Article Text

Abstract
Background Shoulder problems are highly prevalent among elite handball players. Reduced glenohumeral rotation, external rotation weakness and scapula dyskinesis have been identified as risk factors.
Aim Evaluate the effect of an exercise programme designed to reduce the prevalence of shoulder problems in elite handball.
Methods 45 elite handball teams (22 female teams, 23 male teams, 660 players) were cluster randomised (22 teams, 331 players in the intervention group, 23 teams, 329 players in the control group) and followed for 1 competitive season (7 months). The Oslo Sports Trauma Research Center (OSTRC) Shoulder Injury Prevention Programme, an exercise programme to increase glenohumeral internal rotation, external rotation strength and scapular muscle strength, as well as improve kinetic chain and thoracic mobility, was delivered by coaches and captains 3 times per week as a part of the handball warm-up. The main outcome measures, prevalence of shoulder problems and substantial shoulder problems, were measured monthly.
Results The average prevalence of shoulder problems during the season was 17% (95% CI 16% to 19%) in the intervention group and 23% (95% CI 21% to 26%) in the control group (mean difference 6%). The average prevalence of substantial shoulder problems was 5% (95% CI 4% to 6%) in the intervention group and 8% (95% CI 7% to 9%) in the control group (mean difference 3%). Using generalised estimating equation models, a 28% lower risk of shoulder problems (OR 0.72, 95% CI 0.52 to 0.98, p=0.038) and 22% lower risk of substantial shoulder problems (OR 0.78, 95% CI 0.53 to 1.16, p=0.23) were observed in the intervention group compared with the control group.
Conclusions The OSTRC Shoulder Injury Prevention Programme reduced the prevalence of shoulder problems in elite handball and should be included as a part of the warm-up.
Trial registration number ISRCTN96217107.
- Shoulder
- Overuse injury
- Handball
- Injury prevention
Statistics from Altmetric.com
Introduction
Shoulder injuries, predominantly from overuse, have been highlighted as an area warranting preventative efforts in a wide variety of throwing sports,1–13 where the shoulder is exposed to large demands due to repeated overhead motion at high velocity.14–16 Elite handball is no exception; a history of shoulder pain is common (44–75%), the point prevalence of current shoulder pain is high (20–52%) and the average weekly prevalence of shoulder problems (28%) and substantial shoulder problems (12%) is significant.2 ,7 ,17
Several internal modifiable risk factors for shoulder injury have been investigated among throwing athletes, predominantly handball and baseball players. In handball, reduced glenohumeral internal rotation and excessive glenohumeral external rotation have been suggested as risk factors in a cross-sectional study.18 In a prospective study, a reduction of total glenohumeral rotation has been associated with shoulder problems.2 Similarly, in baseball, reduced glenohumeral internal rotation and total rotational range of motion have been linked to shoulder injury.3 ,5 ,19–21 Regarding rotator cuff strength, external rotation weakness and low ratios of concentric and eccentric external to internal rotation strength have been reported as risk factors in handball and baseball.2 ,6 ,22–24 In addition, weakness in glenohumeral abduction strength has been associated with shoulder injury in baseball.6 ,24 ,25 Recently, the presence of scapular dyskinesis was reported as a risk factor correlated with shoulder problems in elite handball.2 However, this factor has not been associated with shoulder injury among baseball players.26 Reduced kinetic chain function and limited thoracic mobility are often implicated in shoulder injuries,27 ,28 despite a lack of evidence associating these factors with shoulder injury.
There are no randomised controlled trials targeting prevention of overuse shoulder injuries in elite handball, or throwing sports in general.29 Thus, the main objective of this randomised controlled trial was to evaluate the effect of an exercise programme designed to reduce the prevalence of shoulder problems in elite handball.
Methods
Study design and participants
This was a two-armed cluster-randomised controlled trial. The authors followed and completed the Consolidating Standards for Reporting Clinical Trials (CONSORT) with the subsequent extension to cluster randomised trials.30 During the off-season (June to July 2014) we invited, in collaboration with the Norwegian Handball Federation, every male and female handball team (n=48) in the two top divisions (elite level) in Norway to participate in the study. Of these, 46 teams agreed to participate and were randomised by team into an intervention or control group (figure 1). A neutral, blinded person who had no further involvement in the study conducted and revealed the randomisation after the final team had been recruited to ensure concealment of allocation. A computer-generated list of random team numbers was used to randomise teams stratified by gender and competition level, where all players from the same team were assigned to the same group. The randomisation aimed to achieve a balanced number of female and male teams from the two top divisions in the intervention and control groups.

Study flow chart showing the recruitment, dropout and the number of players included and analysed.
We visited each team (n=46) during a training session in the preseason (August to mid September 2014) and invited every player present to participate in the study. All players with a team contract were eligible for participation, irrespective of their baseline injury status or history (N=677). Players who consented to participate completed baseline questionnaires and were followed for the duration of the regular season (September 2014 through March 2015). Six times during the season, players reported any shoulder problems using the Oslo Sports Trauma Research Center (OSTRC) Overuse Injury Questionnaire,31 as described in a previous study on risk factors for shoulder problems among male elite handball players.2 During our baseline visit, we instructed teams in the intervention group on how to use the exercise programme to be implemented during the subsequent week. We asked control teams to warm up as usual.
Baseline questionnaires
We registered demographic and anthropometric data, dominant arm, playing position and number of years as an active handball player. Players reported a history of shoulder pain and current shoulder pain using a modified version of the Fahlström questionnaire, previously used in studies on elite handball players.2 ,7 Players reported acute shoulder injuries within the past 6 months and shoulder surgery within the past 12 months. This information was crosschecked with the team medical staff. Finally, we asked them to report any shoulder problems during the previous weeks using the OSTRC Overuse Injury Questionnaire.31
Intervention
We created a preliminary version of the exercise programme based on risk factors for shoulder problems identified among elite handball players.2 ,18 ,22 An expert panel consisting of a fitness coach employed by the Norwegian Handball Federation and four physiotherapists clinically working with handball players nationally and internationally reviewed the exercise programme. A female handball team in a lower division, not included in the study, tested the exercise programme and responded to a questionnaire based on the Reach Effectiveness Adoption Implementation Maintenance framework to provide information regarding their beliefs and experiences of content, duration, load and applicability of the exercise programme.32 ,33
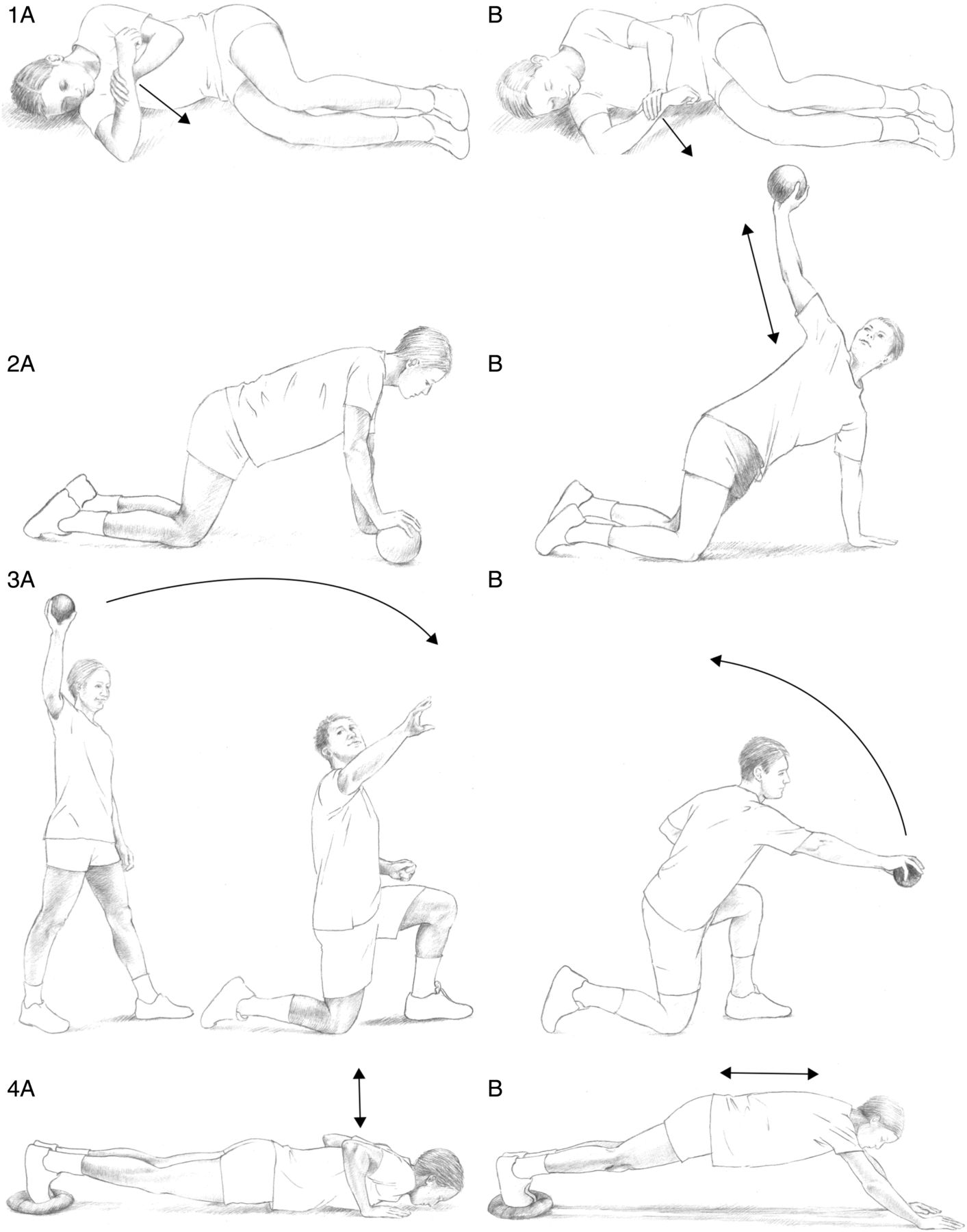
The final version of the OSTRC Shoulder Injury Prevention Programme consisted of five exercises with different variations and levels, aiming at increasing the glenohumeral internal range of motion, external rotation strength and scapular muscle strength. In addition, exercises to improve the kinetic chain and thoracic mobility were included on the basis of recommendations from the expert panel. Examples of exercises included in the programme are illustrated in figure 2. Detailed information on the OSTRC Shoulder Injury Prevention Programme is available as an online supplementary appendix.
Supplementary appendix

Examples of exercises aiming to improve glenohumeral range of motion (1A, B), thoracic mobility (2A, B), external rotation strength (3A, B), scapular muscle strength (4A, B) and kinetic chain (4A, B; A, start position; B, end position).
Players in the intervention group were targets for the exercise programme. Coaches and team captains were delivery agents and received, together with team medical staff, specific training on the content and execution of the exercise programme. We recommended implementing the exercise programme three times per week as a part of the team's regular warm-up to training, before any throwing activity. Teams received posters of the exercise programme, as well as the equipment needed. We instructed the team medical staff to be present at least one session every week during the first 4 weeks, and every second week for the rest of the season, to supervise the quality of the exercises and ensure that players experiencing pain conducted the exercises correctly and with the correct load.
We emphasised the quality of movement, correct positioning of the scapula, good posture and core stability. If a team did not have their own medical staff, we recruited a physiotherapist. We completed follow-up visits to all teams in the intervention group during the mid-season (December 2015 through January 2016) to supervise exercise quality, answer questions and encourage them to complete the exercise programme as recommended. Once players were familiar with the exercises, the programme took about 10 min to complete.
Monitoring of shoulder problems
The OSTRC Overuse Injury Questionnaire was sent electronically by mail to all players in the study on the last Sunday of each month from October 2014 to March 2015, six times in total, using online survey software (Questback V.9692, Questback AS, Oslo, Norway). Automatic reminders were sent to non-responders after 3 and 7 days per email and SMS (Pling, Front Information DA, Oslo, Norway). In addition, we visited teams throughout the season to ensure a high response rate by asking non-responders to complete the questionnaire on paper. The questionnaire gathers information on the extent to which overuse shoulder injuries, expressed as shoulder problems, affect participation, training volume and performance, as well as the level of shoulder pain experienced during the past week. Players were only asked about their dominant shoulder, with shoulder problems defined as any pain, ache, stiffness, instability, looseness or other symptoms related to their shoulder.31 In a supplementary question, players reported any acute injury to the dominant shoulder during the past week, defined as an injury caused by a single identifiable event.34 ,35 Team medical staff also reported any acute shoulder injury by mail at the end of each month (October 2014 to March 2015) and their records were crosschecked with player reports to avoid misreporting of an acute shoulder injury as an overuse injury. Acute injuries were excluded from the analyses.
Outcome measures
Primary outcomes were the prevalence of shoulder problems and substantial shoulder problems in the dominant arm, as measured six times during the season. We calculated the prevalence of shoulder problems in both groups by dividing the number of players who reported any problem (ie, anything but the minimum value in any of the four questions) by the number of questionnaire respondents.31 To filter problems with fewer functional consequences, we calculated the prevalence of substantial shoulder problems in the same way, but only including shoulder problems leading to moderate or severe reductions in training volume or performance, or a total inability to participate.31 Secondary outcome was the severity score of shoulder problems reported during the season. The severity score ranged from 0 to 100 and was calculated on the basis of the four questions in the OSTRC Overuse Injury Questionnaire for every player reporting a shoulder problem.31 The severity scores for all players were summed and divided by the number of respondents. In addition, we calculated the relative impact of shoulder problems in both groups by summing player severity scores during the season and dividing by the total number of responses.
Compliance
We monitored the degree to which the players in the intervention group completed the exercise programme according to our recommendations through self-reporting. Six times during the season, players reported how many times they had completed the exercise programme during the past 7 days, both with the team and by themselves. The total number of sessions completed was summed and divided by the number of respondents to calculate the average weekly compliance with the exercise programme for each measure.
Exposure
Players reported their exposure to handball training, match play and additional strength training six times during the season. We calculated the average weekly exposure to handball training, match play and strength training (minutes) for each measure in both groups by summing up the number of minutes reported and dividing by the number of respondents.
Sample size
We estimated the sample size on the basis of the average prevalence of shoulder problems (28%) and substantial shoulder problems (12%) reported in a prospective risk factor study of shoulder problems among male elite handball players.2 We adjusted for cluster correlations (estimated intraclass correlation coefficient <0.1) based on analysis of variance of within-participant and within-team prevalence, and assumed that we could include 15 players from each of the 48 available teams (n=720). On this basis, we estimated being able to detect a 10% reduction in the prevalence of shoulder problems with a power of 0.94, and a 6% reduction with a power of 0.87, at a 5% significance level.
Statistical methods
Theoretically, we set three responses to the OSTRC Overuse Injury Questionnaire as a minimum to include a player in the analyses. Initial data analyses showed that player response to the questionnaire was sufficient to estimate missing values using multiple imputations. We performed multiple imputations with the assumption of missing at random and used multivariate imputation by chained equation algorithm in combination with a predictive mean matching approach, which led to the pooled results of five multiple imputed data sets.36 In order to assess differences in the prevalence of shoulder problems and substantial shoulder problems between the intervention and control groups over time, we used generalised estimating equation (GEE) models. We used an exchangeable covariance matrix and the significance level (α) was 0.05 for all analyses. Any anthropometric or demographic variables showing a possible difference between groups at baseline (p<0.2) were added to the GEE models using a forward selection procedure. However, since we identified no confounding effects, univariate analyses were performed. All analyses were performed using SPSS statistical software (SPSS V.21, IBM Corporation, New York, New York, USA).
Results
Participants
A total of 22 prevention teams (n=331) and 23 control teams (n=329) entered the study, with no group differences in gender or competition level. Dropout during the study and the numbers included in the analyses are shown in figure 1. The male players in the intervention group were younger compared with the control group, with no other group differences in anthropometrics or demographics (table 1). Players reported having played handball for an average of 14 years (SD 5, range 4–37). The majority were right-handed (78%). There were no group differences in playing position, with 40% backs, 24% wings, 14% line players, 13% goalkeepers and 7% reporting multiple positions.
Age, height and body mass by gender for both groups
Shoulder pain and problems at baseline
At the time of inclusion, 145 players (45%) in the intervention group and 155 players (48%) in the control group reported a history of shoulder pain during the previous handball season. Current shoulder pain was reported by 93 players (29%) in the intervention group and 96 players (30%) in the control group. At baseline, 155 players (47%) in the intervention group and 156 players (48%) in the control group reported a shoulder problem during the previous 7 days based on the OSTRC Overuse Injury Questionnaire. Of these, 45 players (14%) in the intervention group and 46 players (14%) in the control group reported a substantial shoulder problem. There were no group differences in the prevalence of shoulder pain or problems reported at baseline.
Shoulder injuries and surgery at baseline
Five players (1.6%) in the intervention group and seven players (2.2%) in the control group reported an acute shoulder injury within the past 6 months; however, all participated in normal handball activity. Team medical staff confirmed this and specified the diagnoses: two superior labral lesions and three anterior shoulder dislocations in the intervention group and six superior labral lesions and one anterior dislocation in the control group. One player (0.3%) in the intervention group and two players (0.6%) in the control group had undergone shoulder surgery within 12 months before baseline; however, all three were participating in normal handball activity. There were no group differences in the prevalence of acute shoulder injuries or surgery reported at baseline.
Response rate
The average response rate for the OSTRC Overuse Injury Questionnaire was 87% (range 84–93%) in the intervention group and 85% (range 82–87%) in the control group. Complete injury data were available from 57% and 65% of the players in the intervention and control groups, respectively. Eighty per cent (n=264) of the players in the intervention group and 82% (n=270) in the control group met the a priori criteria of at least three responses. Female players had a higher response rate, with no group differences between the intervention (90%) and control groups (89%). The average response rate for the exposure data was 67% (range 58–79%) in the intervention group and 49% (range 30–67%) in the control group. The average response rate for the compliance data in the intervention groups was similar to that for the injury data, 87% (range 84–92%).
Exposure
There were no group differences in the average weekly exposure to handball training or match play (table 2). However, the players in the control group reported having completed 17 more minutes of strength training per week on average (p=0.004).
Average weekly exposure to handball training, match play and strength training in both groups
Compliance
On average, the OSTRC Shoulder Injury Prevention Programme was completed 1.6 times per week (range 1.4–1.8) in the intervention group, 53% of the 3 times recommended. Twenty-one players (7%) did not complete the exercise programme at all during the season. Seventy-nine players (28%) reported an average compliance of between 0.1 and 1.0, 91 players (32%) between 1.1 and 2.0, and 90 players (32%) >2.0 sessions per week. The average compliance per week did not differ between players without shoulder problems compared with players with shoulder problems at baseline (1.57 vs 1.60, p=0.791).
Acute shoulder injuries
A total of 20 and 13 acute injuries were reported in the intervention and control groups, respectively, corresponding to an average prevalence of acute shoulder injuries throughout the season of 1.4% (95% CI 0.8% to 1.9%) in the intervention group and 0.9% (95% CI 0.5% to 1.2%) in the control group (mean difference 0.5%). These injuries were excluded from the following analysis examining the effect of the exercise programme.
Effect of the intervention
The average prevalence of overuse shoulder problems during the season was 17% (95% CI 16% to 19%) in the intervention group and 23% (95% CI 21% to 26%) in the control group (mean difference: 6%). The average prevalence of substantial shoulder problems was 5% (95% CI 4% to 6%) in the intervention group and 8% (95% CI 7% to 9%) in the control group (mean difference 3%). The six prevalence measures in both groups are illustrated in figure 3. GEE analysis revealed a 28% lower risk of reporting shoulder problems over time in the intervention group compared with the control group (OR 0.72, 95% CI 0.52 to 0.98, p=0.038). We did not detect a significant difference in the risk of reporting substantial shoulder problems over time between the intervention and control groups (OR 0.78, 95% CI 0.53 to 1.16, p=0.23).

{kind=link}
{kind=link}
{kind=link}
Prevalence of shoulder problems (open symbols) and substantial shoulder problems (filled symbols) in the intervention (squares) and control group (triangles), with 95% CIs, measured six times during the season.
Within the intervention group, compliance did not influence the risk of shoulder problems (table 3). However, players in the intervention group who reported an average compliance of at least 0.1 sessions per week (n=248) had a 69% lower risk of reporting substantial shoulder problems than players reporting zero compliance (n=16; OR 0.31, 95% CI 0.15 to 0.67, p=0.003).
Generalised estimating equation model including players in the intervention group meeting the a priori criteria of sufficient injury data (n=264)
The average severity score of the shoulder problems reported was 29 (95% CI 28 to 31) in the intervention group and 35 (95% CI 32 to 37) in the control group (mean difference 5). The relative impact of shoulder problems was 64% lower in the intervention group (intervention group 5.2 vs control group 8.1).
GEE models including only players with shoulder problems at baseline revealed a 35% lower risk of reporting shoulder problems in the intervention group than the control group (OR 0.65, 95% CI 0.43 to 0.98, p=0.04). However, we detected no significant difference in the risk of reporting substantial shoulder problems between groups (OR 0.86, 95% CI 0.51 to 1.45, p=0.58). When only including players without shoulder problems at baseline, we identified no significant group difference in the risk of reporting shoulder problems (OR 0.80, 95% CI 0.47 to 1.37, p=0.42) or substantial shoulder problems (OR 0.68, 95% CI 0.36 to 1.31, p=0.25) during the season.
Unintended effects
No severe shoulder injuries were reported due to completion of the exercise programme in the intervention group. However, at the start of the study, two coaches reported a total of four cases of players experiencing muscle soreness after completing the exercise programme.
Discussion
Our main finding was that a 10 min exercise programme, the OSTRC Shoulder Injury Prevention Programme, reduced the prevalence of shoulder problems and substantial shoulder problems among elite handball players; the risk of reporting shoulder problems during the competitive season was 28% lower in the intervention group.
This is the first randomised controlled trial investigating an exercise programme designed to reduce overuse shoulder injuries in elite throwing athletes,29 although similar observations were reported from a 6-month pilot study with 53 female junior handball players (three teams) in the intervention group.37 They found that the prevalence of shoulder symptoms decreased significantly during the intervention period among players completing specific shoulder-strengthening exercises. The exercise programme was completed as a part of the warm-up three times per week and consisted of three exercises, push-up plus, standing glenohumeral internal and external rotation with elastic band as resistance, similar to exercises included in the current study.
On average, the exercise programme was completed 1.6 times per week in the intervention group, only 53% of the 3 times recommended. No clear dose–response relationship was identified. However, players within the intervention group actually performing the exercise programme had a 69% lower risk of reporting substantial shoulder problems compared with players not performing the exercise programme in the intervention group. On this basis, it seems that it is enough to complete the exercise programme between one and two times per week to achieve the reported effect.
Subanalyses including only players with a self-reported shoulder problem at baseline revealed a 35% significantly lower risk of reporting shoulder problems during the season in the intervention group. In contrast, we found no significant effect of the exercise programme when including only players without a shoulder problem at baseline, even if their compliance was as good as that among players with shoulder problems at baseline.
Methodological considerations
A major strength of this trial is the use of cluster randomisation to avoid crossover effects between the intervention and control groups. We also stratified for gender and competition level to ensure that groups were comparable. An injury surveillance method recently developed and validated to study overuse injuries was employed to capture the true extent of shoulder problems.31 ,38 Parallel registration of acute shoulder injuries was done by players and team medical staff to avoid misreporting of acute injuries as overuse injuries. This allowed us to assess the effect of the exercise programme on the prevalence of overuse problems alone. However, a limitation of the injury registration method is the lack of detailed diagnostic information on each case. Our definition of a shoulder problem encompasses all physical symptoms and may have multiple causes, such as subacromial and internal impingement, tendon pathology, glenoid labrum injuries, glenohumeral joint instability and acromioclavicular joint dysfunction.14 ,15 ,39 ,40 The effect of the exercise programme reported in this trial may differ between these; we were unable to discriminate between such relationships.
Traditionally, injury prevention studies exclude players injured at baseline and only record new cases throughout the study, with incidence as the measure for risk. Applying such an approach in the current trial would be inappropriate. First, excluding players reporting a shoulder problem at baseline would have resulted in a biased study population, not representative of athletes from throwing sports, where shoulder problems are very common. Therefore, we included all players participating in normal handball activity, irrespective of their baseline injury status or history. Second, overuse shoulder problems are often chronic, with periods of remission and exacerbation. Only a handful of the cases reported in this trial represented first-time problems. Therefore, the proportion of players affected by shoulder problems at any given time, the population prevalence, is a more appropriate measure of the magnitude of the problem.38
The prevalence of shoulder problems reported in the control group is lower than in a recent study on risk factors for shoulder problems among male elite handball players using the same injury registration method,2 possibly due to a crossover effect. Before agreeing to participate in the study and before the randomisation process, all coaches and players received the same information about the study, both orally and in writing. This may have increased the awareness of shoulder problems in the control group, even though we encouraged them to train as usual. We had no control over whether the control group performed exercises similar to our exercise programme. In fact, the control group reported doing more strength training than the intervention group, possibly because they replaced the exercise programme with additional strength training. Nevertheless, any bias arising from contamination would result in an underestimation of the preventive effect reported in this trial.
Simple comparison of prevalence measures between the intervention and control groups revealed a lower average prevalence of shoulder problems and substantial shoulder problems reported during the season in the intervention group. The main benefits of this comparison are that it is easy to calculate and takes into account all available injury data. It is, however, made on crude summary measures of prevalence and does not account for change over time, confounding or missing. A high response rate and sufficient completeness of injury data allowed us to address missing using multiple imputation techniques. We could therefore perform GEE analysis to include players meeting our a priori criteria of at least three responses to the OSTRC Overuse Injury Questionnaire. The GEE is a more robust analysis which accounts for repeated measures and allowed us to compare changes in prevalence of shoulder problems between the intervention and control groups over time, revealing a significantly lower risk of reporting shoulder problems in the intervention group. However, we underestimated the number of players needed to establish the effects of the exercise programme on substantial shoulder problems.
Baseline demographics, anthropometrics or injury status/history of injury had no confounding effect on the comparison of prevalence of shoulder problems or substantial shoulder problems between groups over time. However, a limitation of our GEE analysis was the inability to include player exposure as a potential confounder, due to a lower response rate for the exposure data, although we found no difference in the reported exposure to handball training or match play between groups.
The exercise programme evaluated in this trial is comprehensive and includes exercises to improve glenohumeral rotation, external rotation strength and scapular muscle strength, as well as improve kinetic chain and thoracic mobility. We did not conduct baseline and follow-up testing to examine the effect of the exercise programme on the different risk factors targeted; this is a limitation of the study.
When developing and introducing the exercise programme, we followed recommendations from implementation research, for example, limit the length of the programme, enhance variation in the exercises and equip the delivery agents with skills to confidently implement the programme.41 ,42 Despite this, the players in the intervention group reported only having completed the exercise programme 53% of the three times recommended per week; this is a limitation of the study. To ensure quality in the performance of the exercises, we instructed the team medical staff to be present at certain periods during the intervention. However, the extent to which this was followed remains unknown; this is a limitation of the study.
The methods used to monitor player exposure and compliance with the exercise programme deviate from former injury prevention studies and have several limitations.43–45 First, exposure was self-reported as the number of minutes and compliance was self-reported as the number of sessions completed during the past 7 days; both are vulnerable to recall bias. Second, the season averages for exposure and compliance are approximations based on the six measurements taken during the season.
Implications
Our results suggest that an exercise programme targeting glenohumeral internal rotation, external rotation strength, scapular muscle strength, kinetic chain and thoracic mobility should be included as a part of the general warm-up in elite handball. Whether the preventive effect observed in this trial can be generalised to other throwing athletes is not known. However, the internal modifiable risk factors associated with shoulder problems in other throwing sports are similar to those in handball.2 ,3 ,5 ,6 ,18–25 It therefore seems reasonable to assume that the OSTRC Shoulder Injury Prevention Programme could benefit other throwing athletes as well.
Conclusion
The OSTRC Shoulder Injury Prevention Programme, an exercise programme to increase glenohumeral internal rotation, external rotation strength and scapular muscle strength, as well as improve kinetic chain and thoracic mobility, reduced the prevalence and risk of shoulder problems in elite handball and should be included as a part of the warm-up in throwing sports.
What are the findings?
The Oslo Sports Trauma Research Center (OSTRC) Shoulder Injury Prevention Programme, an exercise programme to increase glenohumeral internal rotation, external rotation strength and scapular muscle strength, as well as improve kinetic chain and thoracic mobility, reduced the prevalence and risk of reporting shoulder problems in elite handball.
How might it impact on clinical practice in the future?
The OSTRC Shoulder Injury Prevention Programme should be included as a part of the warm-up in throwing sports.
Acknowledgments
The authors would like to thank A Aune, A Skjølberg, C Skovly, D Major, EE Eriksen, HK Vileid, K Røed, K Søderstrøm, M Fagerheim, MJ Olsen, OT Østvold, RM Kristensen and R Nesje for their assistance in data collection. They also thank all players and coaches who participated in the study, as well as the team medical staff. The Oslo Sports Trauma Research Center has been established at the Norwegian School of Sport Sciences through generous grants from the Royal Norwegian Ministry of Culture, the South-Eastern Norway Regional Health Authority, the International Olympic Committee, the Norwegian Olympic Committee & Confederation of Sport, and Norsk Tipping AS.
References
Footnotes
Twitter Follow Stig Andersson at @stighandersson and Benjamin Clarsen at @benclarsen
Contributors All authors contributed to project planning, data collection and manuscript preparation. SHA was responsible for data analysis. SHA is responsible for the overall content as the guarantor.
Competing interests None declared.
Ethics approval The South-Eastern Norway Regional Committee for Research Ethics approved the study. Participation was voluntary and the authors obtained individual written informed consent from players or guardians.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All data are available on request.