Article Text

Abstract
Aims To test the hypothesis that total sitting time is associated with incident diabetes, after adjustment for physical activity and obesity.
Methods 72 608 Danish adults from the DANHES cohort reported their total sitting time in 2007–2008 and were followed-up for 5 years, in relation to register-based incident diabetes mellitus. Cox regression analyses were used, and the effect-modifying influence of obesity and physical activity assessed.
Results The age-sex adjusted HR for developing diabetes among those who sat 10+ h/day as compared to <6 h/day was 1.35 (95% CI 1.17 to 1.57). The relative risks were similar by gender, but were largely attenuated by adjustment for potential confounding factors including physical activity, and statistically non-significant for all categories of body mass index except the obese.
Conclusions The association between total sitting time and incident diabetes is substantially moderated by physical activity and obesity. Total sitting time remains a risk factor for diabetes only in inactive and obese populations.
- Diabetes
- Epidemiology
- Physical activity
- Sitting time
Statistics from Altmetric.com
Introduction
Sedentary behaviour, or ‘too much sitting’, is considered an emerging health risk factor for the development of chronic diseases.1 In developed countries, adult populations spend most of their waking time engaged in sedentary behaviours.2 ,3 Sedentary behaviours encompass sitting at work, watching television, using a computer, and driving a car, but are distinctively different behaviours to a lack of moderate-to-vigorous physical activity, as it is possible to sit for prolonged periods, and also meet the recommendations for leisure time moderate-to-vigorous physical activity.
The mechanisms underlying the physiology of sitting are starting to be understood. It appears that prolonged sedentary behaviour downregulates enzymes involved in glucose transport and lipid metabolism,4 leading to a decrease in their uptake from the circulation; this, in turn, leads to hyperglycaemia, hyperlipidaemia and hyperinsulinaemia, and potentially, increased cardiometabolic risk.1 Cross-sectional studies have shown associations between sedentary behaviour and biomarkers, such as glucose/insulin metabolism,1 ,5 and human experimental studies have suggested that prolonged uninterrupted sedentary behaviour may have harmful effects on cardiometabolic biomarkers.6 A recent meta-analysis of epidemiological studies has demonstrated evidence of associations between TV watching time (as one of the proxy measures for sitting) and diabetes.7 In summary, the evidence is strong for sitting and diabetic precursor biomarkers, and for prolonged TV time and diabetes, but limited evidence exists in assessing total sitting time and the development of diabetes. Further, the magnitude and the consistency of the associations remain unclear.
The purpose of this study is to examine whether total sitting time is associated with subsequent risk of diabetes in a large prospective cohort of Danish adults. Also, we assessed the potential effect-modifying influences of obesity and physical activity.
Methods
The study was based on the Danish Health Examination Survey (DANHES) which was conducted in Denmark in 2007–2008. DANHES is described in detail elsewhere.8 In 13 municipalities, all citizens aged 18 years or more were invited to participate by letter. No reminders were sent. The study was conducted over a period of 1 month in each municipality. A total of 538 163 persons were invited, and 76 478 persons participated (response rate: 14%). At baseline, self-administered questionnaires were used to assess participant's sitting time, leisure time physical activity level and body mass index (BMI). Besides this information, the questionnaires also asked about general health, other lifestyle-related factors, and social relations. In 12 municipalities, an internet-based version of the questionnaire was used. In one municipality, a paper-based questionnaire was used. Besides the questionnaire, a random subsample was invited to participate in a clinical health examination including anthropometric measures and blood samples (n=180 103 were invited). Of these, 18 065 participated (participation rate: 10%). Participants provided informed consent and the protocol was reviewed by the Scientific Ethical Committee B for the Capital Region of Denmark (H-B-2007-050). Participants were followed up for diabetes in national registers, to 10 August 2012.
Diabetes definition
Information on diabetes incidence was obtained from the Danish National Diabetes Register. Here, diabetes was defined if one of the following criteria was fulfilled: hospitalisation with a diagnosis of diabetes (International Classification of Disease (ICD) 8: 249 or 250, ICD-10: DE10–14, DH 36.0 or DO24 (excluding D=24.4)); registration of chiropody (coded for diabetes) in the National Health Insurance Service Registry; frequent measurements of blood glucose either at least five times within 365 days (1 year), or at least two annual measurements of glucose during a 5-year period (registered in the National Health Insurance Service Registry); or prescription of insulin or oral antidiabetic medication at least twice (from the Register of Medicinal Product Statistics).9
Baseline glycosylated haemoglobin and waist circumference
Non-fasting venous blood samples were collected for examination of glycosylated haemoglobin (HbA1c) at the clinical health examination conducted at baseline. The blood sample collection was carried out and analysed by the Department of Clinical Biochemistry, KB 3-01-1, Rigshospitalet. Non-fasting venous blood samples were collected after light stasis and stored at 5°C. The waist circumference (cm) was measured with body tape at a level midway between the lower rib margin and the iliac crest.
Sitting time and physical activity
Information on the amount, frequency and intensity of physical activity and sitting time was obtained from self-administered questionnaires measured by a Danish version of the long International Physical Activity Questionnaire (IPAQ-L). The IPAQ is known to be a valid and reliable instrument for assessing physical activity and sitting time in a European setting such as Denmark.10 ,11 It consists of 31 items that collect information on time spent on sitting time and physical activity in four domains: work, transport, housework/gardening and leisure time.
Total sitting time was assessed by the following question: ‘During the past 7 days, how much time did you usually spend sitting during work and leisure time on: (1) a weekday? and (2) a weekend day?’ The sitting question was prefaced by asking participants to consider multiple domains of sitting, excluding time spent sitting during transport, which was captured in another item of the IPAQ questionnaire. Average daily total sitting time (min/day) was calculated as the sum of weekday sitting minutes × 5, and weekend day sitting minutes × 2, and divided by 7. Time spent travelling in a motor vehicle was also added (min/day). Last, the sum was converted to h/day.
In all four domains, work, transport, housework/gardening and leisure time, participants were asked to indicate the amount of time spent on physical activity during the previous 7 days in relation to frequency (days/week), duration (in h and min) and level of intensity (walking, moderate and vigorous). Questions were provided with examples of common activities. Examples of vigorous physical activity were aerobics, fast bicycling/running, while moderate physical activities comprised activities like swimming and bicycling. Time spent in moderate-intensity to vigorous-intensity physical activities (MVPAs) in leisure time and for transportation was categorised into four categories based on the WHO weekly physical activity recommendations12: (1) <30, (2) 30 to <150, (3) 150 to <300 and (4) 300+ min/week. In addition to MVPA, time spent in walking activities was estimated (in leisure time and for transportation). Walking was studied separately from MVPA because walking is a common behaviour in Denmark and is considered important for reducing the risk of diabetes.13 Walking was grouped into (1) <60, (2) 60 to <150, (3) 150 to <300 and (4) 300+ min/week.
Other covariates
Additional questionnaire variables included in the analyses were: age, education (<12, 12–14 and 15+ years), smoking (never-smoker, ex-smoker, occasional smoker, daily smoker (1–15 g of tobacco/day) and heavy smoker (>15 g of tobacco/day)), alcohol consumption (number of drinks/week), self-reported diabetes measured by a question of ‘Have you ever been told by a doctor that you have diabetes?’ (yes, no), self-reported hypertension (yes current/yes previously, no), self-reported cardiovascular disease (yes current/yes previously, no) and BMI (calculated from self-reported height and body weight measure).
Statistical analyses
We tested the hypothesis that total sitting time is associated with increased risk of diabetes. Participants with diabetes prior to the baseline were identified from their self-reported questionnaire and through linkage to the Danish Diabetes Register, and were excluded from analyses (n=3585). Further, participants who had reported very poor self-rated health status (n=285) were excluded, leaving 72 608 for analyses. Cox regression analysis was applied using Stata V.13.1. Initial models were adjusted for age and sex, and subsequent models further adjusted for education, smoking habits, BMI (as both a linear and a squared term), alcohol consumption (linear and square root terms), hypertension, previous cardiovascular disease, and MVPA.
Data on physical activity and sitting time were checked for out-of-range values, and cleaned according to the IPAQ scoring protocol.14 Around 18% of the values of total sitting time was missing (17% for transportation, 8% for sitting during weekends and 5% for sitting during weekdays). To account for missing values, we performed multiple imputations by chained equations (m=20 imputations).15 Interaction between sitting time and BMI was addressed in a model including sitting time and BMI continuously plus the cross product. Interaction between sitting time and MVPA was addressed in a model including sitting time and MVPA plus the cross-product, and evaluated using a likelihood ratio test.
The absolute risks of diabetes by combinations of categories of daily sitting (10+ h/day), MVPA (<150 and ≥150 min/week) and walking activities (<150 and ≥150 min/week) were estimated using the regression coefficients from a Poisson regression model; these three covariates were included to study the joint association of physical activity and sitting time in more detail. Absolute risks are presented as estimated incidence rates.
Results
Characteristics of participants by categories of total sitting time are shown in table 1. The median total sitting time was 6.3 h/day (25th–75th centiles: 4.4–8.6). Individuals who reported sitting for 10 h or more per day were more likely to be younger, have a high educational level (15-year or more), be physically inactive, smoke, have higher BMI, and have higher average alcohol consumption (table 1). However, they were less likely to suffer from hypertension. Participants not responding to the question on sitting time were more likely to be older (mean=52), and have <12 years of education (41%) but did not vary by other covariates (data not shown).
Baseline characteristics of the study population by total sitting time, using imputed data*
For both men and women, we observed no difference in the baseline HbA1c levels across the categories of sitting time (table 2). Waist circumference was significantly different in the highest compared to the lowest sitting category, with an average difference of 1.4 cm for men and 0.5 cm for women.
Regression coefficients (95% CIs) of baseline HbA1c (mmol/L) and waist circumference (cm) according to total sitting time for men and women*
During a mean follow-up of 4.9 years, 1790 adults developed diabetes, corresponding to an incidence rate of 508/100 000 person-years (623/100 000 and 432/100 000 in men and women). The relationship between sitting time and diabetes is shown in table 3. In the analyses adjusted for age (model b), those reporting 6–10 h of sitting were 15% more likely to develop diabetes, and those reporting 10 or more hours of daily sitting were 35% more likely to develop diabetes. These relationships were no longer statically significant when adjusted for BMI and physical activity (models c and d). For men, similar patterns were seen, whereas for women, only the 10+ sitting h/day showed a significant relationship, which also was attenuated and non-significant after adjustment for BMI and then for physical activity.
HRs (95% CIs) of diabetes by total sitting time in men and women (n=72 608)*
Figure 1 shows the HRs for developing diabetes according to BMI categories. Among participants at all levels of obesity (BMI ≥30) there was a clear dose–response relationship between increased sitting time and diabetes, while there was no increase in diabetes risk among those in the normal weight range (p=0.05 for interaction).

HRs (fully adjusted) of diabetes by sitting time and body mass index (BMI). Tables demonstrate point estimates for selected combinations of sitting time and BMI.
In stratified analyses, participants reporting <150 min/week in MVPA showed an apparent increase in diabetes risk with increasing sitting time, while increased sitting was not associated with an increasing risk of diabetes among those reporting at least 150 min/week in MVPA. However, the p value for interaction was non-significant (p=0.68) (figure 2).

HRs (fully adjusted) of diabetes by sitting time and moderate-to-vigorous intensity physical activity (MVPA). Tables demonstrate point estimates for selected combinations of sitting time and physical activity level.
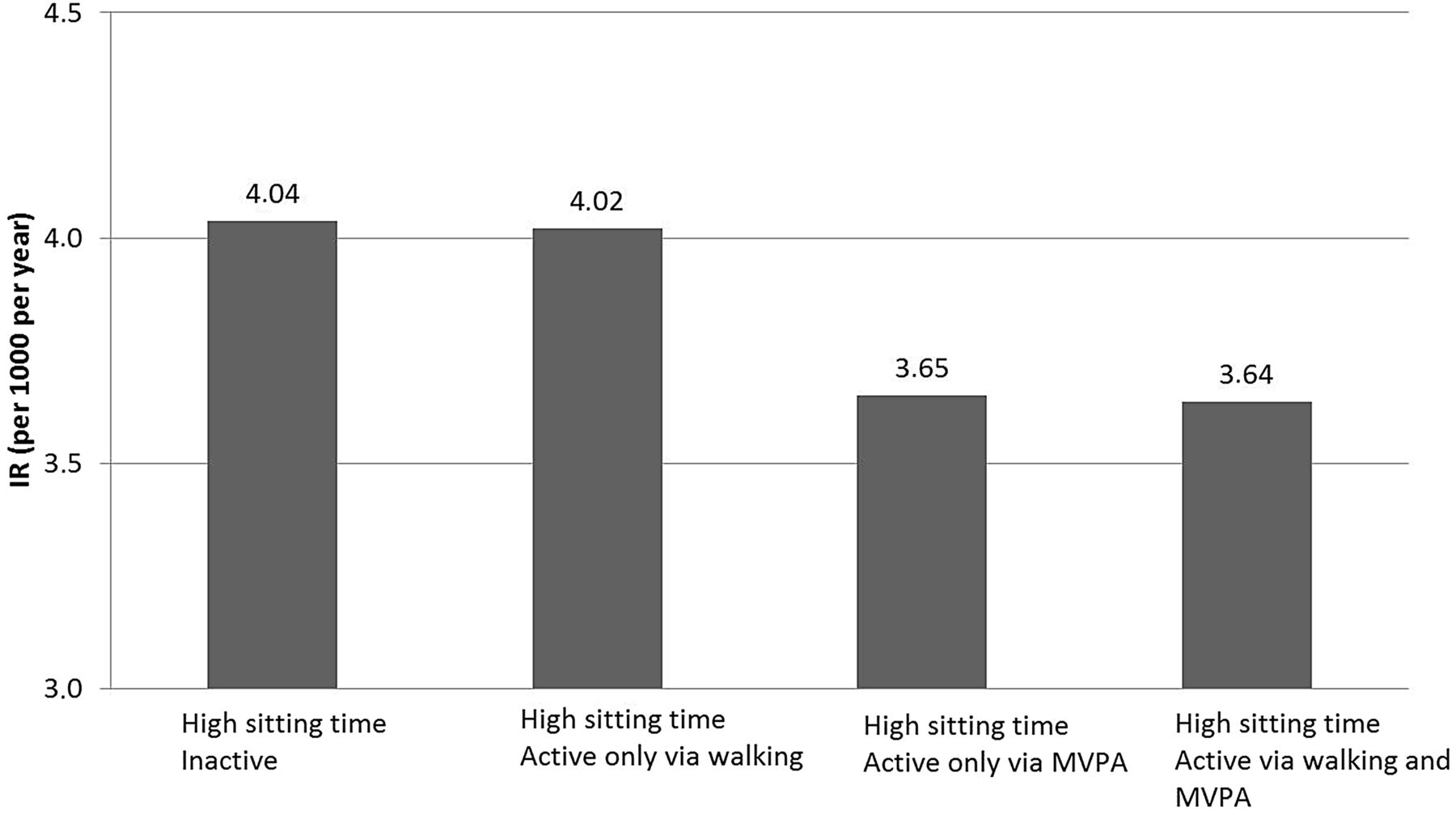
The absolute risks of diabetes among those reporting high levels of sitting (at least for 10 h/day) in combinations with MVPA and walking are shown in figure 3. The annual incidence rate of diabetes was 4.0/100 000 for those with high sitting time (10 h or more per day), and who were also physically inactive (<150 min/week in MVPA, and less than 150 min/week of walking activities). By comparison, those with high sitting time who also spent at least 150 min/week in MVPA had an incidence rate of 3.7/100 000, corresponding to a 9% reduction in the absolute risk of diabetes. Walking activities alone had no apparent influence on the incidence rate of diabetes.

{kind=link}
{kind=link}
{kind=link}
The absolute risks (incidence rate) of diabetes by high sitting time (total sitting time ≥ 10 h/day) and physical activity measured as time spent in moderate-to-vigorous intensity physical activity (MVPA) (<150 min /week, ≥150 min/week), and walking (<150 min /week, ≥150 min/week) among 72 608 Danish men and women were estimated using regression coefficients from a Poisson regression model.
Discussion
To the best of our knowledge, this is the first epidemiological study to date that examined total sitting time and diabetes incidence in a large cohort of both men and women, a relationship that was hypothesised from previous physiological and experimental studies.7 In this Danish cohort, we failed to show a clear relationship with prolonged sitting time. We found partial support for our hypothesis that people reporting many hours of sitting have a higher risk of developing diabetes, but when adjusting for BMI and then for physical activity, the risk was substantially attenuated or abolished. Our stratified analyses showed that increased risks of prolonged sitting for incident diabetes was present only among those who were overweight/obese, and also among those with low levels of MVPA. Our findings suggest that high sitting might potentiate the risk of developing diabetes among obese or inactive adults, but not in physically active or normal weight adults.
Our findings provide an important contribution to the current literature about the associations between sedentary behaviours and adverse health outcomes. Previous work suggests that long hours of sitting is linked to an increased risk of ischaemic heart disease, type 2 diabetes, some types of cancer, and premature death regardless of physical activity, and other coexisting factors.16–18 A previous meta-analysis showed a significant relationship between sedentary behaviour, measured through the domestic sitting domain (with TV time as a proxy measure), and the risk of type 2 diabetes; this review reported a relative risk of 1.20 for each 2 h increase in daily TV time.19 The surprising, novel observation in the present study is the lack of an independent risk of developing diabetes among those reporting prolonged total daily sitting time. This finding is somewhat in contrast with previous prospective studies indicating a positive association between sedentary behaviour and diabetes incidence.20–23 However, all but one study used television time as the sedentary behaviour exposure variable rather than ‘total sitting time’. Hu et al22 studied sedentary behaviour at work and in leisure time prospectively in the Nurses Health Study, and related this to the onset of type 2 diabetes. They found strong associations for time spent in sedentary behaviours in leisure time whereas the associations were weaker for sedentary time at work. A possible explanation is that TV viewing correlates differently with health outcomes compared with sitting for other purposes (eg, at work or transportation). Further, television watching, but not sitting at work, could lead to higher caloric intake and a relatively unhealthy dietary pattern that might contribute to risk of diabetes.23 Also, differences in socioeconomic position may confound the observed associations, as lower socioeconomic position is generally positively associated with greater TV-viewing time but is inversely associated with sitting at work.
Our results showed that waist circumference differed by sitting time, but no difference was seen in baseline HbA1c levels in this cohort. We stratified sitting-related risk by BMI and physical activity levels; as has been done previously for cardiovascular and all-cause mortality outcomes, and metabolic biomarkers.24–27 Recent research has also reported that the associations between total sitting time and diabetes is attenuated by obesity,28 and in a small Canadian study, standing at work was not significantly associated with the risk of diabetes after adjustment for fitness.29 There is a need for replication studies to confirm the modifying effects of obesity and physical activity on the sitting-related risks, specifically for population studies of diabetes incidence. If replicated, this would re-affirm the need to maintain acceptable body weight and regular participation in moderate-to-vigorous physical activity, both for their own health benefits, and to offset their synergistic diabetes risk with prolonged sitting.
The inverse association between physical activity and risk of diabetes is well established.30 Most studies have reported reduced risk with greater moderate-to-vigorous intensity activities, whereas, it is less clear for lower intensity physical activities such as walking.30 Our findings suggest that in this Danish population, physical activity needs to be of moderate and vigorous intensity to offset the adverse health consequences of prolonged sitting time. Thus, our results support the current WHO physical activity recommendations of at least 150 min of MVPA throughout the week to improve and maintain health. Previously, time spent in walking activities, and not only MVPA, has been shown to reduce the risk of diabetes.30 However, it should be noted that the Danish population in general have a fairly high physical activity level and also have high total sitting time compared with several other European countries.31 Also, in general, participants in this cohort were healthier and more physically active than non-participants, and thus, results may differ from what is observed in other cohorts.
The strengths of this study are the large population-based cohort of both men and women; using registry-defined diabetes incidence and a closer temporal relationship to diabetes incidence than studies of sitting and diabetes mortality. Through linkage to nation-wide registers, it was possible to exclude participants with a history of diabetes prior to baseline. Adjustment for, and stratification by BMI and physical activity more clearly delineated the risks of prolonged sitting. The limitations include a single exposure time point, and using self-report measures for sitting, although self-report sitting has shown reasonable measurement properties compared to objective assessment.32 Only 14% of the invited individuals participated, and thus, results may not be representative of the entire Danish population.8 However, given the cohort design of the study, selection should not affect the internal validity. Also, to reduce non-response bias, data were weighted for non-response. Our analyses were adjusted for a range of demographic and behavioural variables, although residual confounding from unmeasured factors remains a possibility.
An advantage of the present study is that it covers the sum of daily sitting during work and leisure time on both weekdays and weekends. For most working adults, time spent sitting in the workplace is likely to be a greater contributor to total sitting time than sitting during leisure time. However, we were unable to examine the potential effects of domain-specific sitting behaviours. As mentioned previously, it is possible that sitting for various purposes (eg, TV-viewing or occupational sitting) may show different patterns of associations with diabetes.
In conclusion, in this Danish cohort, we failed to show that prolonged sitting time is directly related to diabetes risk, as adjusting for BMI and then for physical activity attenuated the risk. Our findings suggest that sitting time remains a risk factor for diabetes only in inactive and obese populations.
What are the findings?
Our findings fail to support a clear association between total sitting time and risk of diabetes.
Previous studies have mostly used TV watching time as a proxy measure of sitting time exposure.
In these data, high total sitting time is associated with a risk of incident diabetes among obese, but not normal weight adults.
High total sitting time is associated with a risk of incident diabetes among physically inactive, but not active adults.
How might it impact on clinical practice in the future?
Our results support the public health initiatives to encourage adults to sit less, but it is particularly important to maintain acceptable body weight and participate in regular physical activity.
Clinical advice to reduce total sitting time is particularly important among the inactive or those who are obese.
Reducing total sitting time does not seem as relevant for diabetes risk among those who are active and normal–overweight.
References
Footnotes
Contributors AB and JST designed the analytical strategy and wrote the article. CBP and JST performed the analyses and wrote the paper. AB assisted in the implications. All authors certify to have participated sufficiently in the work to take public responsibility for the appropriateness of the design, method, collection, analysis and interpretation of the data. Additionally, all authors have read and approved the final version and have agreed to share data used in the study.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.