Article Text

Abstract
The sport medicine clinician is faced with return-to-play (RTP) decisions for every patient who wants to return to activity. The complex interaction of factors related to history, physical examination, testing, activity and baseline characteristics can make RTP decision-making challenging. Further, when reasoning is not explicit, unnecessary conflict can arise among clinicians themselves, or among clinicians and patients. This conflict can have negative health consequences for the patient. In 2010, a transparent framework for RTP decisions was proposed. However, some have identified limitations to the framework and found difficulties in its implementation. This paper presents a revised framework that addresses the limitations, and provides concrete examples of how to apply it in simple and complex cases.
- Method
- Review
- Sports & exercise medicine
Statistics from Altmetric.com
Almost all patients in the office or on the field ask their clinician when they can return to play (RTP). These decisions are based on a large number of factors including the history of the injury, physical examination, type of injury, rehabilitation, type of activity, psychological state, competitive level and ability to protect the injury. In addition, the athlete may receive conflicting opinions from other clinicians, family, friends, coaches and agents. Such conflicts can lead to (1) miscommunication, (2) loss of trust, (3) potential litigation, (4) declines in sport participation rates as some individuals never ‘get back in the game’ due to fear of reinjury (despite acceptable levels of risk) and (5) even more serious medical complications as some athletes return to activity while still at unacceptable levels of risk for subsequent sport-related injury.1–4
One important factor that may minimise the development of such conflict is to have a formal structure or process that makes the RTP decision reasoning more transparent. This would be expected regardless of who has the decision-making authority (eg, clinician, athlete, shared decision-making). In 2010, we adapted a decision theoretic model for RTP decision-making5 (figure 1) that separates the decision-making process into three steps. The first two steps, Medical Factors and Sport Risk Modifiers, assess risk, and the third step evaluates the effect of Decision Modifiers. The model evolved out of a literature review, discussions among three experienced sport medicine physicians, a student and staff, and feedback from colleagues. Later research showed that it is consistent with clinicians’ beliefs independent of country of practice or clinician specialty,6 and serves as a framework to help organise complex information.

The three-step return-to-play (RTP) framework (reproduced from5) is illustrated. This framework groups factors responsible for RTP according to the sociological source of the information (medical culture, sport culture, personal decision modifiers). The first two steps assess risk, and the decision to RTP is based on the interaction of this risk with other factors that affect the patients’ overall well-being (decision modifiers) (see text for details). MSK, musculoskeletal.
In presenting the framework at three different conferences to several hundred participants, questions arose concerning how particular factors fit or do not fit within the model. For example, the factor ‘ability to protect’ is included in step 2, although it is clearly not a medical factor or a decision modifier and is not directly related to sport. Other challenges expressed include the framework's ability to account for very serious conditions such as concussion, or when there are simultaneous risks (eg, short-term risk of reinjury, long-term risk of osteoarthritis). The reason for these difficulties may simply lie in the fact that the original framework was rooted in sociological terms (medical factors, sport risk modifiers and decision modifiers), whereas the decision theoretic framework is really about assessing and intervening on biological causal risks. Categorising biological and physiological causes into sociological constructs may lead to significant challenges and confusion. Therefore, the objectives of this article are (1) to propose a modified framework (Strategic Assessment of Risk and Risk Tolerance: StARRT) where factors affecting risk are grouped according to causal biological constructs, (2) to explain why the previously named ‘decision modifiers’ are better referred to as Risk Tolerance modifiers and (3) to provide examples on how the framework can be applied in practice.
The StARRT framework
At its foundation, the StARRT framework (figure 2) simply considers that the basis of RTP decisions is a risk assessment of the outcome. This risk is then compared with one's risk tolerance. If the risk assessment is greater than the risk tolerance, the decision should not be to allow RTP (more precisely, not allow RTP that generates the level of risk assessed in the first step). In a biological framework, an injury (or osteoarthritis or death) occurs when the stress applied to the tissue exceeds the stress the tissue can absorb. The stress applied to tissue is mostly determined by activity, and is generally analogous to the sport risk modifiers in our previous framework.5 The stress the tissue can absorb is mostly related to tissue health, and is generally analogous to medical factors. Finally, risk tolerance is generally analogous to the decision modifiers. The next sections expand on these principles and show how the new terminology provides a more consistent framework. Throughout, the examples of categories listed in figure 2 are just guides to help structure the thought process, and the focus should be on the underlying concepts.

The Strategic Assessment of Risk and Risk Tolerance (StARRT) framework for return-to-play (RTP) decisions. This framework illustrates that patients should be allowed to RTP when the risk assessment (steps 1 and 2) is below the acceptable risk tolerance threshold (step 3), and not allowed to RTP if the risk assessment is above the risk tolerance threshold. The StARRT framework groups factors according to their causal relationships with the two components of risk assessment (Tissue Health, stresses applied to tissue) and risk tolerance, as opposed to the three-step framework that groups factors according to the sociological source of the information. In some cases, apparently a single factor can have more than one causal connection and would be repeated. For example, play-offs will increase the competitive level of play and therefore increase Tissue Stresses and increase risk. However, it is also expected to affect a patient's desire to compete (ie, mood, risk of depression) and could affect financial benefit as well. These causal effects would lead to increased risk tolerance. In this framework, each outcome is evaluated for RTP, and the overall decision is based on the most restricted activity across all outcomes (see text and table 1 for details). MSK, musculoskeletal.
Step 1: Tissue Health (Medical Factors)
The first step in figure 1 is to assess the stress the tissue can absorb before becoming damaged. This is a function of the health of the tissue. For the same level of activity, the risk of reinjury increases with increasing damage to the tissue. The assessment of tissue damage is generally evaluated through the presence of symptoms and signs such as pain or swelling, or diagnostic tests.
In the original framework,5 the ‘potential seriousness’ of the injury was included in step 1 because it represents a sociological construct related to medical factors. However, steps 1 and 2 of the original framework are only supposed to assess risk. We might assess the risk of all reinjuries, or only severe reinjuries, or only death. In other words, the potential seriousness is really about which outcome we are most interested in, and not about assessing the risk of any particular outcome. In a subsequent section, we will discuss how the StARRT framework should be applied when more than one risk is of interest.
Step 2: Tissue Stresses (Sport Risk Modifiers)
If an unhealthy tissue is exposed to only minimal stress, it continues to heal. If the stress exceeds the capacity of the tissue, an injury or reinjury will occur. Therefore, the second step of the framework is to assess the stress that will be applied to the tissue. Tissue stress is directly related to the planned activity (cognitive stress in concussion is activity), and is therefore considered activity related. This is in contrast to step 1 that evaluates Tissue Health, which exists in a particular state at a particular time.
There are many different ways to categorise activity. Using the ‘FITT’ training principle, activity can be categorised (or modified) according to frequency (eg, 3 days/week), intensity (eg, running fast or climbing hills), timing (eg, 20 min/session) and type. Within the biological framework, it is best to think of ‘type’ in relation to the biological stresses that increase with the specific activity and might cause injury, rather than in general terms such as running or swimming. For example, the biomechanics of freestyle swimming is very different from that of breaststroke (analogous to different positions in other sports). A swimmer with pes anserine tendinopathy might not be able to RTP for breaststroke but might be able to RTP for freestyle.
In our original framework, the ‘ability to protect’ mentioned above was included as a Sport Modifier (step 2) even though it was not directly sport related. In the modified framework, the ability to protect an injury clearly decreases the stress applied to the tissue and is part of step 2.
The original framework placed functional tests that measure functional capacity in step 1. However, the postinjury decrease in endurance and strength, and range of motion of tissues that have not been injured are clearly not related to the health status of the damaged tissue we are trying to evaluate, nor are they related to sport. Within the biological causal framework of StARRT, decreased endurance means an increase in fatigue, which means an increase in stress transmitted to other structures.7 ,8 Similarly, decreased proprioception will increase the stresses that occur across many structures. Other examples include inflexible hamstrings increasing stress on the low back, and scapular dyskinesis increasing the stress on the rotator cuff. Finally, to be internally consistent, two factors along the same causal pathway should be grouped in the same category. Since an ankle brace (protective equipment, original framework step 2) is effective because it limits deficiencies in proprioception (improves results on functional tests, original framework step 1), the two should be in the same category.
Psychological readiness (original framework step 1) is similar to measures of functional capacity. Our original framework implied that anxiety or fear could change the way an athlete participates. This is just another way of saying that it could change the ‘position played’ or competitive level of the athlete, and therefore should be included in step 2.
It is important to stress that the sociological framework is useful in that it categorises factors according to who provides or obtains the information (step 1: clinicians; step 2: those knowledgeable about the sport). However, the stated goal at the end of step 2 is to obtain a risk assessment, which is a causal construct. Grouping factors according to sociological constructs creates unnecessary difficulty when trying to estimate each causal component of steps 1 and 2. The advantage of the StARRT framework is that the factors are more appropriately grouped according to how they inform risk assessment. It is also internally consistent in that factors along the same causal path are grouped together.
Step 3: Risk tolerance modifiers (Decision Modifiers)
Step 3 is designed to explicitly state the clinician's threshold for an acceptable risk (risk tolerance), and what factors affect this value. In this regard, risk of reinjury represents one of several outcomes that affect the overall health or well-being of the athlete.9 How do we define well-being or health? Should this be restricted to pathology of the muscle, tendon or bone (as for reinjury)? Should we also consider mental health or socioeconomic health? Although risk tolerance is subjective and personal, individual risk tolerances are nonetheless shaped by the values of the society that the person lives in.
One can think of the baseline risk tolerance (or general risk tolerance) as the risk tolerance that exists when each factor is set at some arbitrary but constant value for each individual. A factor is included as a risk tolerance modifier if there is any context where changing the factor would change one's threshold of an acceptable risk. For example, we might consider a 10% increased risk of reinjury (compared with the uninjured knee) as acceptable. Now consider an athlete with a knee injury, where the risk of reinjury in competition increases to 15%. If we believe that removing the athlete from the Olympics carries a risk of depression (mental health), we might decide that our risk tolerance for a second knee injury is 20% instead of the original 10%, and allow the athlete to compete. However, if the athlete is a 14-year-old male playing high school basketball, there may be less risk of depression and the clinician's risk tolerance might not change. The competitive level is considered a factor in the framework because there is a context in which it changes the risk tolerance, even though there are other contexts where the factor would not affect risk tolerance.
In summary, an RTP decision (no matter who is responsible for the decision) will be considered appropriate by society when it is based on an accurate risk assessment, and on a risk tolerance that is both related to the patient's well-being and is consistent with societal values.
Applying the framework
The objective of the StARRT framework is to arrive at a decision based on whether the risk assessment exceeds one's risk tolerance. In presenting the framework at conferences, some clinicians had difficulty applying it in a clinical context because one is almost always evaluating risk for multiple outcomes. Below, we begin with a simple example and later illustrate how to incorporate increased complexity. Most important, RTP in clinical practice may refer to ‘full return without restrictions’, ‘partial return’, ‘allowed to practice’ and so forth. The StARRT framework can be applied to any decision-making process and will work equally well with any definition of RTP because these definitions are simply defining the level of stress that is expected in step 2. Further, it is a process that can be followed by any decision-maker, whether this is a clinician, an athlete, a judge or a shared decision-making process.
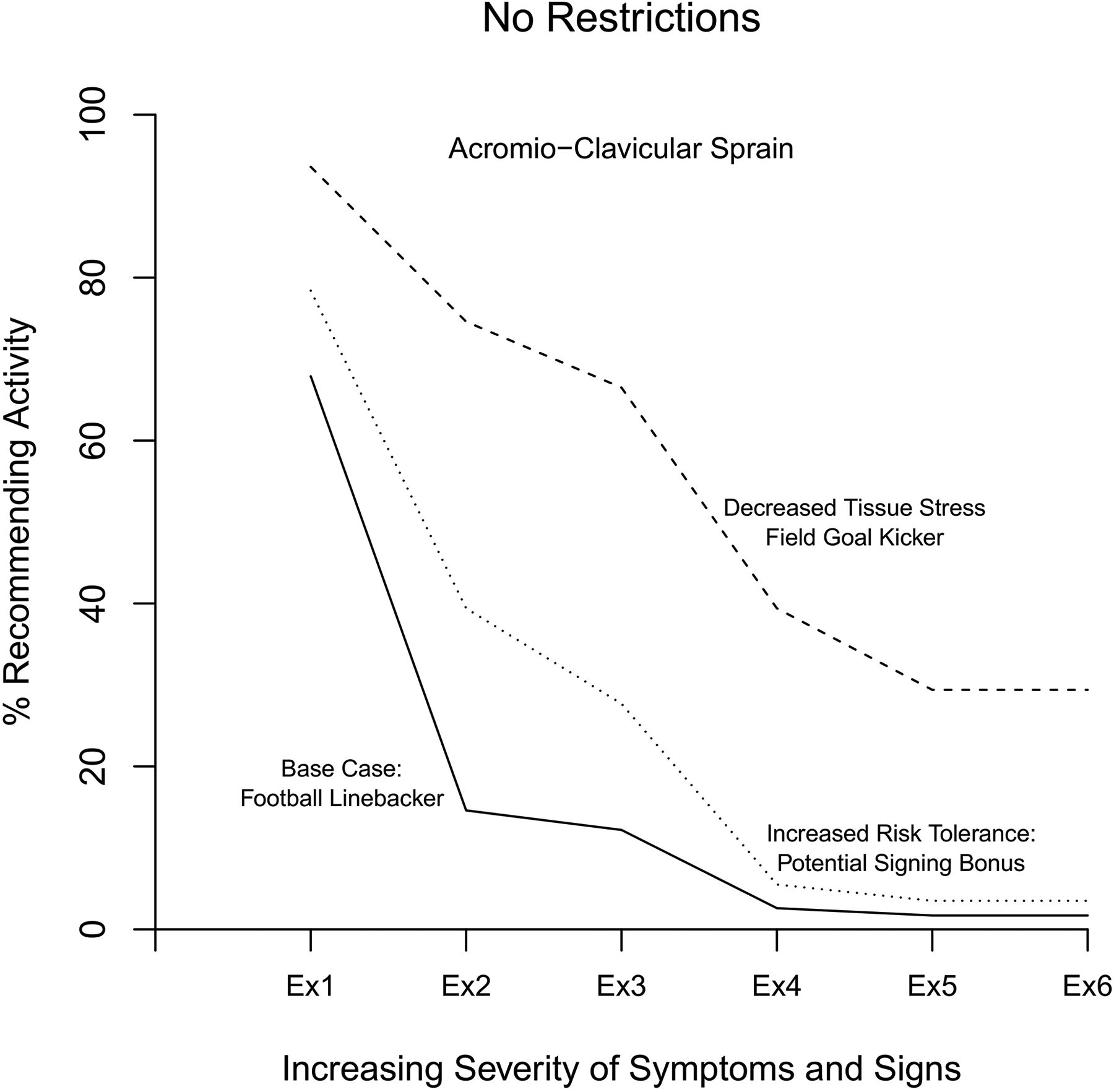
Consider a case described in one of our validation studies where a collegiate American football linebacker (many contacts and collisions at high speed) injured his acromioclavicular joint10 (figure 3, top). As the severity of signs and symptoms increases (from examples 1 to 6 in figure 3), most would agree that the stress the tissue could absorb prior to reinjury would decrease. In our study, as the health of the tissue decreased in the vignettes, clinicians became less likely to allow the athlete full RTP. We then changed the scenario so that the athlete was a field goal kicker (very low risk of contact) instead of a linebacker. By decreasing the risk of applying excessive stress to the tissue (ie, contact), the risk of reinjury decreases, and this explains why more clinicians allowed full RTP than when the athlete was a linebacker. Finally, returning to the context of a linebacker, we changed the vignette to say that the athlete was being evaluated for a million dollar signing bonus. Given the potential benefit to his economic condition and overall well-being, the risk tolerance of many clinicians changed, and these clinicians now allowed the athlete to RTP even though the risk of reinjury remained unchanged.
{kind=link}
{kind=link}
{kind=link}
The proportion of respondents who would allow activity without restriction is plotted for the different acromioclavicular injury severity levels described in the clinical vignettes described in ref. 10. The solid line presents the results for the base case when the athlete is an American football linebacker. The dashed line presents the results when we decreased the likelihood of excessive stress by considering the player to be a field goal kicker instead of a linebacker (Tissue Stresses). The dotted line presents the results when the linebacker (base case) was being evaluated for a multimillion dollar bonus (risk tolerance modifiers). This figure is adapted from survey results in,10 with the steps indicated according to the StARRT framework.
In figure 3, changing the activity affected the decision of many clinicians at every level of injury severity. However, in a separate example from the same study, providing a brace to a hockey player with a severe knee injury (ie, decrease in tissue stress) had little effect even though it had a large effect when the injury was moderate. The explanation is simple; the decreased stress with the brace may have reduced the risk, but the actual value of the risk assessment still exceeded the clinician's risk tolerance.
Assessing across outcomes and probabilities
In our original framework, we included ‘Potential Seriousness’ of the condition in step 1. This was in response to scepticism that the model was not applicable to conditions that had potentially severe consequences (risk of death with RTP in concussion). In these cases, some argued that the clinician should simply stop at step 1, and never consider the level of activity or conduct a formal risk assessment.
The StARRT framework can be used to transparently explain why these objections do not apply. First, there is a risk of death in every sport or activity. Therefore, clinicians not explicitly using the StARRT framework are still subconsciously comparing the risk of death, given the health status of the athlete, with the risk of death among the usual player (or the same player before the injury), to determine if the increased risk is acceptable (below their risk tolerance) or unacceptable (exceeds their risk tolerance). A basketball player who continues to have headaches with reading 5 min on day 5 postconcussion might not be allowed to RTP according to most guidelines because we are worried about death or long-term cognitive impairment. However, a table tennis player might experience an increase in symptoms and potentially prolong the recovery, but there is no increased risk of death while playing. In effect, the activity is always being evaluated but its evaluation is often hidden behind the complex nature of the interacting factors. One of the benefits of the StARRT framework is that it helps make these formerly hidden assumptions more transparent for the clinician and athlete.
The concussion example also highlights that steps 1 and 2 of the StARRT framework assess only one of many risks (2nd concussion, prolonged symptoms, death) at a time. However, the decision to RTP must usually account for many short-term and long-term outcomes simultaneously. For example, important short-term outcomes for most elite athletes with most injuries would include risk of reinjury and risk of decreased performance (leading to decreased competitive standing). Long-term outcomes of interest might include osteoarthritis, disability and quality of life in later years. Each of these represents a different outcome that would be assessed through the framework. The process for combining all of these is the same as when an athlete has more than one injury (eg, assessing overall restrictions for an athlete with a knee injury and an ankle injury). For example, an athlete might be able to play in a restricted role if they only had their ankle injury, but unable to play because the knee injury prevents any level of competition. In other words, the most severe restriction becomes the overall restriction for activity.
Similarly, table 1 shows hypothetical results for Clinician A evaluating RTP for an athlete with a knee injury. For simplicity, table 1 shows the overall risk tolerance for each outcome and omits the factors affecting risk tolerance. This is because to be meaningful, one would have to specify the risk tolerance with and without each potential risk tolerance-modifying factor (which is not currently in table 1). In table 1, Clinician A considered the risks acceptable and allowed RTP for 6/7 outcomes, but unacceptable for short-term disability. In this case, the overall RTP decision remains no RTP because the risk exceeded the risk tolerance for one outcome. Normally, explicitly completing such a table is not required because the risk assessments are far below the risk tolerances. However, completing the table may help make the decision-making process more transparent in more complicated cases.
A hypothetical example of applying the Strategic Assessment of Risk and Risk Tolerance (StARRT) framework for return-to-play (RTP) decision-making across different short-term and long-term outcomes
Risk tolerance modifiers versus multiple outcomes
Risk tolerance modifiers themselves have particular values (eg, Yes/No, or a numerical value if a continuous scale) but are not strictly risks. For example, timing of the season is preseason, regular season, playoffs, off-season. In the play-offs, the increased risk with increased style of play is captured in step 2 under ‘competitive level’. However, the threshold at which we consider any particular risk as acceptable also changes because the play-offs also change the financial compensation and other factors. Therefore, the timing of the season may sometimes have minimal effect on risk assessment (table 1, column 2), but may still have large effects on risk tolerance (table 1, column 3).
In an earlier section, we noted that baseline risk tolerance is just the tolerance under an arbitrary set of values for the risk tolerance-modifying factors. Risk tolerance modifiers are defined by the fact that they change our risk tolerance under some specific context, whereas multiple outcomes by themselves do not. For example, consider the high school athlete with a knee injury. The risk of osteoarthritis does not change the risk of a second knee sprain, nor does it change our risk tolerance for a second knee sprain. If we do not allow RTP, this is because we are concerned with the risk of osteoarthritis. Contrast this with the risk tolerance modifier ‘competitive level’ that we mentioned previously. As the competitive level changes, the potential benefits to the athlete and their well-being change. Therefore, for the same risk assessment on the same injury, our risk tolerance threshold may shift to make RTP acceptable (or non-acceptable). Therefore, risk tolerance modifiers are defined by this interaction, whereas additional outcomes that are non-risk tolerance modifiers are not.
Summary
In summary, the StARRT framework for RTP decision-making organises the available information into factors that determine risk of participation and risk tolerance. Risk of participation is dependent on the interaction between Tissue Health (step 1, stress the tissue can absorb) and Tissue Stresses (step 2, stress applied to the tissue). This risk is then compared with the clinician's and/or athlete's risk tolerance, which is a function of many factors that are (and should be) generally related to a broader concept of athlete well-being. If the risk assessment is less than the risk tolerance after all factors are considered, the decision should be to RTP. Otherwise, the decision should not be to RTP. RTP decisions are considered inappropriate when the risk assessment is poor (research into predictive algorithms might be beneficial), or when: (1) risk tolerance is dependent on factors unrelated to the patient's well-being or (2) personal values conflict with societal values.
What are the new findings?
The Strategic Assessment of Risk and Risk Tolerance (StARRT) framework for return-to-play (RTP) decisions addresses the limitations of the original three-step framework for RTP decision-making.
The StARRT framework can be applied across any injury or definition of RTP.
The paper explains how to apply the framework using concrete examples.
Acknowledgments
The author would like to thank Lyn Charland for her helpful comments on early versions of the manuscript, and for her help in developing the acronym StARRT.
Footnotes
Funding IS is funded by the Lady Davis Institute for Medical Research, Jewish General Hospital, McGill University.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.