Article Text

Abstract
Background Despite the widespread use of periodic health evaluation (PHE) to detect and prevent injury and illness in athletes, its effectiveness in detecting health conditions and relevant risk factors is still debated.
Aim To assess health conditions detected by a comprehensive PHE in professional male football players and evaluate their consequences for participation clearance.
Methods A total of 558 professional football players in Qatar completed a PHE prior to the 2013 or 2014 seasons: history, general medical (including blood test), cardiovascular (12-lead ECG and echocardiography) and a musculoskeletal examination, including a specific test battery targeting lower extremity strength and flexibility. On the basis of the PHE, players were either cleared or not cleared for participation.
Results In 533 players (95.5%), at least one health condition was detected requiring treatment or follow-up. Vitamin D deficiency or insufficiency (≤30 ng/mL) was the most common medical condition (n=499, 89.4%), followed by hepatitis B non-immunity or infection (n=164, 29.4%). Cardiac screening identified 48 players (8.6%) with one or more abnormal findings (ECG (n=19, 3.4%) and echocardiography (n=14, 2.5%)). Musculoskeletal conditions were observed in 180 players (32.3%); injuries to or strength deficits of the hip/groin and thigh accounted for the largest proportion. Medical clearance was temporarily not given in 69 players (12.4%), while further examinations were being conducted. One player was disqualified from competitive football.
Conclusions PHE revealed a high prevalence of health conditions requiring treatment or follow-up in professional footballers; however, only 12.4% of conditions impacted on final clearance for participation.
- Prevention
- Football
- Health promotion
- Sports medicine
- Injury prevention
Statistics from Altmetric.com
Introduction
A periodic health evaluation (PHE) or health screening is widely used to identify potential risk factors for diseases or disorders early with the view of implementing targeted prevention measures to reduce future morbidity and mortality.1 Cancer screening (eg, breast and prostate) and PHE in work settings (eg, for hypertension, musculoskeletal disorders) represent integral elements of public health practice; however, evidence for their effect on total or cause-specific mortality is limited.2 ,3
Professional sport, including football, is well known for its high physical demands with high risk of injury, illness and also potentially negative long-term health consequences.4–6 Protection of the health of the athlete is therefore of utmost importance for sports authorities.7 ,8 In the sport setting, the PHE also serves the purpose of detecting and managing current health problems which may influence the ability to train and compete, as well as to determine whether an athlete is medically suitable to participate in competitive sport. Although the International Olympic Committee (IOC) released a consensus statement on the PHE of elite athletes in 2009, the extent and elements of the PHE vary widely between sport federations. It may vary from a short general health examination to a day-long comprehensive assessment that may include ECG and echocardiography, as well as an extensive general medical and musculoskeletal assessment.7 ,9–11
FIFA encourages all players to complete the FIFA Pre-Competition Medical Assessment (PCMA), which includes a comprehensive cardiovascular, general medical (including blood tests) and musculoskeletal assessment.7 Despite the debatable validity of ECG and echocardiography in detecting serious anomalies,12 ,13 cardiovascular screening with a 12-lead ECG and echocardiography is mandated for some FIFA and UEFA competitions.14 ,15 Most top-level football clubs worldwide complete a comprehensive precompetition musculoskeletal screening, including questionnaires, functional testing and isokinetic strength testing of the lower extremity.9 ,16 While a PHE is recommended by sports authorities such as FIFA and IOC,7 ,8 there is little scientific evidence of its effectiveness.17 ,18 Considerations such as cost (time and financial), possibilities of significant findings, and the impact of these are frequently discussed.8 ,19–21
The purpose of this study was therefore: (1) to assess the health conditions detected on a PHE in professional male football players and (2) to evaluate their consequences for participation clearance.
Methods
Participants and PHE procedure
All male football players eligible to compete in the Qatar Stars League (QSL) were asked to participate in this cross-sectional study. The players were recruited as they presented for their annual PHE at Aspetar Orthopaedic and Sports Medicine Hospital in Doha (Qatar), in the two preseason periods from July through September in 2013 and 2014. The QSL is the highest professional football league in Qatar (including 14 teams), with the majority of players coming from the Middle East and Central Africa. The PHE is part of the qualification procedure for all players expected to play in the QSL, and was divided into two stages performed on the same day.
Stage 1 consisted of a comprehensive history and clinical examination (general medical, cardiovascular and musculoskeletal examination). At stage 2, all test results collected during stage 1 were reviewed by a sport physician and medical clearance was determined. At inclusion, players provided written consent for their data being utilised for research. Refusal to consent or failure to complete key components (stage 2) of the PHE process resulted in exclusion from the study. Ethical approval was obtained from the Institutional Review Board, Anti-Doping Lab Qatar.
History and clinical examination
History and general medical examination was undertaken by a sports medicine nurse. History regarding injury and general medical, cardiovascular family history and personal symptoms was completed using the FIFA PCMA form.7 The general medical examination included a visual acuity assessment, measurements of height (m) and body mass (kg), and respiratory function testing (spirometry (forced expiratory volume, FEV, FEV1, peak expiratory flow, FEV1/forced vital capacity)). Physical examination of bilateral brachial artery blood pressure, heart rate and precordial auscultation in supine and standing positions was performed by an experienced sports medicine physician.22
Since the majority of football injuries are to the lower extremity, particularly hamstring and groin injuries,6 the identification of potential risk factors for these injuries was the primary focus of the comprehensive musculoskeletal test battery. The examination, performed by an experienced sports physiotherapist, included isokinetic muscle strength tests of knee flexors and extensors using an isokinetic dynamometer (Biodex Multi-joint System 3; Biodex Medical Systems Inc, New York, USA), strength, flexibility and pain provocation tests at the hip, groin and ankle, and a functional movement test (Nine-test screening battery; table 1).23–26 26a In addition to the musculoskeletal examination, all players underwent a general musculoskeletal examination by a sports physician using the FIFA PCMA clinical examination form7 at stage 2.
The comprehensive musculoskeletal examination and evaluation criteria for each test
Additional examinations
Additional examinations included laboratory blood tests, X-ray, ECG and echocardiography. Fasting blood samples and urine were sampled by a qualified phlebotomist and underwent immediate analysis (table 2). A chest X-ray was performed if clinically indicated.
Laboratory blood analyses performed in a PHE
A standard 12-lead ECG was obtained by a cardiac physiologist using a GE MAC 5500 (New York, USA) after a period of 5 min rest in the supine position. All ECGs were interpreted by an experienced sports cardiologist using the Seattle ECG criteria.27 Echocardiography was performed by an experienced sports cardiologist and according to protocols previously published for high-level athletes.28 All athletes completed both an ECG examination and an echocardiography as standard.
Athletes with symptoms, a family history of heart disease and/or sudden cardiac death (SCD), or echocardiographic and/or ECG abnormalities indicating possible cardiac pathology were investigated further as indicated (24 h ECG, maximal exercise testing and/or cardiac MRI).
Evaluation and clearance status
At the end of the PHE (stage 2), a sport physician evaluated all results and documented the clinical findings detected on a report form. The physician noted if there were any abnormalities. A diagnostic code (the Sport Medicine Diagnostic Coding System30) was assigned (if possible) to each player and recommended management recorded as free text. On the basis of the interpretation of the results, the sports physician determined whether to give the player medical clearance or to withhold it. Clearance was given if clinical findings were considered to have: no, mild or minimal risk for the player's future health. Clearance was temporarily withheld when clinical findings were considered as a moderate risk to the player's health (usually requiring further investigation or treatment). Permanently not cleared was reserved for a player diagnosed with a health condition considered unsafe for participation in competitive football. At the end of stage 2, the test results were discussed with the player and club doctor and the report form was given to the club medical staff.
Data management and analyses
The clinical findings documented on the report form formed the basis for the current analyses. A health condition was defined as any condition sufficient to require treatment, further investigation or recommendation to follow-up. Only health conditions requiring a follow-up as per the above definition were included for analysis.
History, clinical and report form data from the PHE were entered into a database in Excel (Microsoft Excel 2010 for Windows, Microsoft Office Professional Plus, V.14.0.7147.5001, California, USA) for analysis. In the case of abnormal cardiovascular findings, detailed information on ECG, echocardiography, clinical examination and results of follow-up tests were also entered.
On the basis of the physician's diagnosis and/or clinical findings on the report form, the general medical and musculoskeletal findings were classified post hoc by the researcher (AB) and head physician (ST) at Aspetar Screening Department into groups based on the IOC consensus statement on PHE of elite athletes and IOC injury and illness surveillance protocol for analysis.8 ,31 ,32 Haematology data were classified by the authors into two categories: iron deficiency (serum ferritin <30) with or without anaemia (haemoglobin lower than laboratory normal range) and other complete blood count alterations. We also grouped infection/immunology into hepatitis B and other infective immunology. Health conditions not fitting the categories were classified as ‘other’. The musculoskeletal findings were classified according to body part and type of condition, grouped as a current problem (injury or current physical symptom), abnormal finding on examination or positive history (previous injury or physical symptom reported on history taking).
Descriptive statistics are presented as mean values with SDs, unless otherwise noted. Frequencies are reported as absolute numbers with percentages.
Results
Participants
During the 2-year study period, 858 male professional elite football players attended the annual PHE (figure 1). In total, 22 players (2.6%) did not consent and were excluded. Five players (0.6%) were excluded for not completing stage 2. Of the 490 players screened in 2014, 273 had already been screened in 2013, and their repeat PHE was removed from the analysis. Thus, the final sample included 558 unique players (age 25.5±4.8 years; height: 177±7 cm; body mass: 72.3±9.2 kg; body mass index 23.0±2.0 kg/m2). The players were mainly of Arab (n=316, 56.6%), Black (n=155, 27.8%), Caucasian (n=33, 5.9%) and Persian (n=33, 5.9%) ethnic origins.

Flow chart showing the inclusion of participants during the 2-year study period.
Distribution of health conditions detected on PHE
In 533 players (95.5%), at least one health condition was detected that required further assessment, treatment or recommendation to follow-up. Of all players (n=558), 522 (93.5%) were identified with a general medical condition, 180 (32.3%) with a musculoskeletal condition and 48 (8.6%) with a cardiovascular condition. More than one-third of the players (n=205, 36.7%) were identified with two conditions from the three main domains, while 12 (2.1%) were identified with a condition in all three domains (figure 2).
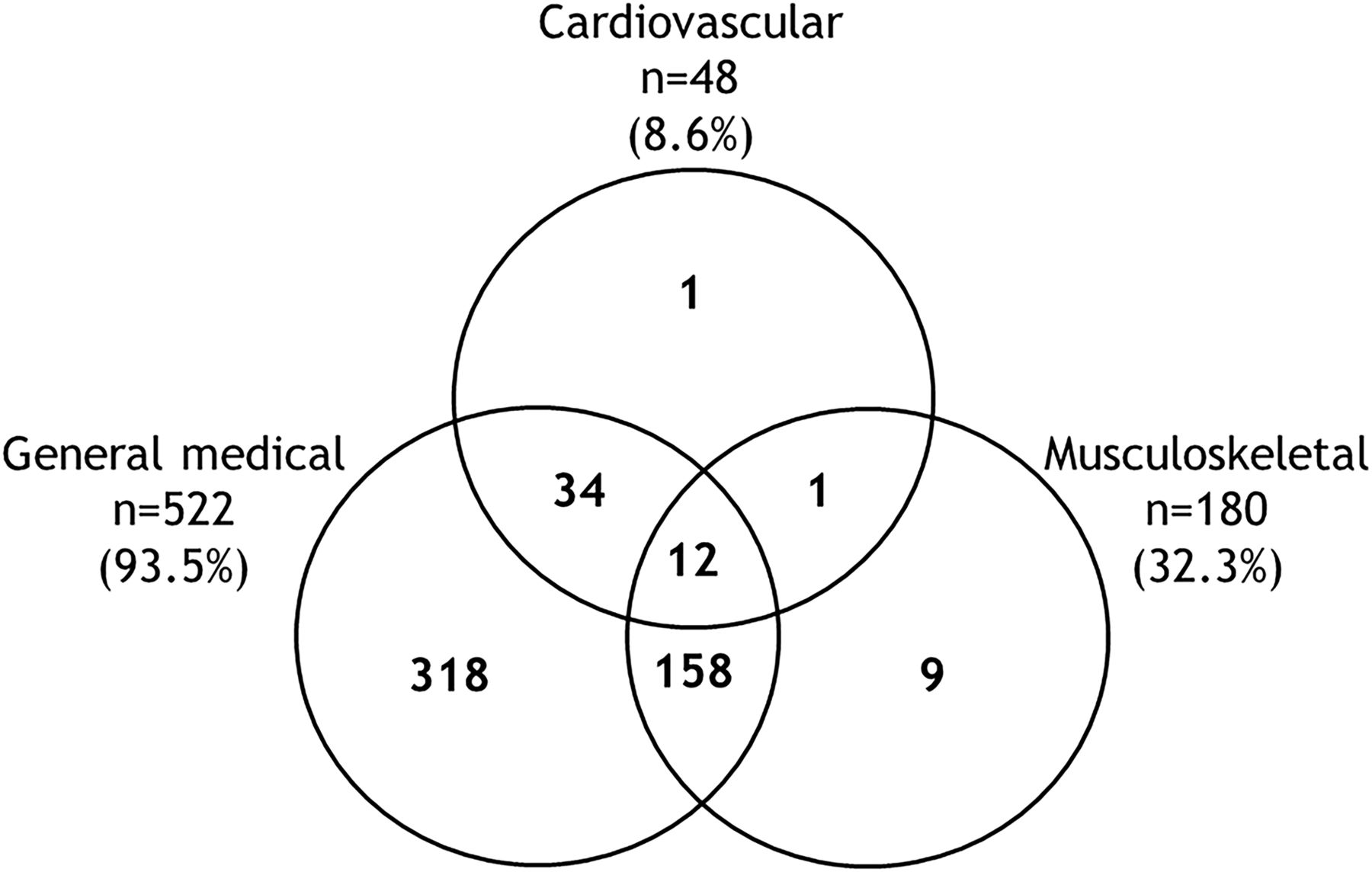
Venn diagram of players detected with one or more health conditions in the periodic health evaluation (PHE) (n=558).
Of all players identified with a health condition (n=533), a total of 1211 health conditions were reported. The total number of conditions for the three main screening components and the type of follow-up required are presented in table 3.
Health conditions detected and type of follow-up required for the 533 players detected with a health condition
General medical findings
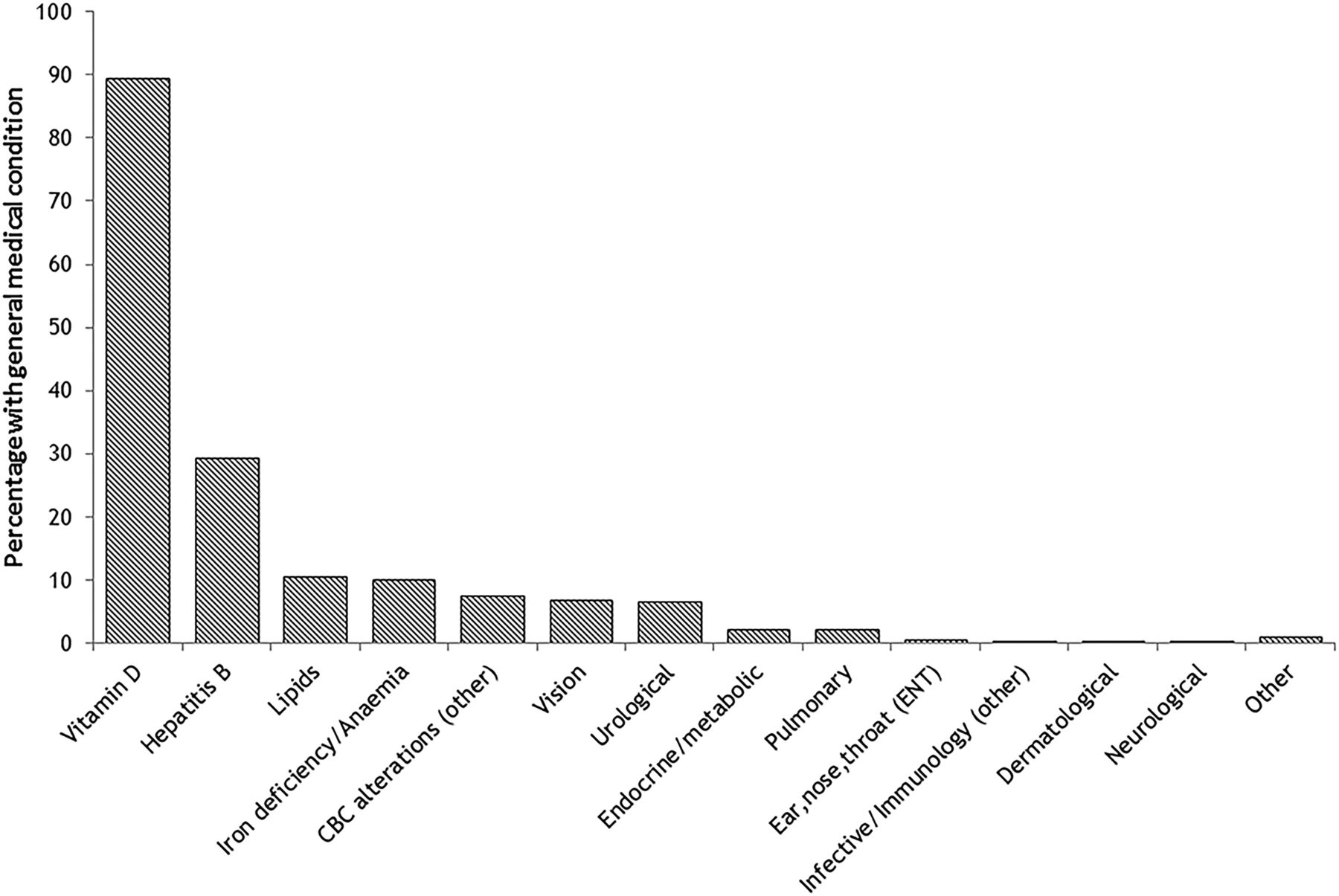
Vitamin D deficiency or insufficiency (≤30 ng/mL) was identified in 89.4% (n=499) of players and accounted for the majority of the medical conditions detected (figure 3). Hepatitis B non-immunity or infection was the second most frequent medical condition (29.4%, n=164), followed by dyslipidaemia (10.6%, n=59), iron deficiency/anaemia (10%, n=56), reduced visual acuity (6.5%, n=38) and abnormal urinalysis test results (blood, glucose or protein) (6.8% n=36).

Proportion of players with general medical conditions detected on a periodic health evaluation (PHE) (n=558). CBC, complete blood count.
In 74.8% of the medical conditions detected, treatment was required and initiated (tables 3 and 4). Further investigation was required in 8.9% of cases, and 8.2% required prevention recommendations (primarily dietary advice), while 8.0% of the conditions required repeat examinations.
Type of follow-up required for the general medical findings
Cardiovascular findings
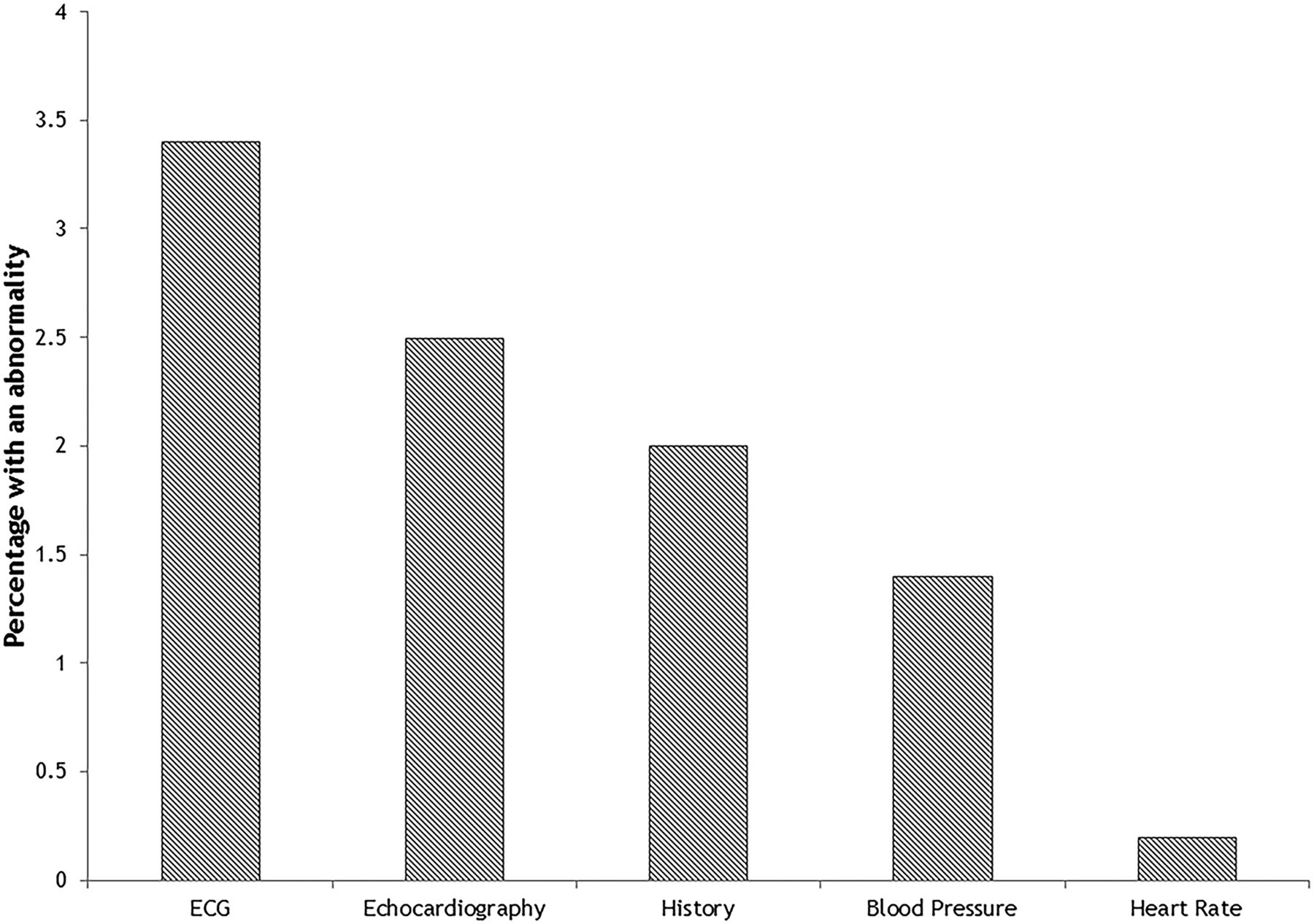
Among the 48 (8.6%) players presenting with one or more cardiovascular findings (table 3), 19 had ECG features associated with cardiac pathology, 14 had abnormal echocardiographic findings, 11 reported symptoms suggestive of cardiac disease (including dizziness and/or chest pain during exercise and/or syncope) and/or a family history of SCD in a first relative, while eight players presented with a resting blood pressure ≥140/90 mm Hg (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Proportion of players detected with an abnormality on cardiovascular screening (n=558).
The most common ECG anomalies were T-wave inversion (n=14), profound first-degree atrioventricular block (>300 ms) (n=2), prolonged QT interval (>490 m) (n=1), and profound sinus bradycardia (<30 bpm) (n=1), with information missing in one case. Echocardiographic abnormalities included reduced right ventricular free wall contractility (n=3), increased right ventricular dimensions above upper physiological limits (n=3), mitral valve prolapse (n=1), abnormal coronary artery origin (n=1), abnormal diastolic function (n=1), profound hypertrabeculation (n=1) and poor subcostal echo windows (n=4).
Almost all (n=51, 96.2%) cardiovascular anomalies required further investigation (table 3). Consequently, a total of 74 additional cardiovascular investigations were ordered. These included 28×exercise stress tests, 16×24 h Holter ECGs, 22×cardiac MRI with late gadolinium enhancement, 6×24 h Holter BP, 1×tilt test and 1×cardiac CT scan.
Musculoskeletal findings
Among the 180 players presenting with musculoskeletal conditions, 225 conditions were detected. Musculoskeletal conditions in the lower extremity accounted for 86.2% (table 5). Of the 225 conditions, 97 represented a current problem (injury or physical complaint), 113 an abnormal finding on musculoskeletal assessment (strength deficits, flexibility or decreased range of motion, (ROM)) but not limiting play or training, while 15 resulted from a self-reported injury history. The majority of the musculoskeletal conditions identified led to prevention recommendations (n=142, 63.1%); 68.3% of these were based on abnormal findings from the musculoskeletal assessment. Prevention recommendations consisted primarily of referral to the club physiotherapist for general prevention programmes (strength training, stretching). Conditions leading to further investigations (n=50, 22.2%) and treatment (n=31, 13.8%) were mostly due to current musculoskeletal problems (injury or ongoing physical symptom).
Musculoskeletal conditions detected related to body part and type of condition (n=558)
Medical clearance status
Immediate medical clearance was given in 481 (86.2%) players (table 6). In 8 cases (1.4%), clearance was temporary, waiting for test results (general medical, n=2; cardiovascular, n=1), pending completion of the specific musculoskeletal assessment (n=1) or pending ongoing rehabilitation for current injury (n=3), and due to cardiovascular findings suggestive but not diagnostic of apical hypertrophic cardiomyopathy, requiring a repeat examination after 6 months (n=1).
Medical clearance status for all players who underwent a PHE (n=558)
In 69 (12.4%) cases, medical clearance was temporarily not given while further investigations or treatment were being carried out. Following the further investigations, one player was disqualified from competitive football (abnormal coronary origin; table 6), whereas another player with a high suspicion of long QT syndrome was still not provided with medical clearance pending additional investigations. The player left the country before completing these. Thus, final clearance status could not be concluded. However, the player was advised against competitive football.
Discussion
The key finding from this study was that a targeted and comprehensive PHE identified at least one health condition requiring further assessment, treatment or recommendation to follow-up in 95.5% of professional football players. General medical and musculoskeletal components had the highest prevalence with 93.5% and 32.3%, respectively. The cardiovascular examination with ECG and echocardiography identified a cardiovascular condition in 8.6% of players. However, the vast majority of cases were given immediate medical clearance for competitive football (12.4% were temporarily not cleared).
General medical examination
In this study, general medical conditions represented more than 9 in 10 of the health conditions requiring treatment, further investigation or recommendations to follow-up. This was predominantly because of a high prevalence of vitamin D deficiency or insufficiency and hepatitis B non-immunity. Almost 90% of players were vitamin D deficient or insufficient. This is consistent with previous findings on Qatari athletes, including footballers,33 but much higher than those reported for athletes in western countries.34 Cultural clothing and training outside of sun hours in Qatar are believed to be the main cause in this population.
The potential role of vitamin D on performance, musculoskeletal health (injury risk, stress fractures), immune function and inflammatory response has increased the awareness of detecting athletes with deficiency upon treatment can be initiated.35 ,36 Oral supplementation was the most common treatment initiated. Supplementing athletes with vitamin D levels below 25 ng/mL may have improved athletic performance;37 however, whether or not to supplement is a topic of debate.38 ,39 A recent systematic review on athletes from different sport suggests that there is limited evidence for an association between low vitamin D levels and injury risk or performance.36 Also, there is currently no consensus on the optimal level of vitamin D for general health, sport-specific benefits or ethnicity.40 Thus, it is debatable at what level supplementation is beneficial.
Almost one-third of the players were treated (vaccination) for hepatitis B non-immunity. A previous study from our group has shown that the prevalence of hepatitis B among sportsmen in Qatar is markedly higher than that observed in Australian Rules footballers or sumo wrestlers.41 Our study population includes large groups originating from countries known not to have routine vaccination schedules41; regular screening for hepatic infection/immunity is therefore beneficial in our athlete population.
Of interest was the relatively high prevalence of dyslipidaemia (10.6%). This is in contrast to the findings of Meyer and Meister,42 who documented much lower rates among German professional football players. However, it supports the findings of Eliakim et al43 and Fallon,44 who found substantial levels of dyslipidaemia in a mixed-sport population. Similar to Eliakim et al,43 several players in our study had a family history of dyslipidaemia. In almost all cases, players were referred to a dietician or given dietary advice.
Contrary to expectations, there was a surprisingly low prevalence of respiratory symptoms (n=12, 2.2%) and gastrointestinal (GI) symptoms (0%) that required further investigations, treatment or recommendation for follow-up in this study. Airway hyper-responsiveness/asthma, respiratory infections and GI problems are common among elite athletes and are the most frequently affected system reported from elite sports events including the FIFA World Cup.32 ,45–47
The lack of cold air and minimal pollens in Qatar is believed to be one cause for the low prevalence. Another explanation for the low number may be that the lung function test in this study was performed only with a general spirometry test at rest along with the self-reported history. Lung function testing with bronchodilator reversibility and bronchoprovocation tests is required to detect bronchial hyper-responsiveness associated with training.46 These tests were not routinely performed in this study.
GI problems are more common in endurance athletes than in other athletes including football players.48 Also, the fact that a PHE is only a snapshot of the time and the limited in-depth questions about GI symptoms in the standard PCMA questionnaire may explain the lack of GI symptoms in this study.
Cardiovascular examination
ECG abnormalities gave reason for further testing in 19 players (3.2%), mostly due to T-wave inversion, and were the main reason for the cardiovascular abnormalities detected. None of the players with T-wave inversions showed any sign of cardiac pathology after additional testing. However, ECG revealed probable long QT syndrome in one player, who was advised against competitive football pending further investigations.
The discussion regarding routine inclusion of an ECG in the PHE of athletes is ongoing, with opposing recommendations from the USA and Europe.12 ,49 The concern is the ability of ECG to correctly differentiate physiological adaptation owing to sustained and intensive exercise from inherited or congenital cardiac pathology.27 Our prevalence of 3.2% of players with an ECG abnormality is lower than that reported by previous studies of footballers or athletes from various sports.50 ,51 In this study, the ECG results were interpreted according to the Seattle criteria, which have reduced the rate of abnormal ECG markedly.52–54
It is argued in the literature that the value of including echocardiography is limited.52 ,55 We found that echocardiography gave reason for additional testing in 14 players (2.5%) and resulted in a diagnosis of abnormal coronary artery origin in one player who presented with a normal ECG. The player was disqualified for competitive football due to elevated risk of SCD.
Musculoskeletal examination
Our targeted and comprehensive musculoskeletal test battery focusing on the lower extremities identified at least one musculoskeletal condition necessitating further investigation, treatment or recommendation for follow-up in more than 1 in 3 players.
Interestingly, we found that the hip/groin was the region most frequently affected, with 11% of the players identified with a hip/groin problem requiring follow-up. However, this may be a reflection of the screening programme, which included a series of tests targeting the groin (pain provocation tests and strength test).
More than one-third of the conditions were identified as a current injury or ongoing physical symptom, which led to further investigation or treatment and resulted in the athlete being temporarily not cleared to play. Given that previous injury and unresolved injuries represent the greatest risk factor for recurrent injury, it is important that these are identified.56 However, self-reported history of previous injury resulted in follow-up in only 15 cases. Most likely, this represents gross under-reporting of past injuries, given that data from injury surveillance of QSL players have reported that a player can expect at least one injury per season.5
Ideally, the PHE should also be used to identify athletes at risk for future injury. In this study, half (50.2%) of the musculoskeletal findings represented an abnormal test result, leading to prevention recommendations. However, the predictive value of the tests used is debatable.20 ,57 Lower adductor strength is identified as a risk factor for groin injuries, whereas there are low levels of evidence for the predictive value of testing isokinetic muscle strength, flexibility, ROM and functional movement tests.20 ,58 ,59
Considering these results, using a targeted physical examination based on careful history seems beneficial in detecting current injury and musculoskeletal problems. However, prospective studies are necessary to assess whether identifying such risk factors and acting on them reduces future injury risk.
To clear or not to clear?
In 86.2% of the players, the health conditions did not restrict the athlete from competitive sport, suggesting that most were interpreted as not being severe. However, they may be significant from the point of view of the athlete. By identifying these conditions, treatment and prevention strategies can be initiated to potentially prevent future health/injury risk.8 The purpose of a PHE is to ensure safe participation for the player, but at the same time not to disqualify athletes unless there is an evidence-based medical reason.60 For the 12.4% of players not given immediate clearance, the delay was caused by the need for further investigations, with suspected cardiovascular conditions as the main reason. However, after follow-up investigations, only one player (abnormal coronary artery) was permanently disqualified, whereas one player (possible long QT syndrome) was advised against competitive football.
Methodological considerations
The strength of the present study was that it was undertaken in one sports medicine hospital with a large group of male football players. This allowed for development of a PHE targeting history and examination characteristics thought to be relevant for the population and sport in question.44
A further strength of our study is that several sports medicine physicians performed the stage 2 assessment. This provides good generalisability, but also adds uncertainty to the reliability of the evaluation of findings and conditions identified. We only included health conditions requiring further investigation, treatment or recommendations for follow-up. This may have been subjective, depending on the physician's experience or field of expertise. Also, we evaluated each athlete's PHE as a separate encounter, even if the player had performed a PHE during the preceding seasons. We do not know how this may have influenced the physician's interpretation of the results.
It should be noted that, in contrast to cardiovascular conditions, there is limited evidence to help clearly define what constitutes a significant general and musculoskeletal finding. In our study, this was a decision based on the interpretation of the physician, most likely representing a source of inconsistency. We also acknowledge that as our study included a homogeneous group of male professional football players in a specific setting, this limits the generalisability of the findings to other sports, settings, age groups and women. Furthermore, the relatively small numbers of players in ethnic groups other than Arabic and black means that the results may not be relevant to other populations.
Positive findings can only be found in tests that are conducted. We recognise that the relative prevalence described here is in part an artefact of the screening battery chosen. We suggest that this is reflective of clinical practice; however, more work needs to be carried out to establish its veracity through prediction of injury and illness events. For PHE to be effective, however, the characteristics of the population and sport in question should be taken into consideration.44 The PHE in this study used the standardised PCMA based on knowledge of our populations. For example, vitamin D deficiency and hepatitis B are known to be prevalent in our population from previous studies.33 ,41 Although the health conditions detected in this study may not be prevalent in other sport settings/groups, we believe that the elements used in our PHE are beneficial to other sport settings in the frame that each sport setting knows the characteristics of their population.
Finally, a major limitation to this study is the cross-sectional design, which does not allow us to infer the predictive value of the conditions detected on future health risk. Prospective studies are warranted to address this question. Also, considering the high prevalence of conditions requiring follow-up, longitudinal follow-up studies are required to examine the usefulness of interventions.
Conclusion
This study demonstrated that a targeted PHE in professional Qatari football players is beneficial in detecting current health conditions for which treatment, investigation or prevention management can be instigated. However, the clinical relevance and benefits on future health are still unclear.
What are the findings
A targeted periodic health evaluation (PHE) of professional football players revealed a high prevalence of current health conditions that required clinical consideration.
Management of health conditions ranged from reassurance, treatment, further investigations or recommendations to follow-up.
General medical and musculoskeletal conditions were the most prevalent.
Delayed clearance was mainly due to abnormalities on the cardiovascular examination and current musculoskeletal injuries.
Disqualification for competitive football was extremely rare in our group.
How might it impact on clinical practice in the future?
The current study documents that a PHE targeted at the characteristics of the population and sport in question detects a number of conditions (musculoskeletal, cardiovascular and medical), which are believed to be relevant for health and performance.
However, whether many of these conditions (such as vitamin D levels below 30 ng/mL) confer future health risk is not known. Prospective studies are needed to determine the benefits of screening (and subsequent targeted interventions) for each of the components of the PHE.
Acknowledgments
The authors would like to sincerely thank all staff at the Aspetar Athlete Screening Department, the Rehabilitation Department and the Qatar National Sports Medicine Programme (NSMP) for their contribution to the study.
References
Footnotes
Twitter Follow Arnhild Bakken at @phbakken and Maria-Carmen Adamuz at @AdamuzC
Contributors AB designed the study, contributed in data collection, analysed and interpreted the data, and drafted the article. RB and KMK designed the study, interpreted the data, revised the article and approved the final revision of the article. ST, M-CA and MGW contributed to quality control and interpretation of the medical data, and revision of the manuscript. TB, JLT, RW and EW contributed to the final paper.
Competing interests KMK is Editor in Chief of BJSM and was at arm’s length (and blinded) from the review process in BJSM.
Ethics approval The study has been reviewed and approved by the Institutional Review Board, Anti-Doping Lab Qatar (ADLQ), Doha, Qatar.
Provenance and peer review Not commissioned; externally peer reviewed.