Article Text

Abstract
Background Data regarding direct athletic muscle injuries (caused by a direct blunt or sharp external force) compared to indirect ones (without the influence of a direct external trauma) are missing in the current literature—this distinction has clinical implications.
Aim To compare incidence, duration of absence and characteristics of indirect and direct anterior (quadriceps) and posterior thigh (hamstring) muscle injuries.
Methods 30 football teams and 1981 players were followed prospectively from 2001 until 2013. The team medical staff recorded individual player exposure and time-loss injuries. Muscle injuries were defined as indirect or direct according to their injury mechanism.
Results In total, 2287 thigh muscle injuries were found, representing 25% of all injuries. Two thousand and three were valid for further analysis, of which 88% were indirect and 12% direct. The incidence was eight times higher for indirect injuries (1.48/1000 h) compared to direct muscle injuries (0.19/1000 h) (p<0.01). Indirect muscle injuries caused 19% of total absence, and direct injuries 1%. The mean lay-off time for indirect injuries amounted to 18.5 days and differed significantly from direct injuries which accounted for 7 days (p<0.001). 60% of indirect injuries and 76% of direct injuries occurred in match situations. Foul play was involved in 7% of all thigh muscle injuries, as well as in 2% of indirect injuries and 42% of direct injuries.
Summary Muscle anterior and posterior thigh injuries in elite football are more frequent than have been previously described. Direct injuries causing time loss are less frequent than indirect ones, and players can usually return to full activity in under half the average time for an indirect injury. Foul play is involved in 7.5% of all thigh muscle injuries.
- Athlete
- Football
- Thigh
- Muscle
- Soccer
Statistics from Altmetric.com
Introduction
If one considers an injury mechanism, muscle injuries can be differentiated into indirect and direct types.1 ,2 Indirect muscle injuries are caused without the influence of a direct external trauma. They are either functional (non-structural) disorders without evidence of a tear, or structural injuries caused by a longitudinal distraction that tears the muscle tissue.1 Direct muscle injuries are caused by a direct blunt (contusion) or sharp (laceration) external force. In most of the direct cases, the injury mechanism is a compressive force to the thigh (such as a direct blow from an opponent's knee) that usually compresses the muscle tissue. In contrast to indirect injuries, muscle fibres are not torn by longitudinal distraction.
While indirect muscle injuries are well described,3–7 information regarding direct muscle injuries is very limited. There is no study in the literature so far that compares indirect and direct muscle injuries.
Ekstrand et al5 reported that indirect injuries constitute 31% of all soccer injuries, causing 27% of the total injury absence. A men's elite level team can expect 15 muscle injuries each season, and the most common single injury type is a hamstring injury.5 Ninety-six per cent of muscle injuries occur in non-contact situations, and only 2% are due to foul play.5 Direct muscle injuries were monitored in that particular study as contusions in general without specific analysis regarding location, epidemiology and nature. Thus, valid epidemiological data for elite football players are missing. However, if we look at the total muscle injury group, direct injuries such as contusions affecting muscles should also be included in the analysis and be compared with indirect injuries.
Direct injuries, especially contusions, are common in sports, especially in team sports with contact situations like football, basketball, American football, rugby and others.8 ,9 These injuries are usually painful and may cause considerable functional disability in the affected area. However, athletes, even those with more severe contusions, can often continue playing for some time. In many cases, players become fully aware of the injury only after leaving the field or later, when the bleeding and swelling has reached a certain level.9 In contrast, a small indirect structural injury, such as a partial tear of the muscle tissue, usually forces the player to stop at once. It has been stated that early return to full function and rehabilitative therapy after direct injuries can usually be more aggressive to the limit of pain tolerance,10 which is not the case in indirect muscle injuries. Even though these observations have great practical consequences for the medical teams, this issue has been little researched.
We aimed to investigate the incidence and characteristics of direct injuries and compare them with indirect muscle injuries in a homogeneous group of male elite football players. Our hypothesis was that time-loss direct muscle injuries would be less frequent and lead to a shorter absence compared to indirect injuries.
Materials and methods
Study population
This study is a substudy of the general prospective injury surveillance of male elite football that started in 2001, the UEFA Champions League (UCL) Injury study (now known as the UEFA Elite Club Injury Study) which is well described in the literature.2 ,5
In total, 1981 players from 30 European elite teams and 10 different countries were followed from July 2001 until May 2013. All contracted players in the first team were invited to participate in the study.
Study design and definitions
The full methodology and the validation of the UCL injury study design are reported elsewhere.11 The study design followed the consensus on definitions and data collection procedures in studies of football injuries.5 ,11 ,12 A recordable injury was defined as “any physical complaint resulting from football activity and leading to a player being unable to fully participate in future training or matches (ie, time loss injury).”
According to the recently described Munich muscle injury classification system, muscle injuries were categorised into indirect and direct types.1 A direct muscle injury was defined as “a traumatic injury caused by a direct external trauma,” an indirect injury as “a muscle injury caused without the influence of a direct external trauma.”1 An overview of further definitions used in this study is demonstrated in table 1.
Operational definitions
Data collection
Player baseline data were collected at the start of the season. Individual player exposure in training and matches was registered by the clubs on a standard exposure form and sent to the study group on a monthly basis. Team medical staff recorded thigh muscle injuries on a standard injury form that was sent to the study group each month. The thigh injury form is an A4 page consisting of ticking boxes for type, location and mechanism of injury as well as diagnostic procedures and treatments. The player was considered injured until the team medical staff allowed full participation in training and availability for match selection. All injuries were followed until the final day of rehabilitation. All reports were checked each month by the study group and feedback was sent to the teams in order to correct any missing or unclear data.
Statistical analyses
Pearson's χ2 test was used to analyse the association between type of thigh muscle injury (direct and indirect) and various categorical variables. Absence days are presented with mean±SD and corresponding median (Md) and IQR. Owing to the skewed distribution in absence days, group differences were analysed using the Mann-Whitney U test. Injury rates (IRs) are reported as the number of injuries per 1000 player-hours and injury burden was calculated as the number of absence days per 1000 player-hours. Rate ratio (RR) with 95% CI was used for group comparisons of injury rates and injury burden, and significance tested using z-statistics. All tests were two sided and the significance level was set at p<0.05. Analyses were completed using IBM SPSS Statistics V.21.0 (IBM Corp, Armonk, New York, USA).
Results
Basic data, exposure, injury types and incidence
There were, on average, 28±5 players included per team. In total, 2287 thigh muscle injuries were recorded during 5013 player seasons. Overall, 1 194 510 h of exposure (1 003 270 of training and 191 240 of match play) were registered.
The 2287 thigh muscle injuries amounted to 25% of all 8993 injuries. Two hundred and eighty-four (12%) of all muscle injuries were not definable as direct or indirect ones, since data from club medical teams were missing or unclear.
The 2003 thigh muscle injuries which could be clearly categorised as indirect or direct mechanism are included in the following results: 1772 (88%) were indirect injuries and 231 (12%) were direct, all of them contusion injuries. Indirect muscle injuries represented 20% and direct ones 3% of all injuries.
The incidence of indirect injuries was eight times higher compared to direct injuries (1.48/1000 vs 0.19/1000 h, p<0.001). An overview of basic data, incidence, absence and the associated injury burden of indirect versus direct thigh muscle injuries is seen in table 2.
Basic data, incidence, absence and injury burden of indirect versus direct thigh muscle injuries
Circumstances of injury
Sixty per cent of indirect injuries and 76% of direct injuries occurred during matches, whereas 40% and 24%, respectively, were recorded during training. Direct injuries tended to occur more frequently during the second half of matches (57% vs 43% in the first half) compared to a more balanced distribution across the full course of the match for indirect injuries (49% in the second half vs 51% in the first half) (in both injury types without significant association, p=0.137). In both groups, there was a tendency for more injuries to occur towards the end of the two halves. The distribution of both injury groups by match period of 15 min is shown in figure 1.
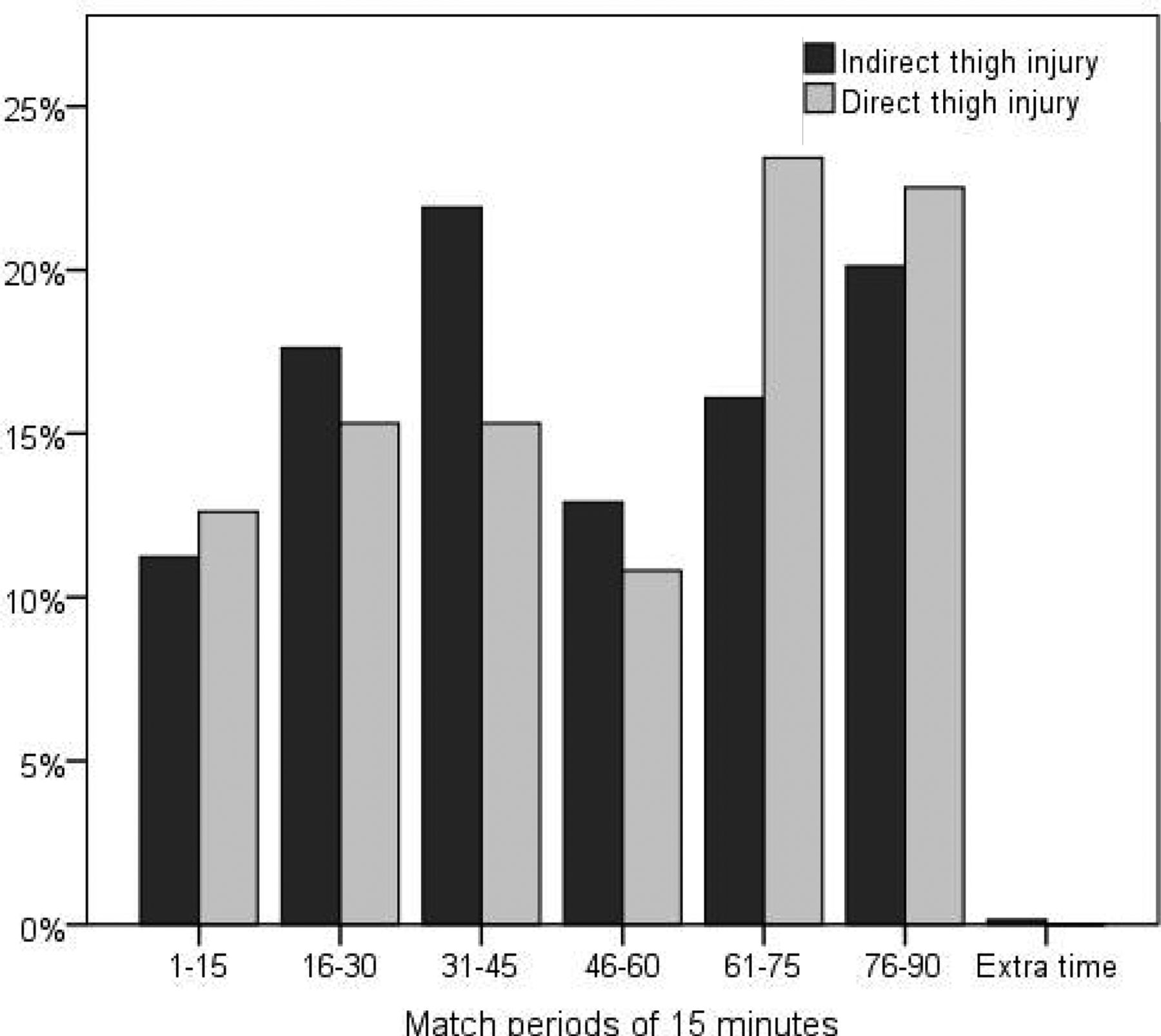
Distribution of indirect and direct thigh muscle injuries by match period of 15 min.
Naturally, and as defined, all direct injuries occurred in contact situations, the vast majority involving other players; in one case, a direct injury was sustained after contact with an object. In contrast, 96% of the indirect injuries occurred in non-contact situations. The majority, that is, 60% of all indirect injuries, occurred during sprinting or high-speed running, 14% resulted from shooting and 3% in stretching situations.
{kind=link}
{kind=link}
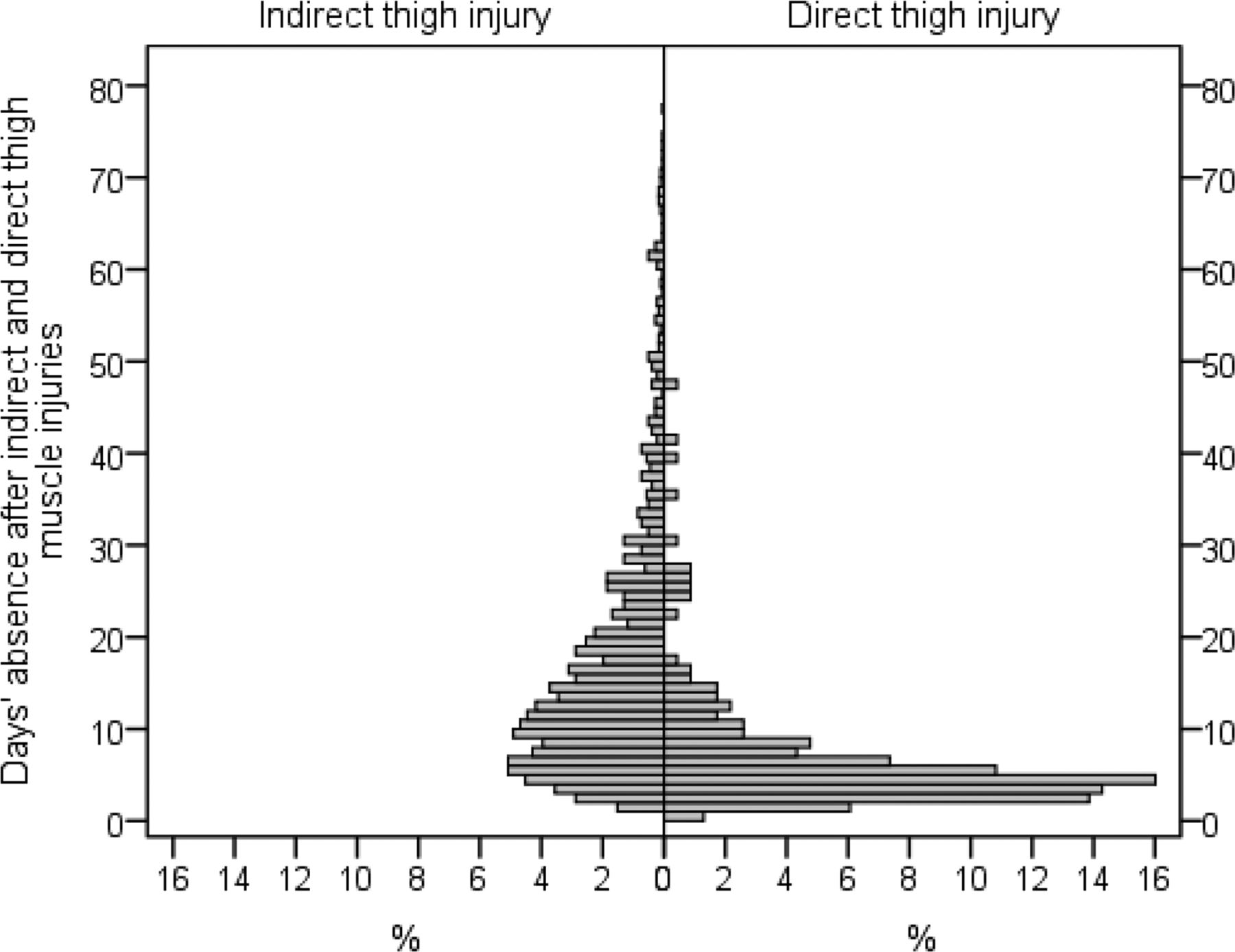
Days of absence after indirect and direct thigh muscle injuries.
Foul play was involved in a total of 7% of all muscle injuries. A distinct difference was observed between the two injury groups: 2% of indirect injuries compared to 42% (56% collision, 23% kicked, 10% tackled) of direct injuries resulted from fouls.
Absence after indirect and direct muscle injury and re-injuries
As seen in table 2, the mean absence of all thigh muscle injuries was 17.2±18.9 (median 12) days. Mean absence after indirect injury amounted to 18.5±19.5 (median 13) days compared to 7.0±9.1 (median 4) days for direct injuries (p<0.001) (figure 2).
The absence in relation to all injuries (total injury absence) was 19.6% for all injuries, 18.7% for indirect injuries and 0.9% for direct muscle injuries, that is, 20.2 times higher for indirect injuries compared to direct injuries.
The injury burden, expressed as the number of days absence/1000 h of total exposure (incidence × mean absence), accounted for 27.5 of indirect injuries and 1.4 of direct muscle injuries (p<0.001).
The re-injury rate for all injuries in the study was 11%. The recurrence rate of indirect muscle injuries was 13% compared to only 0.4% for direct muscle injuries.
Discussion
Muscle injuries of the thigh are even more frequent in elite football than were previously considered and published. In previous studies, these injuries accounted for 17% of all injuries.5 However, this number only represented injuries that had been indirect. Contusions and other direct muscle injuries were not monitored as muscle injuries.5
Direct injuries account for 12% of time-loss thigh muscle injuries
Direct injuries represent almost 3% of all muscle injuries and 12% of time-loss thigh muscle injuries in elite football causing approximately 1% of total injury absence. In contrast, indirect thigh muscle injuries represent almost 20% of all injuries, whereas 88% of time-loss thigh injuries cause almost 19% of the total injury absence.
Shorter absence after muscle contusion compared to indirect muscle injury
Jackson and Feagin13 reported that the average return to sport without proper treatment of thigh contusion was 45 days. On the basis of the present study, the mean absence after direct muscle injuries was 7 days with a median (which is probably the more useful value regarding expected absence) of 4 days. Mean absence after indirect injury was significantly longer and 18.5 days. Total absence for all muscle injuries amounted to 16.2 days, which is comparable to previous studies.5 Compared to the data of Jackson and Feagin, our study possibly indicates that top-level clubs in Europe have effective medical support, providing individualised rehabilitation for players after muscle contusion. However, the high SD as well as the high range shows that there are a range of muscle injury grades within both groups. These injuries could not be further subdifferentiated in our study since a more detailed classification system, the Munich consensus classification, was not implemented in the UCL study until 2013.1 ,2
Total injury absence was 20.2 times higher and injury burden 19.6 times higher for indirect injuries compared to direct. As mentioned earlier, contusion injuries cause pain and loss of motion. However, muscle fibres are usually compressed, but not torn by longitudinal distraction.1 Thus, rehabilitative therapy can usually be more aggressive, up to the limit of pain tolerance. Function is progressively increased as motion and strength return.10 One might speculate that this explains the shorter absence and lower injury burden of direct injuries.
Healing of muscle tears is a gradual process, and time is needed to restore the strength of the muscle to the pre-injury level.15 Thus, returning to full activity without a total healing of the muscle tissue and without a total recovery of tensile strength is likely to lead to a more severe re-injury.1 ,14 The greatest risk is during the initial 2 weeks following return to sport.15
In this study, the recurrence rate of indirect thigh muscle injuries was 13%, confirming previous studies.5 ,6 The re-injury rate of direct injuries amounted to only 0.4%. However, varying degrees of direct muscle injury can occur—some direct injuries in this study caused long absences (see table 2). Another reason for the low re-injury rate might be that team physicians probably report a problem after muscle contusion as a different diagnosis and not as a re-injury.
Many direct injuries during matches
It is well known that muscle injuries occur more frequently during matches than during training.5 However, data were so far only available for indirect injuries. In our study, we found that direct injuries occur even more frequently during matches: 76% of direct injuries compared to 60% of indirect injuries. Direct injuries tended to occur more frequently during the second half of matches and there was a tendency for more injuries to occur towards the end of each half. Our findings suggest that teams play more aggressively during matches compared to training as well as towards the end of matches. This extends previous findings that 90% of footballers are ready to commit an intentional foul if required, depending on the score and importance of the match.16
More than 40% of thigh muscle contusions due to foul play
Around 20% of match injuries are due to fouls.17 Thus, foul play is one of the most important known extrinsic risk factors for injuries in football.18 It is well documented that injuries caused by foul play are mostly sprains or contusions affecting the lower extremity.17–20
Our data indicate that 7.5% of all thigh muscle injuries were related to foul play. A distinct difference was observed between the two injury groups: 1.7% of indirect injuries compared to 42% of direct injuries resulted from fouls. This suggests that stricter refereeing could reduce the risk of direct injuries.
Medical history is the key to differentiate direct injuries from indirect injuries
Diagnosis of muscle injuries can be complex. It should be based primarily on clinical findings, with imaging providing additional information to confirm the diagnosis.4 ,6 ,7 ,21 Medical history is crucial, and the simple question ‘was there a kick or collision’ to the player has a direct practical relevance. It has been described that rehabilitation can be more aggressive to the limit of pain tolerance after muscle contusion,10 which is not the case for indirect muscle injuries.1
MRI has been the preferred imaging for muscle injuries in recent years.22–25 However, when it is used in isolation, it can lead to misinterpretation since there are no specific pathological changes separating direct from indirect injuries.26 Moreover, the resolution of the injury as detected by MRI can lag behind functional recovery, in indirect injuries,27 ,28 as well as in direct injuries.10 A haematoma or oedema can still be apparent on MRI taken weeks and even months after return to play.10 ,27 ,28 Diaz et al10 showed that, despite markedly abnormal imaging studies, athletes were able to compete at the highest professional level without functional loss after a muscle contusion.
Methodological considerations
An obvious strength of this study is its design, with a homogeneous group of male elite footballers followed prospectively with a standardised methodology.11 ,12 Another strength is the number of players included; for the first time, all thigh muscle injuries (ie, hamstring and quadriceps) were analysed, which makes the numbers substantially larger than in previous studies.
A limitation of the study is the absence of subdifferentiation of muscle injuries. Thus, the material includes muscle injuries of different severities and of different sizes. A more detailed classification, for example the Munich consensus classification system, would have been useful. Unfortunately, 12% of all muscle injuries were not definable as direct or indirect ones, since data from club medical teams were missing or unclear. Furthermore, our study population was limited to male elite football players and might therefore not necessarily reflect the injury characteristics of a more general population or other levels of play. Regarding data collection, potential limitations included the risk for observer bias from the lack of an independent injury classification and evaluation for return to play performed by the same team medical staff.
Although our data and considerations represent a high number of muscle injuries, as well as a long clinical experience, more specific data would be useful in order to develop an algorithm for the management of muscle injuries that integrates clinical and imaging information.
On the basis of our data, we propose an updated (new) definition of muscle injury as “an indirect or direct injury to the muscle leading to an athlete being unable to fully participate in training or match play/competition.”
Summary
Muscle injuries in elite football are more frequent than have been previously described. Foul play is involved in 7.5% of all thigh muscle injuries. Medical history is essential to differentiate direct injuries from indirect injuries. Time-loss direct injuries are less frequent than indirect injuries. These direct injuries are associated with a more rapid return to full function as rehabilitative therapy can usually be more aggressive to the limit of pain tolerance. Thus, direct injuries have a shorter absence time compared to indirect injuries.
What are the new findings?
This very large study characterises direct muscle injuries and compares them with indirect injuries. Overall, thigh muscle injuries (ie, anterior and posterior) are more frequent than have been previously described; about 20% of all time-loss injuries were of the indirect type and 3% of all time-loss injuries were direct injuries. Mean absence after direct injuries was 11 days shorter than after indirect injuries.
How might it impact on clinical practice in the near future?
Our data will help team physicians distinguish different types of muscle injuries and provide more accurate estimates of return to play. These data can help to develop an algorithm for the management of muscle injuries. We respectfully suggest that the definition ‘muscle injury’ be updated to be ‘an indirect or direct injury to the muscle leading to an athlete being unable to fully participate in training or match play/competition’.
Acknowledgments
The authors wish to thank the participating clubs, medical staff and players. The statistical advice of Henrik Magnusson (MSc) is gratefully acknowledged.
References
Footnotes
Contributors PU designed this study, analysed the data and drafted and revised the paper, H-WM-W revised the paper. JE designed and monitored data collection, analysed the data and revised the paper. He is the guarantor.
Funding This study was supported by grants from UEFA.
Competing interests None.
Ethics approval The participating medical teams were informed about the study. The study design underwent an ethical review and was approved by the UEFA Football Development Division and the Medical Committee.
Provenance and peer review Not commissioned; externally peer reviewed.