Article Text

Abstract
Background and purpose A programme based on eccentric exercises for treating subacromial pain was in a previous study found effective at 3-month follow-up. The purposes of the present study were to investigate whether the results were maintained after 1 year and whether the baseline Constant-Murley score, rotator cuff status and radiological findings influenced the outcome.
Patients and methods 97 patients on the waiting list for arthroscopic subacromial decompression had been randomised to a specific exercise programme or unspecific exercises (controls). After 3 months of exercises, the patients were asked whether they still wanted surgery and this option was available until a 1-year follow-up. 1 year after inclusion or 1 year after surgery, the number of patients who decided to have surgery in each group was compared. The choice of surgery was related to the baseline Constant-Murley score, ultrasound and radiographs taken at inclusion.
Results All patients had improved significantly (p<0.0001) in the Constant-Murley score at the 1-year follow-up. Significantly more patients in the control group decided to have surgery (63%) than those in the specific exercise group (24%; p<0.0001). Patients who decided to have surgery had a significantly lower baseline Constant-Murley score and more often a full-thickness tear. Patients with partial tears did not differ from those with intact tendons.
Interpretation The positive short-term results of specific exercises were maintained after 1 year, and this exercise strategy reduces the need for surgery. Full-thickness tear and a low baseline Constant-Murley score appear to be a predictive marker for a less good outcome.
Trial registration number Clinical trials NCT01037673.
- Eccentric exercise
- Physiotherapy
- Shoulder injuries
- Ultrasound
- Tendons
Statistics from Altmetric.com
Introduction
Subacromial pain is common and may cause disability as well as negatively influence quality of life.1 ,2 Since the aetiology appears to be multifactorial, involving several anatomical structures, the choice of treatment is challenging.1 Initial treatment is usually physiotherapy and corticosteroid injections.2 The role of exercise treatment has been investigated in several studies but evidence for efficacy is still limited and there is no consensus on the ideal programme.3–6 When exercise treatment fails, surgical intervention with arthroscopic subacromial decompression7 is recommended. Despite the fact that equivalent effects of physiotherapy and arthroscopic subacromial decompression (ASD) have been reported,8–10 the number of operations have continued to increase.11
Rotator cuff tears may be associated with subacromial pain and optimal management is uncertain.1 ,12 The reported success rate of exercise treatment in patients with full-thickness tears varies from 33% to 88%.4 ,13 This variability could be due to the different inclusion criteria, treatment and evaluation methods, stressing the need for search of factors influencing treatment response.4 ,13 We have previously reported successful short-term results after a specific exercise programme with focus on eccentric exercises used for patients on the waiting list for surgery due to subacromial pain.14 Despite the fact that all patients had undergone previous physiotherapy, the majority decided to decline surgery after 3 months of the specific exercises. The purposes of the present study were to examine whether these positive short-term results were maintained after 1 year and whether the baseline Constant-Murley (C-M) score, rotator cuff status and radiological findings influenced the decision about surgery.
Material and methods
Patient enrolment
Ninety-seven patients, 36 women and 61 men with a mean age of 52 years (30–65), had been randomised to a specific exercise programme or a control exercise programme. All patients had clinical signs of subacromial pain but not of a major cuff tear. The study group was recruited from the waiting list for ASD at a University Hospital in Sweden. The inclusion criteria were: at least 6 months duration of lateral shoulder pain at rest or during arm elevation; no clinical signs of major cuff dysfunction (table 1) and an unsatisfactory result after at least 3 months of exercises in primary care. Furthermore, three of the following criteria had to be positive: Impingement sign according to Neer15; or Hawkins-Kennedy16; Jobes Test17; or Patte Test.18 A positive Neer's impingement test (subacromial injection of a local anesthetic)19 was also compulsory. Exclusion criteria were: significant loss of flexion, abduction or strength in rotation indicating a major cuff tear; malignancy; osteoarthritis of the glenohumeral or acromioclavicular joints; previous fracture or surgery of the shoulder girdle; os acromiale; polyarthritis; fibromyalgia; instability in any shoulder joint; frozen shoulder; cervical pain; subacromial corticosteroid injection during the past 3 months or inability to understand written and spoken Swedish. Further, findings indicating mental distress according to the Hospital Anxiety and/or Depression Scale (HAD)20 would also lead to exclusion. All patients gave their written consent after verbal and written information.
Background variables for the two groups according to randomisation
Interventions
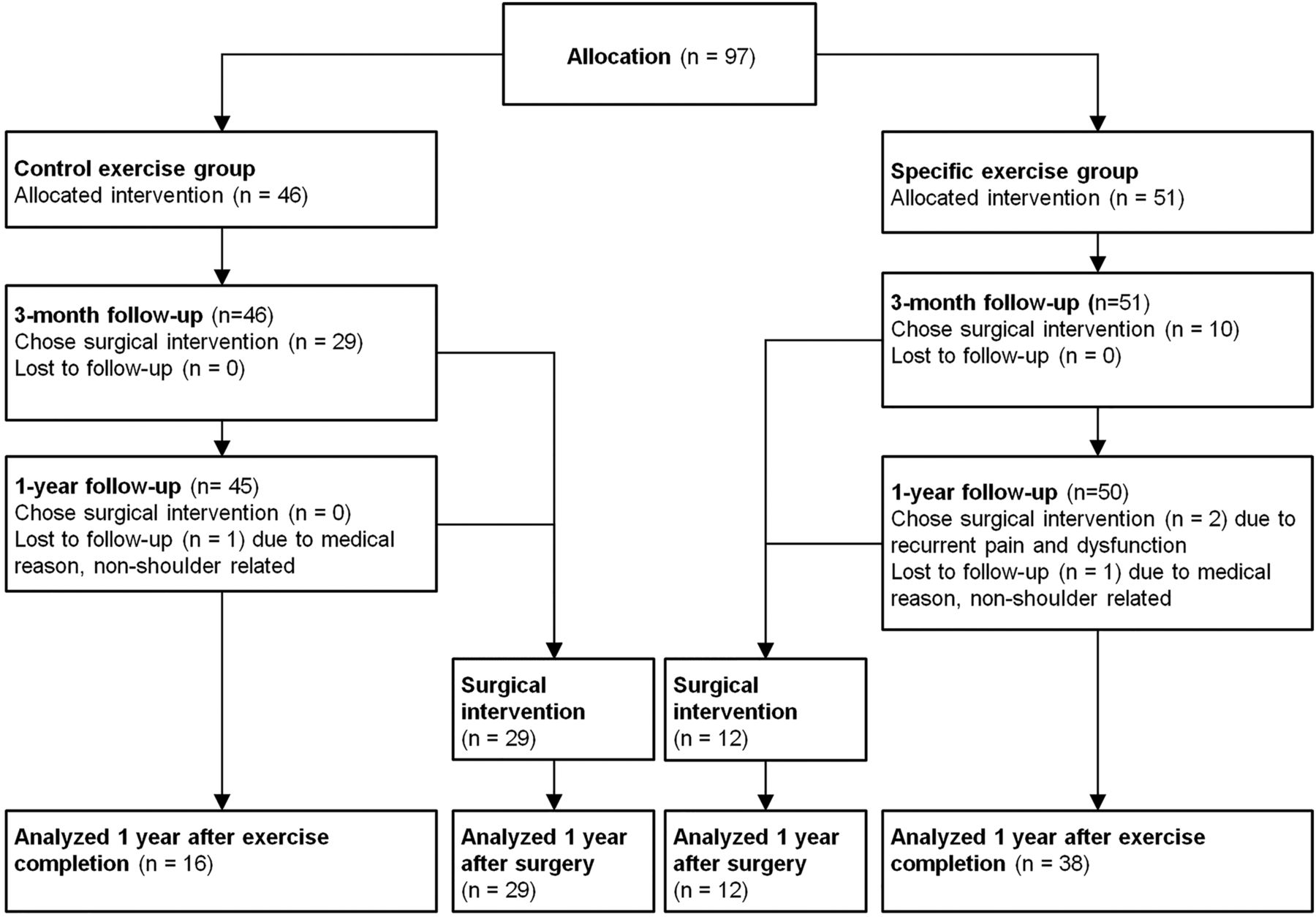
Figure 1 shows an overview of the study design. The included patients had been randomised to one of two exercise programmes. One included eccentric exercises for the rotator cuff and a combination of concentric and eccentric exercises for scapula stabilisers, all with a progression of load which was labelled the specific programme. The patients were recommended to load with pain up to a subjectively assessed 5 on a 0–10 scale according to a pain-monitoring model.21 The other regime, called the control programme, included six active movements for the neck and shoulder without any load or progression. These were: shoulder abduction, retraction and elevation, neck retraction and stretch of the upper trapezius and pectoralis major muscles and the exercises were instructed to be pain free. The programmes have previously been described in detail.14 At inclusion, all patients had received a subacromial corticosteroid injection (1 mL triamcinolon 20 mg/mL mixed with 6 mL mepivacain 10 mg/mL). Within 2 weeks, a physiotherpist introduced the allocated exercises and gave standardised information about the condition and ergonomics. Visits to the physiotherapist were weekly for both groups during the first 2 weeks and then every other week over the following 10 weeks (a total of seven visits). The patients recorded adherence of home exercise sessions in a diary. After 3 months, at a visit to a blinded shoulder surgeon, all patients were asked whether they still wanted surgery and, if so, were operated on within 3 months. The option of surgery was then continuously available until the 1-year follow-up. Surgery included arthroscopic inspection of the glenohumeral joint and subacromial space, bursal and acromial resection (ASD) as described by Ellman.7 One of two experienced senior shoulder surgeons, not involved in the study, performed all surgical procedures. Postoperatively, all patients performed a previously described 3-month exercise programme routinely used after ASD, which was supervised by a physiotherapist.22

Flow chart according to consolidated standards of reporting trials (CONSORT-statement) with the number of patients randomised, adherent and choosing surgery during the follow-up period.
Outcome measures and assessments
Radiographic examination had been performed at inclusion using anterior–posterior, lateral, axillary and acromioclavicular views. An experienced radiologist and a shoulder surgeon independently assessed the radiographs, examining for osteoarthritis in any joint, proximal humeral migration, subacromial calcification and subacromial degeneration, which was considered to be present if sclerosis, cysts or spur formations on the greater humeral tuberosity and/or under the acromion were observed. Findings of subacromial degeneration were dichotomised into two categories: yes (one or more signs) and no (zero signs). After inclusion, a bilateral shoulder ultrasound was performed by an experienced radiologist and repeated independently by a shoulder surgeon. The equipment used was a Siemens Acuson Sequoia 512 (Acuson, Mountain View, California, USA) with a variable 8–10 MHz linear array transducer. The extension of a cuff tear was categorised as total or subtotal, referring to the width of the affected tendon and depth assessed as a partial thickness tear (PTT) or full thickness tear (FTT).23 Tear size was not measured in mm. PTT was defined as a localised absence of the tendon seen in two orthogonal planes as a mixed hyperechogenic and hypoechogenic region. FTT was defined as a non-visualisation of the tendon throughout the entire thickness.23 The patients were kept blinded to their ultrasound findings until the final follow-up.
Inter-assessor agreement was calculated for radiological and sonographic assessments. All score recodings were conducted by the same blinded shoulder surgeon at inclusion, after 3 months and 1 year after the respective treatments (figure 1).
Primary outcomes were the C-M score24 and number of operated patients. Secondary outcomes were: Disability of the Arm, Shoulder and Hand questionnaire (DASH) Score25 ,26 (Swedish version), Visual Analogue Scale (VAS)27 (0–100 mm) to assess pain intensity at rest, during arm activity and at night, and health-related quality-of-life using the EuroQol Instrument (EQ-5D and EQ VAS).28 All instruments are validated or recommended and have high intrareliability.25 ,29
Sample size
A power analysis based on the C-M score24 was calculated for the initial study14 revealing that 82 patients would be required to detect a mean 10-point group difference with a variability of 16 points (β=0.80, two sided α=0.05).3 ,9 ,14 To compensate for dropouts, a further 20 patients were recruited.
Randomisation
Fifty-five numbers of each treatment alternative were concealed in opaque envelopes, mixed and numbered by an independent physiotherapist. Patients were coded consecutively at inclusion by the surgeon and treatment allocation according to the draw of the envelope was decided at the first visit to the physiotherapist. The randomisation procedure has previously been described in detail.14
Statistical analysis
Parametric and non-parametric tests were used for comparison of baseline variables. For within-group comparisons, a paired t test was used to calculate differences in total scores between 3 months and 1 year. The number of patients choosing surgery in each group was compared using Pearson's χ2 test. For proportions of radiological and ultrasound findings, Fisher's exact test was used. Inter-assessor agreement on imaging findings was graded as very good, good, moderate, fair or poor using the κ-value according to Altman.30 Associations between imaging findings, baseline C-M score and the patient's choice of surgery (yes/no) were analysed with logistic regressions. In the logistic regression analysis, the C-M score at baseline was divided into quartiles (0–35, 36–44, 45–58 and 59–100 points) and gender was adjusted for p<0.05 was considered significant. The statistical software package StataCorp LP (College Station, Texas, USA) was used.
Results
Adherence and baseline data
Ninety-five patients were assessed at 1-year follow-up. Two patients in each group did not attend the 1-year follow-up due to non-related disease (figure 1). All included patients had, prior to inclusion, undergone at least 3 months of physiotherapist-assisted shoulder exercises in primary care. No patients had received structured eccentric exercises and the intensity and monitoring varied. Eighty-five of the 95 patients had received one or several subacromial corticosteroid injections more than 3 months before inclusion. There was no significant difference in the number of injections between the treatment groups. Both groups had similar adherence to exercises and physiotherapist appointments. The groups were comparable at baseline except that there were more male patients in the specific exercise group (table 1).
One-year assessment
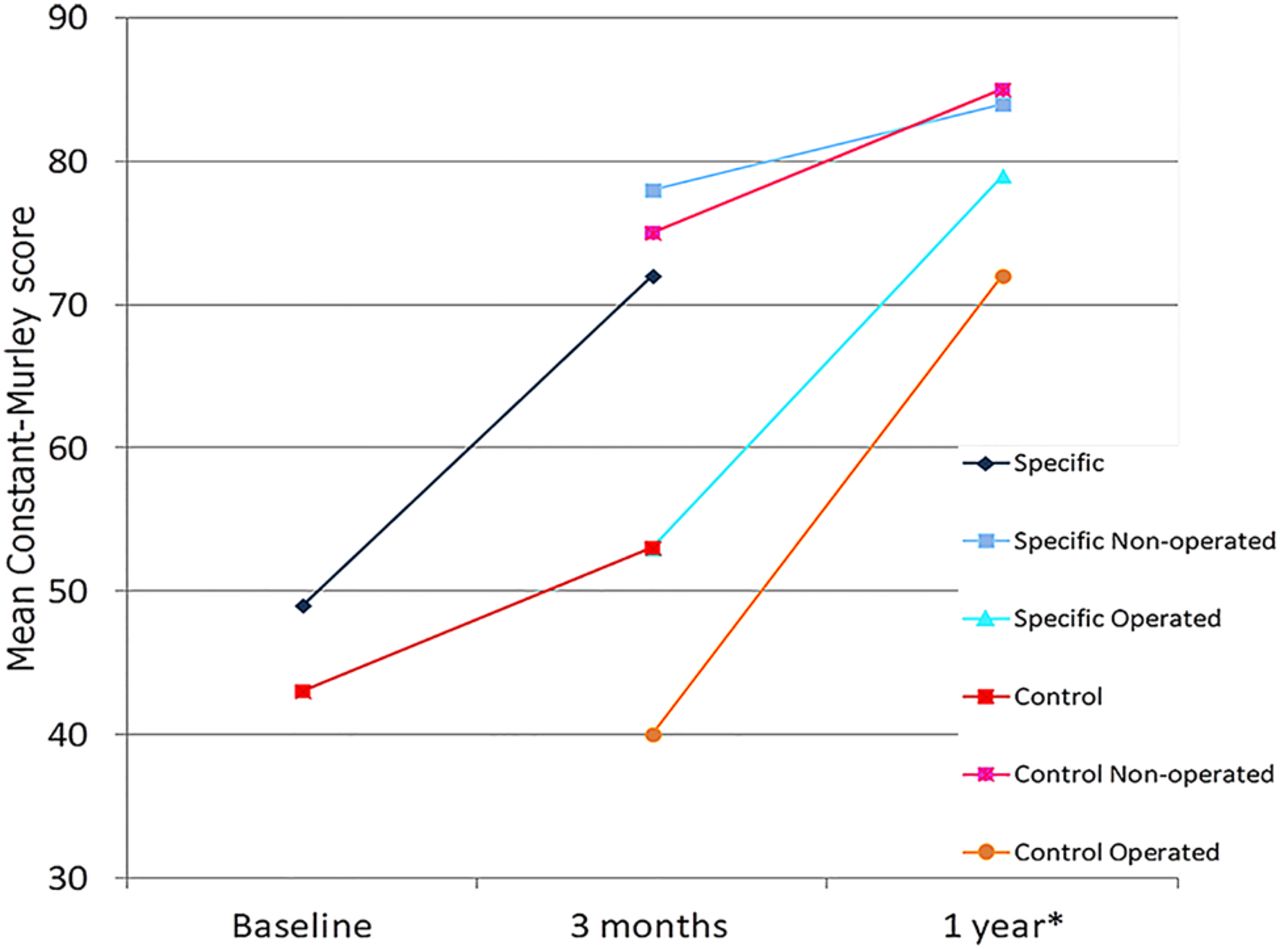
According to the C-M score, there was a significant improvement between 3 months and 1 year (p<0.0001; table 2, figure 2), as well as in all the secondary outcomes (p<0.05; table 3). Significantly more patients in the control group (63%) than in the specific exercise group (24%) had decided to have surgery (p<0.0001; table 2, figure 1).
Mean (SD) values in a Constant-Murley score, the original two groups at baseline and a 3-month follow-up, and the four groups that appeared after the patients’ decision about surgery at a 3-month or 1-year follow-up
Mean (SD) values in all outcomes at baseline, and at 3-month and 1-year follow-ups for the two originally randomised groups and the groups that appeared after the patients’ decision about surgery at the 3-month or 1-year follow-up

{kind=link}
{kind=link}
The mean Constant-Murley score in the two original groups at baseline and at 3-month assessment. The 3-month and 1-year mean Constant-Murley score in the four groups divided by the choice of surgery. Constant-Murley score 0–100 (100=maximum shoulder function). *One year after completion of exercises (non-surgery group) and 1 year after surgery.
Two patients in the specific exercise group decided to have surgery between the 3-month and 1-year visits due to recurrent symptoms (figure 1). The mean C-M score for all patients was 80 (SD 16) at the 1-year follow-up. Patients from both intervention groups not wanting surgery had a mean C-M score of 84 (SD 14) and patients who had undergone surgery had a mean C-M score of 74 (SD 17) 1 year after surgery.
At the 1-year follow-up, five patients in the specific exercise group and four in the control group reported having continued with exercises for another 2 months. The interassessor agreement for radiology and ultrasound was very good.30 Perfect agreement occurred for radiology. In five cases where ultrasound assessments differed between assessors, the radiologist's opinion was used (table 4).
Ultrasound assessments of the rotator cuff of 97 patients with subacromial pain by the two investigators
Thirty of the 97 included patients had cuff tears (table 1). There was no significant difference in tear type between the groups. Twenty-six patients had isolated supraspinatus tears and four had a combination of lesions involving the supraspinatus, subscapularis and long head of the biceps. Twenty-one of the single tendon tears were PTT and five were FTTs. Four patients with FTTs involving the supraspinatus and subscapularis decided to have surgery.
A significantly larger proportion of patients with radiographic signs of subacromial degeneration had an FTT (p=0.03). The presence of subacromial calcification or degeneration did not independently influence the choice of surgery. Patients with a baseline C-M score in the lower quartile had a significantly larger risk of choosing surgery, independently of gender, treatment group and rotator cuff status, compared with the highest quartile, OR 7.7 (95% CI 1.67 to 33.3) and p=0.007 (table 5). Patients in the control group treated non-operatively had the highest mean C-M score 54 (SD 12) at baseline. Gender and decision of surgery were not related. In the retrospective correlation of baseline data and outcome, the overall improvement in C-M score was 44 (88%) in the specific non-surgery group, 37 (88%) in the specific surgery group, 31 (57%) in the control non-surgery group and 35 (95%) in the control surgery group.
The baseline Constant-Murley score divided into quartiles
An FTT significantly increased the risk, OR 5.5, for choosing surgery compared with patients with intact tendons. No increased risk was found to be associated with a PTT (table 6).
The influence of rotator cuff status in relation to the patient's choice of surgery (yes/no) during the follow-up period analysed with logistic regression
Discussion
The principal finding of the present study was that, in a 1-year perspective, most patients with subacromial pain of relatively long duration were treated successfully without surgery. The specific exercise programme used especially in the current study allowed improvement of shoulder function to the extent that surgery could be avoided. The components of the specific exercise programme, which differ from current practice, are the eccentric focus, acceptance of pain during loading and load progression guided by pain assessment. The contribution of each part of the programme, however, cannot be elucidated with the used study design. Eccentric exercises for subacromial pain have previously been evaluated only in pilot studies,31 ,32 but efficacy is reported after treatment of other tendinoses.33 The effect mechanism of eccentric exercises is not fully understood but several theories have been presented.34–37
In the present study, moderate pain was allowed during load in accordance with other programmes for eccentric exercises,38 ,39 which might have contributed to the positive effect.
Baseline characteristics of patients with shoulder pain have been suggested as the most important predictor of outcome in primary care.40 This corresponds to our finding that patients with the lowest baseline C-M score significantly more often decided to have surgery. It has been reported that patients with FTT have less favourable results after physiotherapy13 ,41 as well as after ASD.42 ,43 Moosmayer et al44 compared cuff repair and physiotherapy for small-sized and medium-sized tears and found better outcome for the surgery group. However, 82% of their non-operated patients reported satisfactory results.44 We found that patients with FTT, to a larger extent, decided to have surgery compared with patients with intact tendons and PTT. Four of the nine patients with FTT had two tendons affected and they all demanded surgery, indicating that the extent of the lesion might influence the response to exercises. Since major cuff dysfunction was a criterion for exclusion, no patients with massive tears or tears involving the infraspinatus were included. There were four patients with FTTs of the subscapularis tendon but in no case involved the tear the whole width of the tendon. Therefore no marked reductions of strength were diagnosed by clinical examination. Owing to the limited number of patients with FTTs, any correlation between structural lesions and outcome should be interpreted with caution.
A recent study, evaluating criteria for successful outcome after ASD, found that radiological signs of subacromial degeneration were indicative of a successful outcome.45 In the present study, an association was found between subacromial degeneration and an FTT. This association was expected since these findings are considered to be involved in the same degenerative process.42 ,46 The presence of subacromial degeneration did, however, not independently influence the choice of surgery, which tallies with previous reports.47
All patients, regardless of treatment, had improved in all outcome measurements between 3 months and 1 year, and on a group level the improvements were statistically significant. The final outcome was superior for the specific group in which significantly fewer decided to have surgery, demonstrating that the specific programme is not only preferable but may also serve as a screening tool to select candidates for surgery.
The responsiveness to exercises is probably multifactorial, including psychological, physiological and biomechanical properties, structural tissue changes and the capability of developing compensatory mechanisms.48 Natural course, adaptation to the symptoms and increased attention while being a study participant, may have further added to the favourable outcome. Considering the strict inclusion criteria, long duration, excellent adherence and initial randomisation, it however appears unlikely that natural course and psychological factors could explain the significant group differences.
The corticosteroid injections given at inclusion are likely to have had an initial pain-reducing effect49 and were administered in order to facilitate the start-up of physiotherapy.50 Owing to the relatively short pain-reducing effect of an injection,49 it is less probable that this would have had an impact on the course between 3 months and 1 year. Similarly, the initial physiotherapist guidance may have contributed to the early positive effects but would not have accounted for the group differences after 3 months.51
In interpreting the results, some methodological restraints should be considered. The present study primarily addresses the course between 3 months and 1 year after treatment and is consequently observational, although it is based on an initially randomised study. Therefore, when assessing the retrospective analysis of the baseline data, the fact that two patients were lost to follow-up and that two others had moved between treatment groups must be taken into account. Another cause for concern is the single non-blinded care provider. This avoids interpersonal differences in attitudes and skills but might affect validity. It may be argued that the positive effect of the specific exercises could be attributed to a dedicated physiotherapist that unintentionally influenced the patients’ perception of their treatment, as well as choosing surgery or not. There is a risk that a dedicated physiotherapist may unintentionally influence the patients' perception of their treatment as well as their choice of surgery or not.
One year is a relatively short follow-up period but in the light of previous reports describing early results after ASD and physiotherapy for subacromial pain to be reliable in the long term,8 ,10 ,52 we believe that our results may be long-lasting.
Our findings are in line with previous reports, finding exercise treatment for subacromial pain to be as efficient as surgery,8–10 ,53 but the specific programme used in the present study rendered an even better outcome with a higher number of withdrawals from surgery.31 ,32 Previous studies have reported that physiotherapy is not always prescribed before surgery is considered.54 The present study emphasises that physiotherapy should be part of the management of patients with subacromial pain.
Conclusions
The positive short-term outcomes after our specific exercise programme were maintained and even further improved until the 1-year follow-up, reducing the need for surgery significantly more than unspecific control exercises. Based on these results, we recommend that all patients with subacromial pain, without clinical signs of major cuff tears, should initially be treated with 3 months of specific exercises. The severity of shoulder disability at baseline and the presence of a full-thickness tear seem to influence outcome and the need for surgery.
What are the new findings?
-
Specific exercises reduced the need for surgery for subacromial pain.
-
Results are maintained after 1 year.
-
Patients with a full-thickness rotator cuff tear and a low baseline Constant-Murley score are prone to choose surgery.
How might it impact on clinical practice in the near future?
-
Specific exercises should be the first line of treatment for subacromial pain.
-
Fewer subacromial pain patients require surgery.
-
Specific exercises aid in selecting patients who require surgery for subacromial pain.
-
Patients unsatisfied after specific exercises may reach a satisfactory result after surgery.
Acknowledgments
The authors thank Mats Fredriksson, statistician at the Linköping University, for help with the statistical analyses.
References
Footnotes
-
Contributors HCBH, TH, BÖ, KJ and LEA conceived and designed the study protocol. TH and KJ designed the physiotherapy interventions. HCBH did the statistical analyses with assistance from a statistician employed at the department of medical and health sciences. He was also the blinded assessor. HCBH drafted the manuscript, and TH, BÖ, KJ and LA contributed to the manuscript. All authors read and approved the final manuscript. LA is the guarantor.
-
Funding The study was funded by the Linköping University Hospital, but no other support, financial or other, was received for this study and no financial biases exist for any of the authors or their immediate family.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval The study was approved by the regional committee for medical ethics in Linköping (dnr: M124–07), Sweden (dnr: M124-07), and informed consent was given by all participants.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement The physiotherapy protocols, statistical code and data set are available from the corresponding author.