Article Text

Abstract
Background Physical inactivity accounts for 9% of all deaths worldwide and is among the top 10 risk factors for global disease burden. Nearly half of people aged over 60 years are inactive. Efforts to identify which factors influence physical activity behaviour are needed.
Objective To identify and synthesise the range of barriers and facilitators to physical activity participation.
Methods Systematic review of qualitative studies on the perspectives of physical activity among people aged 60 years and over. MEDLINE, EMBASE, CINAHL, PsychINFO and AMED were searched. Independent raters assessed comprehensiveness of reporting of included studies. Thematic synthesis was used to analyse the data.
Results From 132 studies involving 5987 participants, we identified six major themes: social influences (valuing interaction with peers, social awkwardness, encouragement from others, dependence on professional instruction); physical limitations (pain or discomfort, concerns about falling, comorbidities); competing priorities; access difficulties (environmental barriers, affordability); personal benefits of physical activity (strength, balance and flexibility, self-confidence, independence, improved health and mental well-being); and motivation and beliefs (apathy, irrelevance and inefficacy, maintaining habits).
Conclusions Some older people still believe that physical activity is unnecessary or even potentially harmful. Others recognise the benefits of physical activity, but report a range of barriers to physical activity participation. Strategies to enhance physical activity participation among older people should include (1) raising awareness of the benefits and minimise the perceived risks of physical activity and (2) improving the environmental and financial access to physical activity opportunities.
- Aging
- Elderly people
- Exercise
- Physical activity
Statistics from Altmetric.com
Introduction
Physical inactivity is responsible for 9% of all deaths worldwide.1 In the 2010 Global Burden of Disease Study, physical inactivity was among the top 10 risk factors for global disease burden accounting for 3.2 million deaths and 2.8% of the total disability adjusted-life years.2 Inactivity is a pandemic condition, with far reaching health, economic, environmental and social consequences.3
Despite the well-known benefits of physical activity, 30% of the world's population fails to reach the levels of physical activity recommended for health benefits.4 The situation is even more critical with increased age as around 45% of people aged over 60 do not meet the recommended level of physical activity.4 The proportion of those who do not meet the recommended guidelines increases to 75% for those aged 75 and over.5 This is a rapidly increasing problem as the number of people aged over 65 years in the world is expected to triple in the next 30 years.6 Given this projected trend in population ageing, older people's engagement with physical activities is a public health concern worldwide. Several countries7–9 as well as the WHO10 have issued physical activity guidelines with recommendations specifically for older adults (see box 1).
Recommended levels of physical activity for older adults (adapted from WHO global recommendations on physical activity for health9)
Older people should do at least 150 min of moderate-intensity aerobic physical activity throughout the week or do at least 75 min of vigorous-intensity aerobic physical activity throughout the week or an equivalent combination of moderate-intensity and vigorous-intensity activity.
Aerobic activity should be performed in bouts of at least 10 min duration.
For additional health benefits, adults aged 65 years and above should increase their moderate-intensity aerobic physical activity to 300 min per week, or engage in 150 min of vigorous-intensity aerobic physical activity per week, or an equivalent combination of moderate-intensity and vigorous-intensity activity.
Older people, with poor mobility, should perform physical activity to enhance balance and prevent falls on 3 or more days per week.
Muscle-strengthening activities should be done involving major muscle groups, on 2 or more days a week.
When older people cannot do the recommended amounts of physical activity due to health conditions, they should be as physically active as their abilities and conditions allow.
Older people's engagement with physical activities can be influenced by behavioural factors, such as motivation and personal beliefs, as well as environmental factors, including availability of public transport and exercise venues. Qualitative research can provide better understanding of older people's experiences, beliefs and attitudes towards participation in physical activities and help us translate the strong evidence of benefits of physical activity into practice.11 Previous reviews focusing on specific ethnic groups12–14 or programmes to prevent falls15 have been undertaken in this area, but the inclusion of a targeted population or physical activity type has limited the generalisability of results.
To guide policy for a broad range of community programmes focusing on the promotion and sustainability of active lifestyles, we conducted a comprehensive synthesis that included the perspectives of older people on physical activity. We investigated whether participants’ views differed according to type of physical activity investigated. To increase programme uptake and sustain adherence over time at a population level, it is necessary to identify facilitators and barriers to physical activity that are common across different contexts. Such factor can then inform effective population-wide physical activity policies and strategies.
Methods
We followed the Enhancing Transparency of Reporting the Synthesis of Qualitative research (ENTREQ) framework. ENTREQ is a framework for reporting systematic reviews and syntheses of primary qualitative research. ENTREQ consists of 21 reporting items grouped into five domains: introduction, methods and methodology, literature search and selection, appraisal of included studies, and synthesis of the findings.16
Search strategy and selection criteria
Comprehensive searches were conducted in MEDLINE, EMBASE, CINAHL, PsychINFO and AMED from inception until 14 June 2013. The search strategies are provided in the online supplementary appendix table S1. We also searched reference lists of relevant studies. The search was restricted to studies published in English, Spanish and Portuguese. Qualitative studies published in peer-reviewed journals that explored older people's perspectives on physical activity were included. Studies were included if all participants were at least 60 years of age, or if the mean reported age of participants was 60 years or over. We considered physical activity to include a range of domains such as leisure, sport, transport and household activity as well as structured exercise programmes. Studies investigating physical activity in a population with a specific health condition (eg, coronary heart disease, diabetes) were considered ineligible because people with particular conditions are likely to have perspectives on physical activity that are unique to that condition and less applicable to the general older population. Structured surveys were excluded. Two independent reviewers (MRF and RZP) screened the titles and abstracts, discarded those that did not meet the inclusion criteria and evaluated full-text versions of potentially relevant studies for eligibility.
Comprehensiveness of reporting
Comprehensiveness of reporting of each primary study was assessed using the consolidated criteria for reporting qualitative research (COREQ) framework, which includes three domains: research team and reflexivity (acknowledgement of the role and influence of the researcher on the research process); study methods; and data analysis and reporting.17 Assessment of reporting allows readers to assess the trustworthiness and transferability of the study findings to their own setting.18 Two independent reviewers (MRF and RZP) assessed each study and resolved any disagreements by discussion.
Data synthesis and analysis
We used thematic synthesis to synthesise the findings.18 Participant quotations and text under the ‘results’ or ‘findings’ sections from each study were entered verbatim into HyperRESEARCH V.2.8.3 (ResearchWare Inc., Randolph, Massachusetts, USA) software. One reviewer (MRF) performed line-by-line coding of the findings of the primary studies and recorded concepts on the older adult perspectives on physical activities. Translation of concepts across studies was then performed by grouping similar concepts and creating new ones when necessary. All included studies were re-read to ensure that relevant data were captured and appropriately integrated into preliminary themes and subthemes. All authors reviewed the preliminary analysis to ensure that key data were captured from included studies; and discussed concepts for similarities and differences.19 An analytical thematic schema was also developed to extend the findings of primary studies, by identifying conceptual links across themes and using mind mapping software Freemind V.0.9.0 Beta 14 (Source-Forge Inc., Mountain View, California, USA).
We also conducted a stratified analysis to investigate whether the themes and their subthemes differed according to type of physical activity. The type of physical activity investigated in the included studies was categorised into three groups: structured exercise programmes, other forms of physical activity or combination of both (ie, structured exercise programmes and other types of physical activity). When a study clearly referred to a subset of physical activity considered to be planned, structured and repetitive for the purpose of conditioning any part of the body, the study was categorised as structured exercise programme. Exercise programmes for falls prevention, yoga, Tai Chi, line dancing, walking groups and programmes that incorporated different types of training such as strength, balance, aerobic and/or flexibility were considered as structured exercise programmes. When a study clearly referred to physical activities other than structured exercise programmes, such as household activities, walking for leisure or transport, other forms of active transport, running and other leisure-time physical activities, the study was categorised as other types of physical activity. When a study referred to any type of physical activity, the study was categorised as a combination of structured exercise programmes and other types of physical activity. Our stratified analysis compared themes and subthemes between structured exercise programmes and other types of physical activity.
Results
Literature search results
In total, 132 studies involving 5987 participants were included (figure 1). Characteristics of included studies are described in the online supplementary appendix table S2. The mean age reported among included studies ranged from 60 to 89 years. The studies were conducted in 24 countries with most conducted in the USA (42%), UK (14%) and Canada (14%). Twenty-four studies (18%) restricted participant inclusion to indigenous or immigrant populations (eg, Korean and Vietnamese immigrants living in the USA; South Asians living in England). In the majority of included studies (85%), participants were considered community dwellers. Fewer studies (15%) included participants from long-term care facilities, assisted-living facilities and hospitals. Sixty-one studies (46%) investigated specifically structured exercise programmes, such as exercise for falls prevention, strength training, yoga and walking groups, whereas 22 studies (17%) focused on other types of physical activities, such as walking and leisure-time physical activities. The remaining 48 studies (37%) covered other types of physical activities as well as structured exercise programmes. Table 1 provides detailed information on the studies that reported on each subtheme. This information is also shown stratified by different types of physical activity. The majority of included studies (98%) used focus groups or interviews to collect data.
Illustrative quotations and references reporting each subtheme

Search process and results.
Comprehensiveness of reporting
The comprehensiveness of reporting varied across studies, and ranged from 2 to 15 of the 18 items of the COREQ framework being reported (see online supplementary appendix table S1). More than 85% of the included studies reported the participant selection strategy, audio/visual recording, and provided participant quotations. Less than 30% of studies reported on data saturation, use of software and participants’ feedback given on preliminary findings.
Synthesis
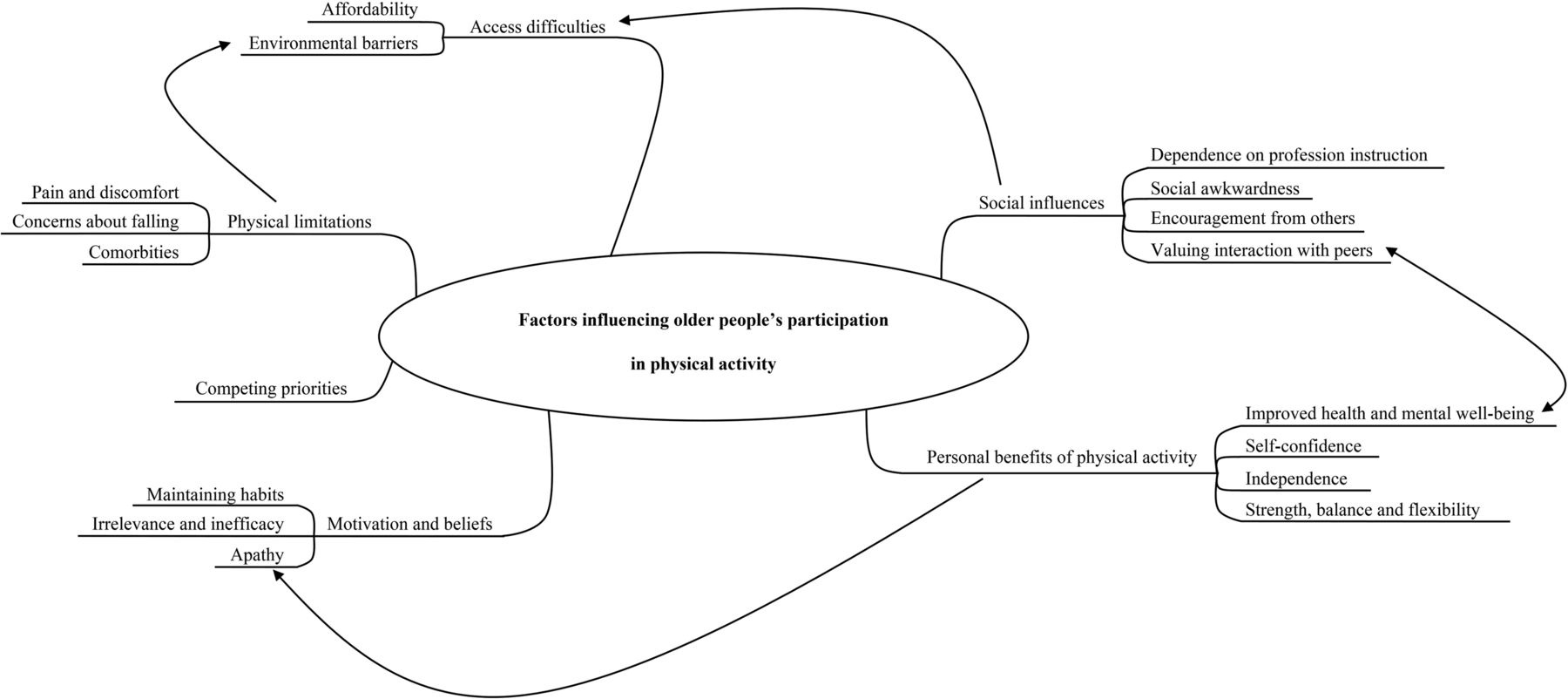
We identified six major themes reflecting older people's perspectives on physical activity: social influences; physical limitations; competing priorities; access difficulties; personal benefits of physical activity; and motivation and beliefs. These major themes and their subthemes are discussed below. Selected quotations to illustrate each subtheme are provided in table 1. Figure 2 shows the thematic schema we developed to illustrate the inter-relationships between the themes.

{kind=link}
{kind=link}
Thematic schema illustrating conceptual interactions among valuing interaction with peers and improved health and mental well-being, personal benefits of exercise and apathy, physical limitations and environmental barriers, and access difficulties and social influences.
Social influences
Valuing interaction with peers
Participants from 84 (64%) studies valued the social contact and enjoyed seeing familiar faces or neighbours when performing physical activities, or preferred group-based activities as they could gain a sense of belonging, enjoyment and establish friendships, and reported that this motivated them to continue with the activity. Some participants, especially men, appreciated friendly and fair competition. Good rapport with instructors also motivated participants to continue exercising in a group.
Social awkwardness
In 29 (22%) studies, participants reported a lack of confidence in social settings and were apprehensive about meeting others, particularly in group-based physical activities that involve people of different ages, gender, physical capabilities or cultural backgrounds. Some felt more self-conscious and intimidated in a group that also included younger people, and felt unable to keep up with those who could exercise at a more advanced level. The perceived pressure to keep pace with the class and complete the exercise routines led to a sense of incompetence and disconnection from others. Moreover, participants from ethnic minority groups suggested cultural sensitivity should be considered when promoting physical activity. For example, some Muslim women would not exercise in groups with men due to religious practices requiring gender segregation.
Encouragement from others
In 82 (62%) studies, participants considered support from others to be essential. Support included verbal encouragement, practical help (transportation) or purchased exercise equipment (pedometer, bike) provided by friends and family. Some participants, particularly those who felt more vulnerable, were reluctant to start physical activities without advice from health professionals. Others felt confident, but reported participation in physical activities to be difficult due to the lack of encouragement or overprotectiveness from others who participants thought were unnecessarily concerned for their safety.
Dependence on professional instruction
In 40 (30%) studies, participants believed that the presence or the quality of exercise instructors influenced physical activity behaviour. Exercise without an instructor was perceived as not being safe, whereas exercises that were tailored to the participant's physical capacity and individual needs were appreciated.
Physical limitations
Pain or discomfort
Participants reported experiencing a range of unpleasant sensations, including muscle aches, chest pain, shortness of breath and dizziness, and these were reported to influence physical activity behaviour in 45 (34%) studies. Physical activity was perceived as being both physically and emotionally demanding and high-intensity physical activity was considered distressing and intolerable. In contrast, inactivity was occasionally recognised as an aggravator for existing pain and some participants remained physically active to cope with or to relieve pain.
Concerns about falling
In 37 (28%) studies, participants feared falling and sustaining serious injuries during physical activities, and lacked confidence to exercise independently. Some reported that physical activity would increase their risk of injury given their frail status. Past falls increased participants’ anxiety about exercising.
Comorbidities
Participants in 74 (56%) studies believed that symptoms and physical limitations caused by existing comorbidities prevented them from exercising. These comorbidities included different health conditions, for instance cancer, urinary incontinence and musculoskeletal disorders. Moreover, participants also reported feeling physically unable to take part in any activity due to poor general health. In contrast, some vigilantly exercised to control chronic conditions, such as hypertension and arthritis.
Competing priorities
In 53 (40%) studies, participants reported having little or no time to perform physical activity due to work and family responsibilities. Some felt that taking care of frail partners and grandchildren was more important than exercising.
Access difficulties
Environmental barriers
Environmental barriers, such as poor access to transport, unsuitable weather, neighbourhood safety, and unavailability of exercise programmes and equipment, were reported in 72 (55%) studies as barriers to physical activity participation. Participants felt unfit and unable to use public transport, when they would need to catch multiple buses, travel for long distances or wait for extended periods. In rural areas, lack of transport options was identified as being an important barrier. Moreover, frail participants living in care homes reported having to rely on others to take them to exercise venues, and appreciated benches placed along the corridor so they could rest. Participants also reported feeling vulnerable when having to walk in busy or unsafe neighbourhoods that demanded more of their attention. Adequateness of pedestrian access to roads, such as short green pedestrian traffic light was also noted as a barrier. Some looked for safer opportunities and preferred walking in shopping centres. Some participants enjoyed walking in quiet areas with attractive scenery.
Affordability
Costs associated with physical activity programmes were considered a major barrier to participation in 32 (24%) studies. Some participants said that they were unable to afford the high costs associated with these programmes but some participants expressed their unwillingness to spend money on physical activity, suggesting that free or government subsidised exercise classes could increase physical activity uptake.
Personal benefits of physical activity
Strength, balance and flexibility
Participants from 69 (52%) studies believed that physical activity would enhance their physical status, resulting in an improvement in muscle strength, balance or flexibility. Some recognised physical activity as an important strategy to reduce the risk of falls, improve mobility and slow the ageing process.
Self-confidence
In 23 (17%) included studies, mastering an activity gave participants a sense of competence that encouraged them to maintain exercising. Some participants experienced an intense improvement in self-esteem and in the sense of self-worth, feeling enthusiastically able to take part in competitions.
Independence
Participants from 26 (20%) studies wanted to avoid having to rely on others and be able to care for themselves and felt that exercising maintained their independence and preserved their sense of self-value. Some participants stated that consideration for family members and taking care of grandchildren was an important reason to stay active.
Improved health and mental well-being
In 103 (78%) studies, participants believed that physical activity was important to maintain general health, to improve mood and relieve stress. Specifically, physical activities were perceived to aid digestion, blood circulation, longevity, weight control, sleep quality and breathing. An immediate improvement in mental alertness was perceived which gave participants the notion that physical activity could effectively prevent mental illness.
Motivation and beliefs
Apathy
Participants from 52 (40%) studies reported that apathy influenced their active behaviour. Some expressed disinterest in physical activity believing that they would not derive any health benefit. However, others—although clearly acknowledging the benefits of physical activity—reported that laziness or low motivation prevented their participation in such activities. In contrast, some participants were proactive in seeking opportunities and demonstrated their willingness to learn and do everything to improve their health.
Irrelevance and inefficacy
In 32 (24%) studies, participants believed that exercise was unnecessary for older adults and may even be harmful. Some participants felt that health inevitably deteriorated with ageing, and that physical activity could not slow this natural process. Others considered that they were too young to fall, and thus, exercise to prevent falls was irrelevant. The notion that falls cannot be prevented but occur by chance or as a result of divine forces, fate or luck was also commonly reported by Chinese people.
Maintaining habits
Participants from 31 (24%) studies reported that their earlier lifestyle influenced their current active behaviour. Some stated being physically active at an older age as the result of having always been physically active, whereas others who had never engaged in any regular physical activity were reluctant to start exercising in the old age.
Stratified analysis based on different types of physical activity
Table 2 shows the number of studies categorised as structured exercise programmes and other types of physical activity per themes and subthemes. The stratified analysis revealed that four subthemes (dependence on professional instruction, pain or discomfort, affordability, strength, balance and flexibility, and self-confidence) seemed more relevant to structured exercise programmes, whereas two other subthemes (environmental barriers and maintaining habits) seemed more relevant to other types of physical activity.
Number (and proportion) of studies grouped by type of physical activity per themes and subthemes
Discussion
This study has shown that some older people believe in the potential of physical activity to improve physical and mental well-being, but key barriers for their participation include lack of social support, previous sedentary habits, competing priorities, accessibility and apathy. Older people also feel they lack the capacity to engage in physical activity because of their perceived frailty and deem age-related deterioration as being unavoidable and unpreventable.
The ecological model of determinants of physical activity proposed by Bauman et al20 can assist the interpretation of our findings. This ecological model is a comprehensive multilevel framework, which includes contributors to an active behaviour at all levels: individual, social, environmental and policy. Our systematic review has identified four themes, which can be categorised as contributors at the individual level: physical limitations; competing priorities; personal benefits of physical activity; and motivation and beliefs. Not surprisingly, some older people seem to have understood the personal benefits of physical activity and its impact on their independence, general health and mental well-being. However, despite the irrefutable evidence demonstrating the benefits of physical activity,21 ,22 some still believe that physical activity is unnecessary or deleterious, increasing the risk of injury.
Participation in physical activity can also be commonly associated with pain and discomfort and some older people believe that comorbidities necessitate sedentary behaviour. Yet well-designed physical activity programmes can actually assist with the management of pain and many common health conditions.23 To overcome the misbelief that physical activity is potentially harmful, educational strategies at population level should focus on communicating the role of physical activity in gaining health benefits for all24 ,25 as well as how well-designed physical activity programmes can help the management of common comorbidities in this age group, such as cardiovascular conditions,26 stroke,27 impaired cognitive function28 and arthritis.29 There also needs to be education of health and exercise professionals to ensure that appropriate programmes are readily available for all older adults.
The remaining two themes (social influences and access difficulties) identified in our review refer to the social and environmental levels, respectively, described in the ecological model by Bauman et al.20 The importance of social interactions inherent to group activities was evident in a large proportion of the included studies. Most participants felt more comfortable to exercise under professional supervision and around people with similar age and background. Interestingly, interaction with peers or instructors was also considered an important motivational factor to drive uptake of those activities that otherwise could be performed individually, such as walking. Provision of group activities as well as other type of supervised activities, which facilitate social interaction should also be considered by policymakers to promote an active lifestyle in this age group. At the environmental level, poor access to transport and lack of adequate venues to safely exercise were reported as access difficulties to sustain an active lifestyle. Despite the importance of building an environment that promotes active behaviour,30 adequate and accessible public transport to exercise venues remains essential for older people. Notwithstanding, these themes are intrinsically correlated, as shown in figure 2, and should be viewed in this context. For instance, the physical limitations of older people seem to influence their perception of environmental barriers, whereas the perceived benefits of physical activity seem to affect older people's motivation towards participation.
Our findings are broadly consistent with the findings of previous qualitative reviews focusing on ethnic minority groups12–14 and mixed methods reviews on programmes to prevent falls15 and on the oldest old,31 which found factors that influence older people's behaviour towards physical activity to include motivation and beliefs, social influences and environmental barriers. A strength of our review is the breadth and comprehensiveness of our results, which are relevant to the general older population and to a range of physical activities. We have included 132 qualitative studies which is a considerably larger number than the four previous systematic reviews with narrower research questions (n=38,12 n=11,13 n=1814 and n=2415). In addition, we included articles in Spanish and Portuguese as well as English. Our review provides a pragmatic and analytical framework that synthesises data from 5987 participants in different healthcare contexts, including participants from developed and developing countries, urban and rural populations, ethnic minority and cultural majority groups. Despite these diverse contexts, many of the themes identified were described repeatedly in a large number of included studies, revealing consistency of results across studies.
The themes which emerged from this review enabled us to delineate and explain in detail factors influencing physical activity participation from older people's perspectives. Our stratified analysis based on the different types of physical activity showed some subthemes such as dependence on professional instruction, pain or discomfort, affordability, strength, balance and flexibility, and self-confidence to be more relevant to those engaging in structured exercise programmes. Other specific subthemes identified in this review such as environmental barriers and maintaining habits seem to be more important in the context of other types of physical activity. These more specific findings can be applied to different physical activity contexts, with important implications for public health.
Our review has some limitations. Most included studies were conducted in developed countries. Therefore, people from developing countries may be under-represented. However, no apparent variation among themes was observed across different countries. Another limitation of this review is the risk of different use of exercise and physical activity terms among participants and authors. This may limit the validity of the stratified analysis based on different types of physical activity.
Research on understanding physical activity behaviour is essential for the development and improvement of public health interventions.32 The lack of conclusive evidence on determinants of physical activity among the ageing population is alarming and needs to be addressed.20 Our view is that the themes identified in this systematic review reflect the needs and preferences of older people and, therefore, should guide the choice of correlates and determinants of physical activity engagement in future studies. Our findings suggest that strategies to enhance physical activity among older people must aim to improve environmental and financial access to physical activity programmes as well as to raise awareness of the health benefits and minimise the perceived risks of physical activity. Moreover, these outcomes should also inform healthcare policy and practice, so that older people's perspectives remain central to future discussions regarding the design of effective health services.
What are the new findings?
Thematic synthesis of multiple qualitative studies offers a range of perspectives across different contexts, provides more complete knowledge than that derived from single studies and can inform practice and policy.
Many older people still believe that physical activity is unnecessary, risky or even potentially harmful; others recognise the benefits to improve physical and mental well-being, but report a range of barriers to physical activity participation.
Strategies to promote and sustain an active lifestyle among older people should include improvement of environmental and financial access to physical activity opportunities as well as to raise awareness of the health benefits and minimise the perceived risks of physical activity.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
Contributors MRF, AT, KH, CS, MLF and PHF were involved in the design of the review. MRF, AT, KH, CS and MLF developed the search strategy. MRF and RZP performed the study selection. MRF and RZP extracted data from included studies. MRF, AT, KH, CS, MLF and RZP were involved in data analysis. All authors were involved in the interpretation and discussion of results. All authors contributed to the writing and review of the various drafts of the report.
Funding MRF is supported by CAPES Foundation, Ministry of Education of Brazil. CS is supported by a research fellowship funded by the Australian National Health and Medical Research Council (NHMRC).
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.