Article Text

Abstract
Objectives There has been no comprehensive injury report of elite-level amateur boxers in competition and training. We reviewed injuries in training and competition in the Great Britain (GB) amateur boxing squad between 2005 and 2009.
Methods Longitudinal, prospective injury surveillance over 5 years of the GB boxing squad from 2005 to 2009. 66 boxers passed through the squad. The location, region affected, description, and the duration of each injury were recorded by the team doctor and team physiotherapist. We recorded whether the injury occurred during competition or training, and also whether it was a new or a recurrent injury. The injury rate during competition was calculated as the number of injuries per 1000 h.
Results More injuries affected the hand than any other body location. This was the case overall, in training and competition individually, and for both new and recurrent injuries. More injuries occurred during training than during competition, and most injuries were new rather than recurrent. Total injury rate during competition was 828 per 1000 h and hand injury rate in competition was 302 injuries per 1000 h. Hand injury rate in competition was significantly higher than at the other locations. The incidence of concussion is comparatively low.
Conclusions Injury prevention should aim to protect the hands and wrists of elite amateur boxers.
- Concussion
- Boxing/Kick Boxing
- Hand
- Wrist
- Injuries
Statistics from Altmetric.com
Introduction
Modern amateur boxing rules, which are described by the l'Association Internationale de Boxe Amateur (AIDA) Open Boxing (AOB) technical rules, have changed frequently.1 From 2005 to 2009, the rules remained stable and the only major change was the move from four rounds of 2 min to three rounds of 3 min in 2009. Importantly, given the prevalence of hand injuries in boxing, the length of the fabric hand wraps was increased in 2009 to 4.5 m for the competition. A longer fabric hand wrap allows a greater number of turns around the hand, increasing the number of layers of fabric and, in theory, shock absorption. In 2013, headguards were removed and the scoring system was changed.
The greatest proportion of injuries in professional boxing occur to the head and face.2 , 3 A retrospective cohort trial analysing injury during competition in 545 professional boxers recorded 214 injuries in 907 fights over 8.5 years, an injury rate of 24 per 100 fights.2 Open wounds or lacerations to the head and face comprised 62% of injuries, concussions represented 12% of injuries, and hand and finger injury accounted for only 7% of injuries.2 A similar retrospective study recorded 195 injuries in 524 fights over 18 months, an injury rate of 17 per 100 fights or 3.4 per 100 boxer-rounds.3 Facial laceration accounted for 51% of all injuries, followed by hand injury (17%), eye injury (14%) and nose injury (5%).3 These are reports on professional boxers during competition, where they do not wear any form of head protection and they wear hand wraps that afford much more protection than that for an equivalent amateur.
Head and face injuries do not account for the largest proportion of injuries in amateur boxing by location. Timm et al 4 retrospectively collected data in training and competition in relation to amateur boxers from the Olympic training centre in the USA over a 15-year period. In total, 25% of injuries occurred in the upper extremity and 19% to the head or face.4 Porter and O’Brien5 collected data over a 5-month period in 147 amateur boxers separately for training and competition. In competition, head and face injuries predominated: 52% of injuries occurred to the head (concussion only), 20% of injuries occurred to the hand or wrist, and 20% of injuries occurred to the face (including the ear, nose and eye). In training, there were no concussions: 41% of injuries were of the lower extremity, 35% occurred in the hand/wrist, and 10% of injuries occurred to the face. Importantly, few reports have described the split of recurrent and new injuries, or the duration of injuries.
The IOC and the International Boxing Federation (AIBA) are committed to promoting the health of the athlete and injury surveillance underpins these efforts.6 , 7 Therefore, we analysed 5 years of prospectively gathered longitudinal injury data from the Great Britain (GB) boxing squad, in both training and competition.
Methods
The participants included all male boxers on the GB boxing squad at any time between 1 January 2005 and 31 December 2009. Injury data relating to these participants for the same period was released for publication by the English Institute of Sport and the British Amateur Boxing Association, following the 2012 Olympic Games. Data relating to the number of minutes spent competing during this period was gathered for each athlete individually from publicly available information. No data were recorded for the number of minutes spent in training in the same period.
An injury was defined as any musculoskeletal condition that prevented the boxer from participating in either training or competition for >24 h.8 Injuries were coded using a modified Orchard Sports Injury Classification System (V.10)9 which recorded: the location of injury; the bodily region affected by the injury; description of the injury; duration (number of days injured) of each injury; participation when injury occurred (training or competition); and whether the injury was new or recurrent. Recurrence of an old injury was defined as the repeated report of an injury with the same code as the previous injury. Injuries were recorded prospectively by the GB medical team.
Statistical methods
Each athlete's personal (age, gender, and weight classification), participation (training or competition), and injury information (description, location, type, duration, and whether recurring or non-recurring) was entered into an Excel spreadsheet (Microsoft, Seattle, USA). All statistical tests and analysis were performed using R.10 χ2 Tests were performed to identify significant differences in respect of the numbers of injuries incurred in different athlete, participation or injury categories. Z scores were calculated to identify the individual differences. Z scores were appropriate as the entire population of the male GB boxing squad was included for the purpose of data collection. Multiple regression analysis was used to assess differences in respect of the duration of injury across anatomical locations. Significance was accepted at p<0.05 for all comparisons.
Results
Participants
Sixty-six boxers (aged 22.0±2.5 years) were members of the GB boxing squad during the relevant period. The mean time that each boxer was a member of the squad was 2 (range 1–5) years (boxers are given a 1 year rolling contract). The total number of boxer-years in the relevant period was 131.5 years. In the cohort, there were boxers in each weight category from 48 to 91 kg+ (48 kg: 8, 51 kg: 4, 54 kg: 7, 56 kg: 1, 57 kg: 5, 60 kg: 8, 64 kg: 5, 69 kg: 13, 75 kg: 7, 81 kg: 1, 91 kg: 5, and 91 kg+: 2).
Injuries: athlete characteristics
Two hundred and ninety-seven injuries were recorded in the GB boxing squad in the 5 year period. Injuries were sustained by 40 of the 66 boxers (60.6%). Each injured boxer sustained a mean number of 7.4 injuries. There were significant differences in the number of injuries sustained across the weight classes (χ2=90.1, p<0.05), but analysis of Z scores did not permit the identification of which individual weight classes sustained more injuries than the others.
Injuries: anatomical location
Injuries occurred significantly more often in the hand (Z score=3.55) than at the other anatomical locations (table 1). There were no other significant differences between anatomical locations (figure 1).
Number and duration (in days) of injuries in each anatomical location in the GB boxing squad, 2005–2009

Number of injuries by weight class in the Great Britain boxing squad, 2005–2009.
Injuries: competition or training
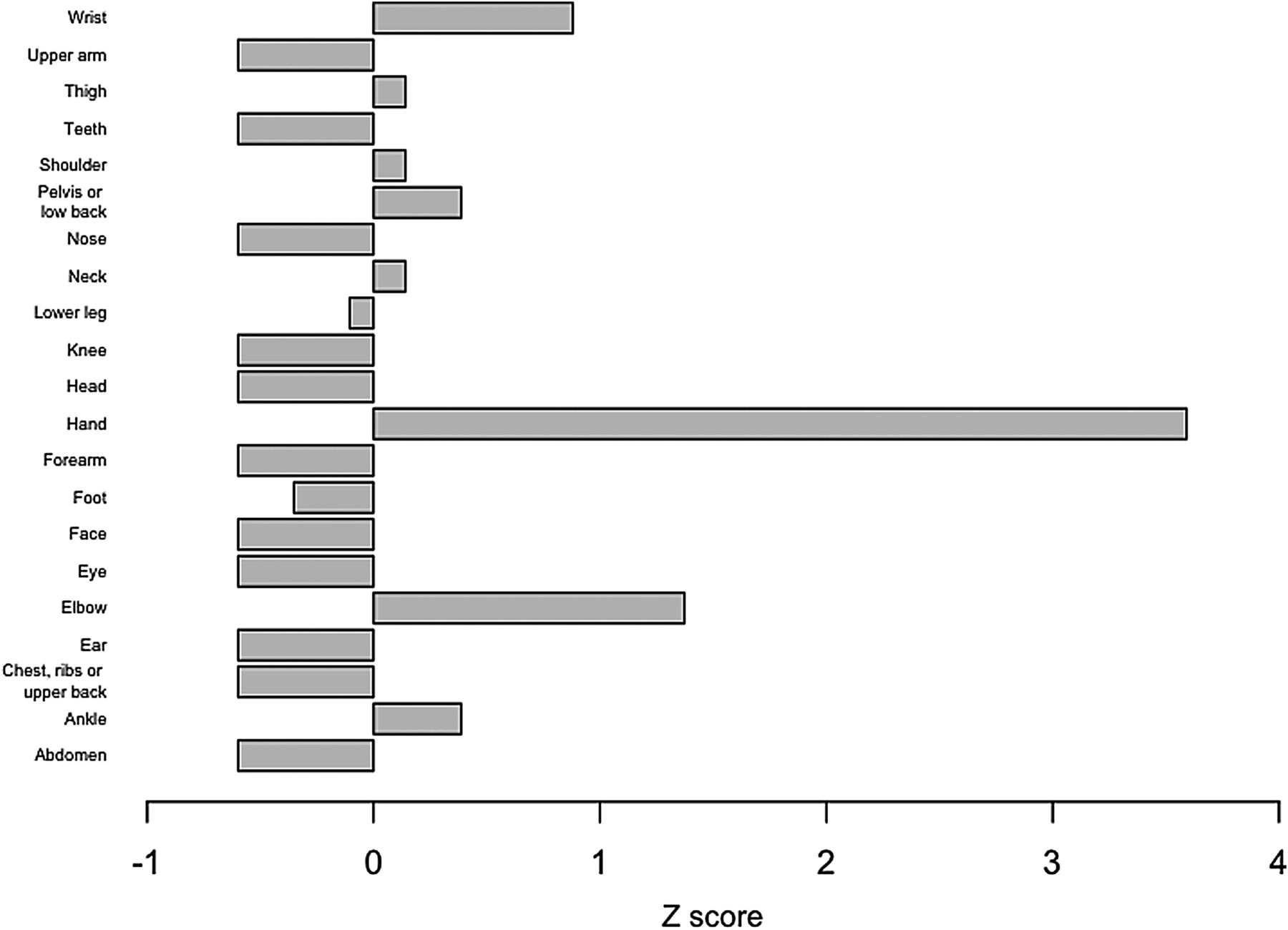
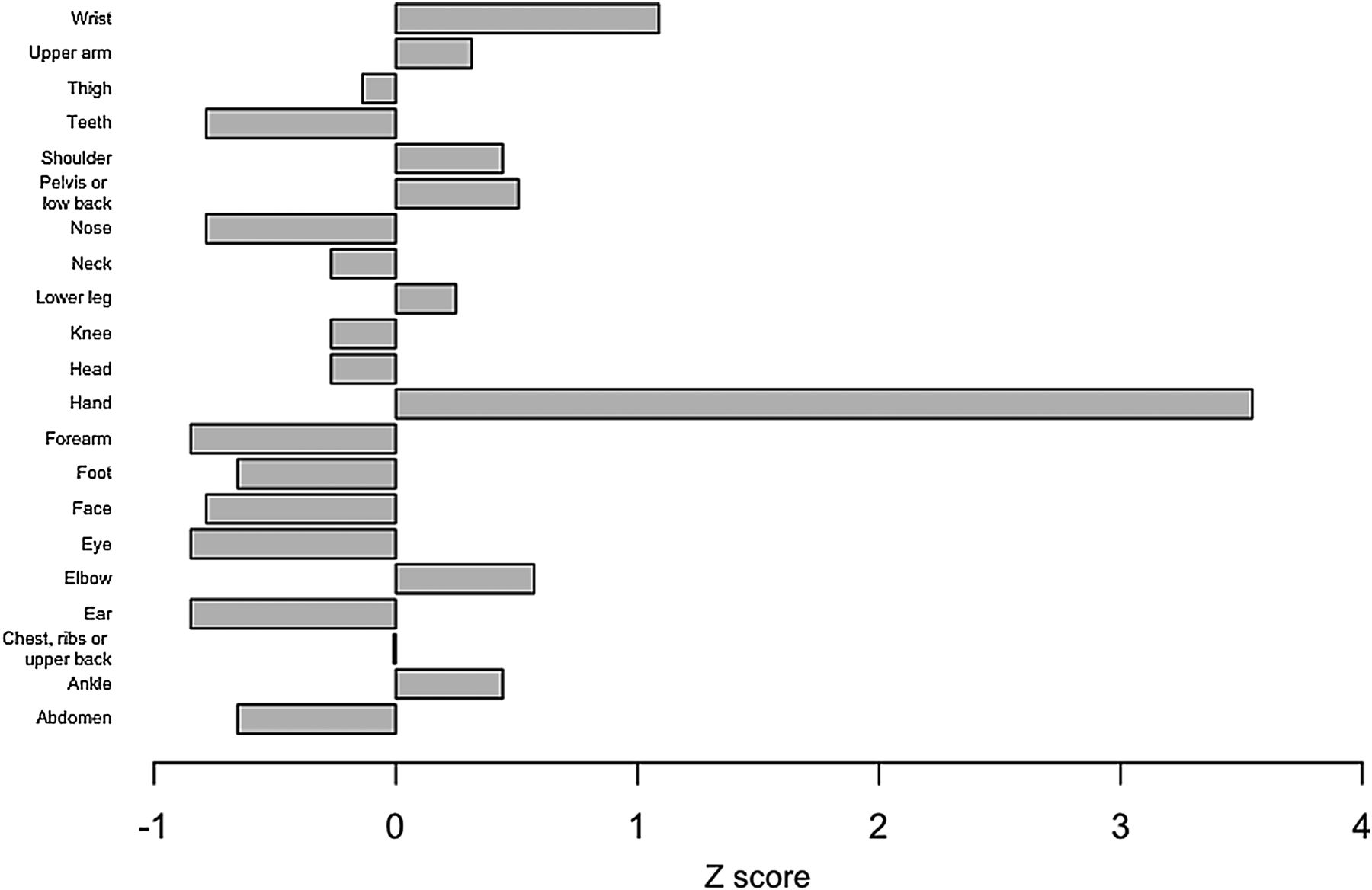
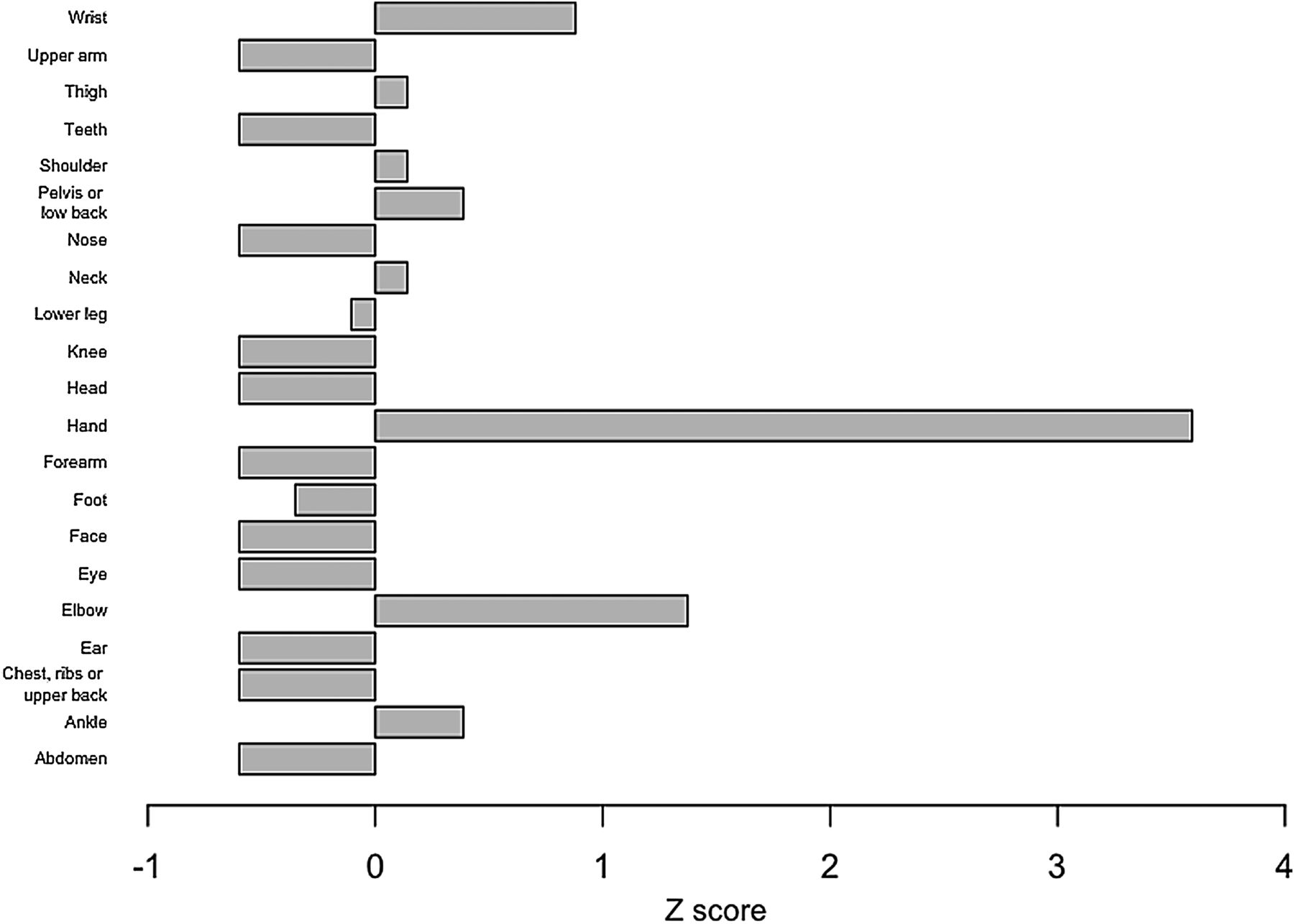
Overall, more injuries were sustained in training than in competition (χ2=49.3, p<0.05). Of the 297 injuries sustained, 209 (70%) were sustained during training and 88 (30%) in competition (29.6%). There were significantly more injuries in the relevant period in the hand in both training (Z score=2.84) (figure 2) and in competition (Z score=3.76) (figure 3) than at other anatomical locations. Hand injuries as a proportion of total injuries in training and competition were 18.2% and 35.2%, respectively. There were no other differences between anatomical locations in either training or competition. Numbers of injuries by anatomical location are provided for the hand (table 2) and the wrist (table 3).
Number of injuries sustained in each anatomical location within the hand in training and competition in the GB boxing squad, 2005–2009
Number of injuries sustained in each anatomical location within the wrist in training and competition in the GB boxing squad, 2005–2009
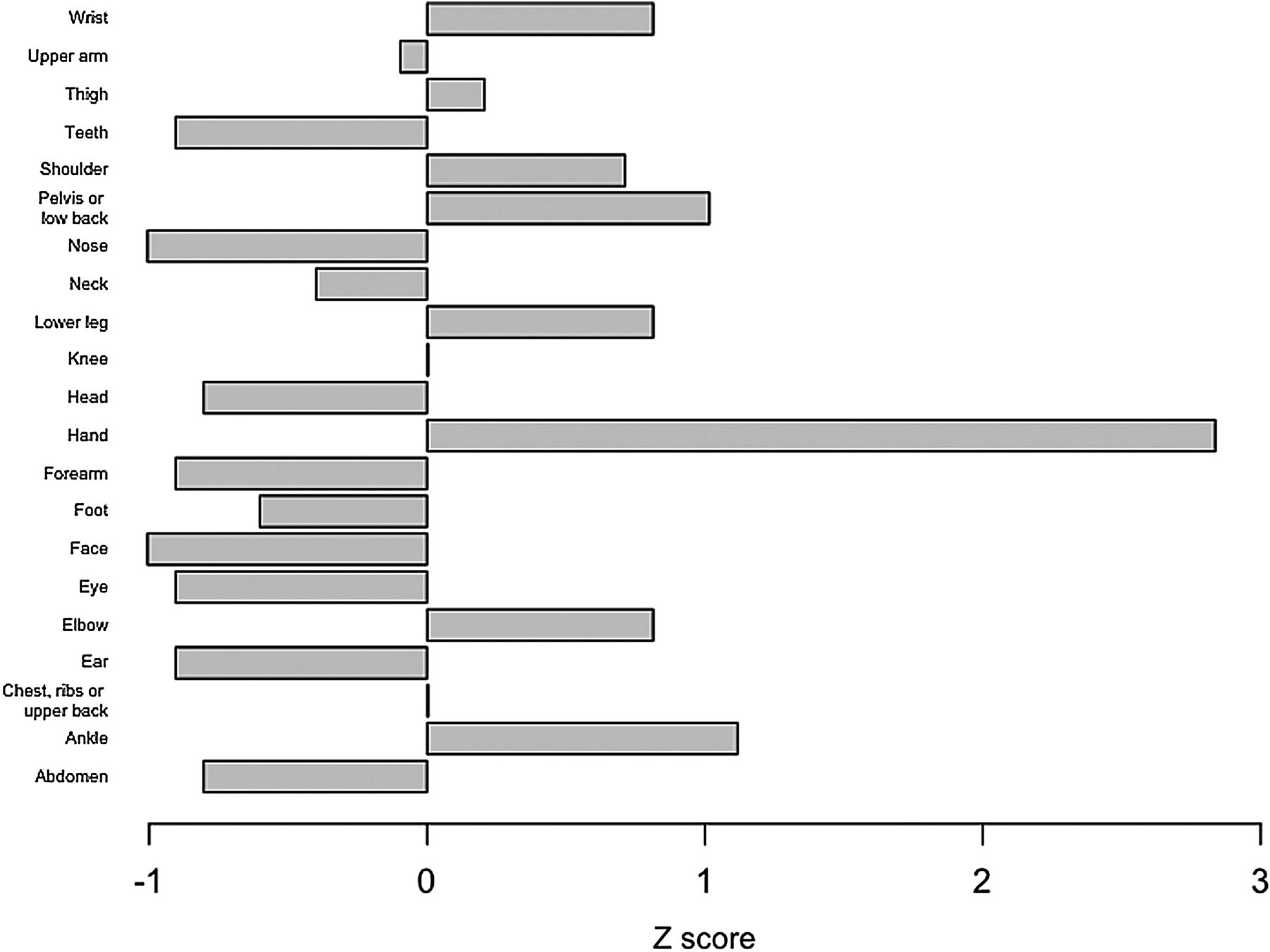
Z scores for the number of injuries in each anatomical location in the Great Britain boxing squad, 2005–2009.

Z scores for the number of injuries in each anatomical location in training in the Great Britain boxing squad, 2005–2009.
Injury rate: competition
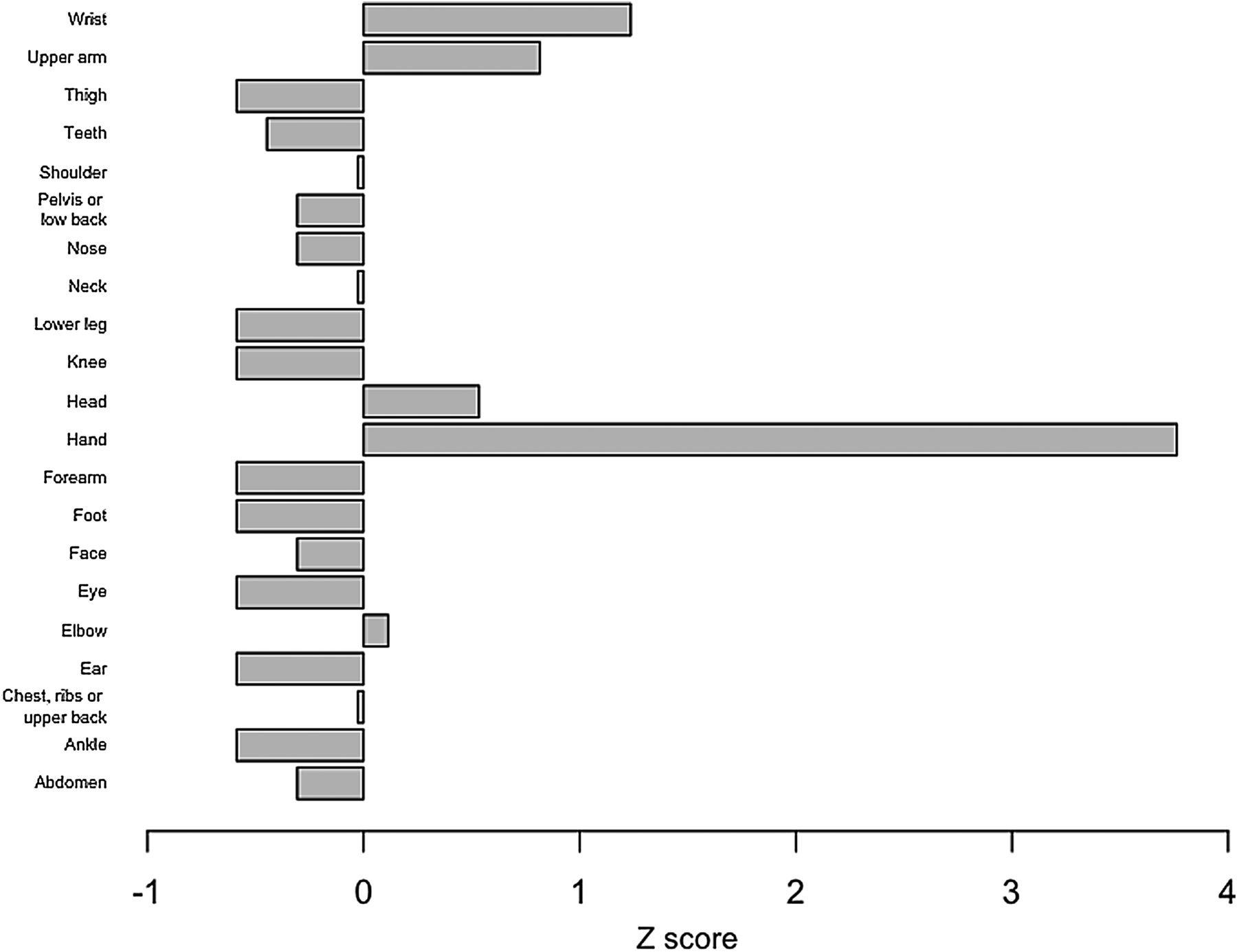
The participants engaged in a total of 6375 min of competition (a mean of 96.6 min per participant, range 2–356 min) during the relevant period, during which 88 injuries were sustained. Thus, the injury rate was 828 injuries per 1000 h of competition time. The injury rate in competition was significantly higher for the hand compared with the other anatomical locations, at 301.6 injuries per 1000 h. There were no other significant differences between anatomical locations in respect of injury rates during competition (figure 4).

Injury rates in each anatomical location in competition in the Great Britain boxing squad, 2005–2009.
Injuries: recurring versus non-recurring
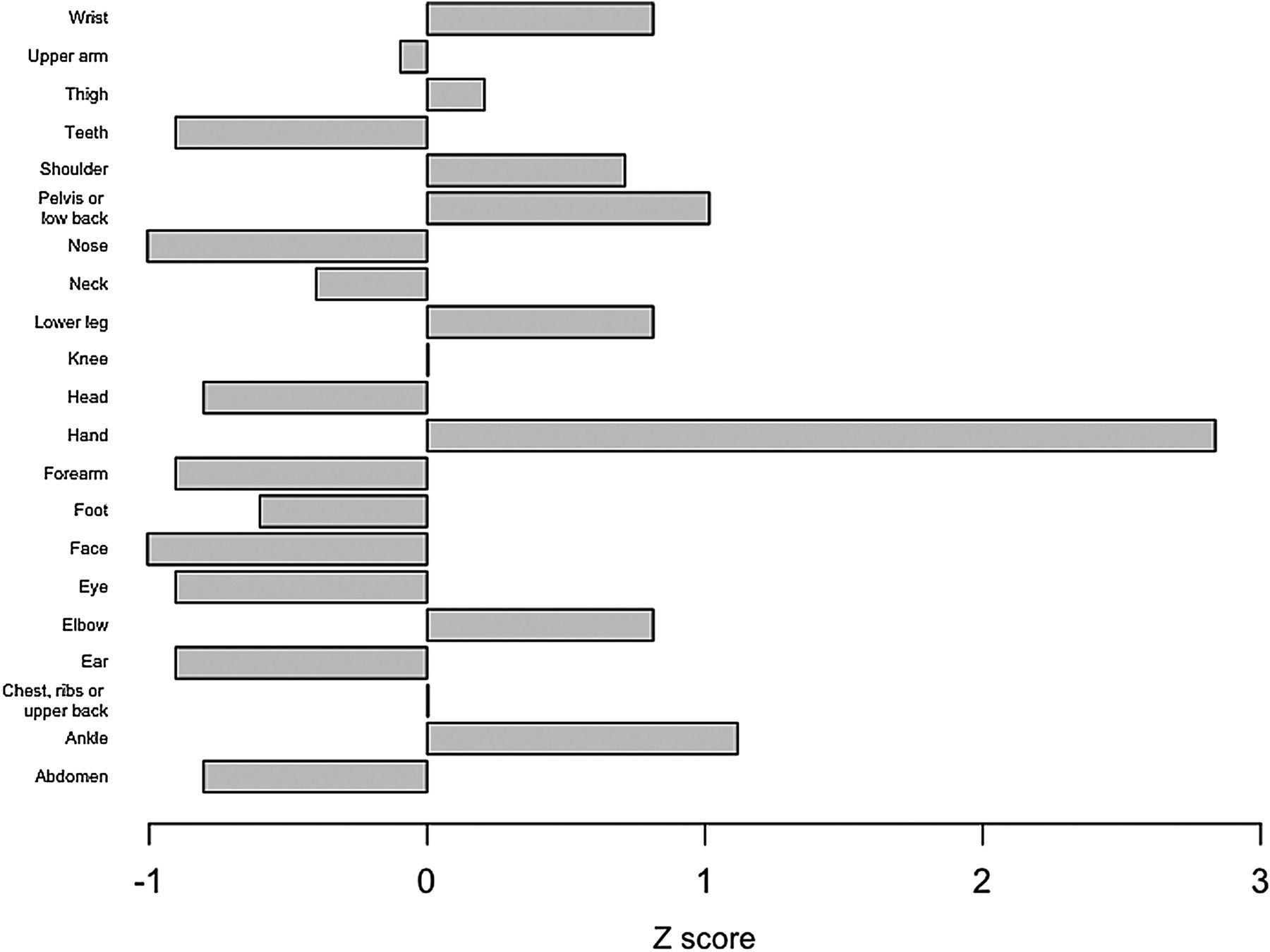
New injuries (n=247, 82.8%) were significantly greater than the number of recurring injuries (n=51, 17.2%) in the relevant period (χ2=128.0, p<0.05). The mean number of recurring injuries per athlete was 1.28 injuries (range 1–8 injuries). The number of hand injuries was significantly greater for recurring (Z score=3.59) (figure 5) and new injuries (Z score=3.41) (figure 6).

Z scores for the number of recurring injuries in each anatomical location in the Great Britain boxing squad, 2005–2009.
Z scores for the number of new injuries in each anatomical location in the Great Britain boxing squad, 2005–2009.
Injuries: type
Only the number of sprain/ligament injuries was significantly greater than the other types for total injuries (Z score=2.27), as well as for both new (Z score=1.99) and recurring (Z score=2.24) injuries individually. The majority of these sprain/ligament injuries were hand or wrist injuries (69%) (figure 7).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Z scores for the number of injuries by type in the Great Britain boxing squad, 2005–2009.
Time lost to injury
The total duration of time lost to injury as a result of all 297 injuries was 9820 days and the mean duration of time lost for an injury was 33 days. The mean duration of time lost to hand injuries (50.7 days) was second highest to the eye (370 days). The occurrence of these injuries was significantly higher than all other injuries. The eye condition was superior limbic keratoconjunctivitis and only affected one boxer. Whether this result is meaningful is doubtful, as this rare condition has not previously been associated with boxing.
Discussion
At the elite-level amateur boxing, the hand was the most commonly injured location (across both training and competition, and across both recurrent and new injuries), while sprains and ligament injuries were the most common type of injury. Most of the sprains and ligament injuries were to the hand and wrist.
Hand injuries
The hand has previously been identified as the location that incurs a high injury risk in amateur boxers4 but not in professional boxers.2 , 3 Differences in hand injuries between amateur and professional boxing might be explained by the amount of protective bandage and tape used. In professional boxing, the amount of bandage and tape used is only limited by the ability of the boxer to insert his wrapped hand into the boxing glove; however, in amateur boxing there is a set limit in competition. It is also possible that injury risk changes in elite rather than club boxers because of the very large impact forces that are displayed by elite boxers.11–13 Such impact forces might reasonably be expected to lead to hand damage, particularly where padding is minimal (as in competition) or when performed over a repeated period of time (as in training).
It is noteworthy that the hand is the location most likely to be injured in competition, as this occurs despite a comparatively short time throwing punches in competition compared with training. Differences between training and competition might account for these results. First, during training, it is allowable to use as much hand wrapping as desired, including tape and padding. During competition, hand bandaging is limited. In the period of this study, hand protection in amateur boxing consisted of up to 2.5 m (4.5 m from 2009) of crepe bandage and no adhesive tape. Second, during training, heavier gloves (up to 18 oz in weight with more stuffing) are worn. Only 10 oz gloves are worn in competition. Finally, during training, punches are thrown in controlled conditions, including hitting bags and sparring, and many punches are ‘pulled’ (a boxing term for not making full contact) but in competition, punches are thrown against a moving target and are not pulled. Thus, differences in respect of hand wrappings, gloves or punching conditions might be responsible for the high level of hand injury in competition despite the small number of punches in comparison with training, but it is unclear why this group of boxers suffered so many hand injuries on the overall.
Head/face injuries lacerations
The level of head and face injury in our study was lower than the published data on professional boxing,2 , 3 , 5 , 14 and broadly in line with data from amateur boxing.2 , 3 Zazryn et al 2 reported that facial lacerations were the most common injury in professional male and female boxers in Victoria, Australia, accounting for 62% of all injuries. Bledsoe et al 3 found that facial lacerations were the most commonly occurring type of injury in professional male and female boxers in the USA, accounting for 51% of all injuries. Reports for amateur boxing15 show lower numbers of facial injuries, which is likely due to the wearing of headguards in amateur boxing. Previous studies have suggested that facial cuts were reduced with the introduction of headguards in 1984.16 Ever since headguards were removed in 2013, there has been an increase in facial cuts in competition.
Concussion, eye injuries, and headguards
The level of concussions was much lower in the GB squad than has been previously recorded in professional boxers.2 , 5 Zazryn et al 2 found that concussions were the second most commonly occurring type of injury in competition in professional male and female boxers in Victoria, Australia, accounting for 12% of all injuries. Similarly, Porter and O'Brien5 found that concussions were the most commonly occurring type of injury in amateur male boxers in Ireland in competitions, accounting for 52% of all injuries. A key finding in our 5-year study was that of no concussions occurring in training and only five cases in competition, that is 0.53 concussions every 1000 h. In a similar study over a 4-year period in elite English rugby league, 35 concussions were reported.17 Despite disagreement with previous studies, the low incidence of concussion in this boxing cohort concurs with earlier studies finding little evidence of chronic traumatic brain injury in amateur boxing.18 , 19
A common concern in professional boxing is the occurrence of eye injuries, including detached retina. There were no detached retinas in our 5-year study and only one eye injury was recorded.
Headguards which offer a degree of protection to the face, ears and eyes likely contributed to the low number of head, facial, ear and eye injuries in the GB boxing cohort. Headguards worn in training by amateur boxers are often significantly larger and provide more facial protection than those worn in competition.
Other injuries
Some studies have noted that amateur boxers might incur overuse injuries of the lower limb from the running that they perform for conditioning.5 Despite the boxers in this cohort running almost every day, the percentage of injuries affecting the lower limb was just 21.6%. In contrast, studies in elite football have reported lower limb injury rates of 75.0%20 and 73.5%.21 This is possibly because the distance over which boxers run is short (4–6 km) and does not involve quick changes in pace or direction or collisions with other athletes. In the boxing ring, changes in direction are required, but this running is not done with high velocity and does not produce high shear forces compared with cutting in soccer. It may also be relevant that boxing training itself is performed on a sprung surface, which may reduce ground reaction forces.
In this study, the overall injury rate observed in competition of 828 per 1000 h might initially appear high, particularly when compared with other sports. However, it is broadly in line with observations in previous investigations among amateur boxers that have used a similar prospective cohort study design. Zazryn et al 14 reported that the overall injury rate in competition was 1220 injuries per 1000 h, and calculated that the injury rate in competition observed by Porter and O'Brien5 was 920 injuries per 1000 h.
Limitations and strengths
Our primary limitation was that we could not collect reliable information about total training hours in the relevant period. Thus, while we were able to report injury rates of 828 per 1000 h of competition time, we were not able to report comparable injury rates for training. Nevertheless, we estimate there were between 900 and 1200 training hours per boxer per year providing rates between 0.7 and 1.8 injuries per 1000 h, respectively. Zazryn et al 14 reported the overall injury rate in training among amateur boxers was just 0.5 injuries per 1000 h, which is considerably lower than during competition and correlates with our findings. Another limitation was that the population of the study changed during the study, with an individual boxer remaining on the squad for a mean of 2 years. Following a static population would have been preferable. Additionally, data were not collected in relation to modifiable factors that might be relevant for an understanding of why hand injuries occurred. In light of the rule changes in AOB since the period of this study, particularly the removal of headguards in 2013, the pattern of injuries since 2013 may well be different. In the light of the new regulations, removing headguards from amateur boxers, and biomechanical studies showing that the glove/headguard combination reduces transmitted forces; further work is required to investigate the injuries sustained by amateur boxers today.22
The strengths of this study are that the data has been collected prospectively by the same practitioner over the 5-year period of the study. The boxing squad was centralised; therefore, an injury date and accurate return to full fitness was recorded, which produced an accurate measurement of the time the athlete was injured.
Future studies should explore whether biomechanical, anatomical, or other physical differences between boxers predispose certain athletes to greater risk of hand injury than others. Moreover, future investigations should explore whether differences between wrapping techniques or between lengths of wrapping used lead to a greater risk of hand injury.
In conclusion, the hand was the most commonly injured location, and sprains and ligament injuries were the most common type of injury in elite-level, amateur boxing. Most of the sprains and ligament injuries were to the hand and wrist. Thus, our study identifies a clear need for developing hand injury prevention interventions.
What are the new findings?
-
This study presents the first longitudinal, prospective study of a national squad in both training and competition.
-
The hand is the most common location injured.
-
The incidence of concussion is comparatively low.
How might it impact on clinical practice in the near future?
-
Greater hand and wrist protection is required.
-
More attention given to wrapping hands might be beneficial. This could include more time for hand wrapping being allowed, or hands being wrapped by a physiotherapist prior to competition.
-
The international federation should consider the use of more tape, padding and larger gloves in competition.
Acknowledgments
The authors acknowledge British Amateur Boxing Association and English Institute of Sport.
References
Footnotes
-
Competing interests None declared.
-
Provenance and peer review Not commissioned; externally peer reviewed.