Article Text

Abstract
Background Despite reported injury rates of up to 3 per 1000 hours exposure, there are no evidence-based prevention programmes in tennis.
Purpose To evaluate the effectiveness of an e-health prevention programme for reducing tennis injury prevalence.
Study design Two-arm, researcher-blinded randomised controlled trial.
Methods Adult tennis players of all playing levels were randomised in an unsupervised programme lasting 12 weeks (TennisReady group or control group). The primary outcome was the overall injury prevalence over a 16-week period, measured at 2 weekly intervals with the Oslo Sports and Trauma Research Centre questionnaire. Estimates for the primary outcome and associated 95% CIs were obtained using generalised estimating equation models. Secondary outcome scores included prevalence of substantial injuries, overall incidence, adherence and time-loss injuries.
Results A total of 579 (83%) (TennisReady n=286, control n=293) participants were included in the primary analysis. The mean injury prevalence was 37% (95% CI 33% to 42%) in the TennisReady vs 38% (95% CI 34% to 42%) in the control group (adjusted p-value 0.93). The prevalence of substantial injuries was 11% (95% CI 9% to 14%) in the TennisReady vs 12% (95% CI 9% to 15%) in the control group (p value of 0.79). Analysis of the secondary outcome scores showed no difference between groups. The mean prevalence rates between high (8%) and low (92%) adherent groups were 32% (95% CI 23% to 44%) and 37% (95% CI 33% to 42%), respectively (p value 0.36).
Conclusion Providing an unsupervised e-health tennis-specific exercise programme did not reduce the injury rates and should not be implemented.
Trial registration number NTR6443.
- tennis
- Injury prevention
- Exercise
- App
- Randomised controlled trial
Statistics from Altmetric.com
Introduction
Tennis is a very popular sport with around 75 million active players worldwide.1 Recent studies show that injury rates vary from 0.04 to 3.0 per 1000 hours played.2–5 The majority of injuries in tennis are overuse injuries, such tendinopathy of the knee, elbow or shoulder (61%–80%) rather than acute injuries.4–6 The high proportion of overuse versus acute injuries is in contrast with previous reports2 and demands new approaches towards injury prevention.
Despite high levels of evidence in favour of exercise-based prevention, predominantly in team sports,7 8 research in this domain for tennis players is lacking. In the absence of any evidence-based prevention strategies in tennis,3 we developed a tennis-specific exercise-based prevention e-health programme9 using the Knowledge Transfer Scheme (KTS) as a guideline.10 The content of this programme was based on exercises from other exercise-based injury prevention programmes.11–14
The aim of this trial was to evaluate whether the TennisReady unsupervised e-health programme reduces the overall injury prevalence compared with usual care. The secondary aims were to evaluate incidence per 1000 hours of tennis exposure.
Methods
Design
The design was a two-arm, researcher-blinded block randomised controlled trial. We followed the Consolidated Standards of Reporting Trials.15 The study protocol was registered in the Netherlands Trial Registry.
Participants
Tennis players were recruited between February 2017 and September 2017 through social media, direct mail, newsletters and flyers at tennis events. Detailed information about the study procedure, participant rights and contact information for further questioning was available online. Eligible tennis players were invited to register online through a survey programme (LimeSurvey, LimeSurvey GmbH, Hamburg, Germany). On registration, online informed consent was obtained.
Tennis players were eligible for inclusion if they were at least 18 years of age, owned an iOS-based or Android-based smart device and were willing to perform an exercise programme at least twice a week. There were no exclusion criteria.
Trial procedure, randomisation and blinding
At the start of the study in May 2017, one author (OK) registered all eligible players who had already indicated that they would like to participate in a data management, survey and randomisation programme (CastorEDC, CIWIT B.V., Amsterdam, The Netherlands). After entry into the database, the players were block randomised in the ratio 1:1 using random blocks of sizes two, four and six. Players registering for participation after this first batch were entered into the system each subsequent week. This meant that each following week, a new batch of players was randomised. A detailed description of the randomisation and blinding procedure is presented in online supplementary appendix A.
Supplemental material
Injury registration
At baseline, all participants received a baseline survey which recorded gender, weight, height and playing level (International Tennis number (ITN))16 for both singles and doubles plays (1–9, 1 being the highest playing level), number of years playing tennis, preferences for singles or doubles play, most frequently used court surface (clay, hardcourt, grass, carpet, all weather courts and multiple courts) and previous lifetime injuries.
The injury survey was sent at 2 weekly intervals over a 16-week period. The injury survey registered the number of hours of tennis exposure, injury locations, injury types, time loss (number of days that players were unable to participate due to injury) and injuries on the modified Oslo Sports and Trauma Research Centre (OSTRC) Questionnaire.4 The OSTRC had been previously validly translated using a forward–backward procedure.4 A detailed description of the OSTRC Questionnaire is given in the online supplementary appendix A.
Intervention
The TennisReady prevention programme was systematically developed and codesigned with the end users (tennis players) through a five-step approach guided by the KTS,10 and has previously been described in full detail.9 The programme was available through a smartphone application (app) on Android and iOS. The app’s content was available for download to enable offline usage.
A detailed description of the 12-week, 7–10 min TennisReady programme is given in online supplementary appendix B, tables S1–S4. Briefly, TennisReady consisted of an on-court warm up programme with cardiovascular, neuromuscular and tennis-specific exercises. An off-court (at home) strengthening programme was available. All exercise regimes were made increasingly difficult every 2 weeks by increasing repetitions or by changing exercises for more complex ones. Players were free to choose between the on-court and off-court alternatives every TennisReady session. All players in the TennisReady group were requested on entry to perform the on-court programme prior to each tennis session or to alternatively perform the off-court programme in order to attempt two exposures to the TennisReady programme per week.
Supplemental material
Participants in the control group were instructed to continue their current warm up and tennis practice.
Outcomes
The primary outcome was the overall injury prevalence as measured with the OSTRC Questionnaire over a 16-week period. A recordable injury was defined as any response above the minimal value on at least one of the four OSTRC questions,14 if the score was not due to an illness.
Secondary outcomes were prevalence of substantial injuries and injury incidence density defined as the total number of injuries per 1000 hours of tennis exposure. Substantial OSTRC injuries were defined as injuries leading to moderate or severe reductions in training, volume or performance, or a total inability to participate.14 We reported injury incidence density and prevalence by anatomical location (ankle, knee, shoulder and elbow). Prevalence and incidence for substantial injuries were also calculated.
Finally, self-reported time loss and self-reported adherence (see online supplementary appendix C) to the intervention were also included as secondary outcomes. Adherence was recorded per survey in five adherence categories (always, almost always, sometimes, never and not applicable) and per exposure category (game play, unsupervised practice and supervised practice). Adherence was then dichotomised into high adherence (always/almost always) and low adherence (sometimes/never/not applicable). In addition, a set of rules was created to summarise the adherence over the three exposure categories into ‘high adherence’ or ‘low adherence’ over all surveys. A more elaborate explanation is available in online supplementary appendix C.
Sample size
We calculated that for a 50% reduction in period prevalence of overall injury from 0.2417 to 0.12, α of 0.05 and β of 0.90, a sample of 230 participants per group was needed. Correcting for an estimated dropout rate of 30%, we set the sample size at 329 per group. Hence, we aimed to randomise at least 658 participants.
Statistical analysis
We used descriptive statistics to present the baseline characteristics, the results of the OSTRC survey, and adherence in both the intervention and control group. We examined whether continuous variables were normally distributed by visually examining histograms. We described normally distributed continuous variables using the mean and SD, non-normally distributed continuous variables using the median and lower and upper limits of the IQR, and categorical variables using counts and percentages. We compared the intervention and control groups’ baseline characteristics using unpaired t-tests, Mann-Whitney U test and Fisher exact test, as appropriate.
The analyses of the primary and secondary outcomes were performed based on an intention-to-treat principle, available data, and a joint analysis of the primary outcome and missing data process. For the modified intention-to-treat analyses, a participant was considered available for the analysis of the primary outcome if the baseline questionnaire and at least one follow-up survey had been completed.
For the primary outcome, injury prevalence was calculated as the number of players reporting an injury divided by the total number of returned questionnaires per injury survey instance.14 Estimates for the injury prevalence over the whole period and associated 95% CIs were obtained using generalised estimating equations (GEEs) with a binomial distribution and logit link function. A similar GEE model was used to examine the association between intervention group and the missing data process. To correct for potential confounders, we performed an additional GEE analysis on the injury prevalence, correcting for previous injury,18 multiple court surface use versus non-multiple court surface use6 and gender.19 These three confounders have been previously identified in a review on risk factors for injuries in tennis players.3 In order to test the robustness of our analysis, worst case, best case and complete data analyses were performed (see online supplementary appendix C). For the secondary outcome testing, see online supplementary appendix C.
Results
Participants and follow-up
Between May and September 2017, 1084 tennis players expressed an interest in participating in the trial. In total, 700 met the inclusion criteria; of these, 349 were randomly assigned to the TennisReady trial arm and 351 were assigned to the control arm. A total of 121 participants (17%) (TennisReady group=63 and control group=58) completed none of the injury surveys and thus were unavailable for analysis. Hence, a total of 579 participants (83%) (TennisReady group=286 and control group n=293) could be included in the analysis of the primary outcome. Seven participants (1%) (TennisReady group=5 and control group=2) withdrew from the trial after having completed at least one survey; their incomplete data were used for the modified intention-to-treat analysis up to their withdrawal. Complete data were available for 152 participants (22%) (TennisReady group=60 and control group=92). Figure 1 shows a flowchart of the entire recruitment process. Online supplementary appendix D, figure S1, illustrates the number of participants included in the study over time.

Flowchart of the study procedure.
The participant baseline characteristics were similar between the groups (table 1). The mean age was 41 years (SD 12) in the TennisReady group vs 42 years (SD 13) in the control group. All participants were recreational tennis players with a median single-player level ITN of 7 in both groups (IQR 5–8 and 6–8 for TennisReady group and control group, respectively). There were 157 (55%) women in the TennisReady group and 149 (51%) in the control group. At baseline, >80% of participants in both groups had experienced a previous injury.
Baseline characteristics
Response rate and exposure
As illustrated by online supplementary figure S2 of online supplementary appendix D, the response rate decreased over the 16-week period from 98% (n=281) and 97% (n=285) (TennisReady and control groups, respectively) to 34% (n=96) and 48% (n=139), respectively. Sixty participants (17%) in the intervention group and 92 (26%) in the control group completed all surveys.
Supplemental material
A total of 22 076 exposure hours were recorded (10 366 hours for the TennisReady group vs 11 710 hours for the control group) over the period of 16 weeks, with a corresponding median of 27 hours (IQR 13–51) per player in the TennisReady group vs 32 (IQR 21–55) hours of exposure per player in the control group. This difference was statistically significant (p value of <0.01).
Primary outcome
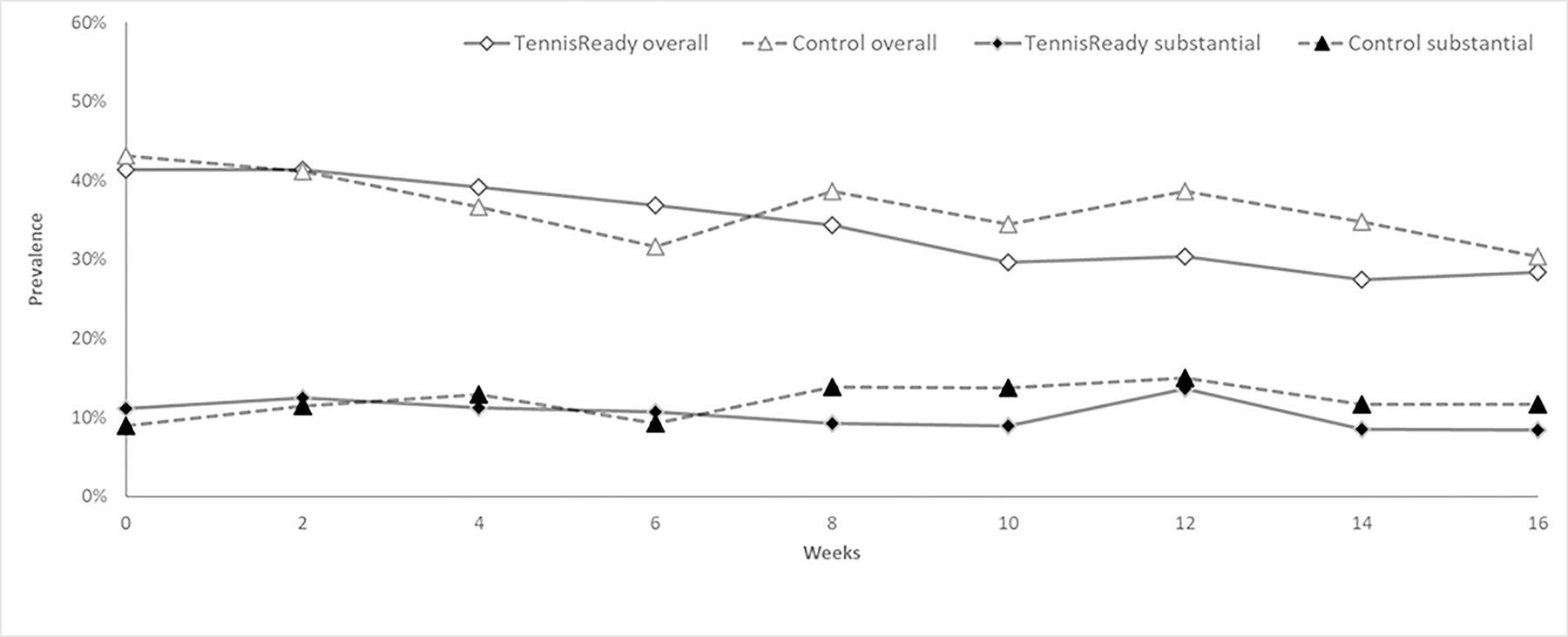
The overall injury prevalence was 37% (95% CI 33% to 42%) in the intervention group vs 38% (95% CI 34% to 42%) in the control group. Figure 2 illustrates the injury prevalence over time. After correcting for previously defined confounders, the adjusted p value was 0.93 (table 2). The sensitivity analysis showed that the outcome of the primary analysis did not change in the outcome effect for the worst-case and complete data scenarios (table 2). The best-case scenario was in favour of the TennisReady group, although CIs overlap.

{kind=link}
{kind=link}
Overall injury prevalence (open symbols) and substantial injury prevalence (filled symbols) in the TennisReady (black lines) and control (dotted lines) at 2 weeks’ interval over the 16-week period.
Primary outcome scores (prevalence) and sensitivity analysis with 95% CIs
Secondary outcomes
Incidence and substantial injuries
The overall injury incidence was 25.4/1000 hours of tennis exposure (95% CI 22.5 to 28.7/1000 hours) in the TennisReady group vs 24.4/1000 exposure hours (95% CI 21.8 to 27.4/1000 hours) in the control group. The prevalence of substantial injuries was 11% (95% CI 9% to 14%) in the TennisReady group vs 12% (95% CI 9% to 15%) in the control group (p value 0.79) (table 3 and figure 2). Poisson corrected GEE showed no difference between groups. No differences were found for location-specific incidences (table 3).
Secondary outcome scores with 95% CIs
Time-loss injuries
The mean time loss per injury was 5.6 days (95% CI 5.4 to 5.9) in the TennisReady group and 6.3 days (95% CI 6.0 to 6.6) in the control group (Poisson corrected GEE model p<0.01). We did not consider this difference to be clinically relevant.
Adherence
For the 2 weeks’ adherence scores during the intervention period, 110 questionnaires out of 1401 (8%) met the algorithm for high adherence. When comparing the algorithmically selected high-adherence group with the low-adherence group, the mean prevalence rates were 32% (95% CI 23% to 44%) and 37% (95% CI 33% to 42%), respectively. This was not statistically significant (p=0.36). When comparing the algorithmically selected high-adherence group, the mean prevalence rates were 32% (95% CI 23% to 44%) for the high-adherence group and 38% (95% CI 34% to 42%) for the control group, respectively, with no statistical significant difference between these groups (p=0.63).
Discussion
Our randomised controlled trial involved almost 600 non-professional tennis players. We showed that providing a 7–10 min e-health tennis-specific unsupervised prevention programme of 12 weeks was not effective for reducing injury prevalence and incidence.
Comparison with other studies
This study was the first randomised controlled trial to evaluate an exercise-based prevention strategy in tennis,3 which prevents comparison with other tennis prevention studies. Exercise-based prevention strategies have previously been investigated in both team and individual sports7 8 20–22 with varying results. In these studies, coach-supervised programmes in team sports (eg, football and handball) were often successful.7 8 Unsupervised exercise-based prevention programmes have been found effective in reducing the number of recurrent acute ankle injuries.12 No other unsupervised exercise programmes in individual sports have been successful in significantly reducing injury rates.7 20–22 Unfortunately, our results are in line with these previous findings.
Adherence
In contrast to some other sports, a warm-up is generally not performed by recreational tennis players.9 Nevertheless, during the systematic development of our intervention, 75% of the respondents reported to be motivated to perform warm-up exercises at least twice a week.9 In our controlled research setting, the overall adherence was not optimal. We cannot exclude that the effect of the intervention was influenced by lack of adherence with the intervention programme.
The definitions of the degree of adherence (high vs low), methods (coach vs player reporting) and frequency of measurements differ among studies.23 We categorically defined a high player adherence as performing the exercises ‘always’ or ‘nearly always’ for at least half of their exposure types, which might be considered as a relatively high threshold. In a comparable multimodal intervention programme in Norwegian amateur youth football players (FIFA 11+),24 a high-adherence threshold was defined as performing the exercises at least once a week (despite the recommended frequency of twice a week). They reported high player adherence in only 47%. Similarly, in professional Norwegian handball,14 a relatively low percentage of high player adherence was scored (53%, threshold 3/week). As both Norwegian studies showed positive outcomes, despite less than one out of two participants meeting the criteria for high adherence, it remains unknown if the negative results in our study can be contributed exclusively to our reported adherence rates.
Content, delivery, receipt and quality of the intervention
Another explanation for the absence of a preventive effect might be that the content, delivery, reception and/or quality of the performance of the exercises were ineffective. Although the content of our programme was based on other effective multimodal exercise-based prevention schemes in sports,9 11–14 there is no evidence that any of the exercises by itself was effective in reducing injuries. In all previously used programmes,11–14 a combination of different exercises was used, often with a specific focus on lower or upper extremity injuries only.
The delivery was through an app-based programme which included offline videos and written instructions in order to improve the delivery of the content. However, no push messages, in case of non-use, were integrated and the app did not include a feedback feature. This might have influenced the reception of and adherence to the intervention. The main limitation of strictly app-based interventions might be the absence of supervision by a coach (quality control). This could have resulted in poor execution of the exercises, rendering them ineffective.
Strengths and limitations
We are the first to publish a large-scale randomised controlled trial investigating injury prevention in tennis players. An important strength of our trial was that the programme was developed using a systematic approach guided by the KTS.9 10 Through this bottom-up approach, the target users were involved throughout the complete process of the development of the intervention. The unsupervised (less controlled) intervention reflected daily practice of predominantly unsupervised exposure at a recreational level, which strengthens the external validity. The biweekly validated OSTRC Questionnaires enabled registration of all acute and overuse injuries without restriction to time-loss injuries only, resulting in a larger number of reported injuries and increased power of the study.
Due to the nature of the intervention, blinding and allocation concealment of the participants was not possible. We did attempt to optimise blinding of the assessors as much as possible, and all involved remained blinded while interpreting the results. In an attempt to ensure unbiased interpretation of the results, the raw data were analysed and recorded by an independent statistician. The code was broken once the authors agreed on the interpretation of the results.
Due to the unsupervised and less controlled setting, we were unable to verify completion of each single exercise (within session adherence) and the quality of the exercises. Random visits could have given us more information about the quality of the performed intervention.
Another limitation was the mean response rate of completing the biweekly questionnaires of 56%–66%, which decreased over time to 17% (intervention)−26% (controls). This resulted in extensive missing data, leaving room for attrition and reporting bias. We have attempted to reduce this risk by performing best-case and worst-case scenarios on the data, which showed no relevant differences.
In the absence of a well-defined golden standard,23 it was decided to categorically evaluate the adherence at player’s level. Registration at player level of the number of completed exercise sessions per week would have enabled quantification of adherence as a continuous variable (instead of categorical). Prior to the trial, we attempted to recruit tennis school trainers and create a supervised setting. However, due to insufficient responses, we were unable to achieve this and missed the unique chance to evaluate whether a supervised setting would have been associated with a higher adherence.
Considering the low response rate, the risk of measurement and attrition bias and the lack of quality control, we urge readers to interpret our data with caution. Based on our experience during this trial, we have made the below-mentioned recommendations for future research in tennis.
Recommendations for future interventions studies in tennis
In future studies, potential improvement of adherence and superior exercise quality control could be tested in a coach-based supervised setting. Alternatively, quality control with random visits could be implemented. The recording of the number of sessions the intervention was used, a limitation we faced in our analysis, seems imperative for future researchers. Other studies using apps will have to show whether this mode of content delivery for exercise-based prevention interventions is effective. Lastly, uniform adherence definitions and validated and reliable adherence measures are required for comparison within and between studies.
Should it change daily practice?
Considering the lack of effect, we do not recommend the use of similar unsupervised e-health injury prevention schemes in tennis players.
Conclusion
In its current form, the unsupervised e-health exercise programme did not reduce the risk of tennis injuries. It questions the use of unsupervised e-health prevention programmes in tennis, and the current intervention is not recommended for implementation.
What are the findings?
Providing an e-health tennis-specific unsupervised exercise programme of 12 weeks, a 7–10 min exercise programme, did not reduce the risk of tennis injuries.
How might it impact on clinical practice in the future?
Our unsupervised e-health prevention programme should not be implemented in recreational tennis.
We suggest evaluating the programme in a coach-based supervised setting.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @docpluim, @Evertverhagen, @vgouttebarge
Contributors HIMFLP, JLT, VG, EV and BMP were involved in the design of the trial. HIMFLP, JLT, BMP and OK were involved in the recruitment. HIMFLP and OK were involved in the data collection. RH designed the statistical plan and performed the statistical analysis. HIMFLP was responsible for drafting the manuscript. All authors reviewed and agreed on the manuscript.
Funding The study was partly funded by a grant (grant number 50-53600-98-015) from the Netherlands Organization for Health Research and Development, a governmental institution that finances research to improve healthcare in the Netherlands.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The medical ethics committee of the Academic Medical Center Amsterdam gave permission for the study with an exempt status (qualified as non-WMO obliged research, W16_321 17.066). The study protocol was registered in the Dutch trial register (NTR6443).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information. -