external scapula fixation was provided during actual testing. Players were asked to perform all strength measures twice and the best attempt was recorded. A detailed protocol of ROM and strength testing is available as an online supplementary appendix.
Scapular control
A physiotherapist observed players perform five repetitions of flexion and abduction while holding a 5 kg weight. Each shoulder was rated as having normal scapular control, slight scapular dyskinesis or obvious dyskinesis, according to the methods proposed by McClure et al.19 All assessments were performed by the same physiotherapist, who made their rating based on live observation and, if necessary, inspection of recordings made by a video camera situated 3 m behind the player.
Reliability of shoulder tests
Strength and ROM testing was performed by two physiotherapists, each of whom tested six teams. Each test's inter-rater reliability was determined using a pilot study of 38 shoulders which were measured in a randomised order by both physiotherapists, blinded to the results of each other. As all ROM and strength measures were performed twice during actual player testing, the two measures were used to assess intra-rater reliability. For scapular dyskinesis testing, intra-rater reliability was determined using 30 anonymised videos which were viewed in a randomised order and rated by the tester on two occasions separated by 1 week.
Injury registration
The OSTRC Overuse Injury Questionnaire was emailed to all players in the project every second Sunday for the entire regular season using online survey software (Questback V. 9692, Questback AS, Oslo, Norway). Questions included the extent to which shoulder problems affected the player's participation, training volume and performance, as well as the extent to which he had experienced shoulder pain over the previous 7 days.20 Players were asked about their dominant and non-dominant shoulders separately, with shoulder problems defined as any pain, ache, stiffness, instability, looseness or other complaints related the shoulder. The survey software prevented questionnaire submission if all items were not fully completed and automatically sent reminder emails to non-responders after 3 and 7 days.
The prevalence of shoulder problems was calculated for the dominant and the non-dominant shoulder each time the questionnaire was administered by dividing the number of players who reported any problem (ie, anything but the minimum value in any of the four questions) by the number of questionnaire respondents. At the end of the study, the average prevalence of shoulder problems was calculated for each shoulder.
The average prevalence of substantial shoulder problems was also calculated and expressed for each shoulder in the same way as described above. However, the numerator in the prevalence calculations only included shoulder problems leading to moderate or severe reductions in training volume or sporting performance, or a total inability to participate.20 This filtered out problems with little functional consequences.
Each time a player responded to a questionnaire, their responses enabled the calculation of a severity score ranging from 0 to 100.20 At the conclusion of the study, each player's scores were summed and divided by their number of questionnaire responses to determine their average severity score. This was used as the outcome measure in risk factor analyses, as described below.
Statistical methods
Players with fewer than four questionnaire responses were excluded from all analyses due to insufficient data. As average severity scores were heavily skewed in the positive direction they were dichotomised using a cut-off value of 40 to distinguish ‘injured’ from ‘uninjured’ players. This value was chosen as it indicates that the player had substantial shoulder problems throughout the season. Post hoc Receiver Operator Characteristic curve analyses confirmed that this value had the greatest predictive ability to identify significant risk factors.
We considered accounting for clustering of data by teams in the statistical methods. However, the variance between teams was estimated to be zero. Therefore, associations between risk factors and shoulder injury were assessed using normal multivariable logistic regression models. The following were analysed as potential risk factors: obvious scapular dyskinesis, slight or obvious scapular dyskinesis, IR strength, ER strength, ratio of ER to IR strength, IR ROM, ER ROM, TROM, >5° TROM difference between shoulders, <5° ER gain in the dominant shoulder (ER deficit) and glenohumeral IR deficits of 5°, 10°, 15° and 20°. Strength measures were adjusted for body mass and demographic variables possibly associated to shoulder injury (p<0.2) were added to each model using a forward selection procedure.
We compared dominant and non-dominant shoulder strength and ROM using paired-samples t tests and Wilcoxon's rank-sum test. Associations between participant characteristics and data completeness were analysed using logistic regression. The reliability of the ROM and strength tests was assessed by calculating the intraclass correlation coefficient (ICC), using a two-way mixed model (absolute agreement) for inter-rater reliability and a two-way random model (absolute agreement) for intra-rater reliability.21 The intra-rater reliability of scapular dyskinesis testing was assessed using Spearman's r (RS).
Results
Participants
A total of 206 of 230 Postenliga players agreed to participate in the study (90%). On average, players were 24 years old (SD 4, range 18–48), 189 cm tall (SD 7, range 167–207) and weighed 89 kg (SD 10, range 64–114). They had been playing handball for an average of 14 years (SD 5, range 4–34) and had played in the elite series for an average of 4 years (SD 4, range 0–15). A majority of players were right handed (73%). Eighty-six were back players (42%), 48 were wing players (23%), 30 were line players (15%), 29 were goalkeepers (14%) and 15 played in a combination of positions (6%). All participants completed the baseline questionnaire. The number that was tested and included in each analysis is shown in figure 1.
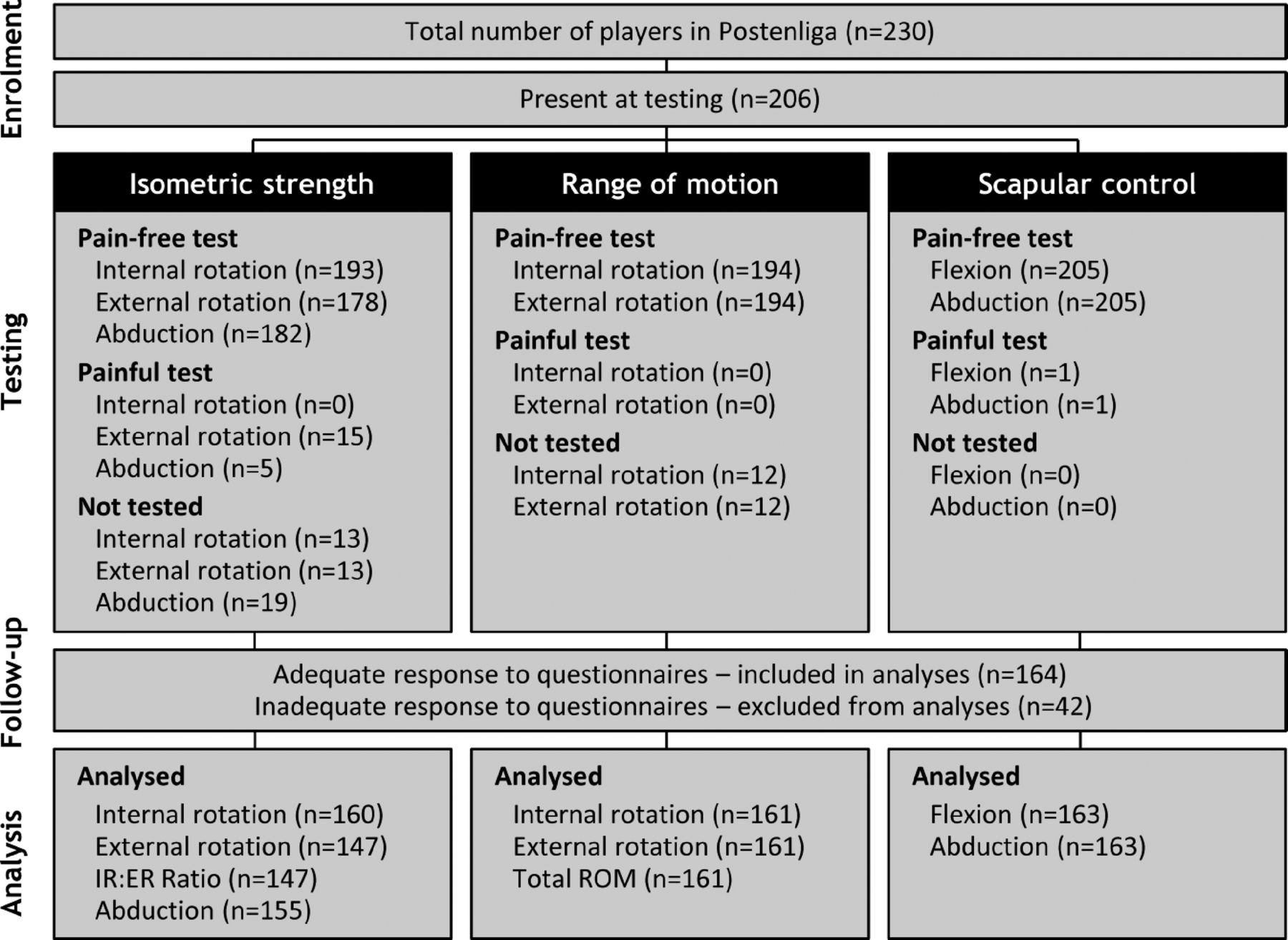
Study flow chart showing the number of players included, tested and analysed (ER, external rotation; IR, internal rotation; ROM, range of motion).
Fahlström questionnaire
At the time of testing, 154 players (75%) reported a history of shoulder pain associated with handball. Sixty-five players (32%) reported current shoulder pain and 44 players (21%) reported having to modify their training or match participation due to pain. Of these, 23 (11%) were currently unable to play matches due to shoulder pain, 12 had difficulties in normal daily activities (6%) and 9 had sleep disturbances due to pain (4%). Seven players (3%) had undergone shoulder surgery.
Shoulder testing
Range of motion
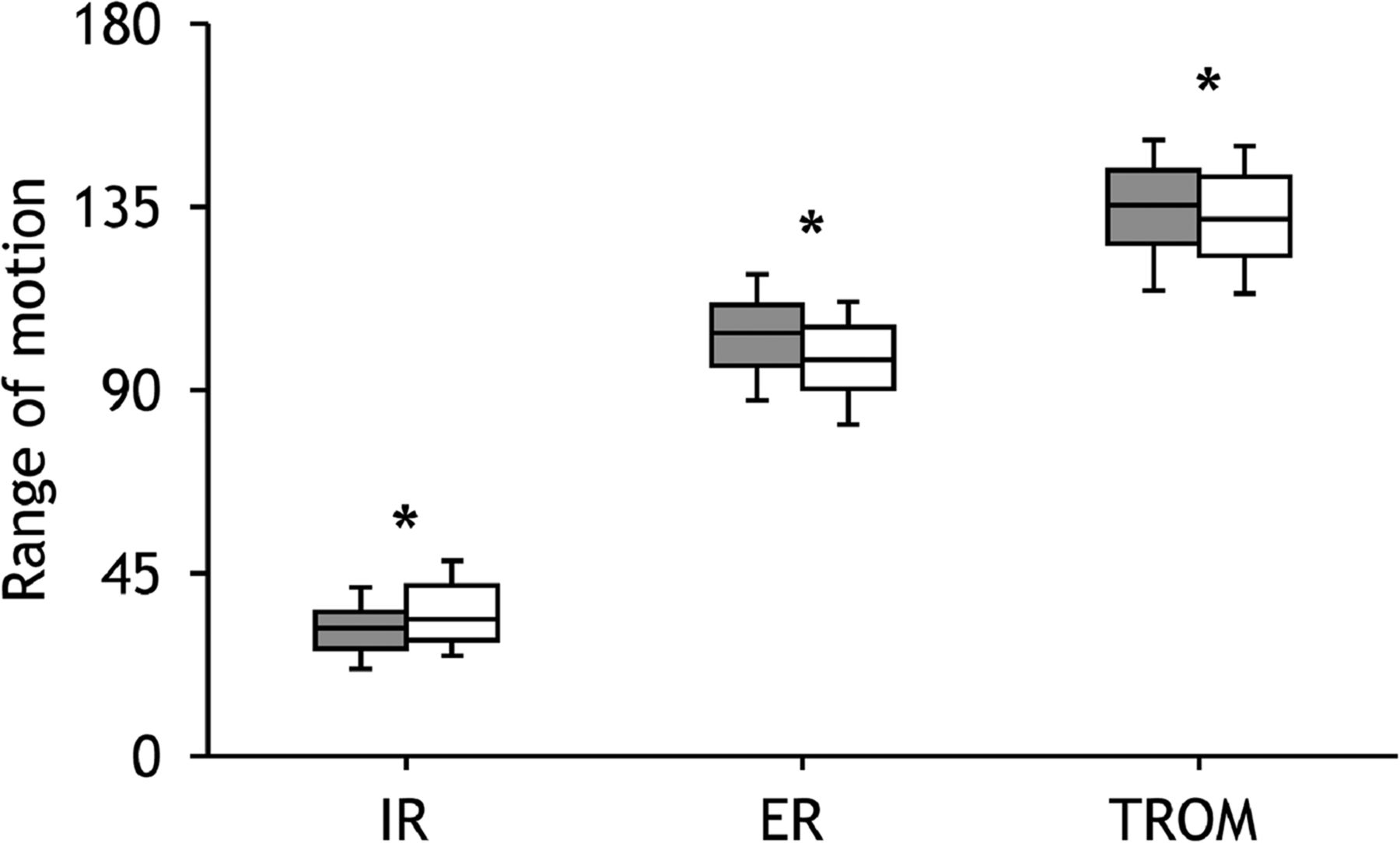
Dominant shoulders had significantly less IR than their non-dominant shoulders (mean difference: 4°, 95% CI 3 to 5°, p<0.01), with eight players having greater than 20° glenohumeral IR deficit. Dominant shoulders also had a greater ER range (mean difference: 6°, 95% CI 5 to 8°, p<0.01) and a significant increase in TROM (mean difference: 3°, 95% CI 1 to 4°, p<0.01; figure 2). Eighty-seven players had <5° ER gain in their dominant shoulder (ER deficit), and 19 players had a TROM difference of more than 5° between sides.

Range of motion differences between dominant shoulders (grey boxes) and non-dominant shoulders (white boxes; ER, external rotation; IR, internal rotation; TROM, total rotational motion; *p<0.05).
Isometric strength
Compared with the non-dominant shoulders, dominant shoulders were significantly weaker in ER (mean difference: 0.09 Nm/kg, 95% CI 0.04 to 0.13, p<0.01) and stronger in abduction (mean difference: 0.07 Nm/kg, 95% CI 0.2 to 1.2, p<0.01). The ratio of ER to IR was lower for dominant shoulders (mean difference: 4%, 95% CI 2 to 6%, p<0.01; figure 3).
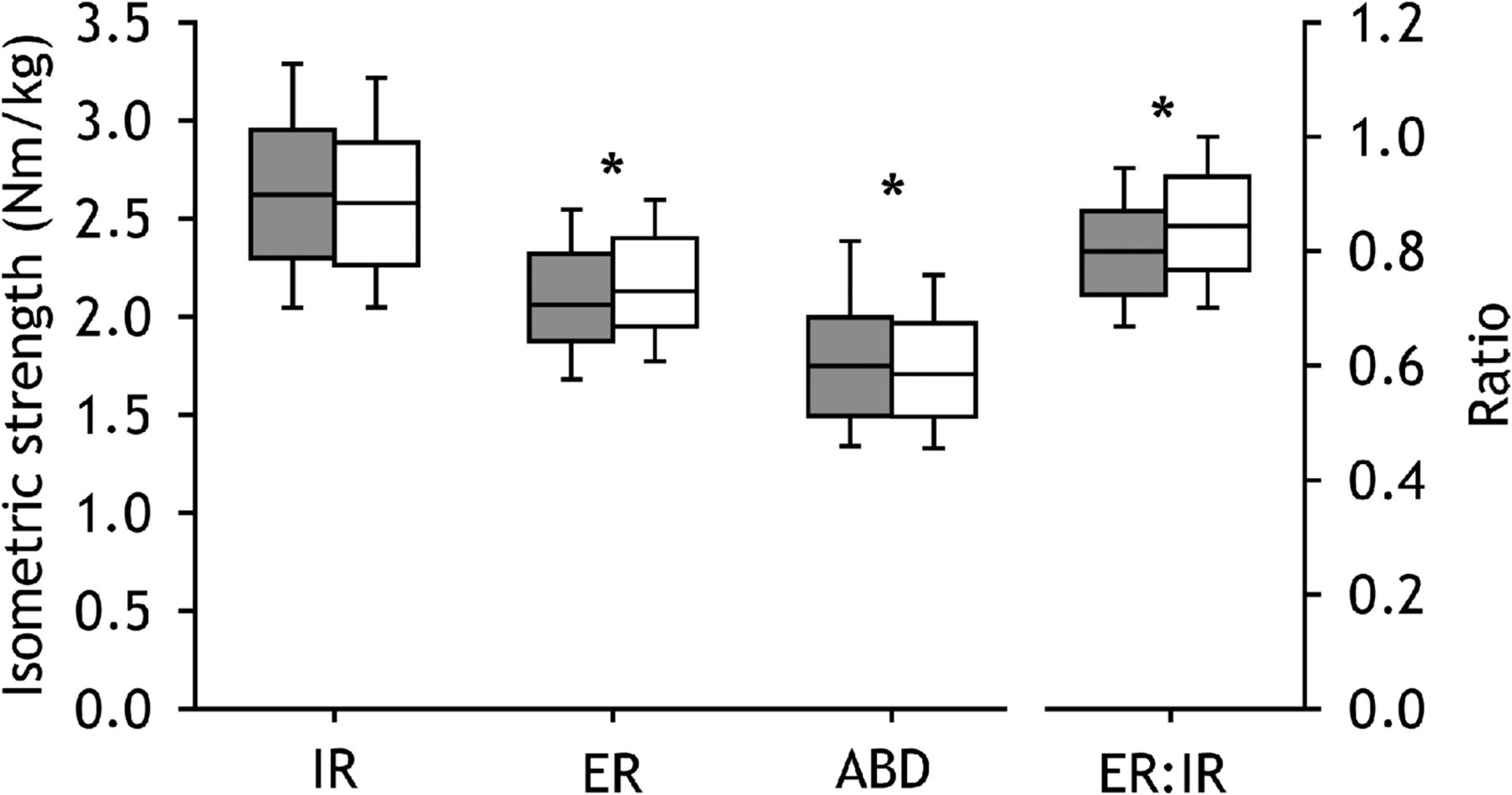
Isometric strength differences between dominant shoulders (grey boxes) and non-dominant shoulders (white boxes). ABD, abduction; ER, external rotation; IR, internal rotation; *p<0.05.
Scapular control
A total of 86 players (42%) were rated as having slight scapular dyskinesis in their dominant shoulders during flexion and 44 (21%) during abduction. Fourteen players (7%) were rated as having obvious scapular dyskinesis in their dominant shoulders during flexion and five (2%) in abduction.
Reliability of shoulder tests
The inter-rater and intra-rater reliability (ICC) of ROM and strength tests is shown in table 1. For classification of scapular control into three groups (normal, slight or obvious dyskinesis) the intra-rater reliability (RS) was 0.78 for flexion and 0.69 for abduction. For classification into two groups (normal or abnormal) the RS was 0.76 for flexion and 0.69 for abduction.
ICC for measures of strength and ROM
Prospective monitoring of shoulder problems
The OSTRC Overuse Injury Questionnaire was administered 15 times during the course of the season and the total response rate was 63%. Complete data were collected from 25% of players, 53% of players completed 10 or more questionnaires and 80% of players completed four or more. The response rate varied from 40% to 81% between teams. However, no other demographic characteristics were associated with missing data and there were no associations between players’ baseline shoulder status or injury history and data completeness.
One hundred and eight players (52%) reported problems in their dominant shoulder at some point during the season. Of these, 15 players only reported mild pain with no functional consequences and 50 players reported problems causing moderate or severe reductions in participation or performance (defined as substantial problems). Fifty-five players (27%) reported problems in their non-dominant shoulders during the season, 7 of which only involved mild pain and 14 of which were substantial problems.
The average prevalence of shoulder problems during the season was 28% (95% CI 25% to 31%) in the dominant shoulder and 7% (95% CI 6% to 9%) in the non-dominant shoulder. The average prevalence of substantial shoulder problems was 12% (95% CI 11% to 13%) in the dominant shoulder and 1% (95% CI 0.7% to 1.3%) in the non-dominant shoulder.
Risk factor analyses
Demographic factors
A history of shoulder surgery (OR 8.3, 95% CI 1.3 to 51.4, p=0.02) and playing in a back position (OR 16.4, 95% CI 2.0 to 132.3, p<0.01) were significantly associated with average severity scores. No associations were identified between players’ average severity scores and their age, height, body mass, years of handball participation, years of participation at an elite level or their team.
Shoulder tests
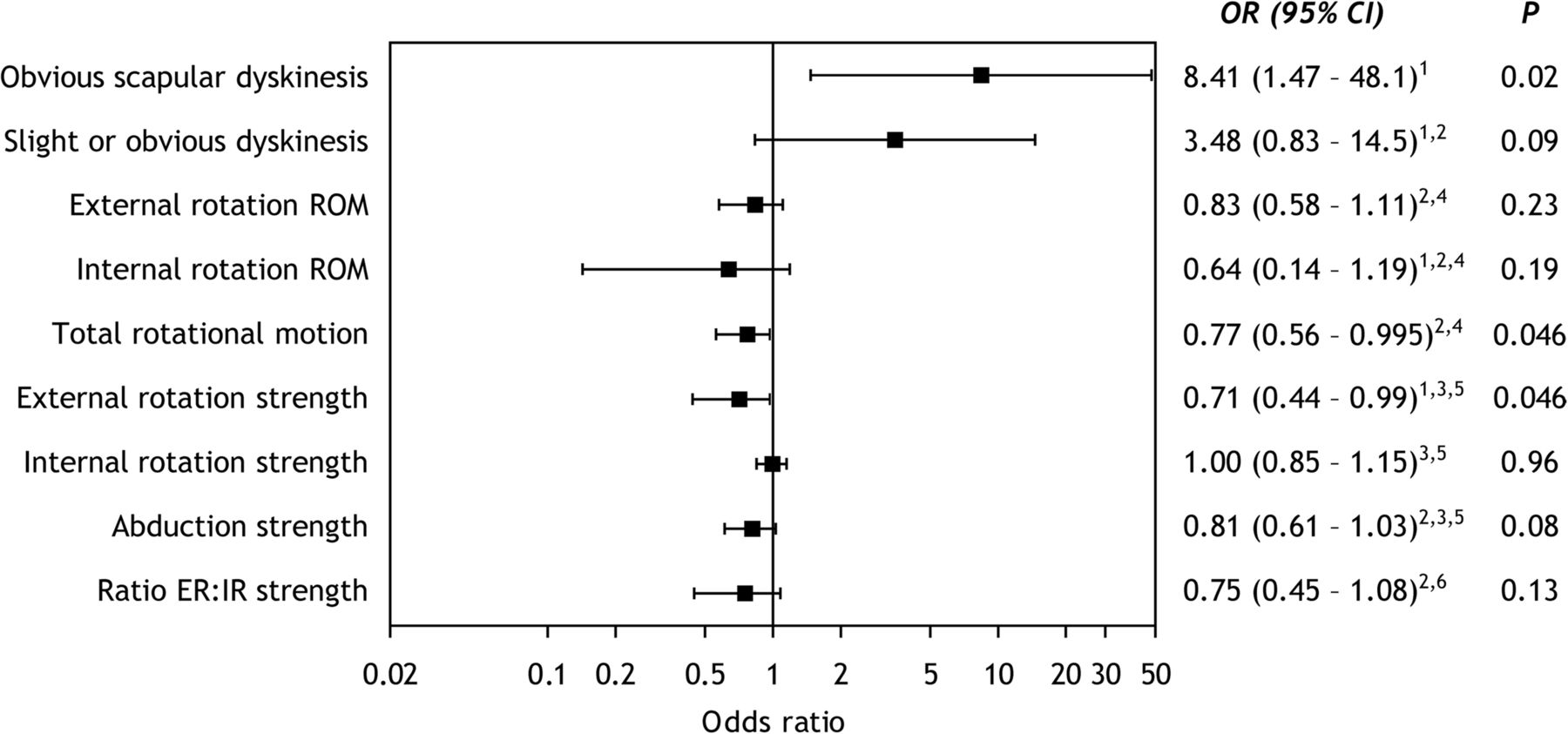
Obvious scapular dyskinesis, reduced TROM and isometric ER weakness were significantly associated with average severity scores (figure 4). As shown in the figure, slight scapular dyskinesis (p=0.09), IR ROM (p=0.19), supraspinatus strength (0.08) and the ratio of ER to IR strength (p=0.13) failed to achieve statistical significance. No associations were found between average severity scores and glenohumeral IR deficits, ER deficits or the difference in TROM between sides.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
ORs and 95% CIs for associations between risk factors and substantial shoulder problems (average severity score >40) based on multivariable logistic regression analyses adjusted for 1player position (back player), 2history of shoulder surgery and 3body mass. Expressed per 45° change, 510 Nm change, 65% change. ER, external rotation; IR, internal rotation; ROM, range of motion.
Discussion
This is the first prospective cohort study on risk factors for shoulder injuries among elite male handball players. The prevalence of shoulder problems was high, and we identified several internal risk factors associated with shoulder injury. In particular, players with obvious scapular dyskinesis, reduced ER strength and reduced TROM had a higher probability of experiencing substantial shoulder problems throughout the season.
Our surveillance data support previous epidemiological studies that have found shoulder problems to be common in handball. This has been found in investigations of various player populations, using a variety of study designs and measurement methods.1 ,3 ,6 In the current study, we used a new surveillance method designed specifically to capture overuse problems in sport.20 The prevalence of all shoulder problems and of substantial problems was among the highest we have measured in any anatomical area in any sport using these methods.3 ,22 This is obviously an injury problem that warrants preventative efforts. The results of our risk factor analyses may provide guidance in the development of prevention programmes.
Glenohumeral ROM and shoulder injury
Reductions in IR and increases in ER have been demonstrated in the dominant shoulders of uninjured overhead athletes from a variety of sports.1 ,7 ,8 ,12 ,23–26 This is regarded as a normal soft tissue and/or bony adaptation to the repeated throwing,15 which may even be protective against injury.27 However, several studies have linked large differences in IR and TROM between dominant and non-dominant shoulders to throwing-related shoulder injuries.7–11 For example, Wilk et al7 found that glenohumeral IR deficits of more than 20° and TROM differences exceeding 5° between shoulders were significant risk factors for injury among baseball pitchers. The same group has also recently proposed that ER deficits may also be an important risk factor.24 In the current study, dominant shoulders demonstrated a small but significant reduction in IR, an increase in ER and an increase in TROM compared with non-dominant shoulders. However, we were unable to find any associations between glenohumeral IR deficits, ER deficits or TROM differences and injury, despite using a range of cut-off values to define these terms.
Our TROM measures were approximately 40° lower than those reported for baseball pitchers.24 Although this might be due to differences in measurement technique, other studies of handball players,1 ,8 as well as of tennis,26 volleyball25 and badminton players28 report similar values. Handball players throw with wide variety or overarm and underarm techniques and their shoulders are frequently exposed to contact and blocking while in an elevated position. This may affect their ROM profiles and explain why concepts and criteria developed for pitchers, such as glenohumeral IR deficit, were not identified as risk factors in the current study.
In this study, absolute rather than relative TROM values were significantly associated with shoulder problems. This suggests stretching should be considered in the development of injury prevention programmes.
Rotator cuff strength and shoulder injury
We found a significant association between ER weakness and an increased probability of substantial shoulder problems throughout the season. There was no association between IR strength and injury. However, non-significant trends in the data suggest that lower ER to IR ratios and abduction strength may also be noteworthy risk factors.
Similar findings have been reported in studies of baseball pitchers, where isometric ER, abduction and ER to IR ratio have been associated with shoulder injury.12 ,14
Among female youth handball players, Edouard et al13 found no association between isokinetic ER or IR strength and injury. However, players with low ratios of concentric ER to concentric IR strength, and high ratios of eccentric IR to concentric ER strength had an increased risk of injury. As a different method was used to measure strength, their results cannot be directly compared with the current study. Nevertheless, the two studies can be interpreted in a similar way, as both suggest that ER strengthening exercises may be important in injury prevention programmes.
Scapular dyskinesis and shoulder injury
Scapular dyskinesis is a common finding among people with shoulder pain and a variety of shoulder pathologies such as impingement syndrome, rotator cuff tears, glenoid labrum tears and instability.16 It has also been shown to be common among athletes from a variety of overhead sports, such as baseball, swimming and tennis.29–31 However, it is common among symptom-free athletes as well as those with pain, and evidence of an association between scapular dyskinesis and shoulder symptoms among overhead athletes is lacking.32–35 A significant association has been demonstrated among rugby players,36 but as the mechanism of shoulder injury in rugby differs greatly from throwing sports such as handball the implications of this finding to the current study are unclear. In contrast to previous studies of overhead athletes, we may have been able to demonstrate a relationship due to a sufficient number of players being included in the study, and because the outcome measure was sufficiently sensitive to detect those with the greatest amount of shoulder problems.
Although we were able to demonstrate a significant, robust association between obvious scapular dyskinesis and shoulder problems, the size of the relationship is unclear. This is reflected in the width of the OR CI. Studies involving larger numbers of players are necessary to determine this with greater accuracy. Nevertheless, this study clearly indicates that injury prevention programmes for shoulder injuries in handball should include exercises to improve scapular control.
Methodological considerations
The major strengths of this study were that we used a prospective cohort design and included a large, representative sample of elite male handball players. We also used sensitive injury surveillance methods that capture all physical complaints. This proved necessary despite shoulder problems being highly prevalent, as few cases satisfied the time-loss injury definition most commonly used in surveillance studies.37 However, this study also has several limitations which should be considered when interpreting its results.
The challenge of overuse injuries
Traditionally, risk factor studies exclude injured players from baseline testing and record newly incurred injuries throughout the study. This temporal sequence allows for an assumption of cause and effect between risk factors and injury. However, challenges exist when applying this model to the study of overuse and chronic injuries, such as in the current study. First, a large proportion of players reported having shoulder problems at the time of testing. Excluding them would have biased the cohort such that it would not have been a representative sample. Therefore, only players who experienced pain during actual testing were excluded from analyses. Second, the majority of cases reported during this study represented chronic problems, with only a few minor cases occurring for the first time. Therefore, this study is limited to assessing associations between risk factors and shoulder problems and causation cannot be assumed.
Test selection
As with all risk factor studies, a key limitation of this study is the choice of screening tests and measurement techniques. In order to maximise clinical relevance, we chose simple and inexpensive testing in the field rather than in our biomechanics laboratory. The reliability of the tests ranged from moderate to very high, but in certain cases their validity could be questioned. Strength tests were isometric rather than dynamic, and for IR and ER they were performed in a supine position with the shoulder in neutral. This position has previously been shown to be reliable,21 and was selected based on a pilot study where we found that testing strength in an elevated position provoked pain in a greater number of players. However, the degree to which isometric testing in this position relates to dynamic shoulder strength during overhead throwing is unknown.
For ROM measurement, we used a single tester with a digital inclinometer rather than two testers with a bubble goniometer, as commonly described. Both methods have been shown to be reliable,21 but their results may differ systematically.38 ,39 Therefore, the absolute ROM values reported in this study may not be directly comparable to previous research.
For scapular dyskinesis, we used a subjective criterion-based assessment as recommended in a recent consensus statement.16 We chose a method with three rating options which has been shown to be valid for assessing three-dimensional scapular motion in overhead athletes.19 ,33 However, it has been suggested that a two-option rating (normal or abnormal) is more reliable than when multiple criteria are used.40 In this study, there was no improvement in intra-rater reliability when a two-option classification was applied. A strength of this study is that we used only one rater to assess scapular dyskinesis, as inter-rater reliability has been found to be moderate to low.40 ,41
We also chose to focus only on local risk factors at the shoulder rather than the entire kinetic chain, which is often implicated in throwing injuries.15 It is possible that factors such as hip and trunk rotation are associated with shoulder injuries in handball, and kinetic chain exercises should probably be considered in future injury prevention programmes. However, testing these factors was beyond the scope of this study.
Diagnostic accuracy
A second limitation to this study is that we have monitored self-reported shoulder problems and lack detailed diagnostic information on each case. Shoulder pain and dysfunction in throwers may have many causes, such as tendon pathology, subacromial and internal impingement, glenoid labrum injuries, glenohumeral joint instability and acromioclavicular joint dysfunction.27 ,42 The risk factors for each of these conditions may be different. Furthermore, several cases in this study were acute flare-ups of chronic problems or long-term problems initially caused by an acute trauma. Separation of the database into acute and overuse injuries according to current definitions was therefore particularly difficult, and no attempt was made to do so. As a result, it is likely that some injuries are included that were purely caused by acute trauma. This may have reduced our ability to identify relationships between risk factors and non-traumatic shoulder injuries.
Missing data
This study's third limitation is that the response rate was limited, especially compared with previous studies using similar surveillance methods.3 ,22 ,43 Based on players’ injury history and baseline status, it seems unlikely that there were systematic differences between responders and non-responders. However, the degree to which non-responders experienced shoulder problems during the course of the season remains unknown. The extent of missing data prevented us from using multiple imputation to estimate missing values and from using longitudinal statistical methods. Despite this, we felt that the existing data enabled us to identify players with the greatest amount of shoulder problems throughout the season, which was the main objective of surveillance.
Nevertheless, 42 athletes had to be excluded from analyses due to insufficient data, which reduced the statistical power of the study. This may have affected the accuracy of our coefficient estimates and prevented us from detecting other risk factors.
Conclusion
Shoulder injuries are highly prevalent among elite male handball players and preventative efforts are warranted. This study identified a number of internal modifiable risk factors associated with substantial shoulder problems, including TROM, ER strength and scapular dyskinesis. Injury prevention programmes incorporating these factors should be tested using randomised controlled trials.
What are the new findings?
-
Shoulder injuries are highly prevalent among elite male handball players.
-
Obvious scapular dyskinesis, reduced total range of motion and reduced external rotation strength are associated with an increased probability of shoulder injury.
How might it impact on clinical practice in the near future?
-
Programmes aimed at preventing shoulder injuries in handball should incorporate exercise to improve total rotational motion, external rotation strength and scapular control.
Acknowledgments
The authors would like to thank SE Steenstrup, A Wangensteen and E Hanssen for their assistance in data collection. The Oslo Sports Trauma Research Center has been established at the Norwegian School of Sport Sciences through generous grants from the Royal Norwegian Ministry of Culture, the South-Eastern Norway Regional Health Authority, the International Olympic Committee, the Norwegian Olympic Committee & Confederation of Sport and Norsk Tipping AS.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors RB, SHA, RM and GM contributed to project planning, data collection and manuscript preparation. BC was responsible for data analysis also for the overall content as the guarantor.
-
Competing interests None.
-
Ethics approval South-Eastern Norway Regional Committee for Research Ethics.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement Unpublished data are available upon request.