Article Text

Abstract
Background/aim To investigate the role of eccentric knee flexor strength, between-limb imbalance and biceps femoris long head (BFlh) fascicle length on the risk of future hamstring strain injury (HSI).
Methods Elite soccer players (n=152) from eight different teams participated. Eccentric knee flexor strength during the Nordic hamstring exercise and BFlh fascicle length were assessed at the beginning of preseason. The occurrences of HSIs following this were recorded by the team medical staff. Relative risk (RR) was determined for univariate data, and logistic regression was employed for multivariate data.
Results Twenty seven new HSIs were reported. Eccentric knee flexor strength below 337 N (RR=4.4; 95% CI 1.1 to 17.5) and possessing BFlh fascicles shorter than 10.56 cm (RR=4.1; 95% CI 1.9 to 8.7) significantly increased the risk of a HSI. Multivariate logistic regression revealed significant effects when combinations of age, history of HSI, eccentric knee flexor strength and BFlh fascicle length were explored. From these analyses the likelihood of a future HSI in older athletes or those with a HSI history was reduced if high levels of eccentric knee flexor strength and longer BFlh fascicles were present.
Conclusions The presence of short BFlh fascicles and low levels of eccentric knee flexor strength in elite soccer players increases the risk of future HSI. The greater risk of a future HSI in older players or those with a previous HSI is reduced when they have longer BFlh fascicles and high levels of eccentric strength.
- Prospective
- Muscle injury
Statistics from Altmetric.com
Introduction
Hamstring strain injuries (HSI) are the most prevalent cause of lost playing and training time in elite soccer and account for approximately 37% of all muscle strain injuries.1–3 Of these HSIs the majority occur in the biceps femoris long head (BFlh).1–3 Despite a concerted scientific effort over the past decade, the incidence of HSIs has not declined in elite soccer.4 What is known is that a number of non-modifiable risk factors, including increasing age and injury history, have been shown to increase the risk of a future HSI in elite soccer.5–7 Recently greater attention has been directed to modifiable risk factors that can be altered via a range of interventions.8–10 These risk factors include isokinetically derived eccentric knee flexor strength10 and muscle imbalances (between-limb and hamstring:quadriceps ratios).10 ,11
In addition a recent prospective cohort study in elite Australian Rules Football identified eccentric weakness during the Nordic hamstring exercise as risk factor for a future HSI.9 This study also showed that there was a decreased risk of sustaining a future HSI in older athletes and those with a prior HSI if coupled with high levels of eccentric knee flexor strength.9 Despite this evidence, there is still no consensus regarding the role that eccentric knee flexor strength plays in the aetiology of a HSI in soccer and this warrants further attention.12
Despite a lack of direct evidence, it has been proposed that hamstring muscle fascicle length may alter the risk for a future HSI.13–15 One retrospective study has shown BFlh fascicles are shorter in previously injured muscles than in the contralateral uninjured muscles,16 but due to the retrospective nature of the available evidence,16 it is not possible to determine if these differences in fascicle length increased the risk of a HSI occurring or were the result of the initial insult.
The purposes of this study were to determine if eccentric knee flexor strength and between-limb imbalances during the Nordic hamstring exercise and BFlh fascicle length influenced the risk of a future HSI in elite Australian soccer players. Additionally, this study aimed to assess the interrelationship between these two modifiable factors (fascicle length and eccentric strength) and the non-modifiable risk factors of increasing age and previous HSI in determining the risk of a future HSI. It was hypothesised that shorter BFlh fascicles, low levels of eccentric knee flexor strength and larger between-limb imbalances would be associated with an increased risk of HSI. The interaction between increasing age and a HSI history with eccentric strength and BFlh fascicle length will provide novel information for an athlete's risk profile.
Methods
Participants and study design
This prospective cohort study was completed during the preseason (June 2014–July 2014) and in-season period (October 2014–May 2015) of the 2014/2015 elite, professional Australian Football (soccer) competition. Ethical approval for the study was granted by the Australian Catholic University Human Research Ethics Committee (approval number: 2014 26V). Eight of the ten invited teams elected to take part in the study. Recent staffing changes resulted in two teams deciding not to participate. All outfield members of the playing squad (18–22 athletes per team) were approached and provided written, informed consent. In total, 152 elite male football (soccer) players participated in this study. Club medical staff completed a retrospective injury questionnaire that detailed each athlete's history of hamstring, quadriceps, groin and calf strain injuries and chronic groin pain in the past 12 months, as well as the history of ACL injury at any stage throughout the athlete's career. Playing positions were defined as: defender (n=52), midfielder (n=59) and attacker (n=41) as per previous research.17 The athletes had their maximal voluntary isometric contraction strength (n=141) (MVIC), BFlh architecture (with relaxed hamstrings (n=152) and while performing isometric knee flexion at 25% of MVIC (n=141)) and eccentric knee flexor strength (n=131) assessed at the beginning of preseason. Some athletes did not complete the maximal eccentric and isometric strength assessments at the advice of their team's medical department.
BFlh architecture assessment
Muscle thickness, pennation angle and fascicle length of the BFlh was determined from ultrasound images taken along the longitudinal axis of the muscle belly utilising a two dimensional, B-mode ultrasound (frequency, 12 MHz; depth, 8 cm; field of view, 14×47 mm) (GE Healthcare Vivid-i, Wauwatosa, USA). The scanning site was determined as the halfway point between the ischial tuberosity and the knee joint fold, along the line of the BFlh. All architectural assessments were performed with participants in a prone position and the hip neutral following at least 5 min of inactivity. Assessments at rest were always performed first followed by an isometric contraction protocol. During all assessments of the BFlh architectural characteristics (passive and 25% of MVIC), the knee joint was fully extended. Assessment of the MVIC of the knee flexors was undertaken in the same position and was performed in a custom made device.18 ,19 Participants were instructed to contract their knee flexors maximally over a 5 s period. The peak force value during this effort was used to determine their MVIC strength. The assessment of the BFlh architectural characteristics during a 25% isometric contraction then occurred in the same position and device, with the participants shown the real-time visual feedback of the force produced to ensure that target contraction intensities were met. To gather ultrasound images, the linear array ultrasound probe, with a layer of conductive gel was placed on the skin over the scanning site, aligned longitudinally and perpendicular to the posterior thigh. Care was taken to ensure minimal pressure was placed on the skin by the probe as this may influence the accuracy of the measures.20 Finally, the orientation of the probe was manipulated slightly by the sonographer (RGT) in order to optimise fascicle identification. Ultrasound image analysis was undertaken off-line (MicroDicom, V.0.7.8, Bulgaria). For each image, six points were digitised as described by Blazevich et al.21 Following the digitising process, muscle thickness was defined as the distance between the superficial and intermediate aponeuroses of BFlh. A fascicle of interest, which was the clearest and could be seen across the entire field of view, was outlined and marked on the image. The angle between this fascicle and the intermediate aponeurosis was measured and given as the pennation angle. The aponeurosis angle for both aponeuroses was determined as the angle between the line marked as the aponeurosis and an intersecting horizontal reference line across the captured image.21 ,22 Fascicle length was determined as the length of the outlined fascicle between aponeuroses. As the entire fascicle was not visible in the field of view of the probe it was estimated via the following equation from Blazevich and colleagues:21 ,22
where FL, fascicle length; AA, aponeurosis angle; MT, muscle thickness; PA, pennation angle. Fascicle length was reported in absolute terms (cm) and relative to BFlh length. The same assessor (RGT) collected and analysed all scans and was blinded to participant identifiers during the analysis. Reliability of the assessor (RGT) and processes used for the determination of the BFlh architectural characteristics have been reported previously.16
Eccentric hamstring strength
The assessment of eccentric knee flexor strength using the Nordic hamstring device has been reported previously.9 ,16 ,18 ,19 Participants were positioned in a kneeling position over a padded board, with the ankles secured superior to the lateral malleolus by individual ankle braces that were secured atop custom made uniaxial load cells (Delphi Force Measurement, Gold Coast, Australia) fitted with wireless data acquisition capabilities (Mantracourt, Devon, UK). The ankle braces and load cells were secured to a pivot that ensured that force was always measured through the long axis of the load cells. Following a warm up set of three submaximal efforts with a subsequent 1 min rest period, participants were asked to perform one set of three, maximal bilateral repetitions of the Nordic hamstring exercise. Participants were instructed to gradually lean forward at the slowest possible speed while maximally resisting this movement with both lower limbs while keeping the trunk and hips in a neutral position throughout, and the hands held across the chest. Verbal encouragement was given throughout the range of motion to ensure maximal effort.
Prospective HSI reporting
A HSI was defined as any acute posterior thigh pain that resulted in the immediate cessation of exercise and was later diagnosed by the club medical staff. The injury diagnosis also included the presence of pain during an isometric contraction and during any knee flexor muscle length test (stretch). Injury reports were not completed for injuries that did not fulfil the criteria (eg, acute posterior thigh pain, however, completed the session/match). A recurrent injury was a HSI that occurred on the same side of the body that had already suffered an injury in the current season. For all recurrent and new HSIs that fit the above criteria, the club medical staff completed a standard injury report form that detailed which limb was injured (dominant/non dominant, left/right), the muscle injured (BFlh/biceps femoris short head/semimembranosus/semitendinosus), location of injury (proximal/distal, muscle belly/muscle-tendon junction), activity type performed at time of injury (eg, running, kicking etc), grade of injury (I, II or III)23 ,24 and the number of days taken to return to full participation in training/competition. These reports were forwarded to the investigators throughout the season.
Injury specifics and rates
The determination of playing time missed as a result of a HSI was measured as missed matches per club per season.25 Recurrence rate was defined as the number of recurrent injuries in the same season as a percentage of new injuries.25 Additionally time lost as a result of the injury was defined as the amount of days from when the injury occurred to the resumption of full training participation.
Data analysis
While positioned in the custom made device, shank length (m) was determined as the distance from the lateral tibial condyle to the mid-point of the brace that was placed around the ankle. This measure of shank length was used to convert the force measurements (collected in N) to torque (Nm). Knee flexor eccentric and MVIC force data were transferred to a personal computer at 100 Hz through a wireless USB base station (Mantracourt, Devon, UK). The peak force value during the MVIC and the three Nordic hamstring exercise repetitions for each of the limbs (left and right) were analysed using custom made software. Eccentric knee flexor strength, reported in absolute terms (N and Nm) and relative to body mass (N/kg and Nm/kg), was determined as the average of the peak forces from the three repetitions for each limb, resulting in a left and right limb measure.18 Knee flexor MVIC strength, reported in absolute terms (N and Nm) and relative to body mass (N/kg and Nm/kg), was determined as the peak force produced during a 5 s maximal effort for each limb.
Between limb imbalance of BFlh fascicle length, muscle thickness, eccentric and MVIC knee flexor strength was calculated as a left:right limb ratio for the uninjured players and as an uninjured:injured limb ratio in the injured players. As recommended, between limbs imbalance was converted to a percentage difference using log transformed raw data followed by back transformation.26 Negative percentage imbalances indicate that the variable of the left limb was greater than the right limb in the uninjured players, or that the injured limb was variable was greater than the uninjured limb in the injured players. For athletes who did not suffer a HSI, as the limbs did not differ for any variables (p>0.05) the left and right limb were averaged to give a single control ‘score’.
Statistical analyses
All statistical analyses were performed using JMP V.11.01 Pro Statistical Discovery Software (SAS Inc., Cary, North Carolina, USA). Where appropriate, data were screened for normal distribution using the Shapiro-Wilk test and homoscedasticity using Levene's test.
The mean and SD of age, height, weight, BFlh fascicle length (passive and 25% MVIC), BFlh muscle thickness (passive and 25% MVIC), eccentric and MVIC knee flexor strength were determined for all participants. Univariate analyses were performed to compare between limb differences for all variables of the injured and uninjured groups, as well as comparing the injured limb to the contralateral uninjured limb and the average of the left and right limbs from the uninjured group. Univariate comparisons were undertaken using two-tailed t-tests with Bonferonni corrections to account for multiple comparisons. To determine univariate relative risk (RR) and 95% CIs of future HSI, athletes were grouped according to:
Those with or without prior
Hamstring injury (past 12 months)
Calf injury (past 12 months)
Quadriceps injury (past 12 months)
ACL injury (at any stage in their career)
Chronic groin injury (past 12 months)
Those with passive fascicle lengths above or below
10.56 cm
This threshold was determined utilising receiver operator characteristic (ROC) curves based on the fascicle length threshold that maximised the difference between sensitivity and 1-specificity.
Those with 25% MVIC fascicle lengths above or below
9.61 cm
Threshold determined as above
Those with passive muscle thickness above or below
2.35 cm
Threshold determined as above
Those with 25% MVIC muscle thickness above or below
2.61 cm
Threshold determined as above
Those with average eccentric knee flexor strength above or below
337 N
Threshold determined as above
Those with MVIC knee flexor strength above or below
400 N
Threshold determined as above
Those with limbs above or below arbitrarily selected cut offs of 10%, 15% and 20% between limb imbalance for
passive fascicle length
25% MVIC fascicle length
Average eccentric knee flexor strength
MVIC knee flexor strength
Athletes above these age cut offs (which represent the 10th, 25th, 50th, 75th and 90th centiles for this sample)
18.0 years
20.4 years
23.7 years
28.8 years
32.6 years
Athletes above and below the height (182.3 cm) and weight (77.9 kg) means as defined previously by Hägglund et al.27
HSI rates from these groups were then compared and RR calculated utilising a two-tailed Fisher's exact test to determine significance. Additionally, univariate logistic regressions were conducted with the prospective occurrence of a HSI (yes/no) as the dichotomous dependant variable and eccentric knee flexor strength and BFlh fascicle length as continuous independent variables in separate analyses. These data are reported as ORs and 95% CI per 10 N increase in knee flexor force and 0.5 cm increase in fascicle length.
As per a previous investigation in elite Australian Football,9 to improve the understanding of the risk from the univariate analysis and remove the possible confounding effects, multivariate logistic regression models were built using risk factors from previously published evidence.1–3 ,5 ,9 The first model included passive fascicle length (average of both limbs) and history of HSI and their interaction. The second model included fascicle length (average of both limbs) and age and their interaction. The third model included mean eccentric strength (average of both limbs) and history of HSI and their interaction. The fourth model included mean eccentric strength (average of both limbs) and age and their interaction. The final model included fascicle length (average of both limbs) and mean eccentric strength (average of both limbs) and their interaction. Additionally for this final model the Nagelkerke R2 coefficient28 was used to display the strength of the association between the two continuous independent variables (eccentric strength and fascicle length) with a prospective HSI occurrence. Significance was set at a p<0.05 and where possible Cohen's d29 was reported for the effect size of the comparisons, with the levels of effect being deemed small (d=0.20), medium (d=0.50) or large (d=0.80) as recommended by Cohen (1988).
Results
Power calculations
Power analysis was undertaken post hoc using G-Power. Using BFlh architecture data, power was calculated as 0.97 for the use of two-tailed independent t tests to compare groups (input parameters: effect size=0.80; α=0.05; sample size group 1=125; sample size group 2=27). Using a similar post hoc comparison for eccentric knee flexor strength, power was calculated as 0.95 (input parameters: effect size=0.80; α=0.05; sample size group 1=105; sample size group 2=26).
Participant and injury details
One-hundred and fifty-two athletes were assessed at the beginning of preseason (age 24.8±5.1 years; height 1.80±0.06 m; body mass 76.9±7.5 kg). One hundred and twenty-five did not sustain a HSI (age 24.2±5.1 years; height 1.78±0.06 m; body mass 75.3±6.6 kg) and 27 did (age 27.0±3.8 years; height 1.80±0.07 m; body mass 76.4±6.7 kg). The athletes who went on to be injured displayed no differences in height and weight, but were significantly older than those who did not suffer an injury (mean difference: 2.8 years; 95% CI 1.1 to 4.5; p=0.002; d=0.62). Twenty-seven initial HSIs were sustained (11 left limb, 16 right limb) and of these, eight went on to reoccur in the same season (recurrence rate=29.6%). Of the initial injuries, 10 occurred during the preseason period, with the remaining 17 occurring during the competitive season. The total amount of matches missed as a result of a HSI (initial and recurrent) was 63, resulting in 7.8 matches missed per club for the competitive season. Of the 27 initial injuries, the average time lost was 17.7 (±9.3) days, with the eight recurrent injuries resulting in an average of 28.4 (±23.7) days.
Of the twenty-seven initial HSIs, 88.8% occurred in the BFlh, with the remaining 11.2% occurring in the semimembranosus (7.5%) and semitendinosus (3.7%), respectively. The primary mechanism for the initial injuries was high-speed running (81.5%), followed by stretching for a ball or opponent (11.1%) and then kicking (7.4%). All recurrences occurred during high-speed running. No injuries occurred during the Nordic hamstring exercise testing sessions. The distribution of player positions in the injured group (defender: 29.6%, midfielder: 37.1%, attacker: 33.3%) compared to the uninjured group (defender: 36.8%, midfielder: 40.0%, attacker: 23.2%) suggested that defenders were under-represented and attackers over-represented in the subsequently injured group.
Univariate analysis
Eccentric and isometric knee flexor strength, BFlh architectural characteristics and between limb asymmetries of the injured and uninjured limbs from the injured players and the average of both limbs from the uninjured players can be found in table 1.
Preseason BFlh architectural characteristics (n=152), eccentric knee flexor strength during the Nordic hamstring exercise (n=131) and MVIC knee flexor strength (n=141) in elite Australian soccer players
BFlh architectural characteristics
The subsequently injured limbs had shorter BFlh fascicles than the two-limb-average of the uninjured players when assessed at rest (mean difference: 1.37 cm; 95% CI 0.8 to 1.8; p=<0.001; d=1.08; table 1) and during 25% MVIC (mean difference: 1.02 cm; 95% CI 0.5 to 1.5; p=<0.001; d=0.92; table 1). In comparison to the contralateral uninjured limb, the BFlh fascicles of the subsequently injured limbs was significantly shorter when assessed at rest (mean difference: 1.05 cm; 95% CI 0.6 to 1.5; p=<0.001; d=0.91; table 1) and during 25% MVIC (mean difference: 0.65 cm; 95% CI 0.3 to 1.0; p=<0.001; d=0.57; table 1). Whereas, the BFlh architectural characteristics of the left and right limbs in the uninjured players were not significantly different when assessed in a relaxed state or during 25% MVICs (p>0.05).
Using univariate logistic regression, BFlh fascicles (OR=0.261; 95% CI 0.10 to 0.57; p=0.002) had a significant inverse relationship with the incidence of prospectively occurring HSIs. For every 0.5 cm increase in BFlh fascicle length, the risk of HSI was reduced by 73.9%. Muscle thickness measures of the BFlh (at rest and during 25% MVIC) from the subsequently injured limbs were no different from either the contralateral uninjured limbs or the two-limb-average of the uninjured players (p<0.05, d range=0.13–0.23; table 1).
The measures of between limb asymmetry in BFlh fascicle length and muscle thickness, assessed at rest and at 25% MVIC, did not differ significantly between the injured and uninjured players (p<0.05, d range=0.03–0.48; table 1).
Eccentric and isometric knee flexor strength
Between-limb differences in absolute eccentric knee flexor forces in the left and right limbs of uninjured players and between the subsequently injured and contralateral uninjured limbs of injured players, were not significant (p>0.05, d range=0.02–0.21; table 1). However, between group comparisons of absolute eccentric knee flexor force showed that subsequently injured limbs were weaker (260.6 N±82.9) than the two-limb-average of uninjured players (309.5 N±73.4) (mean difference: 48.9 N; 15.8%; 95% CI 16.2 to 81.5 N; p=0.004; d=0.62; table 1). Additionally, the uninjured limbs of the injured players were also significantly weaker (262.6 N±63.2) than the uninjured players’ two-limb-average (mean difference: 46.9 N; 15.1%; 95% CI 15.9 to 77.9 N; p=0.003; d=0.68; table 1).
Eccentric strength represented as knee flexor torque showed similar differences, with the subsequently injured limbs (115.2 Nm±37.1) being weaker than the two-limb-average (135.5 Nm±33.7) of uninjured players (mean difference: 20.3 Nm; 14.9%; 95% CI 5.3 to 35.1 Nm; p=0.008; d=0.57; table 1). Similarly, the uninjured limbs (116.2 Nm±28.7) from the injured players were weaker than the two-limb-average of the uninjured players (135.5 Nm±33.7; mean difference: 19.3 Nm; 14.2%; 95% CI 4.9 to 33.4 Nm; p=0.008; d=0.62; table 1).
Using univariate logistic regression, eccentric knee flexor strength (OR=0.910; 95% CI 0.85 to 0.97; p=0.004) had a significant inverse relationship with the incidence of prospectively occurring HSIs. For every 10 N increase in eccentric knee flexor strength, the risk of HSI was reduced by 8.9%. Comparisons of between-limb imbalance in eccentric knee flexor strength did not differ between the subsequently injured and uninjured players (mean difference: 9.6%; 95% CI −3.6 to 22.7; p=0.147; d=0.40; table 1).
There were no significant differences in knee flexor MVIC strength between either the subsequently injured limbs or the contralateral uninjured limbs of the injured players and the two-limb-averages of uninjured players (p>0.05; d range=0.07–0.22; table 1).
Relative risk
The univariate RRs of a future HSI associated with all variables examined can be found in table 2. Athletes with a relaxed BFlh fascicle length shorter than that of the ROC-curve-determined threshold of 10.56 cm (area under the curve=0.71; sensitivity=0.70; 1-specificity=0.29) were 4.1 times more likely to suffer a subsequent HSI than those with longer fascicles (RR=4.1; 95% CI 1.9 to 8.7; p<0.001). Similar RR values were seen for BFlh fascicle length assessed during 25% MVIC (table 2). Furthermore, athletes with average eccentric knee flexor forces below the ROC-curve determined threshold of 337 N (area under the curve=0.65; sensitivity=0.96; 1-specificity=0.68) had 4.4 times greater risk of a subsequent HSI than stronger players (RR=4.4; 95% CI 1.1 to 17.6; p=0.013). Similar RR values were seen for the other measures of knee flexor strength (torque, force/kg body mass and torque/kg body mass) (table 2). No measure of MVIC strength or between-limb imbalance in this measure led to a statistically significant increase in RR (table 2).
Univariate RR to sustain a future HSI using BFlh fascicle length, muscle thickness, eccentric strength, MVIC strength, between-limb imbalances of these variables, previous injury history and demographic data as risk factors
Multivariate logistic regression
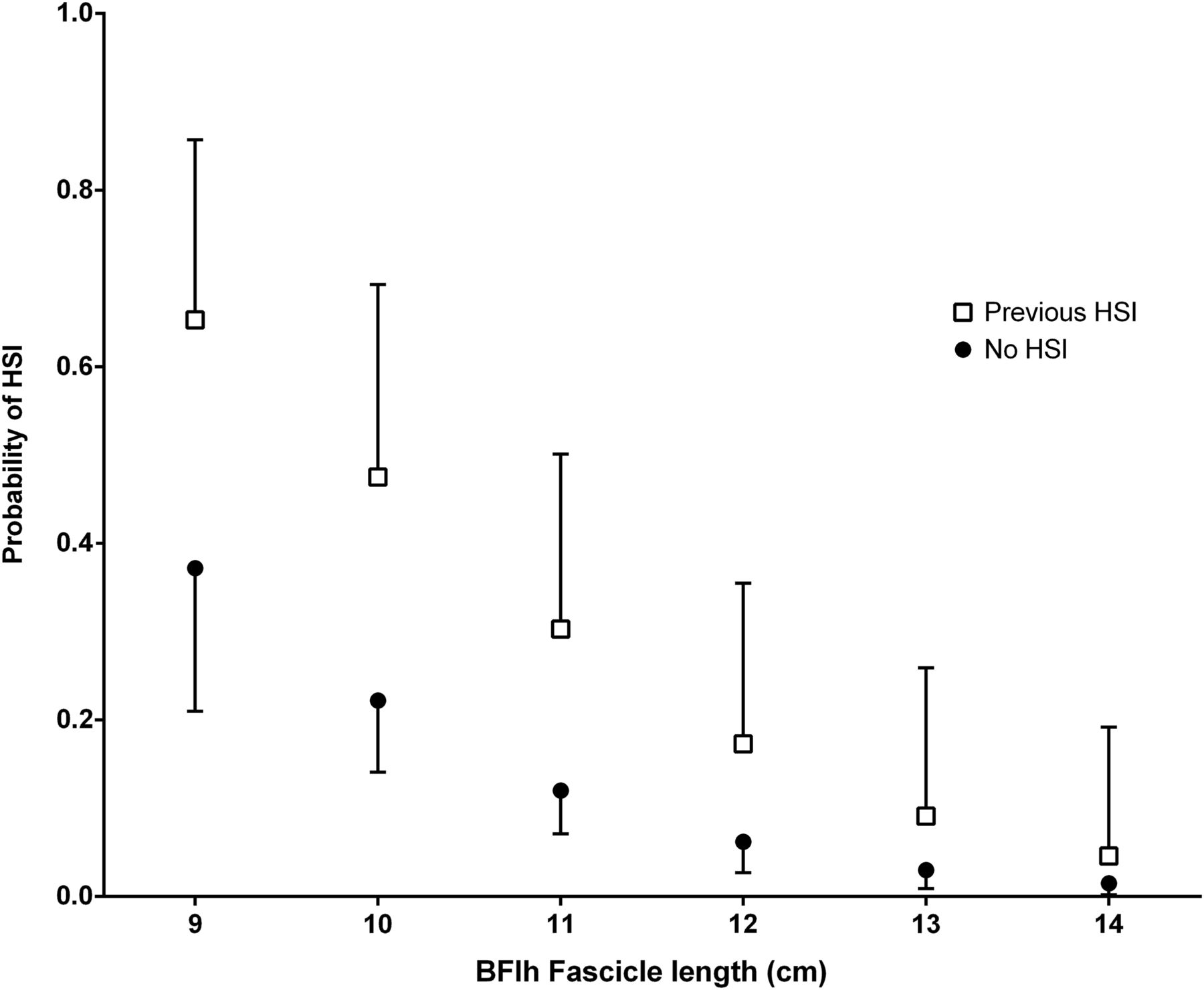
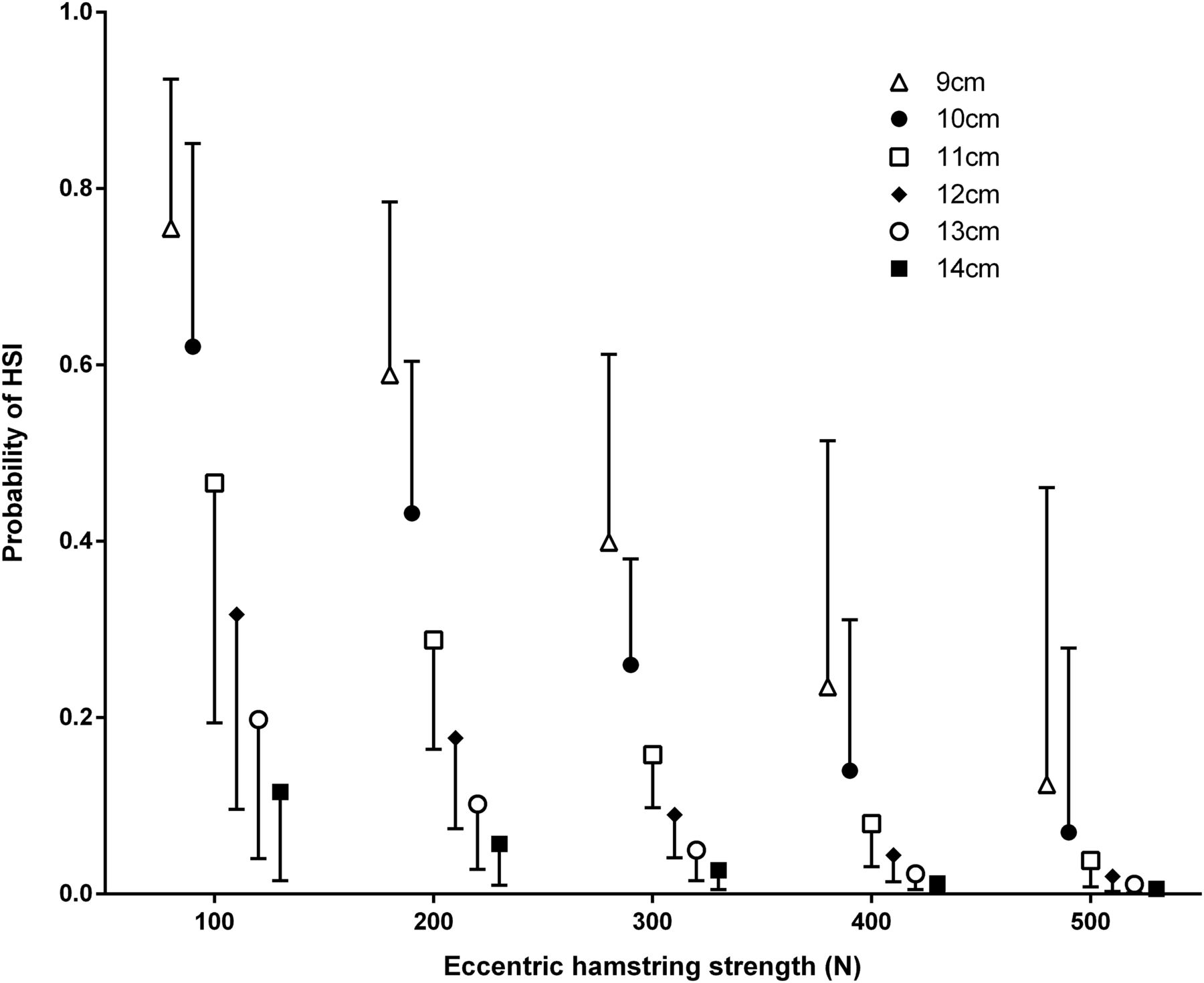
Details of all of the logistic regression models can be found in table 3 and figures 1⇓⇓⇓–5. All of the models were significant (model 1: prior HSI and BFlh fascicle length, p<0.001; model 2: age and BFlh fascicle length; p<0.001; model 3: prior HSI and eccentric strength, p=0.009; model 4: age and eccentric strength, p=0.007; model 5: eccentric strength and BFlh fascicle length; p<0.001), however, none of the interactions reached significance (table 3). For all models in which fascicle length was included, it made the most significant contribution to the model. A Nagelkerke R2 coefficient of 0.31 was found, when using a binary logistic regression, to determine the strength of the association between the two continuous independent variables (eccentric strength and fascicle length) with the dependent variable of a prospective HSI occurrence (yes/no).
Multivariate logistic regression model outputs and receiver operator characteristic curve data using prior HSI, age, BFlh fascicle length and eccentric knee flexor strength

The interaction between BFlh fascicle length, history of HSI and the probability of a future HSI (error bars indicate 95% CI). BFlh, biceps femoris long head; HSI, hamstring strain injury.

The interaction between BFlh fascicle length, age and the probability of a future HSI. The ages are representative of the 10th, 25th, 50th, 75th and 90th centile of the cohort. Note that the data has been offset (to the left or right) on the x-axis to allow for the visibility of the error bars of all the age groups. The data points and error bars are reflective of data at 9, 10, 11, 12, 13 and 14 cm for all groups (error bars indicate 95% CI). BFlh, biceps femoris long head; HSI, hamstring strain injury.

The interaction between eccentric knee flexor strength, history of HSI and the probability of a future HSI (error bars indicate 95% CI). HSI, hamstring strain injury.

The interaction between eccentric knee flexor strength, age and the probability of a future HSI. The ages are representative of the 10th, 25th, 50th, 75th and 90th centile of the cohort. Note that the data has been offset (to the left or right) on the x-axis to allow for the visibility of the error bars of all the age groups. The data points and error bars are reflective of data at 100, 200, 300, 400 and 500 N for all groups (error bars indicate 95% CI). HSI, hamstring strain injury.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The interaction between eccentric knee flexor strength, BFlh fascicle length and the probability of a future HSI. Note that the data has been offset (to the left or right) on the x-axis to allow for the visibility of the error bars of all the age groups. The data points and error bars are reflective of data at 100, 200, 300, 400 and 500 N for all groups (error bars indicate 95% CI). BFlh, biceps femoris long head; HSI, hamstring strain injury.
Discussion
Main findings
This is the first study that has examined the role that BFlh fascicle length plays in the aetiology of HSI. The main findings were that (1) athletes that suffered a HSI possessed shorter BFlh fascicles than those that remained uninjured; (2) athletes that suffered a HSI were weaker during eccentric contractions than those who remained uninjured; (3) between-limb imbalances in eccentric strength and BFlh fascicle length were not different between the injured or uninjured groups and between-limb imbalances did not infer any increased HSI risk; (4) the probability of future HSI associated with non-modifiable factors (increasing age and a history of HSI) appears to be influenced by BFlh fascicle length and eccentric knee flexor strength and (5) measures of MVIC knee flexor strength were not different between the injured and uninjured groups and did not infer any increased HSI risk.
BFlh fascicle length and the risk of a future HSI
In the current study short BFlh fascicles were associated with an increased risk of future HSI in elite soccer players. One previous retrospective investigation reported that individuals with a unilateral HSI history have shorter BFlh fascicles in the previously injured limb than the contralateral uninjured limb.16 It was previously hypothesised that shorter fascicles, with fewer in-series sarcomeres, may be more susceptible to being overstretched and having damage caused by powerful eccentric contractions, like those performed during the terminal swing phase of high-speed running.13 ,30 Given that more than two-thirds of the HSIs noted in the current study occurred during high-speed running, the shorter BFlh fascicles in the subsequently injured limbs may have increased the susceptibility of the muscle to damage and altered their HSI risk.
Knee flexor strength and HSI risk
Low levels of eccentric knee flexor strength during the Nordic hamstring exercise increased the risk of a future HSI in elite soccer players. This has also been recently observed in elite Australian footballers.9 As the hamstrings are required to contract eccentrically during the terminal swing phase of the gait cycle,31 low levels of eccentric strength may reduce the hamstrings ability to do this and as a result potentially lead to an acute injury. Interestingly, low levels of isometric knee flexor strength were not associated with future HSI rates and this suggests that the contraction mode of strength tests is a critical factor in determining their predictive value. This is of particular relevance given that isometric assessments of the knee-flexors have been developed and advocated as clinically convenient32 and minimally ‘intrusive’ in athlete training programs33 given the low levels of muscle damage and soreness involved. Without discounting the value and convenience of such isometric tests as measures of strength and indicators of fatigue,33 the present results suggest that eccentric hamstring tests are of greater value in determining injury risk.
Between-limb imbalance and HSI risk
The current study also found that a larger between-limb strength imbalance during the Nordic hamstring exercise did not increase the risk of future HSI and this is consistent with a similar recent study in Australian Football League (AFL) players9 but contrary to previous findings in elite soccer, which indicated that isokinetically derived between-limb eccentric strength imbalances are associated with an increased risk of HSI.11 Bourne and colleagues have also recently observed, in a prospective study, that between-limb imbalances >15% in the Nordic strength test (as employed in this study) are associated with elevated HSI rates in rugby union players while absolute strength levels are not.34 The diverse findings in these studies are hard to explain. The different physical demands of these three football codes are readily apparent34 and the mode of testing may also influence the results of these prospective studies.
Multivariate comparisons
Multivariate exploration into combinations of variables including BFlh fascicle length, eccentric strength, age and a HSI history provides novel insights regarding HSI risk. Advanced age and a history of HSI have been previously reported to increase the risk of a future HSI in elite soccer.5–7 The data in the current study indicate that the risk of a future HSI is lower in older athletes or those who have a history of HSI when coupled with longer BFlh fascicles and/or high levels of eccentric knee flexor strength. Most notably, older athletes with shorter BFlh fascicles and lower levels of eccentric strength were at an increased risk when compared to younger athletes.
As an example, the results of the current study allow us to estimate that a 33-year-old athlete with a BFlh fascicles of 10 cm has a 65% probability of HSI occurring, while a 22-year-old has a 17% probability of injury. Similarly, 33-year-old athletes with two-limb-average eccentric strength level of 200 N have an estimated probability of HSI injury of 46% while a 22-year-old player has an injury probability of 27%. Despite these results, the Nagelkerke R2 coefficient indicated that eccentric strength and BFlh fascicle length accounted for approximately 30% of the risk associated with a prospective HSI occurrence. Therefore future research is still needed to identify the other 70% of the risk associated with a prospective HSI that is not accounted for.
Limitations
The authors acknowledge that there are limitations in the current study. First, there is a lack of athlete exposure data and this does not allow for the determination of injury incidence relative to exposure to training and match play. Future work should focus on determining the interaction between high-speed running demands and the risk of a future HSI. Second, the study was undertaken in elite soccer players and as such generalising the results to athletes of different sports may be done with caution. For example, in Australian Rules Football the ROC-curve determined threshold for an elevated risk of future HSI was 256 N at the start of preseason.9 This differs when compared to the 337 N found in the current study. One explanation for this variance is the different sporting populations utilised in the two studies that highlights the population specificity of the results. It also indicates that the need for future research in other sporting cohorts is warranted. It should be noted that the thresholds for elevated risk of future HSI determined using the ROC-curve approach should not be compared across studies as an indicator of which cohort have greater strength. Third, the measures of eccentric knee flexor strength were not made relative to an anterior muscle group such as the knee extensors or the hip flexors. Doing so may have enabled the determination of a hamstring-to-quadriceps ratio, or something of a similar nature. Despite the lack of this relative comparison, the eccentric knee flexor strength measures in this study provided valuable information regarding HSI risk, which suggests such ratios may not be crucial. The assessment of muscle fascicle length was only performed on the BFlh. Considering the high rates of BFlh strain injury in the current study, the authors believe it was justified to focus on this muscle. Future research could aim to assess the risk associated with short fascicles in the other hamstring muscles.
Conclusion
Elite soccer players with short BFlh fascicles and low levels of eccentric knee flexor strength are at an increased risk of HSI compared to athletes with longer fascicles and greater eccentric strength. Isometric knee flexor strength and large between-limb imbalances in eccentric strength did not influence the risk of HSI. The inter-relationship between the non-modifiable risk factors of increasing age and previous HSI history, with the modifiable variables of eccentric strength and BFlh fascicle length, provides a novel approach to constructing an athlete's risk profile.
What are the findings
Having short biceps femoris long head (BFlh) fascicles (a newly identified risk factor) increased the risk of a future hamstring strain injury.
Low levels of eccentric knee flexor strength increased the risk of a hamstring strain injury occurring in the subsequent season.
The increased risk associated with increasing age and a history of hamstring strain injury can be mitigated with greater levels of eccentric knee flexor strength and longer BFlh fascicles.
How might it impact on clinical practice in the future?
Hamstring injury prevention strategies should consider structural adaptations (e.g. fascicle length changes), as well as functional (e.g. eccentric strength).
The interrelationship between modifiable risk factors (eccentric strength and BFlh fascicle length) and non-modifiable risk factors (increasing age and a previous injury history) should be understood when designing injury prevention/rehabilitation programs.
References
Footnotes
Twitter Follow Ryan Timmins at @ryan_timmins, Matthew Bourne at @mbourne5 and David Opar at @davidopar, Anthony Shield at @das_shield, Morgan Williams at @drmorgs, Christian Lorenzen at @athleticexcel
Contributors RGT was the principle investigator and was involved with study design, recruitment, analysis and manuscript write up. MNB was involved with recruitment, analysis and the manuscript preparation. AJS, MDW, CL and DAO were involved with the study design, analysis and manuscript preparation. All authors had full access to all of the data (including statistical reports and tables) in the study and can take responsibility for the integrity of the data and the accuracy of the data analysis.
Funding This study was partially funded by a Faculty of Health Sciences Research Grant from the Australian Catholic University.
Competing interests A Faculty of Health Research Grant from the Australian Catholic University partially funded the research; AJS and DAO are listed as co-inventors on a patent filed for a field test of eccentric hamstring strength (PCT/AU2012/001041.2012) as well as being shareholders in a company responsible for commercialising the device; RGT, MNB, MDW and CL have no relationships with companies that might have an interest in the submitted work in the previous 3 years; their spouses, partners, or children have no financial relationships that may be relevant to the submitted work; and RGT, MNB, AJS, MDW, CL and DAO have no financial interests that may be relevant to the submitted work beyond what is already declared
Ethics approval This study was approved by the Human Research Ethics Committee of the Australian Catholic University (approval number: 2014 26V) and informed consent was provided to all participants.
Provenance and peer review Not commissioned; externally peer reviewed.