Article Text

Abstract
Background The optimal timing of MRI following acute hamstring injury is not known and is mainly based on expert opinions.
Aims To describe the day-to-day changes in the extent of oedema and investigate the optimal timing for detection of fibre disruption on MRI following acute hamstring injuries.
Study design Prospective, descriptive study.
Methods We performed standardised MRI (1.5T) ≤1 day after injury in male athletes with acute hamstring injury. If initial MRI revealed positive signs of injury (increased signal intensity on fluid sensitive sequences), consecutive MRIs were obtained daily throughout the subsequent week (ie, 7 times). The MRI parameters (day 1–7) were scored by a single radiologist using a standardised scoring form. The day-to-day changes in the extent of oedema (distance from tuber, craniocaudal length, mediolateral width and anteroposterior depth) and the presence and extent of fibre disruption (tear) were assessed with descriptive statistics and repeated measures using analysis of variance of log-transformed data. The overall main effect for time was reported with a significance level set at p<0.05.
Results 13 out of 132 male athletes assessed for eligibility between January 2014 and December 2015 were included. 1 dropped out, while 12 (31 years, range 20–49) completed the study; 11 had 7 MRI scans each and one had 5 MRI scans performed. There were no significant day-to-day changes for any of the extent of oedema measures (p values ranging from 0.12 to 0.81). Fibre disruption (tear), present in 5 of the athletes, was detectable from day 1, with small and insignificant day-to-day changes (p values ranging from 0.45 to 0.95).
Conclusions We observed insignificant day-to-day changes in the extent of oedema throughout the first week following acute hamstring injury. Fibre disruption (tear) was detectable from the first day after injury. These findings indicate that MRI can be performed on any day during the first week following an acute (hamstring) muscle injury.
- Hamstrings
- Muscle
- MRI
Statistics from Altmetric.com
Introduction
Acute hamstring injury is the most frequent non-contact muscle injury in sports involving high-speed running1–10 with a consistently high incidence7 ,11 ,12 and reinjury risk.2 ,7 ,13–16 MRI is widely and increasingly used as a diagnostic and prognostic tool following acute hamstring injury. A positive MRI diagnosis is established if increased signal intensity consistent with characteristic MRI features of a muscle strain injury, such as oedema and fibre disruption (presence of well-defined fluid collection/focal area), is demonstrated on fat-suppressed fluid-sensitive sequences (spin-echo T2-weighted, proton density-weighted images or short-τ-inversion-recovery images).17–19
There is currently no consensus on the optimal timing for MRI following an acute hamstring injury.20 A recent literature review and expert opinion20 recommended imaging at 1–2 days post-trauma. However, this recommendation was based on an in vivo rabbit study21 where controlled strain was applied to the tibialis anterior muscle, showing that the amount of oedema was histologically maximal after 24 hours and decreased after 48 hours. A similar time frame (24–48 hours) is also requested in the large UEFA Champions League injury studies,14 ,15 ,22 whereas Speer et al23 recommend MRI between 1 and 3 days postinjury as an ideal time, based on the occurrence of oedema (which is one of the predominant histological findings in muscle strains). However, evidence to support these expert-based recommendations for the optimal timing to detect the presence and extent of oedema and fibre disruption is lacking. Other experimental studies have suggested that signs of acute muscle strain injuries are best detected on MRI between 24 hours and 5 days,24 ,25 but data are limited to small samples sizes, different muscle groups investigated and no continuous daily MRI throughout the first week after injury.
The prognostic value of various MRI findings for return to sports (RTS) after acute hamstring injuries has been investigated in observational studies,14 ,15 ,26–39 where the average values for single MRI performed within 1–6 days after injury are reported. It is, however, not known whether the poor predictive value of MRI for RTS recently reported32 ,33 ,39 may have been affected by the variation in the timing of the MRI investigations.
Serial MRI of intramuscular haematoma has been studied in one rat model study,40 but there are no human data available on the time course of MRI changes during the acute stage (≤7 days). The aims of this study were therefore: (1) to describe the day-to-day changes in the extent of oedema and (2) to investigate the optimal timing for detection of fibre disruption following acute hamstring injuries.
Materials and methods
Study design
This prospective descriptive study was conducted at a specialised orthopaedic and sports medicine hospital in Qatar. The study was approved by the Ethics Committee of Aspetar Orthopaedic and Sports Medicine Hospital, the Shafallah Medical Genetics Centre Ethics Committee and the Anti-Doping Lab Qatar (ADLQ) Institutional Review Board (IRB) Committee. We obtained written informed consent from all participants.
Participants
Between January 2014 and December 2015, we consecutively recruited professional and recreational male athletes with acute onset of posterior thigh pain and presentation within 24 hours after the injury. An overview of the eligibility criteria is presented in table 1. The athletes were recruited from clubs and federations in Qatar, mainly through the Qatar National Sports Medicine Program (NSMP). We also encouraged colleagues at the hospital to contact the principal investigator if they became aware of any athletes with an acute hamstring injury. Eligibility was assessed and determined at the outpatient department by a sports medicine physician.
Eligibility criteria
Clinical and MRI examinations
Clinical diagnosis
Within 24 hours after the onset of the index injury, the sports medicine physician performed standardised comprehensive patient history taking and clinical examinations, including active and passive range of motion testing, active SLUMP test, manual muscle resistance testing and palpation.41 If an acute hamstring injury was clinically suspected, an initial MRI examination was performed within the first day after index injury.
MRI protocol
The initial MRI examination was performed with the patient in the supine position. Images of the hamstring muscle were obtained from the ischial tuberosity to the knee using a 1.5 Tesla magnet system (Magnetom Expert, Siemens, Erlangen, Germany) with a phased-array surface coil and additionally two-body matrix coils, which were strapped over the injured thigh and centred over the painful area. We attached a vitamin E capsule to the patient's posterior thigh corresponding to the point of maximal tenderness on palpation to function as a marker and confirmed with the athlete. Coronal and axial fast-spin echo proton density-weighted images were first obtained and subsequent coronal and axial fast-spin echo proton density fat-saturated images were obtained. In table 2, we present a detailed overview of the MRI sequences used.
MRI parameters
Consecutive MRI examinations
When the initial MRI examination was positive for an acute hamstring injury (increased signal intensity on fluid-sensitive sequences), MRI examinations were obtained every day throughout the subsequent week using an identical protocol. We attempted to perform the MRI as close to a 24-hour interval as possible.
MRI assessments
One experienced radiologist with more than 10 years of experience within musculoskeletal radiology assessed and scored the MRIs using a standardised scoring form based on the literature.14 ,26 ,28 ,29 ,36 ,42 In a previous study, we reported good-to-excellent intratester and intertester reliability with the same radiologist involved.43 The radiologist was blinded to the clinical status of the injury. We considered the muscle injured if the MRI demonstrated increased signal abnormality on fluid-sensitive sequences (proton density-weighted fat-saturated images), defined as abnormal intramuscular increased signal compared with the unaffected adjacent muscle tissues. Quantitative assessments of the maximal extent of the oedema included tridimensional measurements (mm) of the craniocaudal length, mediolateral width and anteroposterior depth of increased signal intensity in the slice where the maximal extent of oedema was present. We also scored the distance from the most cranial pole of the injury to the ischial tuberosity on the coronal sequences. The extent of tear (presence of fluid collection/focal area of well-defined high signal intensity indicating fibre disruption) was measured in the same three dimensions (mm) as described above.
The involved muscle(s) were described and the anatomical location within the muscle was scored (proximal tendon, proximal musculotendinous junction, proximal muscle belly, distal muscle belly, distal musculotendinous junction, distal tendon),36 ,44 and within the same third (proximal, middle, distal) of this anatomical location. Conjoint tendon injury was scored if the common tendon of the biceps femoris and semitendinosus was injured.45 Finally, we scored the overall severity injury grading (grade 0–III) using an MRI modification14 of Peetrons'42 classification (grade 0: no abnormalities, grade I: oedema (increased signal intensity) without architectural distortion, grade II: oedema (increased signal intensity) with architectural disruption, grade III: complete tear). If more than one muscle was injured or more than one lesion within the muscle was observed, the muscle (or lesion) with the greatest extent of signal abnormality was defined as the ‘primary’ lesion and included in the analysis. The seven consecutive MRIs of each case were scored in sequence, day 1–7.
Treatment and rehabilitation throughout the course of imaging
Eligible participants were also asked to participate in an ongoing randomised controlled trial (RCT; ClinicalTrials.gov Identifier: NCT02104258) on the effectiveness of two different hamstring rehabilitation protocols. Rehabilitation appointments were scheduled directly following each MRI examination, leaving ∼23 hours between potential loading and the next MRI examination. Athletes not included in the RCT did not receive any standardised treatment.
Throughout the first week participants were not allowed to take any medications (non-steroidal anti-inflammatory drugs, NSAIDs) or receive any local treatment or physical modalities (including soft tissue treatment/massage, taping, needling techniques at the injury site). They were also strongly discouraged to load their injured leg with exercises provoking pain or perform any high-speed running or heavy eccentric exercises. All athletes completing the study received a computer tablet as compensation.
Statistical analysis
We performed the statistical analyses using SPSS software (V.21.0; SPSS, Chicago, Illinois, USA). Continuous variables were tested for normality using the Kolmogorov-Smirnov test (where a p value >0.05 was considered as normally distributed) and presented as mean (95% CI) and median values (IQR). We described categorical variables (such as type and level of sports, number of muscles injured and injury location) as frequencies and proportions.
To assess the effect of time on the changes in the extent of oedema (dependent variables: distance from tuber; craniocaudal length; mediolateral length; anteroposterior length), we conducted a one-way repeated measures analysis of variance (ANOVA) using time (day; 7 days) as within-participants factor (independent variable). Similar ANOVA analyses were conducted to assess the effect of time on the extent of tear (dependent variables: craniocaudal length; mediolateral length; anteroposterior length). In these analyses, we excluded one case with 2 days of imaging missing. We performed a log transformation when data were not normally distributed and if our data violated the assumption of sphericity, a Greenhouse-Geisser correction was applied. The significance level was set at p<0.05.
In absence of comparable studies, we were unable to perform a power calculation. We therefore arbitrarily decided that n≥8 would be adequate for descriptive analyses.
Results
An overview of the flow of participants is presented in figure 1. Of 132 professional and recreational athletes assessed for eligibility, 13 met the criteria for inclusion and volunteered to take part in the study. They all had the initial MRI examination within the first day after injury (day 1) with positive MRI findings, indicating acute hamstring injury, and were scheduled for consecutive MRI examinations in the 6 subsequent days. All athletes had their MRI within the first 12–24 hours after injury, except for one athlete, who due to logistical reasons, had the first initial MRI after 27 hours. Median (IQR) time from injury until initial MRI examination was 18 hours (2.5). One athlete dropped out after initial MRI examination (due to difficulties attending the follow-up MRI examinations), while 12 completed the study with a median age of 30.5 years (range 20–49), median weight 86 kg (range 71–106) and median height 183 cm (range 170–203). Of these, 11 completed all 7 days of imaging and 1 completed 5 days (missed appointments at days 4 and 5). One athlete reported having taken NSAID after injury before the initial examination, but refrained from it after first consultation. Out of these 12 athletes, 6 agreed to participate in the RCT and started standardised physical therapy within the first 3 days after injury. The remaining athletes did not start physical therapy during the first week. Baseline characteristics of the included athletes are listed in table 3.
Baseline characteristics (n=12)

Study flow chart.
Anatomical location
In the seven cases where only the biceps femoris long head was involved, four were located in the proximal myotendinous junction, two in the distal myotendinous junction and one in the distal muscle belly. For the case involving the semimembranosus, the injury was in the proximal myotendinous junction. In the four cases with a conjoint tendon injury, the biceps femoris was the most affected muscle. Of the five cases with fibre disruption, four were scored with involvement of the central tendon.
Extent of oedema
The day-to-day changes (from days 1 to 7) in the extent of the oedema are shown in figures 2 and 3. The intraindividual day-to-day changes of the MRI features (within participants) were considerably smaller than the interindividual variability (between participants). There was no main effect for time for any of the oedema measurements when including the 11 athletes with complete imaging data (ANOVA with repeated measures and Greenhouse-Geisser corrections): distance to tuber (F(1.105, 11.045)=2.287, p=0.16), mediolateral width (F(2.347, 23.472)=2.285, p=0.12), anteroposterior depth (F(2.347, 23.475)=0.255, p=0.81), craniocaudal length (F(2.949, 29.486)=1.733, p=0.18).
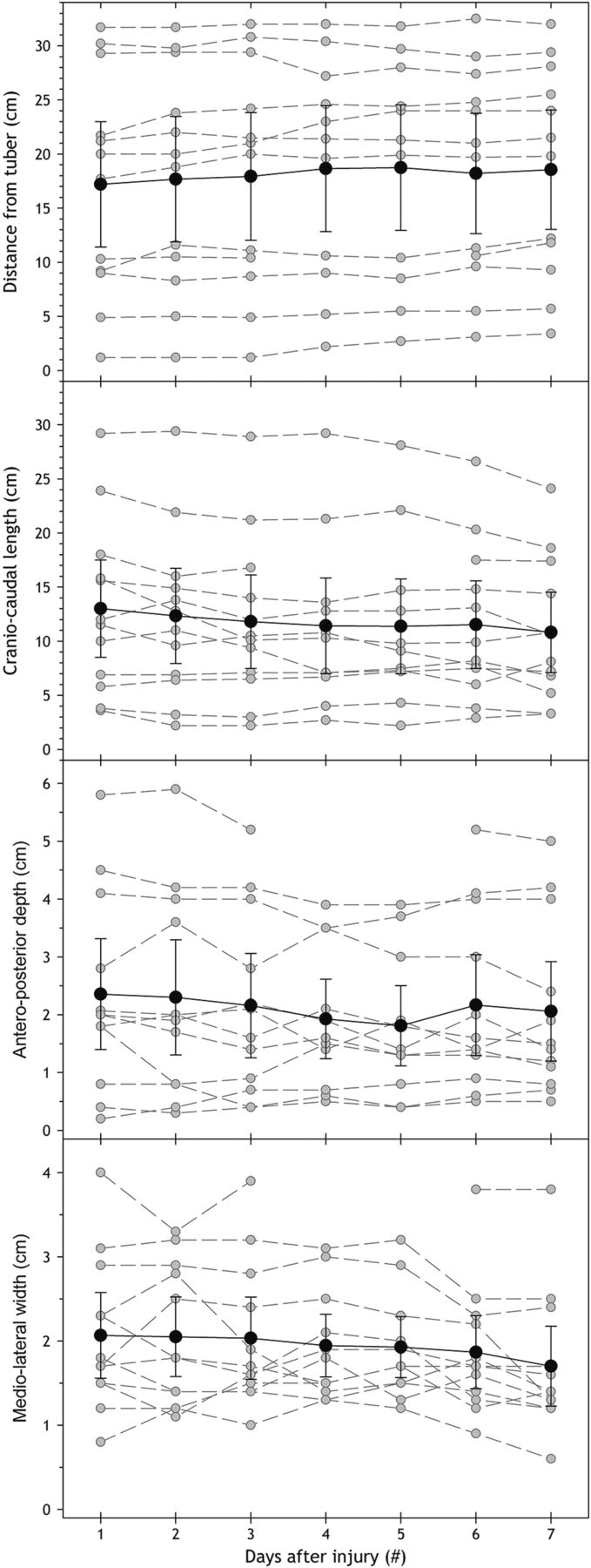
Day-to-day changes in the extent of the oedema measures from days 1 to 7, n=12. The grey circles and dotted lines represent individual cases, while the black circles and solid lines represent the group mean values with the corresponding 95% CI.

Consecutive axial proton density-weighted (fat-saturated) MRIs from days 1 to 7 for one of the participants show the extent of increased signal intensity (oedema) at the musculotendinous junction of the conjoint tendon of the long head of the biceps femoris and semitendinosus.
Extent of tear (fibre disruption)
The presence of fibre disruption was detectable from day 1 in five cases. The day-to-day changes of the extent of the tear from days 1 to 7 are presented in figure 4, illustrating the day-to-day changes in the craniocaudal length of the tear. There was no main effect for time for any of the measurements in the four athletes with complete imaging data (ANOVA with repeated measures): mediolateral extent (F(6, 18)=0.266, p=0.95), anteroposterior extent (F(6, 18)=0.875, p=0.53), craniocaudal extent (F(6, 18)=1.007, p=0.45; figure 5).

Day-to-day changes of craniocaudal length of the tear (fibre disruption) from days 1 to 7, n=5. The grey circles and dotted lines represent individual cases, while the black circles and solid lines represent the group mean values with the corresponding 95% CI.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
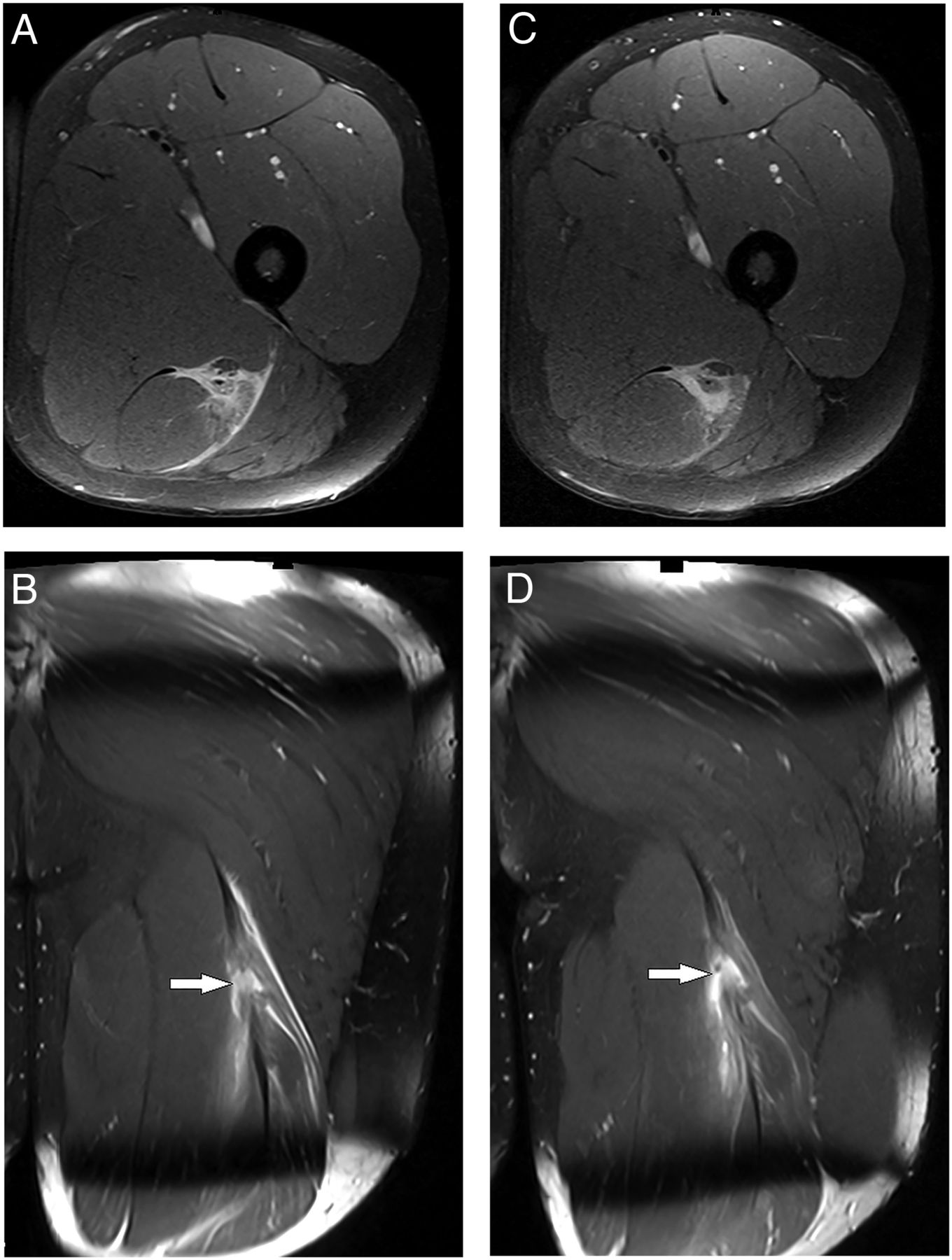
Axial (A) and coronal (B) proton density-weighted (fat-saturated) MRIs on day 1 after injury show oedema and fibre disruption demonstrated as a well-defined area (gap) filled with heterogeneous increased signal intensity (fluid collection) in the conjoint tendon (white arrows). On day 7, the increased signal intensity has not changed significantly and the fibre disruption is still present (C and D).
Discussion
Daily serial MRI examinations performed throughout the first week following acute hamstring injuries in 12 professional and recreational athletes showed that the extent of oedema and fibre disruption (tear) essentially remain unchanged. Hence, from a clinical point of view, the MRI can be performed on any of these days within the first week.
We observed only minor changes in the extent of oedema, where the intraindividual day-to-day changes of the MRI features were insignificant and considerably smaller than the large interindividual variability. The presence of fluid collection indicating fibre disruption (tear) was detectable from the first day after the injury and remained virtually constant in size during the course of the MRI.
There are no clinical studies in the literature investigating the day-to-day changes of MRI features of acute muscle injury throughout the first week. Previous recommendations, which are mainly based on expert opinions or small experimental studies, advise that MRI should be performed between day 1 (24 hours) and day 3 postinjury.14 ,20 ,23 However, these recommendations cannot be supported by the data presented here, as we found a time frame between 1 and 7 days to be sufficient for performing MRI after acute hamstring injuries.
For the extent of the oedema, we found no significant changes between days 1 and 7 after the injury. Muscle healing after a muscle strain injury follows a complex process of well-coordinated steps including degeneration and inflammation (occurring within the first days postinjury), followed by regeneration (usually occurring between 5 and 10 days postinjury) and a proliferative phase during which development of muscle fibrosis (scar tissue) occurs.46–50 The ultrastructural changes as a result of the injury, where torn myofibrillar Z bands cause protein degradation with release of protein-bound ions leading to oedema, may be visualised (as increased signal intensity) if beyond the resolution of MRI.19 ,51
The evolution of acute hamstring injury throughout this acute stage, during which degeneration and inflammation occur, has not previously been described in athletes with MRI and our findings cannot directly be compared with the previous histological literature. However, since there is an overlap between the inflammatory phase and the regenerative phase,47 oedema is still expected to be present at this stage, which corresponds with our findings.
As we did not continue the MRI after the first 7 days, we do not know when and how fast the signal intensity decreases after the first week. Askling et al35 ,36 found changes in MRI parameters over time, where the changes were significant between initial MRI at day 4 and the first MRI follow-up at day 10 for the length, depth and volume in sprinters36 and for the length and volume in the ballet dancers,35 whereas no significant changes were found for the distance from the ischial tuberosity between these time points. As we did not find any significant changes between any of the oedema measurements between days 1 and 7, the decrease in signal intensity seems to occur after 7 days from the initial injury. However, due to small samples sizes, no definite conclusions can be drawn. Moreover, increased signal intensity has been reported to be present for a prolonged time following injury in a major part of injured athletes long after they have clinically recovered and have returned to sports participation,28 ,35 ,36 ,52–54 and an exact time point for when a significant reduction in the extent of oedema might be challenging to identify and likely due to individual variations. For fibre disruption, the extent can only be indirectly measured on MRI as the presence of fluid collection/focal area of well-defined high signal intensity indicates fibre disruption, thus an exact description of the fibre disruption cannot be given without using advanced technical software.
Although studies have reported associations between MRI findings and time to RTS following acute hamstring injuries,14 ,15 ,22 ,26–31 ,34–38 there is currently no strong evidence for any MRI finding that might accurately predict an RTS prognosis after acute hamstring injury, which is at least in part attributable to the high risk of bias in current literature.39 The additional predictive value for RTS of MRI above clinical examinations is also found to be limited.32 ,41 It may be questioned whether consistent or appropriate timing (in the first week) of the MRI in these studies has contributed to the poor prognostic ability of imaging findings in predicting RTS duration. The findings in this study indicate that the limited predictive value of MRI for time to RTS is not explained by the variation in timing of the MRI after the acute hamstring injury.
Strengths
This is the first study investigating the day-to-day changes of MRI characteristics following acute muscle injury. The standardised examination procedures performed at the same study centre (using the same 1.5 T MRI scanner) increases the consistency (and internal validity) of our study.
Limitations
There are some limitations that need to be acknowledged. First, the relatively small sample size prevents us from performing more advanced statistical analysis (such as repeated measures linear mixed models) and might have increased the risk of a type II error. However, given the data presented, we suggest that a larger sample size is unlikely to substantially change our main findings that no significant day-to-day changes occur during these first 7 days. Also, because the athlete population in Qatar is predominantly male, we chose to include only male participants. The sample was also biased towards a relatively low grade of injury.
We performed the MRI measurements based on two-dimensional images and the same MRI machine with high spatial resolution and adequate field strength (1.5 Tesla). It remains unknown whether using more advanced MRI techniques and software17 ,55 and/or higher field strength MRI would have provided more accurate measurements or different results.
Fibre disruption (extent of tear) was only observed in five athletes, and although the presence and extent of the tear were consistent between those five, studies with larger numbers are needed to confirm these findings.
Although the athletes were advised not to perform any activity provoking pain or heavy eccentric loading, they were not restricted to refrain from normal, pain-free activity. As the pain reduced through the course of imaging, they might have increased their general activity level, and we cannot ensure that the injured leg was loaded more towards the last days of imaging as a result. This might have resulted in smaller reduction (or enlargement) of the extent of oedema than expected, due to a possible exercise-related increase in signal intensity, which is seen in studies using T2 relaxation time mapping (functional MRI) during and after exercise.17 ,56–58 However, the athletes following a structured rehabilitation programme had their rehabilitation scheduled directly after the MRI each day, leaving ∼23 hours between the rehabilitation session and the next MRI appointment. All the initial MRI examinations were obtained the first day after injury (between 12 and 27 hours), leaving at least 12 hours between the acute onset of injury and the first MRI. The evolution of an acute hamstring injury on MRI within the very first hours directly after injury therefore still remains unknown.
Clinical implications
In daily clinical practice, MRI is used as a supportive tool for confirmation of the diagnosis and grading of the injury. Time pressure on the availability of the MRI scanner (efficiency of healthcare), physical distance to an MRI facility (eg, during a training camp) and environmental pressure (RTS decisions) are practical issues for medical staff dealing with acute muscle injuries. This study clearly shows that MRI can be performed on each day during the first week after the injury. This gives the medical staff and athlete more flexibility in the timing of the MRI without sacrificing the diagnostic accuracy.
Conclusion
We observed insignificant day-to-day changes in the extent of oedema throughout the first week following acute hamstring injury. Fibre disruption (tear) was detectable from the first day after injury without change over time. Therefore, MRI can be performed on each day during the first week following an acute (hamstring) muscle injury with equivalent findings.
What are the findings?
There were no significant day-to-day changes in the extent of the oedema throughout the first week following acute hamstring injury.
The extent of tear was detectable from day 1 after injury and virtually constant throughout the first week.
How might it impact on clinical practice in the future?
This study shows that optimal MRI can be performed on any day during the first week after the injury, which gives the medical staff and athlete more flexibility in the timing of the MRI without sacrificing its accuracy.
Acknowledgments
The authors direct a special thanks to the radiologists and the radiographers in the Radiology Department at Aspetar; without their great support and assistance, this study could not have been executed. The authors thank the Sports Medicine Physicians, the staff in the Outpatient Department and the National Sports Medicine Program (NSMP) for taking the time in a busy schedule contributing to the study. Thanks to Andreas Serner for assisting with data collection. Finally, the authors acknowledge all the participants for their contribution.
References
Footnotes
Twitter Follow Arnlaug Wangensteen @arnlaugw
Contributors AW designed the study, monitored data collection, analysed and interpreted data and drafted the article. JLT and RB designed the study, interpreted the data, revised the article and approved the final revision of the article. EA analysed the MRIs, interpreted the data, revised the article and approved the final revision of the article. EW and RW interpreted the data, revised the article and approved the final revision of the article.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Ethics Committee of Aspetar Orthopaedic and Sports Medicine Hospital, the Shafallah Medical Genetics Centre Ethics Committee and the Anti-Doping Lab Qatar (ADLQ) Institutional Review Board (IRB) Committee.
Provenance and peer review Not commissioned; externally peer reviewed.