Article Text

Abstract
Background Older people are at high risk of physical inactivity. Activity trackers can facilitate physical activity. We aimed to investigate the effect of interventions using activity trackers on physical activity, mobility, quality of life and mental health among people aged 60+ years.
Methods For this systematic review, we searched eight databases, including MEDLINE, Embase and CENTRAL from inception to April 2018. Randomised controlled trials of interventions that used activity trackers to promote physical activity among people aged 60+ years were included in the analyses. The study protocol was registered with PROSPERO, number CRD42017065250.
Results We identified 23 eligible trials. Interventions using activity trackers had a moderate effect on physical activity (23 studies; standardised mean difference (SMD)=0.55; 95% CI 0.40 to 0.70; I2=86%) and increased steps/day by 1558 (95% CI 1099 to 2018 steps/day; I2=92%) compared with usual care, no intervention and wait-list control. Longer duration activity tracker-based interventions were more effective than short duration interventions (18 studies, SMD=0.70; 95% CI 0.47 to 0.93 vs 5 studies, SMD=0.14; 95% CI −0.26 to 0.54, p for comparison=0.02). Interventions that used activity trackers improved mobility (three studies; SMD=0.61; 95% CI 0.31 to 0.90; I2=10%), but not quality of life (nine studies; SMD=0.09; 95% CI −0.07 to 0.25; I2=45%). Only one trial included mental health outcomes and it reported similar effects of the activity tracker intervention compared with control.
Conclusions Interventions using activity trackers improve physical activity levels and mobility among older people compared with control. However, the impact of activity tracker interventions on quality of life, and mental health is unknown.
- physical activity
- walking
- aging/ageing
Statistics from Altmetric.com
Introduction
There is compelling evidence that regular physical activity is among the most important lifestyle factors for maintaining physical function, improving quality of life, and decreasing depression and cognitive impairment in older age.1 2 However, older people are at the highest risk of inactivity, particularly those aged 80 years and older.3 4 In the context of a rapidly ageing global population, there is clearly a need for effective strategies to increase physical activity participation in older age.5
Public health physical activity guidelines for adults recommend at least 150 min per week of moderate-to-vigorous intensity activity plus strengthening exercises to provide substantial health benefits.6–9 It can also be expressed as 30 min of brisk walking 5 days a week.6 7 10 Walking is an easy, inexpensive and highly accessible way of meeting physical activity guidelines with few adverse effects.10–12 Thirty minutes of daily moderate-to-vigorous physical activity (MVPA) accumulated in addition to habitual daily activities in healthy older adults equates to approximately 7000–10 000 steps/day.7 8
Physical activity trackers such as pedometers are portable, easy-to-use and affordable devices that quantify and provide immediate feedback on the number of steps walked per day.10 13 A previous systematic review identified that use of pedometers was associated with a 27% increase in adults’ physical activity levels and was associated with significant reductions in body mass index by 0.38 (95% CI 0.05 to 0.72; p=0.03) and blood pressure by 3.8 mm Hg (95% CI 1.7 mm Hg to 5.9 mm Hg, p<0.001).14 Interventions using activity trackers can facilitate physical activity behaviour change by prompting goal setting and enhancing motivation and self-efficacy.10 15 16
There is a lack of published research investigating the effectiveness of interventions using activity trackers in the older population. Only one previous review has examined the effect of activity tracker use in improving physical activity in adults (mean (SD) age of 49 (9) years),14 and as it included only five studies involving participants with a mean age older than 60 years, the generalisability of their results to older populations is limited.
To address this current evidence gap, we conducted a systematic review and meta-analysis of randomised trials that investigated the effect of interventions using physical activity trackers on physical activity levels compared with usual care or another physical activity intervention among people aged 60 years and older. Additionally, we evaluated the effect of activity trackers on mobility, quality of life and mental health among people aged 60 years and older.
Methods
Search strategy
We conducted this systematic review following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.17 This review was performed following the methods documented in the protocol registered with the PROSPERO database prior to commencement (#CRD42017065250).
We searched the following eight databases from inception to April 2018: MEDLINE (Ovid) (from 1946), Embase (Ovid) (from 1980), Cochrane Central Register of Controlled Trials (CENTRAL) (Ovid) (1991), PsycINFO (ovid) (from 1806), the Physiotherapy Evidence Database (PEDro) (from 1999), SPORTDiscus (EBSCO) (from 1949), Lilacs (from 1987) and CINAHL (EBSCO) (from 1982). Keywords, MeSH and other index terms, as well as combinations of these terms and appropriate synonyms, were used to construct the search strategy, including ‘pedometer’, ‘activity tracker’, ‘step counter’, ‘older people’, ‘aged’, ‘randomised’ and ‘controlled trial’ (see online supplementary appendix 1). We also screened reference lists of relevant reviews and trials for additional studies. No restrictions were placed on the language, date, the setting or context of the included studies.
Supplemental material
Two reviewers independently screened titles and abstracts of potential articles. Where there was uncertainty about the eligibility of a trial, the full text was retrieved. Two independent reviewers read full-texts and assessed eligibility criteria using an electronic screening form. Articles were independently screened in two stages: screening of title and abstracts, and screening of full-text articles by two reviewers (JSO and ERYZ) using the eligibility criteria (box 1). Disagreements regarding the eligibility of studies were resolved through discussion and, when necessary, with the help of a third reviewer (AT). The PRISMA study flow diagram was included to document the screening process.
Inclusion criteria
Design: Randomised controlled trials.
Participants: Adults aged 60 years and over.
Intervention: Activity tracker-based intervention aimed at increasing physical activity participation.
Control: No intervention, usual care, wait-list control or another physical activity intervention.
Outcomes measured related to: Physical activity (steps per day), mobility, quality of life and mental health.
Selection criteria
Type of studies
We included individual and cluster-randomised controlled trials (RCTs).
Type of participants
Trials conducted with participants aged 60 years and older, or trials in which participants had an average or median age of at least 60 years were included in this review. We considered eligible trials that included healthy older adults as well as trials that included older people with specific health conditions.
Type of interventions
Trials were included if the intervention was an activity tracker-based intervention aimed at increasing physical activity participation. We included studies in which the activity tracker was: (1) The single component of the intervention. (2) The main focus of the intervention but supported by physical activity counselling. (3) Incorporated as an important part of a broader physical activity intervention. Additionally, trials were considered eligible if the intervention was designed to allow participants to monitor their number of steps per day. We excluded trials if the intervention: (1) Did not involve an individualised activity tracker intervention. (2) Included more than two face-to-face visits. (3) Did not allow participants to see the number of steps taken on the activity tracker. (4) If the activity tracker was used only as a measure tool, but not as part of the intervention. For example, if a study involved physical activity counselling, but did not include the use of an activity tracker as a motivational tool component of the intervention, this study was excluded, even if the activity tracker was used to measure the physical activity outcome.
Type of outcome measures
Although physical activity encompasses a broader term such as ‘any bodily movement produced by skeletal muscles that requires energy expenditure, including activities undertaken while working, playing, carrying out household chores, travelling, and engaging in recreational pursuits’,18 for the purpose of this review, the primary outcome was physical activity operationalised as steps per day only, measured by activity tracker or accelerometer. Other types of objective measures, such as counts per minute and accelerometer-determined MVPA, as well as self-reported physical activity measures were not included in the analysis. Measurement of steps per day was required as part of the eligibility criteria of trials for this review. The secondary outcomes were (1) Mobility, including any validated method measuring gait speed, sit to stand, functional tests or other mobility scales. (2) Quality of life, including any validated questionnaire of health-related quality of life, health status or functional status. (3) Mental health, including self-reported validated questionnaires of depression and anxiety.
Data extraction
Two independent reviewers (JSO and ERYZ) extracted the characteristics and intervention outcomes of each trial according to the PRISMA statement19 using a standardised electronic data extraction form. The following data were extracted from each included trial: author, year of publication, country, sample characteristics (sample size, age and sex of participants and setting), intervention description (duration; type of intervention; type of device) and methodological quality assessment using the PEDro Scale. We also extracted intervention details of the included studies according to the Template for Intervention Description and Replication (TIDieR) framework.
Outcome data were extracted from baseline, at first follow-up and subsequent follow-up score when available. Preintervention and postintervention scores were used when available. If baseline values were not reported, groups were compared at follow-up. If multiple follow-up data points were provided, the scores obtained as close to the completion of the intervention as possible were used for the primary analysis.
Authors of the included studies were contacted by email if the trial reports were incomplete or data were missing. If the author did not reply within 2 weeks, a second email was sent as a reminder. If at the end of the fourth week a reply was not received, available data were used.
Methodological quality assessment
We evaluated the methodological quality of included trials using The PEDro Scale, which assesses the internal validity of an RCT.20 21 The PEDro Scale evaluates 11 items: inclusion criteria and source, random allocation, concealed allocation, similarity at baseline, subject blinding, therapist blinding, assessor blinding, completeness of follow-up, intention-to-treat analysis, between-group statistical comparisons, and point measures and variability. Scores on the PEDro Scale range from 0 (very low methodological quality) to 10 (high methodological quality) and were downloaded from the PEDro database (https://www.pedro.org.au/). Methodological quality was not an inclusion criterion for this review.
Assessment of quality of the evidence
We used the GRADE system to assess the overall quality of the evidence22 for an outcome which has results from three or more studies. We evaluated the general statement regarding the quality of the body of evidence as ‘High’, ‘Moderate’, ‘Low’ or ‘Very Low’ based on the presence or extent of four factors: risk of bias, inconsistency of the effect, imprecision and publication bias. The GRADE classification was downgraded by one level for each of five factors we encountered: (1) Design limitations (a sensitivity analysis showing change of results with removal of the trials with low methodological quality: PEDro score <6). (2) Inconsistency of the effect (large heterogeneity between the trials I2 >60%). (3) Imprecision (wide CIs). (4) Reporting bias (a funnel plot showing evidence of small study effects). We did not consider the indirectness criterion, a feature from GRADE, in this review as it encompasses a specific population (older people) with relevant outcome measures (physical activity, mobility, quality of life and mental health) and direct comparisons. Standardised qualitative statements were used to describe the different combinations of effect size and the certainty of evidence.23
Data analysis
We performed meta-analyses with Comprehensive Meta-Analysis software (V.3, Biostat, Englewood, New Jersey, USA) using the random effects model for each outcome (physical activity, mobility, quality of life and mental health). We calculated treatment effects using standardised mean differences (SMDs) (Hedges’ g) standardised by postscore SD (or its estimate) with 95% CIs. SMD was calculated using the premean and postmean and SD or, when this was unavailable, we used the mean change score. If the trial had more than two arms, we examined the overall effects of the intervention versus control by pooling the individual effect of each arm (means and SD). Effect sizes were categorised as small (0.2), medium (0.5) or large (0.8 or greater).24
As SMD is reported in units of SD, the size of the overall intervention effect can be difficult to interpret.25 For that reason, we also calculated the difference in means (postintervention minus preintervention steps per day), which facilitates clinical interpretation. We visually inspected the forest plot for evidence of heterogeneity with consideration of the I2 and χ2 tests. We determined clinical heterogeneity by consensus among the investigators.
Meta-regression was conducted for the primary outcome to examine the effect of participants’ characteristics on the pooled effect size. We investigated if there were significant differences in the intervention effect sizes between trials that included participants with clinical conditions and those that were recruited from the general older population. Additionally, a meta-regression was carried out for physical activity to explore the impact of trial sample size on the pooled effect of the activity tracker-based intervention. We dichotomised the trial sample size into two categories: small trials (n ≤100 participants) and large trials (n >100 participants). A meta-regression was also carried out to explore whether there were differences in the effect of interventions that used accelerometers and those that used pedometer to measure the physical activity outcome. Further meta-regression was undertaken to determine if there were significant differences in the intervention effect sizes between trials involving short-term interventions (less than 12 weeks) and long-term interventions (equal to or more than 12 weeks). To assist with the GRADE rating, we undertook another meta-regression to examine the impact of trial methodological quality, as measured with the PEDro Score, on the pooled effect of the activity tracker-based intervention. Trials were dichotomised into two categories of higher methodological quality (PEDro Scores ≥6) and lower methodological quality (PEDro Scores <6). Furthermore, we used funnel plots of the effect estimates from included studies to assess small study effects. We assessed funnel plot asymmetry visually and by using Egger’s test, with p<0.1 as evidence of publication bias.26
Results
Flow of trials through the review
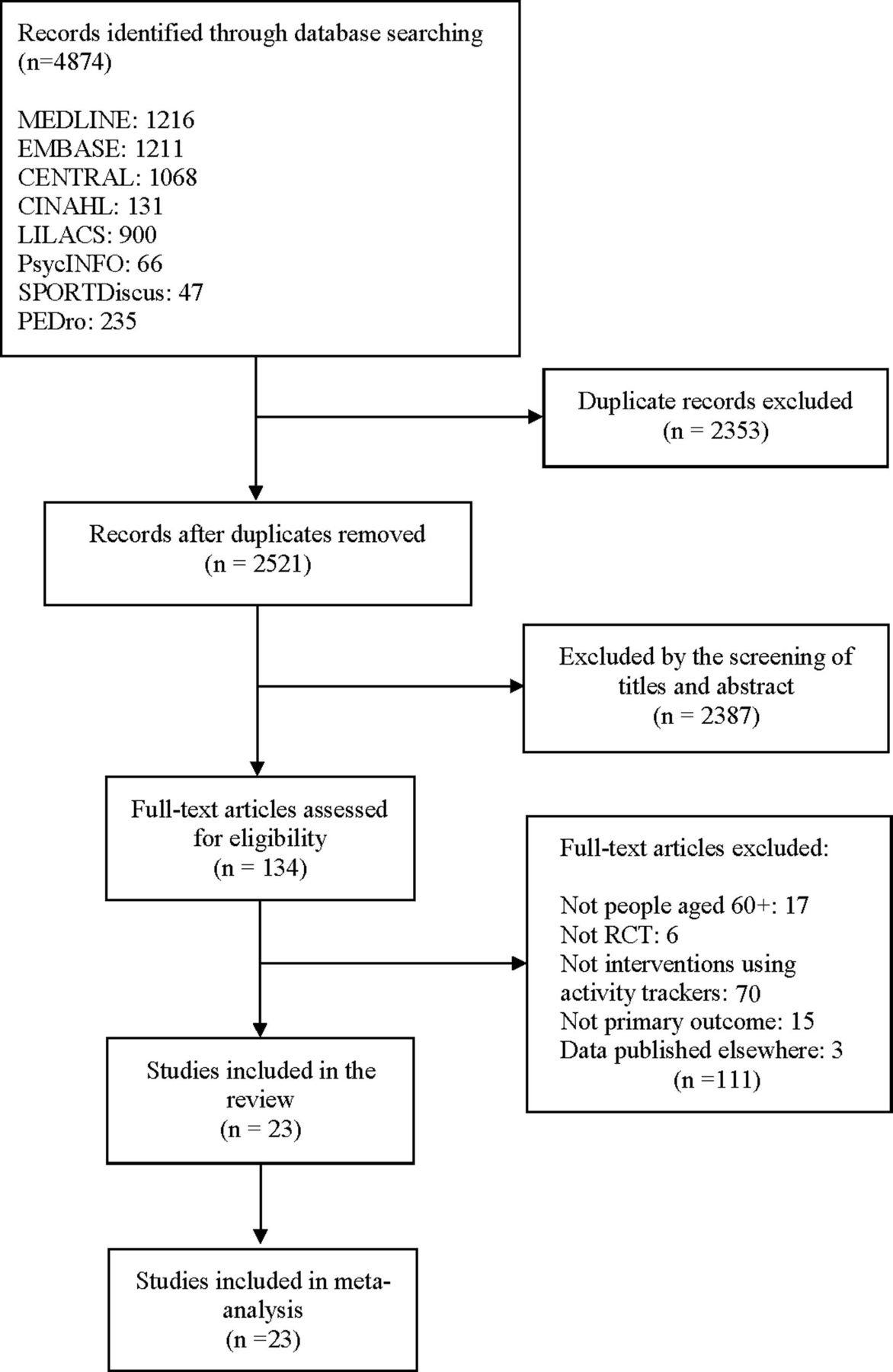
Our literature search identified a total of 4874 studies. After removing duplicate citations, 2521 studies remained for the title and abstract screening, of which 134 were considered potentially eligible studies for full-text review. After the full-text screening, 23 eligible trials were identified and included in the review.27–49 Figure 1 outlines the flow of studies through the review.

Flow of studies through the review. RCT, randomised controlled trial.
We pooled all included trials in the primary meta-analysis evaluating the effect of interventions that use activity trackers on physical activity in older people.27–49 For one trial that presented the data by gender, gender groups were separated for analysis. For secondary analyses, three trials were included reporting a mobility outcome,28 39 44 nine trials were pooled reporting quality of life outcome29 32 33 36 38 39 45 47 49 and only one trial included mental health outcomes (depression and anxiety).49 There were no included trials comparing an intervention that used activity trackers to another physical activity intervention.
Characteristics of included trials
Publication dates ranged from 2003 to 2017 (median, 2014) with 48% of trials published after 2015. Studies were conducted in 10 different countries: single trials were conducted in Canada,30 Chile,36 Portugal29 and Belgium/Greece/UK/Switzerland/The Netherlands;32 two in Belgium;31 33 eight in the UK34 35 37 38 45 47–49 and nine in USA.27 28 39–44 46 Details of all included trials are summarised in online supplementary appendix 2.
Supplemental material
Quality
Online supplementary appendix 3 summarises the methodological quality and reporting of eligible trials. The total PEDro Score ranged from 3 to 8 (mean of 6). For the physical activity outcome, 14 trials were of high methodological quality on the PEDro Scale, and 9 were of low quality. For mobility, all three trials were of low methodological quality. For the quality of life, six trials were of high methodological quality, while three were low. For mental health, the only trial that reported this outcome was of high methodological quality. All participants were randomly allocated and provided the calculation of point estimates and variability (PEDro items 2 and 11). Nine trials out of 23 (39%) failed to undertake an intention-to-treat analysis. None of the trials included blinded participants or blinded therapists, as it is expected in this type of intervention.
Supplemental material
Participants
A total pooled sample of 2766 participants was included in the primary analysis of physical activity. Trials reporting data on 218 participants were included in the mobility analysis. Trials included in the quality of life analysis involved 1436 participants, and for mental health, one included trial involved 657 participants for the anxiety outcome and 657 for the depression outcome.
In the trials reporting age, the mean age of participants ranged from 60 years to 80 years, and all included studies recruited both men and women. Participants were recruited from five settings: community,27 28 39 40 42–44 hospital,31–33 36 38 45 46 primary care,30 34 37 41 47–49 primary care and hospital,29 and workplaces.35 Of 14 trials that recruited participants with clinical conditions, 5 recruited patients with chronic obstructive pulmonary disease (COPD),29 32 33 36 38 4 trials recruited participants with type 2 diabetes,31 34 46 49 2 trials included participants with osteoarthritis,41 44 and single trials recruited participants with impaired glucose tolerance,48 intermittent claudication,45 and type 2 diabetes and hypertension.30
Outcome measures
For the primary outcome of physical activity, 16 studies27 28 30 31 36–44 46–48 used a pedometer and 7 trials32–35 45 49 50 used accelerometers to measure steps per day (see online supplementary appendix 2). Scores from the chair-stand test39 44 and Short Physical Performance Battery28 were pooled to investigate the impact of the interventions using activity trackers on mobility. Scores from the St George’s Respiratory Questionnaire29 36 EuroQol-5D,45 47 health status measured using the COPD assessment test,32 33 Chronic Respiratory Disease Questionnaire,38 15D health-related quality49 and the 36-item Short Form Health Survey,39 42 were pooled for quality of life analysis. For mental health the Hospital Anxiety and Depression Scale was used to measure anxiety and depression.49
Intervention
The duration of the interventions in the included trials ranged from short (ie, 4 weeks) to as long as 52 weeks, and the mean duration was 12 weeks. Three studies30 40 43 used activity trackers as a single component of the intervention and 20 included studies27–29 31–39 41 42 44–49 incorporated activity trackers as an important part of the intervention. All included studies incorporated supporting components to increase motivation, such as setting of daily step goals and/or use of step diaries. No studies compared interventions using activity trackers to another physical activity intervention.
The activity tracker-based intervention of 11 studies used the Yamax pedometer,27–31 38 42 44–46 49 3 studies used the Omron pedometer,35 40 43 2 studies used the New Lifestyles pedometer37 47 and single trials used Fitbit Ultra,33 Fitbug air,32 Jawbone Up,41 Tanita36 and e-style pedometer.39 Two trials did not report the type of activity tracker used in the intervention.34 48 Details of included studies according to the TIDieR framework are summarised in online supplementary appendix 4.
Supplemental material
Adverse events
Only four included trials measured adverse events related to the physical activity intervention.32 38 41 Two trials reported musculoskeletal events that were possibly attributable to the intervention, such as knee pain, back pain and rib fracture.32 37 A single trial reported hospital admissions; however this trial included participants with COPD, and the proportion of participants who experienced hospital admissions was similar between intervention group and control group.38 The remaining trial reported that no major adverse events related to the intervention occurred.41
Publication bias
The funnel plot for physical activity displayed overt asymmetry, and the Egger’s tests revealed significant publication bias (p=0.002, see online supplementary appendix 5). However, no significant publication bias was found for quality of life outcome (p=0.11, see online supplementary appendix 5).
Supplemental material
The effect of interventions using activity trackers on physical activity levels
The pooled effect of the interventions using activity trackers on physical activity showed that participants allocated to activity tracker intervention significantly increased their physical activity by 1558 steps per day more than control participants (95% CI 1099 to 2018 steps per day; p<0.001, I2=92% (95% CI 90% to 94%), prediction interval (PI)= −594 to 3711, figure 2), and this represented a medium effect of the intervention on the primary outcome (23 studies; SMD=0.55; 95% CI 0.40 to 0.70; p<0.001, I2=86% (95% CI 80% to 90%), PI=−0.08 to 1.19; figure 3). The overall quality of evidence for the effect of activity tracker intervention on physical activity was rated as ‘low quality’ (see online supplementary appendix 6).
Supplemental material

Difference in means (95% CI) of interventions using activity trackers on physical activity by pooling data from 23 studies comparing activity tracker use versus control using random-effects meta-analysis (n=2766).

Effect size (95% CI) of interventions using activity trackers on physical activity by pooling data from 23 studies comparing activity tracker use versus control using random-effects meta-analysis (n=2766).
There is some indication of maintenance of the effect of activity tracker use in increasing physical activity at 6 months (three studies; SMD=0.69; 95% CI 0.16 to 1.23; p=0.016, I2=76%), but not at 3 months (four studies; SMD=0.14; 95% CI −0.08 to 0.35; p=0.64, I2=0%) (see online supplementary appendices 7 and 8). Only one study reported data for ≥12 months.49 Overall, the differences between the activity tracker intervention and control group were not sustained at 12 months (mean difference=210; 95% CI −148 to 567; p=0.25) and 24 months (mean difference=184; 95% CI −378 to 746; p=0.52) after intervention completion.
Supplemental material
Supplemental material
We found no significant difference in the impact of interventions using activity trackers on physical activity levels between trials that included participants with clinical conditions and those recruited from the general older population (p=0.76). In the 14 trials that included participants with clinical conditions (SMD=0.54; 95% CI 0.25 to 0.82; p=0.001), a medium pooled effect of activity tracker-based interventions was found. However, for the nine trials that included general population participants, a larger pooled effect on physical activity was found (SMD=0.61; 95% CI 0.25 to 0.96; p=0.002).
In the 10 trials that had a sample size greater than or equal to 100 participants, the pooled effect of interventions that use activity trackers was medium (SMD=0.40; 95% CI 0.10 to 0.70; p=0.011). For the 14 trials with a sample size of less than 100 participants, a larger effect was found (SMD=0.72; 95% CI 0.42 to 1.01; p<0.001). The difference between groups was not statistically significant (p for comparison=0.14).
In the 14 trials with PEDro Score of 6 or more (indicating reduced risk of bias), the impact of the interventions using activity trackers was medium (SMD=0.65; 95% CI 0.37 to 0.93; p<0.001), which was similar (p=0.34) to the effect in 9 trials with PEDro Score less than 6 (SMD=0.44; 95% CI 0.092 to 0.78; p=0.02).
We did not detect a significant difference in the impact of activity tracker-based interventions on physical activity between trials that used accelerometers and those that used pedometers to measure physical activity (p=0.054). In the 7 trials that used accelerometers, a small pooled effect on physical activity was found (SMD=0.24; 95% CI −0.15 to 0.63; p=0.23), and in the 16 trials that used pedometers, a larger pooled effect on physical activity was detected (SMD=0.69; 95% CI 0.45 to 0.93; p<0.001).
In the 18 trials involving long-term interventions (defined as 12 or more weeks), the impact on physical activity was large (SMD=0.70; 95% CI 0.47 to 0.93; p<0.001). For the five trials involving short-term interventions (less than 12 weeks), a small pooled effect was found (SMD=0.14; 95% CI −0.26 to 0.54; p=0.47). The difference between the subgroups was statistically significant (p=0.02).
The effect of pedometer-based interventions on secondary outcome measures
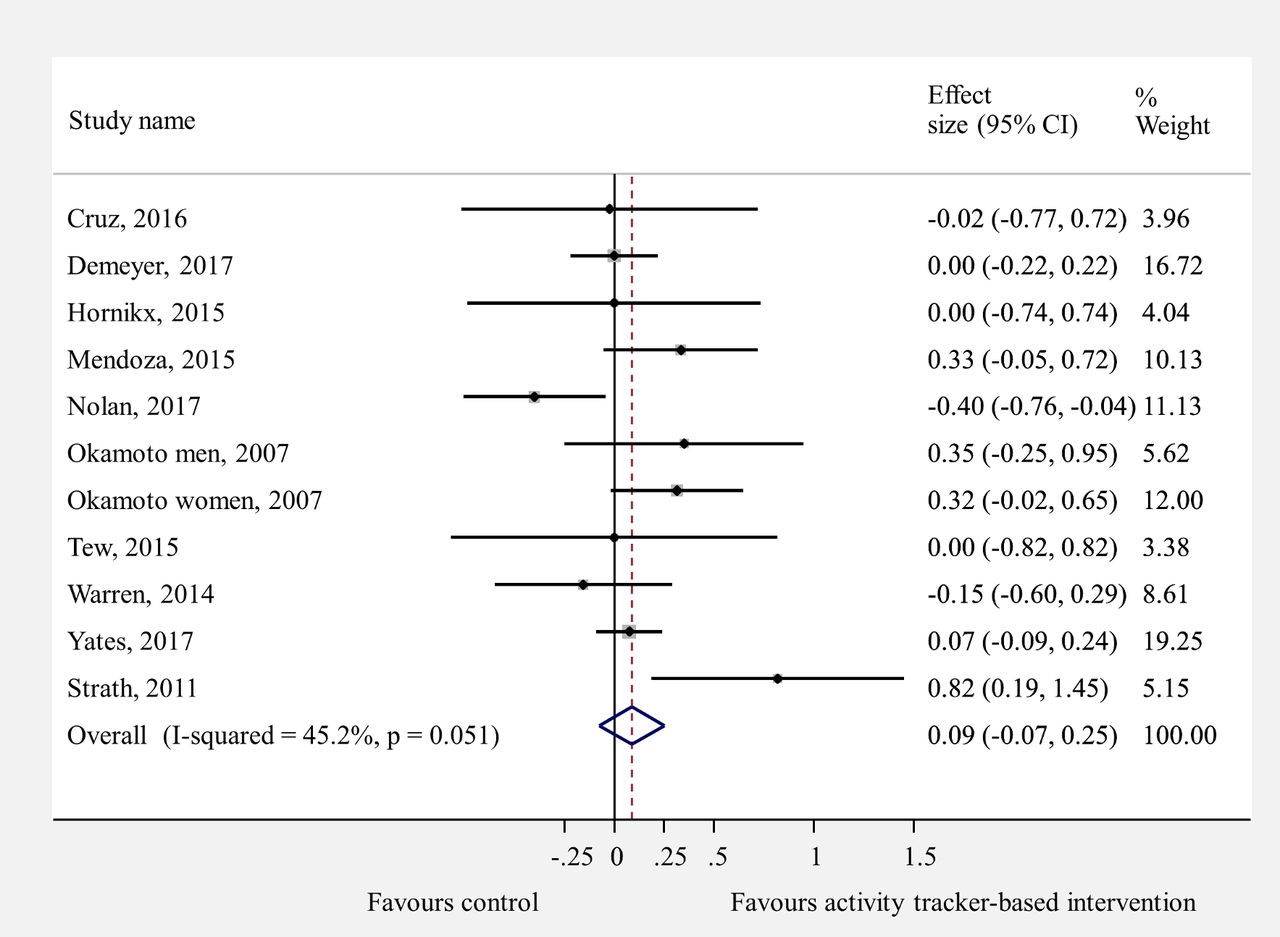
The meta-analysis of activity tracker-based interventions showed a medium effect of activity tracker use in improving mobility in intervention participants versus control participants (three studies; SMD=0.61; 95% CI 0.31 to 0.90; p=0.35, I2=10% (95% CI 0% to 87%), PI=−0.17 to 1.38; figure 4). We found no effect of interventions using activity trackers compared with control on quality of life (nine studies; SMD=0.09; 95% CI −0.07 to 0.3; p=0.051, I2=45% (95% CI 0% to 73%), PI=−0.34 to 0.51; figure 5). The quality of evidence (GRADE) for both pooling was rated as ‘moderate quality’ (see online supplementary appendix 6).

Effect size (95% CI) of interventions using activity trackers on mobility by pooling data from three studies comparing activity tracker use versus control using random-effects meta-analysis (n=218).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Effect size (95% CI) of interventions using activity trackers on quality of life by pooling data from nine studies comparing pedometer use versus control using random-effects meta-analysis (n=1436).
One trial49 reported the effect of interventions using activity trackers on mental health outcomes. Overall, participants allocated to the activity tracker intervention had similar effects on the anxiety (mean difference=−0.69; 95% CI −1.84 to 0.45; p=0.24) and depression (mean difference=−0.22; 95% CI −1.12 to 0.67; p=0.63) component score compared with control group.
Discussion
Principal findings
This systematic review and meta-analysis demonstrated that interventions using activity trackers may be effective in increasing physical activity among older people. Our meta-regression results demonstrate a similar impact of activity tracker-based interventions on physical activity levels in participants with clinical conditions and participants from the general population. We identified an indication towards the maintenance of the effects of activity tracker use at 6 months after intervention completion, but not at 3 months. However, the effect of activity tracker-based intervention over 12 months was not sustained over 12 months and 24 months. It is important to highlight that only one study reported long-term effects of activity tracker use and further research is needed. Additionally, the size of the intervention effect on physical activity was not influenced by the methodological quality, trial sample size and type of device used to measure steps per day. Our meta-regression results also found that greater effects on physical activity were seen from trials involving interventions of 12 or more weeks compared with interventions of less than 12 weeks.
Our results revealed that activity tracker interventions may increase the daily number of steps taken by over 1550 steps. The magnitude of these findings is comparable to another published meta-analysis of the impact of activity tracker use in adults, where the use of activity trackers was associated with significant improvements in physical activity by approximately 2500 steps per day.14
Furthermore, we found moderate evidence that interventions using activity trackers led to significant improvements in mobility outcomes. There is also moderate evidence of no effect of activity tracker-based interventions in improving quality of life among people aged 60 years and older. It is possible that increases in physical activity were not large enough to translate to improvements in overall quality of life, however further investigation in this area is needed. We also found no effect of activity tracker use on mental health outcomes. As only one included trial evaluated the impact of the interventions using activity trackers on this outcome, the mental health analysis was limited, and caution is recommended in interpreting this finding.
Strengths and limitations
This is the first systematic review and meta-analysis that provides an up-to-date summary of the impact of the activity tracker-based intervention on physical activity levels among people aged 60 years and over. We conducted this systematic review in accordance with PRISMA guidelines and followed a prespecified protocol registered on PROSPERO. To identify as many relevant studies as possible, we searched in eight different electronic databases, and we did not restrict our search by publication, language or date. Furthermore, the majority of the trials included were of relatively high methodological quality (mean PEDro Score of 6). Additionally, we included trials with a wide range of characteristics, including participants from the general population and participants with clinical conditions. Another strength of this review is the use of steps per day to measure physical activity levels. Although steps per day does not measure the frequency, duration and intensity of exercise, it is an objective, easy to use and accurate measure of physical activity that has strong associations with physical health variables.51 52
Despite these strengths, this review has certain limitations that can be addressed with future research. First, we were unable to make any significant comparison between interventions that used activity trackers and other interventions. Therefore, our results are limited to the comparison of activity tracker-based interventions and usual care or no intervention. Second, only one study reported data for ≥12 months; therefore, the longer-term sustainability of effects are unclear and warrant further investigation. Third, the asymmetrical funnel plot and Egger’s test revealed that the analysis might be affected by small study effects. However, it is worth emphasising that this was not supported by the pooled analysis based on the subgroup analysis that showed no significant effect of sample size on the effect size. Fourth, our data were limited to trials that included at least steps per day measured by pedometer or accelerometer as an outcome. Therefore, we may have missed relevant studies including measures of mobility, quality of life and mental health. Fifth, the meta-regression analysis found greater intervention effect estimates in studies including fewer than 100 participants (SMD=0.72; 95% CI 0.42 to 1.01) compared with studies including 100 or more participants (SMD=0.40; 95% CI 0.10 to 0.70). We acknowledge the tendency for small trials to report greater intervention benefits than large trials, and this may have influenced the magnitude of treatment effect. Finally, high statistical heterogeneity was present in the meta-analyses for physical activity, with I2 values from 86% to 92%, contributing to the pooled estimates.
Implications for clinicians and policymakers
Recently published physical activity guidelines9 showed that even small increases in older people’s routine physical activity can provide substantial benefits. Walking is an easy and accessible way of meeting physical activity recommendations—it is one of the preferred forms of physical activity for older people.53 Our findings support including activity trackers to increase physical activity levels in older people at a relatively low cost that could potentially be implemented at scale.
Unanswered questions
Our results identified evidence of the effect of interventions that use activity trackers on physical activity among older people. However, the long-term impact of this type of intervention is not clear. Therefore, studies that evaluate the long-term sustainability of physical activity behaviour in older people are needed. Our findings also point to the need for future studies to establish the ideal dose of interventions using activity trackers to produce improvements in quality of life and mental health.
Furthermore, research is warranted to explore the best way to optimise activity tracker-based interventions with the following suggested comparisons: (1) Interventions that use activity trackers including activity trackers that record only steps versus activity trackers with smartphone apps or motivational reminders. (2) Interventions that use activity trackers versus activity trackers in addition to physical activity counselling. (3) Activity tracker-based intervention versus another physical activity intervention.
What is already known?
Regular physical activity is among the most important lifestyle factors for maintaining physical function and health in older age.
There is clearly a need for effective strategies to increase physical activity participation in older age.
What are the new findings?
Activity trackers may be recommended as an effective approach to promote physical activity participation among healthy older people and those with clinical conditions. Longer duration activity tracker-based interventions are more effective than short duration interventions.
Activity tracker use also offers substantial promise for improving mobility outcomes.
The impact of interventions that use activity trackers on quality of life and mental health requires further investigation.
References
Footnotes
Contributors JSO, AT and CS conceived the study and JSO, AT, CS, MRF contributed to study design. JSO coordinated the literature search and data collection with assistance from ERYZ. JSO, AT, CS contributed to data analysis and interpretation of the data. JSO drafted the manuscript, and all authors contributed to revisions and approved the final manuscript. JSO is the guarantor for the study.
Funding JSO is supported by Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES), Brazil. CS and AT hold research fellowships from the National Health and Medical Research Council (NHMRC), Australia.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.